dysphagia related to tracheostomy & ventilation · replaced every 28-30 days ... inflated cuff...
TRANSCRIPT
1
Presented By:
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
DYSPHAGIA RELATED TO TRACHEOSTOMY &
VENTILATOR DEPENDENCE
Ventilation
Ventilation Indications
Disruption of normal air exchange into and out of lungs
Causes of respiratory failure:
Respiratory illness
Cardiac events
Neurological injury
Neuromuscular disease
Trauma
Environmental contamination
Airway obstruction
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Ventilation Associated Complications
Lung barotrauma
Oxygen toxicity
Atelectasis
Nosocomial pneumonia
Decreased venous return
Decreased cardiac output
Hypotension
Gastrointestinal bleeding
Malnutrition
Decreased urine
output/altered renal
function
Altered fluid balance
Increased intracranial
pressure
Respiratory alkalosis
Accidental disconnect of
ventilator/power loss
Loss of airway pressure
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Artificial Airways
Artificial Airway Purposes
Maintain patent airway
Connect to mechanical ventilation
Provide access to lungs for pulmonary toilet
Control ventilation
Control oxygenation
Circumvent airway obstruction
Reduce aspiration potential
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

2
Endotracheal Intubation
Insertion of endotracheal tube into airway
Somewhat flexible but retains shape in airway
Used for short-term:
To provide artificial airway
To connect to mechanical ventilation for airway protection and
ventilation
May stabilize severe facial fractures
May not be possible with tracheal stenosis and tumors
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Orotracheal Intubation
Orotracheal: Inserted into mouth, passing through pharynx and vocal
folds into trachea
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Nasootracheal Intubation Nasotracheal: Inserted into nose, passing into pharynx and vocal
folds into trachea
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Short-Term Endotracheal Intubation
Complications
Trauma
Otitis media
Damage to vocal folds or recurrent laryngeal nerve
Hypoxemia
Improper positioning
Esophageal intubation or rupture
Cardiac complications
Traumatic extubation with cuff inflated
Increased intracranial pressure
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Long-Term Endotracheal Intubation
Complications
Pressure necrosis
Granuloma
Stenosis
Laryngeal web
Glottic incompetence
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Cricothyroidotomy
Emergency surgical opening into
cricothyroid membrane
Potential complications:
Chronic vocal changes
Injury to:
Trachea
Larynx
Vocal cords
Esophageal perforation
Subglottal stenosis
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

3
Tracheotomy
Surgical opening directly into trachea
May be maintained as long as needed
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheotomy
Surgical or endoscopic
procedure
Between 2nd and 3rd
tracheal rings
Horizontal vs. vertical
incision Thyroid Cartilage
Tracheal Rings Cricoid Cartilage
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Materials
Disposable:
Can retain bacteria
Should be discarded and
replaced every 28-30 days
Non-disposable: Must be
sterilized routinely
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Materials: PVC
Disposable
Inexpensive
Widely used
More rigid than silicone
Soften in heat
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Materials: Silicone
Disposable or non-disposable
Flexible
Softer than PVC or metal
May weaken and collapse over
time
Contains fewer chemical additives
Properties reduce encrustation of secretions and tendency of
bacteria to adhere to tube
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Materials: PVC/Silicone Mix
Commonly used
Strength of PVC with bacteria resistance of silicone
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

4
Tracheostomy Materials: Metal
Silver or stainless steel
More sanitary
Not typically used for individuals
requiring ventilation
Less comfortable
Often used at home
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Size
Often denoted on flange
Typically measured in French sizes
Determined based on age, weight, and height
Goal:
Tube with sufficient airflow but not too large
Fill no more than ⅔-¾ of tracheal lumen
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components
1. Outer Cannula
2. Cuff
3. Pilot Line
4. Pilot Balloon
5. 15 mm hub
6. Flange
7. Obturator
8. Button
9. Inner cannula
10. Syringe 1 2
3 4
5
6
7
8 9
10
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Flange
Allows tube to be held in place with
string ties
Prevent:
Tube from advancing into trachea
Accidental decannulation
Often denotes some features
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Outer
Cannula
Provides basic structure
Remains in place to maintain airway
Single lumen tubes:
Have only outer cannula
Least airway resistance
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Inner
Cannula
Can be removed: For cleaning
Quickly if obstructed
Smaller lumen increases work of breathing
May be disposable or non-disposable
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

5
Tracheostomy Components:
Fenestration
Windows/holes in body of outer or
inner cannula
Allows air to pass from trachea to vocal
folds
Not used in individuals at high risk for
aspiration
Often used as part of weaning process
Improperly aligned fenestration may
result in:
Granulation
Occlusion Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components:
Fenestration
Non-Fenstrated
Inner Cannula Fenstrated Inner
Cannula Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Cuff
Cuff:
Internal balloon surrounding body of
tracheostomy tube
Compensates for area in tracheal
lumen not filled by tube
Soft plastic molds to tracheal walls
Prevents air from escaping around
tube, especially during ventilation
Reduces risk of aspirated material
immediately entering trachea
Cuffless: Allows air to escape around
body of outer cannula to upper airway
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Cuff
High volume, low pressure
Low volume, high pressure
Pressure-controlled
Foam
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Cuff
Inflated Cuff & Pilot Deflated Cuff & Pilot
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Components: Pilot
If tracheostomy is cuffed:
Pilot line: pathway for air
to inflate and deflate cuff
Pilot balloon:
Indicates amount of air in
cuff
Prevents air escape from
cuff
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

6
Tracheostomy Components
Obturator
Button:
Closes tracheostomy
Used during
weaning/decannulation
process
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Benefits (Compared to
ET tube)
Decreased risk of accidental decannulation
Improved secretion management
Larynx is not involved in procedure
Decreased airflow resistance
Increased comfort
Decreased physical restriction
Increased options for oral feeding and communication
Options for transfer out of intensive care unit
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Tracheostomy Complications Pneumothorax
Bleeding
Inadvertent decannulation
Cardiorespiratory arrest
Thyroid injury
Recurrent laryngeal nerve damage
Cuff rupture
Discomfort
Infection at stoma
or in trachea
Tracheal web
Pneumonia
Aspiration
Ineffective cough
Dysphagia
Tracheal granuloma
Tracheomalacia
Tracheal stenosis
Fistulae
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Swallowing Physiology
Impact
Swallow may or may not be affected by presence of
tracheostomy
Potential for dysphagia is increased due to:
Tracheostomy tube presence
Surgical procedures
Neurological/respiratory impairments
Risk of aspiration is increased by presence of tracheostomy
Consequences of aspiration are more serious
Impaired smell and taste
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Impact: Laryngeal Excursion
Reduced due to:
Fixation of muscles
Weight of equipment and tubing
Cuff inflation anchors tracheostomy tube
Results in:
Decreased tongue base movement and propulsion force
Dragging along walls during attempts at elevation
Inflated cuff partially obstructing esophagus
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

7
Impact: Laryngeal Excursion
Esophageal
Bulge Cuff in Place
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Impact: Secretions
Disturbance in saliva and secretion management due to:
Airflow disruption
Medication side effects
Thick secretions
Infections
Interruption of filtration and hydration
Results in:
Insufficient saliva
Excess saliva
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Impact: Airway Pressure
Decreased subglottic pressure:
When normal, prevents oropharyngeal contents from entering
airway
Valsalva maneuver
Results in: accumulation of residue in pharynx
Mechanical ventilation may result in less aspiration than
spontaneous breathing with tracheostomy
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Impact: Glottic Competence
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Impact: Glottic Competence
Decreased glottic closure response:
Gradual loss of laryngeal sensation
Eliminates reflexive cough and throat clear
Reduced cough effectiveness
May use expiratory airflow of ventilator for airway
clearance if cuff is deflated
Incoordination of glottic closure with swallow
Disruption of apneic interval when ventilator is required
Protective function does not immediately return once cuff
is deflated
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Normalizing Airway Pressure During swallow, nearer normal pressure can be attained by: Digital occlusion
One-way valve
Capping
Individuals who are ventilator-dependent: Often swallow worsens when on ventilator
Tidal volume may be increased to compensate for lost volume and to provide increased subglottic pressure
Must learn to time swallow with ventilator cycle of expiration
With ventilator, instruct in glottic control to compensate for air leak during cuff deflation
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

8
Cuff Deflation for Swallow
Cuff Deflation
At least partial cuff deflation should be attained prior to
swallow assessment and feeding:
Cuff deflated sufficiently for air to move through larynx
Allows brief occlusion of tracheostomy
Cuff must be at least partially deflated to identify
potential aspiration
Full cuff deflation is goal
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Cuff Deflation
Partial Deflation Full Deflation
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
With Cuff Inflation
Fully inflated cuff should not completely seal against tracheal
walls
Aspirated material can pool on top of cuff and may:
Fall into airway when cuff is deflated even with proper
suctioning after cuff deflation
Fall between trachea and cuff, especially as cuff slides with
movement of larynx
Become bacterially colonized
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
With Cuff Inflation
With fully inflated cuff, individual cannot cough through
larynx to clear laryngeal vestibule
With repetitive swallow movements, inflated cuff rubbing
on tracheal walls can cause tracheoesophageal fistula
Without cuff deflation, only oral stage and ability to trigger
swallow can be assessed
Individuals who are so medically fragile as to preclude cuff
deflation are usually not candidates for significant oral intake
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
With Cuff Inflation Material Above and
Around Cuff
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
9
With Cuff Inflation
Oral intake should be deferred until at least partial cuff
deflation is achieved
If medical clearance cannot be attained:
Fully explain and document limitations and dangers of
swallowing in presence of inflated cuff
If physician has been educated and still desires individual eat
with fully inflated cuff, recommendations made during
dysphagia assessment are useless
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Suctioning and Cuff Deflation
Suctioning and Cuff Deflation
“…Clinicians must be competent to perform any activity by virtue of education, training, and experience”
Appropriate training and support is necessary to undertake any activity in which SLP is not already competent
SLP may perform suctioning and cuff deflation if accepted under State Licensure and fully trained
“Suctioning is complicated and can be a life threatening procedure. The procedure should always be done by those who are properly trained and know the complications and the individual.”
ASHA's Code of Ethics
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Suctioning and Cuff Deflation
Mississippi Department of Health is silent, stating “it is a
scope of practice issue”
It is advisable for each facility to develop written policy that
addresses:
Level of involvement of SLP
Training required
Mechanism for verifying competency
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Suctioning Indications
Inability to effectively clear secretions
Need to remove material from airway to prevent obstruction
Respiratory conditions
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Suctioning Material Above Cuff
Foreign materials collect in airway above
level of cuff
Suctioning through tracheostomy tube
with inflated cuff does not remove
material above cuff
Materials above cuff are cleared by
suctioning via mouth and through vocal
folds or after cuff deflation
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
10
Suctioning Complications
Mucosal trauma
Cardiac arrhythmia
Hypoxemia due to oxygen being removed from lungs
Laryngospasm
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
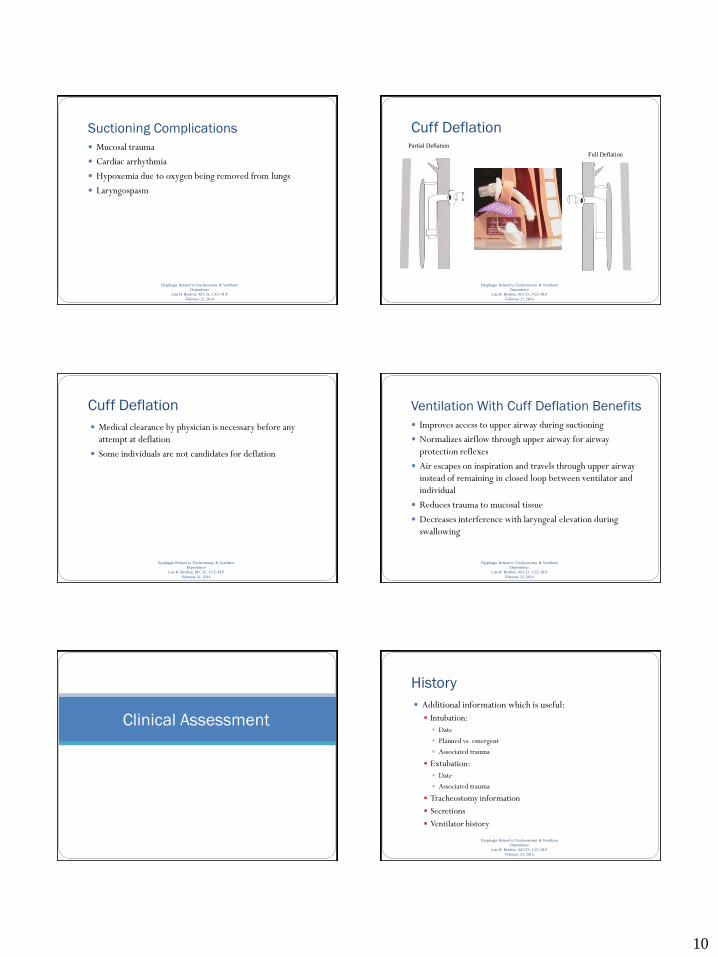
Cuff Deflation
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Partial Deflation
Full Deflation
Cuff Deflation
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Medical clearance by physician is necessary before any
attempt at deflation
Some individuals are not candidates for deflation
Ventilation With Cuff Deflation Benefits
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Improves access to upper airway during suctioning
Normalizes airflow through upper airway for airway
protection reflexes
Air escapes on inspiration and travels through upper airway
instead of remaining in closed loop between ventilator and
individual
Reduces trauma to mucosal tissue
Decreases interference with laryngeal elevation during
swallowing
Clinical Assessment
History
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Additional information which is useful:
Intubation:
Date
Planned vs. emergent
Associated trauma
Extubation:
Date
Associated trauma
Tracheostomy information
Secretions
Ventilator history

11
Contraindications to Assessment
Decreased alertness
Extreme agitation
Severe cognitive impairment
Medical instability
Extreme fragility
Inflated cuff
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Clinical Assessment
Valuable but limited information is gathered
Rarely is final step in tracheostomy dysphagia assessment:
Typically leads to instrumental assessment
Only if completely confident of individual’s ability to manage
oral intake should recommendation for oral feeding be made
based solely on clinical assessment
More often, stand0alone when already eating and there are
questions regarding management of particular diet or when
aspiration is overt
May require multiple sessions
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Clinical Assessment Procedure
Oro-motor assessment
Suction
Deflate cuff
Digital occlusion or one-way valve placement:
Phonate
Cough
Clear throat
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Clinical Assessment Procedure
Dry test swallow:
Prior to advancing to trial swallows, consider if individual
can:
Swallow
Phonate
Clear throat
Expectorate secretions
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Clinical Assessment Procedure
Trial swallows:
Assess with tracheostomy unoccluded and with tracheostomy
occluded during swallow
Provide controlled bolus sizes and types
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Clinical Assessment Procedure
Observe:
Oral transit/control
Initiation speed
Pharyngeal swallow
Vocal quality changes
Cough: cough may occur unrelated to swallow due to changes in
sensations and pulmonary status
Increased secretions or need for suctioning
Typical signs of dysphagia and aspiration
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

12
Clinical Assessment Procedure
Encourage cough or throat clear if needed
Suction, rest, re-suction
Re-inflate cuff and return to baseline ventilator settings, if
needed
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Clinical Assessment Reliability
Limitations
Possible loss of cough reflex
Changes in vocal quality or inability to phonate
Secretion management differences
General decreased reliability of clinical assessment in
identifying aspiration
Cannot assess:
Cause of aspiration
Compensatory strategies
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Cervical Auscultation
Tracheal sounds observed with tracheostomy differ from those without tracheostomy
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Blue Dye Test Used to enhance ability to discern bolus from surrounding
mucosa or secretions
May identify aspiration of more than trace amounts
May not effectively identify trace aspiration
Optimally performed over several sessions during 48-72 hour period
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Blue Dye Test Protocol Place 2-3 drops of sterile water mixed with blue food
coloring on tongue
Suction trachea immediately and at 15-minute intervals over 1 hour period, recording presence of any blue material in tracheal secretions
Can repeat secretion testing every 4 hours over 48-hour period
Does not compromise individual, as individual only aspirates own secretions
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Blue Dye Test Protocol If no evidence of aspiration of saliva, can mix blue dye with
food consistencies
Proceed one consistency at time, waiting at least 4-6 hours between consistencies
Positive result: Presence of blue material in any tracheal suctioning
Alerts to presence of aspiration
Dictates conservative approach to further assessment
Negative result:
Absence of dye
Allows further test swallows
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

13
Blue Dye Test Protocol Alert nursing and respiratory care staff that blue dye test is in
progress
Cuff status should be noted during presentations and suctioning
Bedside tracking sheet assists with documentation of suctioning results
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Blue Dye Test Tracking Sheet
DATE
TIME
CONSISTENCY
PRESENTED
CUFF
STATUS
DYE PRESENCE
None Min. Mod . Sev.
INITIALS
Name:___________________ Date:______________
SLP: _____________________ Phone #: ____________
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Blue Dye Test Limitations
Up to 50% false-negative error rate
Subjective grading of degree of dye present
Unable to determine:
Cause of aspiration
Timing of aspiration
Quantity of aspiration
Effectiveness of compensatory strategies
Should be interpreted conservatively and not used exclusively to determine candidacy for oral feeding
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
One-Way Valve Use
One-Way Speaking Valves
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
“It is the role of the speech-language pathologist, following
referral from and in collaboration with medical specialists,
to determine the need for and appropriate type of voice
prostheses. The speech-language pathologist also assesses the
effectiveness of these communication devices and provides
rehabilitation to help the individual obtain an optimum level
of communication function.”
One-Way Speaking Valves
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Function:
Allows air to enter tracheostomy tube on
inspiration
During expiration, valve is closed, and air is
directed into trachea and upward to vocal
folds
Can be used with individuals using
oxygen, humidified air, or ventilator
Entire team should be aware of purpose
and use of valve One-Way
Valve

14
One-Way Speaking Valve Benefits
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Normalizes airflow
Restores more normalized
physiology
Design inhibits secretions from
entering tracheostomy
One-Way Speaking Valve Requirements
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Awake and alert
Tolerance of full cuff deflation:
Proper size of tube relative to tracheal
lumen
48-72 hours after tracheostomy initially
performed or tracheostomy change to
allow for decrease in edema
Airflow with One-Way Valve
and Cuff Inflated
One-Way Speaking Valve
Contraindications
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Inflated cuff
Tracheostomy tube with sponge or foam-filled cuff
Airway obstruction that affects airflow through upper airway even when tracheostomy size is adjusted and cuff deflated
Bilateral adductor vocal cord paralysis
Severe tracheal/laryngeal stenosis
Unstable medical/pulmonary status
Reduced lung elasticity which may create air trapping
Unmanageable, thick, copious pulmonary secretions
Endotracheal tube
Unconscious; comatose; sleeping
Laryngectomy
One-Way Speaking Valve Cautions
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Respiratory treatments or medications should not be
administered during valve use
Caution should be taken with:
End-stage pulmonary disease
Heat moisture exchange device
One-Way Speaking Valve Procedure
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Position individual optimally
Instruct with procedure for deflation and speaking valve
placement
Suction appropriately (tracheal and oral)
Deflate cuff:
Allow acclimation prior to initial placement of valve
Make necessary changes to ventilator settings
Cuffless tracheostomy is ideal and should be considered
Monitor continually
Remove T-Piece if needed
One-Way Speaking Valve Procedure
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Attempt digital occlusion
If digital occlusion tolerated place valve
If inner cannula of tracheostomy has grasp ring:
Ensure ring does not extend beyond hub of tracheostomy tube
If ring does impede valve movement, remove inner cannula

15
One-Way Speaking Valve Procedure
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Observe for:
Adequate airflow around tube
Signs of respiratory distress
Prolonged, excessive coughing
If any distress (or at completion of trial):
Remove valve
Replace T-piece
Re-inflate cuff
Return to original ventilator settings
Swallow Treatment
Treatment After assessment, treatment can proceed similarly to
individuals without tracheostomy
If swallow is not elicited, treatment focus is on indirect treatment to elicit swallow until individual consistently swallows independently
Therapeutic feeding trials: considerations same as with clinical assessment with tracheostomy
When full cuff deflation is not possible: Some exercises can be used to strengthen and prepare for swallow
Repeated laryngeal elevation required by some exercises increases potential for tracheo-esophageal fistulae
Consider each exercise individually
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Compensatory Techniques
Changes in posture:
Chin tuck
Head turn
Chin tuck & turn
Head tilt
Head back
Reclined
All may be physically difficult due to equipment in place
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Compensatory Techniques
Diet modifications:
Non-oral options
Changes in consistency of liquids
Changes in consistency of solids
Teach digital occlusion during swallow and for several
seconds after swallow
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Compensatory Techniques
Changes in bolus presentation:
Bolus size
Rate
Placement
Clearance
No straw
Liquid by spoon
No talking
Moisten mouth prior to meal
Can proceed as without tracheostomy
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

16
Compensatory Techniques
Increased sensory input:
Temperature
Pressure
Flavor
Texture
Can proceed as without tracheostomy
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Facilitation Strategies (Caution with
Full Cuff Inflation)
Effortful Swallow
Mendelsohn Maneuver: Often used in individuals with tracheostomy
Supraglottic Swallow Maneuver: Difficult to maintain breath hold unless digital occlusion or one-way valve is in place
Super-Supraglottic Swallow Maneuver: Difficult to maintain breath hold unless digital occlusion or one-way valve is in place
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Therapeutic Techniques Oral motor exercises
Tongue base exercises
Pharyngeal exercises: Masako: Caution with full cuff inflation
Laryngeal elevation exercises: Contraindicated with full cuff inflation
Laryngeal closure exercises: Breath hold difficult to maintain unless digital occlusion or one-way valve is in place
Thermal-tactile stimulation
Sour bolus swallows
VitalStim: Adjustments are made to electrode positioning
DPNS: Contraindicated
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Other Issues
Endotracheal Intubation First meal after extubation, individual
is at high risk for aspiration
Greatest risk of aspiration is within 24 hours following extubation
Greatest risk of respiratory distress and re-intubation is within 4-6 hours after extubation
Immediately after extubation, individual often exhibits hoarseness, spontaneous coughs, and congestion, making clinical observations unreliable
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Consider
Goal is to reduce risk for clinical decompensation
Must consider when treating individuals with tracheostomy:
Aspiration characteristics
Condition of individual
Underlying lung condition
Systemic factors can interfere with compensation
Continued monitoring is crucial, since individuals with
tracheostomy often demonstrate more rapid and frequent
changes in tolerance of feedings than other populations
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014

17
References
American Speech-Language-Hearing Association. (1993). Position statement and guideline for the use of voice prostheses in tracheotomized persons with or without ventilator dependence. ASHA, 35, Suppl. 10: 17-20: [Position Statement]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2004). Role of the speech-language pathologist in the performance and interpretation of endoscopic evaluation of swallowing guidelines [Guidelines]. Available from www.asha.org/policy.
American Speech-Language-Hearing Association. (2010). Code of ethics [Ethics]. Available from www.asha.org/policy.
Conway, N. (1994). Speech evaluation of the individual with a tracheostomy tube. Imaginart. Bisbee, AZ.
Crary, M. A., Groher, M. E. (2003). Introduction to adult swallowing disorders. Butterworth Heinemann. St. Louis.
Dikeman, K. J., Kazandjian, M. S. (1995). Communication and swallowing management of tracheostomized and ventilator dependent adults. Singular Publishing, San Diego.
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Dougherty, D. (2009). Bedside evaluation of the dysphagia individual. Cross Country Education.
Feldman, S. A., Deal, C. W., Urquhart, W. (1966). Disturbance of swallowing after tracheotomy. Lancet, 1: 954-955.
Finucane, B. T., Tsui, B. C. H., Santora, A. H. (2011). Principles of airway management. New York: Springer.
Fornataro-Clerici, L., Roop, T. A. (1997). Clinical management of adults requiring tracheostomy tubes and ventilators: A reference guide for healthcare practitioners.
Groher, M. E. (1984). Dysphagia: Diagnosis and management. Butterworth Publishers. Boston.
Logemann, J. (1992). Management strategies during videofluoroscopy. Course III.
Logemann, J. A. (1993). Manual for the videofluorographic study of swallowing, Second Edition; Pro-Ed.
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Logemann, J. A. (1998). Evaluation and treatment of swallowing disorders.
Pro-Ed. Austin, Tx.
Murray, J, Sullivan, P. A. (2006). FEES and modified barium swallow (MBS)
for fragile individuals. ASHA Health Care 2006.
Nash, M. (1988). Swallowing problems in the tracheostomized individual.
Otolaryngologic Clinics of North America, 21(4): 701-709.
NMMC Policy & Procedure. (2005).Tracheostomy care of site.
NMMC Acute Rehabilitation Services-Speech-Language Pathology Policy &
Procedure. (2011). Bedside swallow assessment.
Passy-Muir Inc. (2008). Passy-Muir tracheostomy & ventilator swallowing
and speaking valves instruction booklet.
Siddharth, P., Mazzarella, L. (1985). Granuloma associated with fenestrated
trachestomy tubes. American Journal of Surgery, Vol. 150: 279-280.
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014
Sottille, F. D., Marrie, T. J., Prough, D. S., Hobgood, C. D., Gower, D. J.,
Webb, L. X., Coserton, J. W., Gristina, A. G. (1986). Nosocomial pulmonary
infection: Possible etiologic significance of bacteria adhesion to endotracheal
tubes. Critical Care Medicine, 14(4): 265-270.
Sullivan, P. A. (2006). Aspiration syndromes and polypharmacy in critically
ill individuals. ASHA Health Care 2006.
Tippett, D., Siebens, A. (1991). Using ventilators for speaking and
swallowing. Dysphagia, 6: 94-99.
Weymuller, E. A. (1992). Prevention and management of intubation injury of
the larynx and trachea. American Journal of Otolaryngology 13(3): 139-144.
Dysphagia Related to Tracheostomy & Ventilator
Dependence
Lisa H. Renfroe, M.C.D., CCC-SLP
February 21, 2014