dx imaging #2 –5/14/08 - logan class of december...
TRANSCRIPT

Dx Imaging #2 –5/14/08
*** Syllabus Review ****** Pretest ***
PRE TEST AND REVIEW*** The first part of the info is a review of CT scans, MRI’s and other imaging tools…This is a review of DX Imaging #1 and Fundamentals of diagnostic imaging…See those notes for more info ***
4.Definne: A). Congenital anomaly: Something that you are born with. (ex. Straight back syndrome, pectus excavatum, and mechanical/patholgical murmurs) B). Normal Variant: Ex.Limbus…Does not change clinical picture, but is not truly normal. These are often acquired but have lack of clinical significanceC). Dysplasia: Often imvolves multiple systems and look repeatable with similar features and risk profiles…Every dysplasia is a congenital anomaly but not every congenital anomaly is a dysplasia.
5.What is the classification system used for soft tissue calcificationCategory Serum Ca+ Tissue Function
Physiological Normal – Tissue is easy to see Normal TissueDystrophic Normal-local pH changes Damaged TissueMetastatic High Normal
Physiologic: Thyroid cartilage, rib cartilage, iliolumbar ligament, pineal glandDystrophic: Myositis Ossificans, Calcific tendonitis, Calcific Bursitis Metastatic: Hyperparathyroidism (PTH elevates serum calcium way too much), Widespread lytic metastasis and multiple myeloma.
DX IMAGING – 5/19/08
OVERVIEW OF THE CATEGORIES OF ARTHRITISCategories1. Degenerative (the biggest category of arthritis)/OA 2. Inflammatory 3. Metabolic Arthritides (all members have crystalline deposition) 4. Septic
DJD/OAThe most common arthritide we know is degenerative joint disease/osteoarthritis (OA). It is the poster-child for the category of degenerative arthritis.
RARheumatoid arthritis is an autoimmune problem. We describe RA as the poster child for inflammatory arthritides.
MetabolicGout: Crystal deposition that creates physical problems. The sequence is a breakdown in purine metabolism.
SepticInfection within a joint that creates arthritis.
TermsEnthesis: The sharpey fibers embed in bone and help to anchor soft tissues (tendons, ligaments, and sometimes bone). The enthesis is a musculo-tendinous insertion in bone. In the condition, “seudotumor of the humerus” the rotator cuff attaches to sharpey’s fibers and presents as a “pseudotumor.”Osteophyte: Bone spur/bone growth…Locations typically involve vertebra and specifically come in areas of intersegmental instability or peri-articular areas or joint marginsSyndesmophytes: Calcification of outer annular fibers…(DJD is the only entity that produces osteophytes).Sero Negative: Abscense of rheumatoid factor in circulating blood.Sero Positivee: Rheumatoid factors in circulating blood.
For Each Category Answer the Following?

DJDA1. Who is the poster child? OA and DJD. We do have local inflammation within the joint complex; however the condition is not systemic (the inflammatory category has systemic inflammation).
A2. Key clinical Features: 1. Stiffness in the morning2. Time to loosen up with DJD – DJD patients loose up with time vs. RA patients who are stiff most of the day )3. ROM affected – Decreases and varies side to side4. Asymmetrical side to side presentation. 5. Local Swelling and Osteophyte formation6. Palpable changes in contour of the joint7. DJD is the most common arthritide 8. Local inflammation (very important that the event is local)9. Soft tissue changes and local swelling may be present10. Knee is commonly affected by pressure changes
A3. Key lab findings: No prominent lab profile1. Many – Tests: A). Sero NegativeB). ESR (Erythrocyte Sed Rate is not affected or – with DJD)C).Lab Biopsises show thin articular cartilageD).Higher accumulation of MMP (methyl metallo proteinases)E).Activation of cytokine pathway F). Histological changes
A4. Key radiographic features: Decrease Joint SpaceSubchondral SclerosisOsteophytesGeode Formation – Subchondral Cysts
.
Radiographic Development/PathologicProcess :1. The articular cartilage thins = The job of the articular cartilage is to decrease friction and provide cushioning.
When the cushion thins, bone receives more energy. A classic finding for knee DJD is medial joint space narrowing. The pattern is asymmetric.
2. Subchondral Sclerosis =When bone is stressed, it bone develops subchondral sclerosis. The sclerosis is a stress response for the bone to maintain integrity via a richer, trabecular network. The sclerosis absorbs more X-ray beams. Subchondral sclerosis presents radiographically after joint space narrowing.
3. Osteophytic Development = The 3rd thing to present radiographically is osteophyte formation/bony hypertrophy. When we see this, we assume the first 2 stages have already occurred.
4. Geode Formation = Geodes/subchondral cysts are filled with fluid and are located below the articular cartilage. The cysts are largely fluid filled and create pressure disturbances. There can be blood/bruising, synovial fluid, and other fluid within the cysts.
Dx Imaging – 5/21/08
DJD DefinitionGradual loss of articular cartilage combined with thickening of the subchondral bone with bony outgrowths at the joint margins, and nonspecific synovial inflammation.
Inflammatory ConditionsRAThe posterchild is RA for inflammatory arthritides. RA classically affects the hands presenting with decreased painful hand movement. RA is a polyarticular process affecting multiple parts of the body vs. DJD which usually is monoarticular. If DJD affects multiple joints, it is asymmetric affecting one area more than another. RA includes bilateral soft tissue swelling.

RA patients are often on medication to help control the inflammatory response. Diet (Mediterranean diet, Omega 3’s, flax seed oil) can be an important factor in helping to decrease the inflammatory process.
Depression can be linked with RA because of loss of function and chronic pain. There is a definite genetic component. New studies are searching for environmental triggers to the genetic component. Dietary modifications are important with inflammatory arthritis. New protocols call for supplementation of omega 3 and omega 9.
Juvenile RAAge is the most important criteria to separate juvenile from adult RA. The name doesn’t change, so if they are 40 years old with first episode at 12, it is called juvenile RA.
Locations of RARA affects: 1). Hand 2). C-Spine 3). Big joints (hips, knees, elbow)...The first place affected are small joints like the hands. Soft tissue swelling and pain are often associated with RA. Be cautious of their hands! Hands are often painful to touch, red and swollen. RA patients have pannus tissue that distorts periarticualr soft tissues creating the red and swollen appearance. There is asymmetric pull by tendons presenting with deformities and ulnar deviation of the tissues. The deformities are not reduceable and attempts to reduce are contraindicated.
Physical Presentation1. 4 Classic Descriptors apply to RA: Rubor, Dolor, Calor, Tumor (pannus tissue and local injury)2. This condition is bilateral and symmetrical (with joint involvement and soft tissue swelling)3. The MCP joints are commonly affected 4. Polyarticular5. Pannus Formation6. Non-reduceable Deformities7. Linked to Depression8. Genetically Linked with an environmental trigger9. Dietary modification and medication are helpful10. Cannot work on RA patients during periods of excacerbation due to painful, tender, and swollen joints
Laboratory Testing for RA and Inflammatory ARthritides1. Sero (Rheumatoid Factor) = Rheumatoid Factor is not universally found in all cases of RA. It may be in 90%-94%
of the patients with RA (strong association). 2. ESR = Varies within patient and within the condition3. C-Reactive Protein = C-reactive proteins is an important marker of inflammatory conditions.
Radiographical Presentation1. Deformity evidenced on radiograph…The film makes the full impact of the condition
evident2. Bilateral, Symmetric loss of joint spacing is present3. Periarticular soft tissue swelling4. Abnormal Underlying bone contour 5. Osteopenic/Periarticular osteoporosis (early presentation) 6. “Rat bite lesions”… Due to pressure erosion by pannus tissue….We lose borders of
bones (later presentation)
Metabolic ArthritidesGoutGout is the poster child. Eventually gout and the category will be named CPPD ( Calcium Pyrophospate Dihydrate). The condition affects older white males with a 3:2 ration (males:females). Protein diets coupled with dehydration cause gout to flare up. Typically, the big toes, heel and thumb of the hand are affected. These areas are thought to have increased blood flow and blood supply contributing to crystal deposition. Soft tissue contour and distortions can be present.
Crystal formation of uric acid is met with granulation tissue response by the body causing pannus formation. Pannus formation occurs with metabolic arthritides and with RA due to the formation of granulation tissue as a physiologic response to stress imposed to the body. Eventually, pressure erosion and pushing in occur.
Metabolic arthritides don’t change bone make up till quite late in the process. This is a separate and distinct quality of metabolic arthritides and gout.
The process is typically monoarticular. There can be bilateral presentation but one side will be worse. The presentations shows distortions of soft tissue causing the doctor to have difficulty inspecting and palpating the affected area (ex.-great toe.) There is deposition of uric acid crystals (ear – tophi, heel, big toe, or thumb). Pannus formation is present along with redness (hyperemia). Years of uncontrolled gout create joint alignment changes. Early radiographs show early soft tissue change and no bony changes. Uric acid crystals can calcify tissues (dystrophic calcification – due to local pH changes).
Lab FindingsThere aren’t specific lab findings for metabolic acidosis. Tissue biopsy or structural biopsy can be used. Synovial fluid can be used to determine what the CPPD is (the actual crystal involved). Needle biopsy is used for gout. Blood and urine findings can be normal for gout conditions because the crystal must be present in the blood stream or urine to present. This may only occur during excacerbations because often the crystals have decreaed productions or are eliminated normally in periods where the condition is not excacerbated.
Review of Metabolic Arthritides1. Gout is the poster child2. Can be called CPPD3. Affects older white males with more males than females affected (3:2)4. Common areas affected are big toes,heel, thumb and ear5. Areas of good blood supply are affected first6. Soft tissue contour changes and distortions may be present7. Pannus formation occurs causing eventual pressure erosion8. Boney changes are often last to present (unique to gout and metabolic
arthritides)9. Typically monoarticular process, and if bilateral it is asymmetrical10. Difficulty inspecting and palpating involved area (painful to move or touch)11. Crystal deposition can cause joint alimgnet changes (late) and soft tissue changes
(eearly)12. Dystrophic Calcification is present (due to pH changes)13. Tissue biopsy is the best test to diagnose…Urine or blood may not show
crystals
Septic/InfectionPatients present with a bad looking joint, lots of swelling and pain. Younger patients get sick quick vs. elderly patients who have an insidious onset. Both eldery and young show TTT (tenderness to touch), lots of joint swelling, destruction of both joint surfaces, warmth to the touch, and the 4 classic descriptors (rubor, dolor, calor, tumor).
Key clinical features are an upper respiratory infection, skin infection, or GI/GU infection that travels to the joint. Expect white cell elevation in this condition. ESR may not change in small joints, but larger joints may show elevated ESR. The greater the size of the joint, the greater the elevation of ESR.
Radiographical Presentation 1). Destruction of both sides of the joint space 2). Soft tissue swelling 3).cortical destruction
Overview of Septic/Infection Arthritides1. Tender to touch2. Increased Jiont swelling3. Warm to the touch4. Rubor, Dolor, Calor, and Tumor5. Associated with URTI, Skin or GI/GU infection6. White Cell Elevation7. Larger Jionts show elevated ESR
8. Radiographic Presentation: a). Both sides of joint destroyed b). Soft tissue swelling c). Cortical destruction
DJD (IN DEPTH)The approximation of the joint is at the expense of articular cartilage. This is the only condition required to be directly at the joint space. Most common joint disorder in the worldStriking age correlation
1/3 of all 65 years olds affectedMore common in men vs. women younger than 50More Common in women vs. men older than 50 – This is due to hormonal changes.
Preference for weight bearing joints of the lower extremity (hips and knees)…Also involved are cervical and lumbar spine, and some joints of the hand.
Wear and tear is a valuable and viable model to predict DJD, but it is not the only model associated with DJD.
DJD Etiology -- Known local factors associated with secondary DJDWeightInjury (occupational, recreational)Skeletal anomaliesQuadriceps strength (knee)
It has been shown that as little as 10% reduction in weight or even 10 lbs has helped to eliminate the pains associated with DJD. Proprioception and strength exercises can also help avoid injury and DJD.
Skeletal anomalies liked blocked vertebra are prone to DJD above and below the level of blocked vertebra. You may want to educate the patient on proper mechanics (good mechanics decrease the risk for DJD). Quadriceps strength is a strong predictor of DJD and knee pain. Strengthen the quadriceps to help prevent DJD in the knee.
DJD Etiology Continued -- Known Systemic Factors Reduction in estrogen levelsGenetic susceptibilityLow vitamin D and C intakeCrystal deposition diseases (can change contour and lead to secondary DJD and polyarthropathy)Paget’sMost sero- and sero + arthritides (disturb joint function to accelerate wear and tear)
DJD: A 3 Stage ProcessPhase 1: Edema and micro-cracks
Edema of the extracellular matrix, cartilage loses its smooth aspect and micro-cracks appear. There is focal loss of chondrocytes, alternating with areas of chondrocyte proliferation.
Phase 2: Fissuring and PittingThe micro-cracks deepen in the direction of forces of tangential cutting along fibrils of collagen. Clusters of chondrocytes appear and surround these clefts and at the surface.
Phase 3: ErosionFissures cause fragments of cartilage to detach. The loose fragments cause the mild inflammation. This form of inflammation is much more limited than the typical RA. Subchondral microcysts form. Microcysts can become geodes. Underlying bone exposure can pressure erode and cause cysts.
PathogenesisThe physiological homeostasis of normal articular cartilage is driven by chondrocytes. Chondrocytes synthesize collages, proteoglycans, and proteinases. DJD results from failure by chondrocytes to synthesize good quality matrix. The abnormal chondrocyte synthesis is the result of tissue activation by cytokines, lipid mediators (mainly prostaglandins), free radicals (NO, H2O2) and constituents of the matrix itself, such as fibronectin fragments. Activated chondrocytes become capable of producing pro-inflammatory mediators.
Certain proteinases are involved in the destruction of cartilage. Matrix metalloproteinases( MMP’ s) are the most potent proteinases that destroy cartilage. The MMP’s are held in check by tissue inhibitor metalloproteinases ( TIMP’s ). As long as
the MMP’s and the TMP’s are in balance, no degradation occurs. The enzyme aggrecanase also plays a major role in the degradation of the matrix.
Although DJD is classified as a non-inflammatory arthritis, inflammatory cytokines may stimulate chondrocytes to release cartilage-degrading enzymes. Lipid mediators and eicosanoids activate chondrocytes to increase synthesis of MMP’s, tipping the balance towards degradation.
Nitric Oxide pays an uncertain role in DJD. Some studies suggest an ability to induce DJD, while other studies suggest some protection of the cartilage.
DX. IMAGING #2 – 5/28/07
Table 10.1 -- General Guide to Relative Frequency of ArthritisWeekly: DJD (Osteoarthritis) Monthly: Ankylosing spondylitis, CPPD (pseudogout), DISH (more common), Osteitis Condensans Ilii (more common), Psoriatic Arthritis (more common), Rhemaotid Arthritis (more common), Synoviochondrometaplasia (some degenerative and some inflammatory features with genetic links)Yearly: Gout, Infection, Lupus Erythematosus, Reiter’s syndrome, Scleroderma
Table 10.2 – General age of Onset of Arthritis0-20 years: Juvenile rheumatoid arthritis (both sero positive and sero negative types can be in this condition)20-40 Years: Ankylosing spondylitis, osteotis condensans illii, lupus erythematosus, psoriatic arthirits, Reiter’s syndrome, Rheumatoid Arhtrhritis, scleroderma40 and Over: DJD, DISH (diffuse idiopathic skeletal hyperostosis), gout, hypertrophy osteoarhtropathy, pseudogout (CPPD – crystal deposition disease)
Table 10.3 – Arthropathies associated with GenderMale: Ankylosing Spondylitis, Gout, Hypertrophic Osteoarthropathy, Reiter’s Syndrome Secondary OsteoarthritisFemale: Juvenile Rheumatoid Arthritis, Lupus Erythematosus, Osteitis Condensans Illi, Primary Osteoarthritis, Rheumatoid Arthritis, Scleroderma
SLE fits into the inflammatory category because it is a systemic inflammatory condition.
DJD in AthletesRunning sports, martial artists, spring board divers – May get some DJD in the tibia
The DiscDiscs are cartilaginous joints that may be a site for DJD. The outer fibers of the annulus are collagen, the inner fibers of the annulus are fibrocartilage. Hyaline cartilage is present on the superior and inferior parts that attach to the end plates.
The highest concentration of GAG’s (glycosaminoglycans) is within the disk. Disc’s are very hydrophilic and grab GAG’s during a discogram. Tearing in the disc will show migration of GAG’s and fluid migration (can be seen on discograms).
Preferred site for DJDSpine, Large Weight Bearing Joints (Hip and Knee) ...We can also get DJD in other non-weight bearing joints.
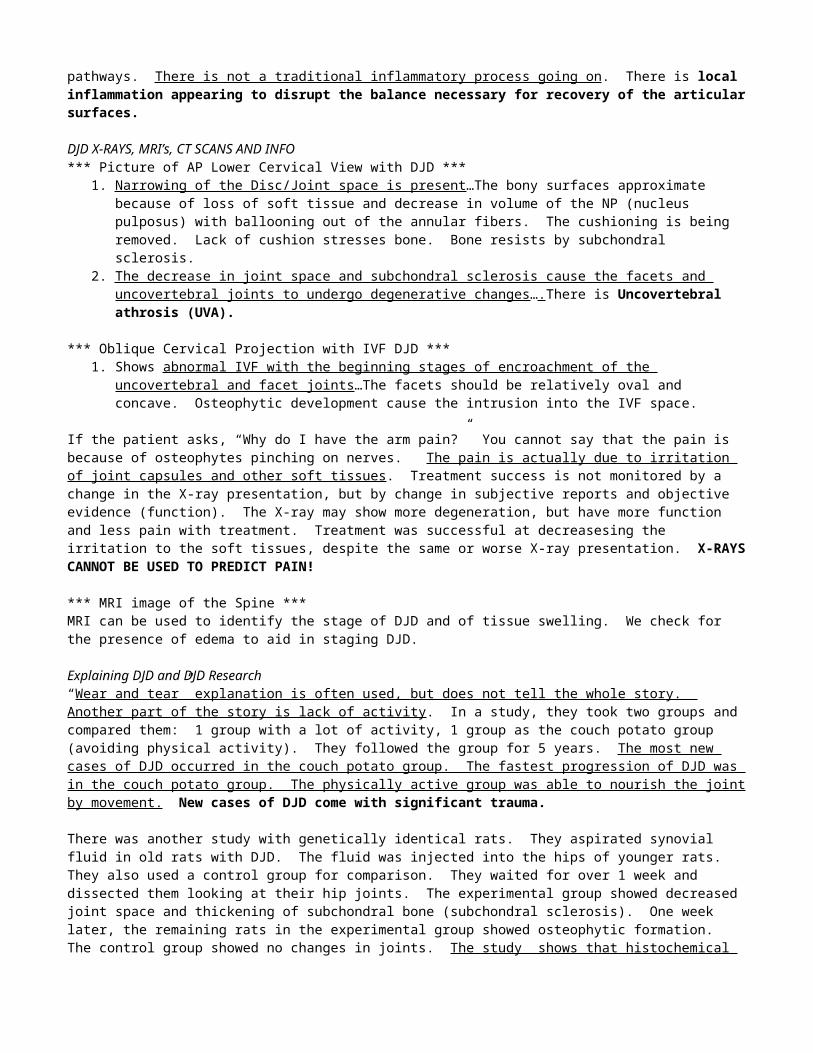
We still don’t have a clear picture of the pathogenesis of DJD. There may be multiple ways to explain DJD. DJD appears to be an endpoint of many pathomechanical pathways. There is not a traditional inflammatory process going on. There is local inflammation appearing to disrupt the balance necessary for recovery of the articular surfaces.
DJD X-RAYS, MRI’s, CT SCANS AND INFO*** Picture of AP Lower Cervical View with DJD ***
1. Narrowing of the Disc/Joint space is present …The bony surfaces approximate because of loss of soft tissue and decrease in volume of the NP (nucleus pulposus) with ballooning out of the annular fibers. The cushioning is being removed. Lack of cushion stresses bone. Bone resists by subchondral sclerosis.
2. The decrease in joint space and subchondral sclerosis cause the facets and uncovertebral joints to undergo degenerative changes….There is Uncovertebral athrosis (UVA).

*** Oblique Cervical Projection with IVF DJD ***1. Shows abnormal IVF with the beginning stages of encroachment of the uncovertebral and facet joints…The facets
should be relatively oval and concave. Osteophytic development cause the intrusion into the IVF space.
If the patient asks, “Why do I have the arm pain?” You cannot say that the pain is because of osteophytes pinching on nerves. The pain is actually due to irritation of joint capsules and other soft tissues. Treatment success is not monitored by a change in the X-ray presentation, but by change in subjective reports and objective evidence (function). The X-ray may show more degeneration, but have more function and less pain with treatment. Treatment was successful at decreasesing the irritation to the soft tissues, despite the same or worse X-ray presentation. X-RAYS CANNOT BE USED TO PREDICT PAIN!
*** MRI image of the Spine ***MRI can be used to identify the stage of DJD and of tissue swelling. We check for the presence of edema to aid in staging DJD.
Explaining DJD and DJD Research“Wear and tear” explanation is often used, but does not tell the whole story. Another part of the story is lack of activity. In a study, they took two groups and compared them: 1 group with a lot of activity, 1 group as the couch potato group (avoiding physical activity). They followed the group for 5 years. The most new cases of DJD occurred in the couch potato group. The fastest progression of DJD was in the couch potato group. The physically active group was able to nourish the joint by movement. New cases of DJD come with significant trauma.
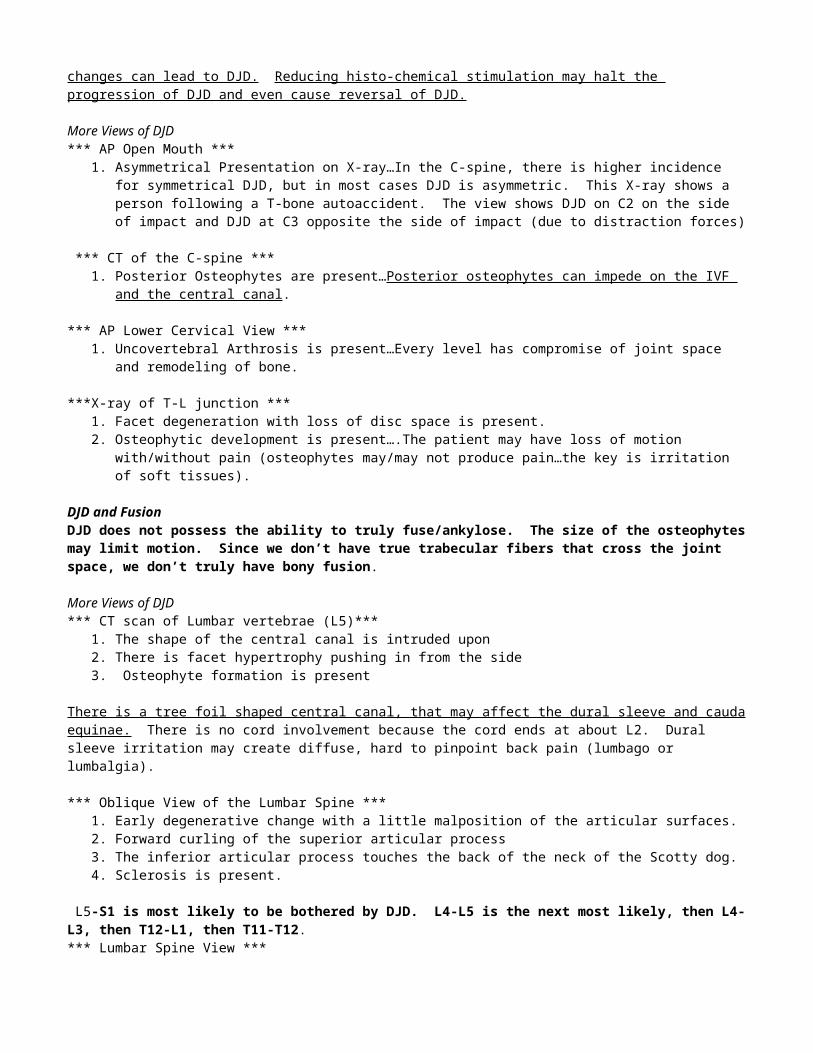
There was another study with genetically identical rats. They aspirated synovial fluid in old rats with DJD. The fluid was injected into the hips of younger rats. They also used a control group for comparison. They waited for over 1 week and dissected them looking at their hip joints. The experimental group showed decreased joint space and thickening of subchondral bone (subchondral sclerosis). One week later, the remaining rats in the experimental group showed osteophytic formation. The control group showed no changes in joints. The study shows that histochemical changes can lead to DJD. Reducing histo-chemical stimulation may halt the progression of DJD and even cause reversal of DJD.
More Views of DJD*** AP Open Mouth ***
1. Asymmetrical Presentation on X-ray…In the C-spine, there is higher incidence for symmetrical DJD, but in most cases DJD is asymmetric. This X-ray shows a person following a T-bone autoaccident. The view shows DJD on C2 on the side of impact and DJD at C3 opposite the side of impact (due to distraction forces)
*** CT of the C-spine ***1. Posterior Osteophytes are present…Posterior osteophytes can impede on the IVF and the central canal.
*** AP Lower Cervical View ***1. Uncovertebral Arthrosis is present…Every level has compromise of joint space and remodeling of bone.
***X-ray of T-L junction ***1. Facet degeneration with loss of disc space is present.2. Osteophytic development is present….The patient may have loss of motion with/without pain (osteophytes may/may
not produce pain…the key is irritation of soft tissues).
DJD and FusionDJD does not possess the ability to truly fuse/ankylose. The size of the osteophytes may limit motion. Since we don’t have true trabecular fibers that cross the joint space, we don’t truly have bony fusion.
More Views of DJD*** CT scan of Lumbar vertebrae (L5)***
1. The shape of the central canal is intruded upon2. There is facet hypertrophy pushing in from the side3. Osteophyte formation is present
There is a tree foil shaped central canal, that may affect the dural sleeve and cauda equinae. There is no cord involvement because the cord ends at about L2. Dural sleeve irritation may create diffuse, hard to pinpoint back pain (lumbago or lumbalgia).
*** Oblique View of the Lumbar Spine ***1. Early degenerative change with a little malposition of the articular surfaces.2. Forward curling of the superior articular process3. The inferior articular process touches the back of the neck of the Scotty dog. 4. Sclerosis is present.
L5-S1 is most likely to be bothered by DJD. L4-L5 is the next most likely, then L4-L3, then T12-L1, then T11-T12. *** Lumbar Spine View ***
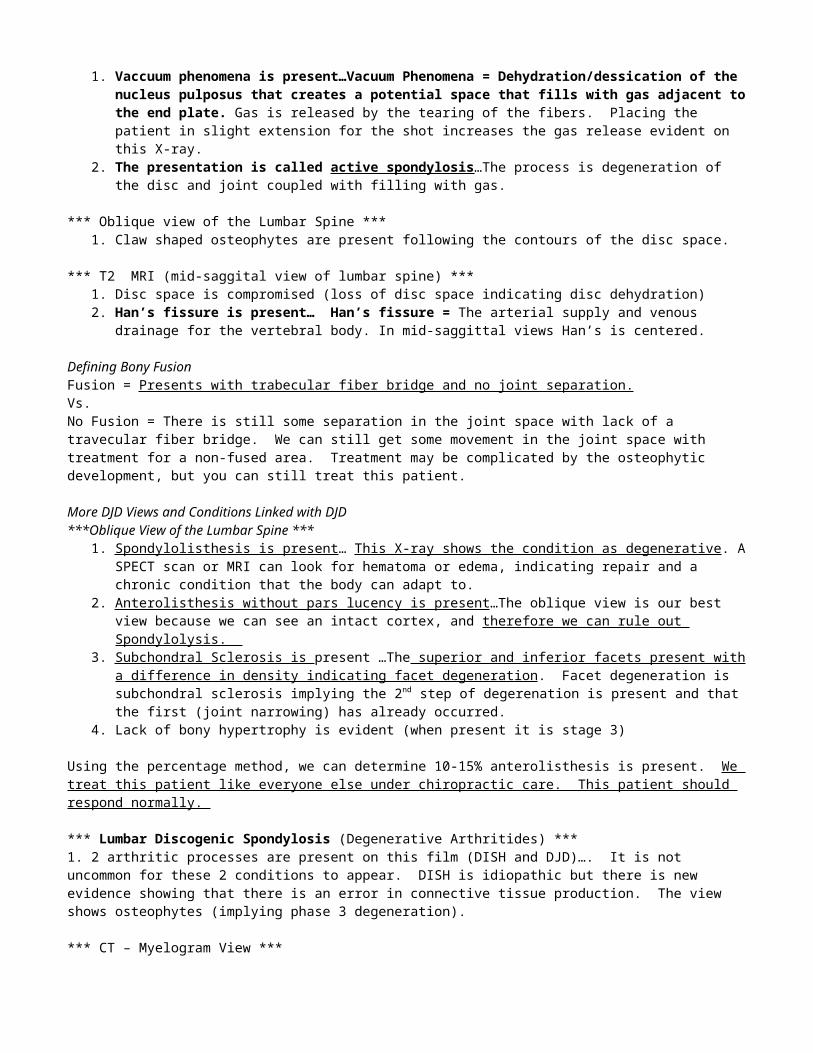
1. Vaccuum phenomena is present…Vacuum Phenomena = Dehydration/dessication of the nucleus pulposus that creates a potential space that fills with gas adjacent to the end plate. Gas is released by the tearing of the fibers. Placing the patient in slight extension for the shot increases the gas release evident on this X-ray.
2. The presentation is called active spondylosis…The process is degeneration of the disc and joint coupled with filling with gas.
*** Oblique view of the Lumbar Spine ***1. Claw shaped osteophytes are present following the contours of the disc space.
*** T2 MRI (mid-saggital view of lumbar spine) ***1. Disc space is compromised (loss of disc space indicating disc dehydration)2. Han’s fissure is present… Han’s fissure = The arterial supply and venous drainage for the vertebral body. In mid-
saggittal views Han’s is centered.
Defining Bony FusionFusion = Presents with trabecular fiber bridge and no joint separation. Vs. No Fusion = There is still some separation in the joint space with lack of a travecular fiber bridge. We can still get some movement in the joint space with treatment for a non-fused area. Treatment may be complicated by the osteophytic development, but you can still treat this patient.
More DJD Views and Conditions Linked with DJD***Oblique View of the Lumbar Spine ***
1. Spondylolisthesis is present … This X-ray shows the condition as degenerative. A SPECT scan or MRI can look for hematoma or edema, indicating repair and a chronic condition that the body can adapt to.
2. Anterolisthesis without pars lucency is present …The oblique view is our best view because we can see an intact cortex, and therefore we can rule out Spondylolysis.
3. Subchondral Sclerosis is present …The superior and inferior facets present with a difference in density indicating facet degeneration. Facet degeneration is subchondral sclerosis implying the 2nd step of degerenation is present and that the first (joint narrowing) has already occurred.
4. Lack of bony hypertrophy is evident (when present it is stage 3)
Using the percentage method, we can determine 10-15% anterolisthesis is present. We treat this patient like everyone else under chiropractic care. This patient should respond normally.
*** Lumbar Discogenic Spondylosis (Degenerative Arthritides) ***1. 2 arthritic processes are present on this film (DISH and DJD)…. It is not uncommon for these 2 conditions to appear. DISH is idiopathic but there is new evidence showing that there is an error in connective tissue production. The view shows osteophytes (implying phase 3 degeneration).
*** CT – Myelogram View ***1. Neuritis is Present…The nerve roots present differently side to side. The root is hard to visualize (poorly demarcated
and fuzzy presentation) on one side vs. the other indicating inflammation and swelling,. An inflamed, swollen nerve root gives bad demarcation indicating neuritis.
2. Osteophytes are Present … The nerve root rests up against osteophytes close to the facet. Joint capsule irritation creates inflammation that irritates the nerve root.
Adjustments, ice and other conservative care can help this person because irritation of the nerve root is a mechanical condition as demonstrated by this CT myelogram. You can think of this condition as irritated soft tissues and as chiropractors you can treat with success the irritated soft tissues. You will not see a decrease in osteophytes size with treatment, but can have success in reduction of soft tissue inflammation (the cause of the neuritis).
*** Lumbar Scoliosis ***1. Scolisios is present on this X-ray…Spine straightening is not going to occur. This X-ray and patient shows wedging of the spine due to asymmetric loading. Wolff’s laws and Volkmann’s laws apply to physiologic loading and adaptation. Loading can adapt growth causing increased or decreased growth. The goal with this patient is palliative relief or even slow the progression of the curve. This is a patient you can help to some degree, but probably won’t reverse the curve. You can teach them about pain management, ergonomic positions, and personal habits to aid in care.
*** L5 Anterolisthesis and L4 Anterolisthesis ***1. DJD is present …The facets have increased density demonstrating DJD.2. Anterolisthesis is present …Compression and Distraction views can help to identify the amount of anterolisthesis.3. Vaccum Phenomenon is present…Gas density is present in the film at the center of the disc space. The NP used to be
there. The NP was thoroughly dehydrated and/or dessicated allowing gas to fill the space.
The disc tends to be symptomatic in these patients. The joint is sloppy and stability is an issue. We have problems successfully treating these patients. We need to improve core strength, regain motion, change their lifting habits, and modify activities to decrease microtrauma to the area.
*** CT of the Same patient as above ***1. One facet is larger than the other…Asymmetric loading causes the disproportional size of one facet over the other. The joint response is hypertrophy on the side of greater facet loading.
PLL ThickeningPLL thickening is more problematic in cervical and thoracic region. Disc herniation is more common in the lumbar spine. Disc herniation presents asymmetrically vs. PLL thickening which tends to present symmetrically (especially the central PLL).
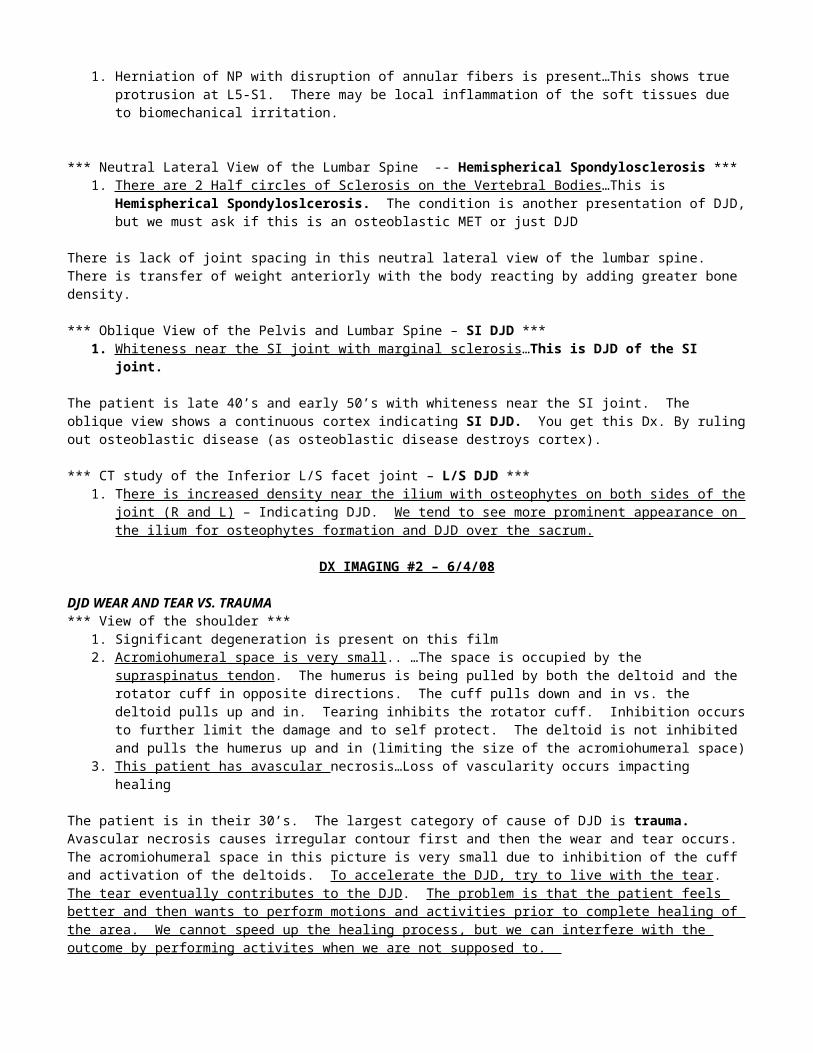
*** MRI of the Spine -- HNP ***1. Herniation of NP with disruption of annular fibers is present…This shows true protrusion at L5-S1. There may be
local inflammation of the soft tissues due to biomechanical irritation.
*** Neutral Lateral View of the Lumbar Spine -- Hemispherical Spondylosclerosis ***1. There are 2 Half circles of Sclerosis on the Vertebral Bodies …This is Hemispherical Spondyloslcerosis. The
condition is another presentation of DJD, but we must ask if this is an osteoblastic MET or just DJD
There is lack of joint spacing in this neutral lateral view of the lumbar spine. There is transfer of weight anteriorly with the body reacting by adding greater bone density.
*** Oblique View of the Pelvis and Lumbar Spine – SI DJD ***1. Whiteness near the SI joint with marginal sclerosis …This is DJD of the SI joint.
The patient is late 40’s and early 50’s with whiteness near the SI joint. The oblique view shows a continuous cortex indicating SI DJD. You get this Dx. By ruling out osteoblastic disease (as osteoblastic disease destroys cortex).
*** CT study of the Inferior L/S facet joint – L/S DJD ***1. There is increased density near the ilium with osteophytes on both sides of the joint (R and L) – Indicating DJD. We
tend to see more prominent appearance on the ilium for osteophytes formation and DJD over the sacrum.
DX IMAGING #2 – 6/4/08
DJD WEAR AND TEAR VS. TRAUMA*** View of the shoulder ***
1. Significant degeneration is present on this film2. Acromiohumeral space is very small .. …The space is occupied by the supraspinatus tendon. The humerus is being
pulled by both the deltoid and the rotator cuff in opposite directions. The cuff pulls down and in vs. the deltoid pulls up and in. Tearing inhibits the rotator cuff. Inhibition occurs to further limit the damage and to self protect. The deltoid is not inhibited and pulls the humerus up and in (limiting the size of the acromiohumeral space)
3. This patient has avascular necrosis…Loss of vascularity occurs impacting healing
The patient is in their 30’s. The largest category of cause of DJD is trauma. Avascular necrosis causes irregular contour first and then the wear and tear occurs. The acromiohumeral space in this picture is very small due to inhibition of the cuff and activation of the deltoids. To accelerate the DJD, try to live with the tear. The tear eventually contributes to the DJD. The problem is that the patient feels better and then wants to perform motions and activities prior to complete healing of the area. We cannot speed up the healing process, but we can interfere with the outcome by performing activites when we are not supposed to.
Historically, they used to unload this injury with traction casting. The casting stimulated breakdown, repair, and revascularization of cancellous bone. The problem was bony atrophy due to lack of trabecular bone formation. Bone is built through loading. Pulling on the long axis causes the joint surfaces not to touch. The bone will collapse if when loaded because the support structure was not stimulated to form during traction casting.
Proper management is incremental loading. This is loading the area slowly over time to achieve proper healing. We can follow the healing rate of avascular necrosis by MRI. The other alternative may be joint replacement; however, that option is not as good as maintaining your own joint. A good protocol would be pool exercises, exercise bike, resistance exercises with partial loading, and later on complete loading.
This patient’s age is a factor because they are in their 30’s. The cause of degeneration is not wear and tear. It takes a traumatic event to cause this type of DJD. We can treat this patient. The humerus in the superior position causes stress on the rotator cuff. Exercises, range of motion, and release of adhesions may help improve the position of the humerus and decrease the forces on the rotator cuff. Conservative care may be beneficial to avoid surgery. It may take several weeks of care to help this patient.
*** CT image of Chest – SC DJD ***1. Decreased articular cartilage over the SC Joint on one side with contour change…The diagnosis is SC DJD.
*** X-ray of the Pelvis and Hip – Hip DJD ***1. L Hip Joint Narrowing 2. Osteophytes are present…This means that the condition is in the 3rd stage (moving past the first 2 stages). The hip is a
common area of DJD. You can appreciate the continuous cortex making it an osteophyte. Osteophytes present as broad ridge that summates on X-ray to make it look smaller and more hooked.
The hip (1st) and knee (2nd) are common weight bearing joints of DJD. The ankle mortise is not as unlikely to get DJD unless there is trauma.
*** View of the Knee – DJD of the Knee ***1. Exaggerated superior pole of the patella …The patella is being tractioned.2. Dystrophic Calcification and Calcific Bursitis of the suprapatellar bursae are present … This tells us that there is
underlying change/damage and local pH change to an alkaline environment. Alkaline environments induce the calcification.
The knee is a tri-joint complex. The lateral and sunrise view give us the best view of the patello-femoral joint. We can treat this patient. A method of treatment may be ultrasound with specific cream (phonophoresis) and/or iontophoresis with acetic acid (using electric current to send a acetic acid into the body to induce an acidic environment). The patient suffered an acute injury that did not heal. Repeated microtrauma occurred causing the pH change.
*** Tunnel View of the Knee – Knee DJD ***1. Asymmetric loss of joint space is present 2. Subchondral Sclerosis is present 3. Osteophytic Development is present
There will be pain in this condition due to irritation of soft tissues and joint structures. The patient may be afraid of activity thinking it will cause pain, further contributing to osteopenia. You must separate an inflamed knee from a DJD
DISH (Degenerative Arthritide)
*** View of the Cervical Spine – DISH **DISH Overview and X-ray Pesentation
1. Calcification of the ALL is Present on X-ray
DISH (Diffuse Idiopathic Skeletal Hyperostosis). The actual condition is not painful and presents on X-ray as worse than what it actually is. The patient presented in the above X-ray has Dysphagia. The patient likely has Dysphagia due to calcification of the ALL that is described as toothpaste.
ROM would exceed what you predict with observation. They do have hypertrophic and calfcified ligaments, but have better ROM than you would expect. Dysphagia occurs in 1/5 of DISH patients.
This is a management issue. Past treatments focused on cutting out the ligament and it grew back bigger and thicker. They later tried radiation and chemotherapy and there was increased risk for cancer. We only manage this aggressively with PLL thickening because it can impose on the canal. We would do a laminectomy to increase the space in cases of PLL thickening. A simple solution to the above patient’s problem may be to chew food more, drink more water with food, and other simple management techniques (instead of surgery). The problems may be mechanical with dyspahgia. A decrease in available space due to DISH (hyperostosis) is the cultpirt for the mechanical loss of space. Mechanical advice may be best rather than aggressive treatment.
There may be a 13-40% incidence of diabetes mellitus in DISH patients. The #1 location in the spine for dish is T6-T11. #2 spot is mid C-spine. #3 spot is L3-S1.
*** View of the Thoracic Spine with DISH*** (progression of X-rays from 1988)1. Film #1 “Big White Glob on the Lower T Spine2. Film #2 (1990) – Big white glob increased in size and now crosses two adjacent vertebra with good disc space and
small osteophytic development. Small osteophytic development is present. 3. Film #3, the 1994 X-ray shows multiple levels involved with the white globs…DISH classification (Forrestier’s
Disease) requires 4 segments to be involved. In the 1994 film, it presents as crossing 4 levels. 4. Film #4, the 1998 film has more levels involved in the thoracic spine. Almost every thoracic verterba has thick
ossification evident on the X-ray.
Ligamentous hypertrophy and ossification are early signs of DISH. We really don’t understand the patho-mechanics well enough to know what to do. This is a common arthritide, that may have minimal to no detrimental affects. We have shown that chiropractors can be beneficial for palliative treatment. These patients may not cavitate as easy as others. These patients may respond a little slower vs. the DJD patients with similar presentation.
*** View of the Lumabr Spine -- Flame Shaped Syndesmophytes ***1. Flame Shaped Syndesmophites are Present – Flame Shaped Syndesomophites are present with 3 diagnoses including
DISH, Reactive Arthritis – Reiter’s, and Psoriactic Arhtritis.
The differential includes 3 for Flame Shaped Syndesmophytes 1). DISH 2). Reactive Arthritis-Reiter’s 3).Psoriatic Arthritis. Reactive Arthritis and Psoriatic Arthritis are radiographic twins. We must exclude the other 2 members of the differential.
Posriatic arthritis will present with skin lesions. If they don’t have a skin lesion with the flame shaped syndesmophyte, you can rule out psoriatic arthritis (red raised flaky lesions). Retier’s presents with conjuctivitis, ploylarticualr arthritis and urethritis. Often the 4 th feature is buboitis or ballinitis. This is inflammation of the glans penis in the male body. The description is can’t see, can’t pee and can’t dance with me. Can’t dance with me is polyarticular arthritis, osteophytes on the calcaneus ( Lover’s Heel) , and fluid filled pustules on their feet or palm of their hands (you don’t want to dance on pustules, they’ll break)
DISH does not share the other features. The only feature it shares with the other members of the differential is the flame shaped vertebra. Don’t assume it DISH first, because you’ll leave 2 inflammatory arthritides in the differential that my cause more harm than DISH.
*** View of the C-spine ***1. Thick ALL Calcification (atypical DISH) …This is DISH. The disc is good with thick ALL ossification present. 2. Decreased joint space and subchondral sclerosis is persent…DJD
This X-ray shows DISH coupled with DJD.
Study Guide Definitions

Bony Outgrowths of the Spine – Paravertebral OssificationOssification of the paravertebral connective tissue which is separated from the edge of the vertebral body and disc. The osteophytes are large, coarse and asymmetrical.
1. Reiter’s 2. Psoriatic ….Both arthritides are C shaped/comma shaped, stuck on and non-marginal.
Claw OsteophytesArising from the vertebral margin with no gap and having an obvious claw appearance. Claw osteophytes are a stress response, but in the absence of disc space narrowing does not indicate disc degeneration.Undulating Anterior OssificationUndulating ossification of the ALL, intervertebral disc and paravertebral connective tissue (flowing exuberant ossification of the ALL or PLL). This ossification indicates DISH.
SyndesmophytesOssification of the annulus fibrosus that is thin and symmetrical. Syndesmophytes, when extreme, results in the “bamboo spine.” 1. AS 2. Alkaptonuria...Both of these should be in the differential. (Alkaptonuria is the twin of AS in enteropathic arthritis).
DX IMAGING #2 – 6/9/08
*** Picture of the T-Spine…DISH ***1. Exuberant calcification of the ALL is presen t
There may be a 13-40% incidence of diabetes in DISH patients. We know there is a relationship, but we don’t know the extent of the relationship between DISH and diabetes. The cause of DISH is idiopathic. Human antigen #8 is elevated in DISH. PLL thickening is much more devastating than ALL because it can impact the cord. The C-spine and L-spine are the most common location for PLL thickening.
*** View of the Lumbar Spine…DISH, DJD and Discogenic Spondylosis *** 1. L4-L5 Level -- Discogenic Spondylosis (DJD of the disc joint)2. Superior L-Spine (L1-L3) – Early DISH
We can still manage this condition with conservative care.
*** View of the L Spine ***1. Flame Shaped Syndesmophutes -- This brings up 3 choices. The patient actually has DISH. Flame shaped is the key
sign here indicating DISH. There is normal disc space present.2. End Plate Fracture -- Upper L-spine end plate fracture. The picture shows a wedge shaped fracture from compression.3. Check Sign -- This suggest bone pathology at the root of the vertebra. 4. DJD Arthritis – Lower L Spine
This patient has DISH from the mid-thoracic spine down. The DISH crossed into the upper lumbar area from the thoracic spine. In the lower spine, there is DJD arthritis. This patient also had a compression fracture in the T-L junction. This injury could be due quick folding of the patient approximating the end plates causing the compression fracture. This may occur in automobile accidents, falls, and other trauma.
*** Upper thoracic and Lower Cervical Spine X-ray ***1. 1 st Costotransverse Ligament Calcification -- This is a common site of increased bone density and tufting.
Calcification indicates DISH. The iliac crest and ischial tuberosity are also a common location for calcification.
*** Thoracic Spine View – DISH ***1. Flowing Exuberant Calcification is Present – Flowing Exuberant Calcification indicates DISH.
Pencil thin line vs. Flowing exuberant -- Flowing exuberant is DISH vs. Pencil Thin (AS). The only examples of pencil thin are AS and EA. Enteropathic arthritis includes bowel diseases like Crohn’s or Whipples that develop spinal arthropathy.
*** MRI of the C spine ***
1. PLL thickening at multiple levels -- Ligaments are typically black on MRI and when ossified they become more black. Ossification of the PLL on both T1 and T2 show up as increased darkness. PLL ossification can intrude on the dural sleeves and generate diffuse low back pain.
*** CT scan of the C-Spine ***1. Central Canal Stenosis --There is PLL ossification that contacts the cord and narrows the canal. The patient does not yet show neurological signs indicating a long standing process that the body can adapt to functionally.
*** Chest Film ***1. Wavy and undulating pattern -- Common in DISH. It is not exclusive to dish, but common to DISH. The ligamentous structures of the vertebral bodies are involved often in addition to ALL and PLL.
EROSIVE OSTEOARTHRITIS (Degenerative Arthritide)EOA DescriptionEOA presents similar to RA. Some Differentiation:
1. Bilateral Condition that can be symmetric or asymmetric2. Swelling of the digits and rays3. EOA often involves the DIP’s (RA does not usually involve the DIP’’s)4. Called “Hand Disease”5. Gull-Wing Deformity – Up and down sweeps of the digits and rays.6. No involvement of Rheumatoid or C-Reactice Protein in EOA.
*** Teacup view of the hand and fingers ***1. The 1st metacarpal-carpal joint space is decreased in the R hand2. Osteophyte on the R trapezium -- DJD in a joint that normally shouldn’t get DJD. 3. Opposite of L hand Decreased Joint Space at the 1st MCP-Carpal Joint.-- This is EOA.
The L hand or second radiograph presented is worse when looking at the film, but the patient notes pain in the R hand more. A key question is to ask what they do for a living and what their hobbies are. If they don’t have history of use or trauma, it is not DJD-OA. A bilateral presentation indicates EOA. The most frequent joint involved with EOA is DP. Another joint classic but less involved is the 1 st metacarpal-carpal joint.
DX IMAGING #2 – 6/11/08
RA (Inflammatory Arthritide)Table 10.24 Diagnostic Criteria for Rheumatoid ARhtritisPhysical
1. Morning Stiffness2. Pain on motion or tenderness in at least one joint3. Soft tissue swelling or joint effusion in at least one joint4. Swelling of at least one other joint (within 3 months)5. Bilateral, symmetrical, and simultaneous joint swelling (except DIP joints).6. Subcutatnoue nodules, -- boney protuberances (extensor surfaces, juxtaarticular).
Laboratory7. Positive sheep agglutination test (rheumatoid factor): We take antibodies from sheep and put them in patient’s
blood and look for clumping (indicating high levels of rheumatoid factor)…Be careful because rheumatoid factor is in many conditions including arthritis, mixed arthritis, and connective tissue disorders. If you see a + test, there is a strong indication of RA, if not, it may still be RA, but may require additional methods of testing.
8. Poor mucin precipitate from synovial fluid.—Joint aspiration is done to get synovial fluid. This is an aggressive, invasive test. The synovial fluid is lubrication. As a consequence, the patient may feel very stiff afterwards.
9. Synovium – at least three of the following (to get this they need to open the joint capsule and scrape from the capsule) a. Marked villous hypertrophyb. Superficial synovial cell proliferationc. Marked inflammatory cell infiltrate with fibrin depositiond. Foci of cell necrosis
10. Nodules – Granulomas with central necrosis, proliferated fixed cells, and peripheral fibrosis …They find a nodule/bump cut it out and send it to the lab to test.

11. Typical changes – uniform joint space loss, marginal erosions, etc….These are radiographic findings. Inflammatory arthritis is linked with pannus tissue. Pannus tissue pushes on soft tissue and on bone (causing pressure erosion). It tends to start in the soft, bare areas of the joint, where the articular cartilage ends and the periosteal tissue begins.
ClassificationClassic: Greater than 7 criteria (with swelling for greater than 6 months)Definite: Greater than 5 criteria (with continuous joint symptoms greater than 6 weeks)Probable: Greater than 3 criteria (with continuous joint symptoms) (4-6 weeks)Possible: At least two of stiffness, pain, swelling nodules, elevated ESR or CRP, or iritis with joint symptoms for at least 3 weeks.
*** Diagram of RA Joint with progression ***1. Synovial Proliferation in Soft Tissues Adjacent to Joint Space (Early Pathological Change)2. Pannus Growth invading bony areas3. Pressure Erosion of Bone with Osteoclastic cleaning of the area4. Ankylosis (only present with inflammatory arthritides like RA and psoriatic arthritis)
Table 10.6 Pathologic Radiologic Correlation in Rheumatoid ArthritisPathologic Features1. Synovial edema and effusion. 2. Rheumatoid nodule 3. Cartilage destruction by pannus 4. Pannus eroding in the “bare area” 5. Intraosseus pannus and synovial fluid intrusions 6. Inflammatory hyperemia 7. Periostitis 8. Fibrous Tissue Metaplasia 9. Capsule and ligamentous, laxity, tendon rupture
Radiologic Features1. Periarticular soft tissue swelling 2. Subcutaneous soft tissue mass 3. Uniform loss of joint space 4. Marginal Erosion 5.. Subchondral bone cysts 6. Juxtaarticualr osteoporosis 7. Juxtarticular periosteal new bone (linear) 8. Ankylosis 9. Deformity *** Know the above charts ***
DefinitionsHyperemia = Flowing blood that washes away bone. Usually the blood comes from circumflex arteries that can bleed and wash away bone. Fibrous tissue metaplasia: Loss of joint space by growth of fibrous tissueCapsule and ligamentous laxity with Tendon rupture: Deformity of the capsule, ligaments and tendon occur with RA. The structures deform and do not go back into normal alignemtn. The goal of treatemtn is to maintain function and lessen the chance for progression.
*** Picture of the PA Hand and Oblique Hand ***1. Soft tissue density is different between some of the metacarplas and phalanges – The patient has an implant in the
joint space due to the harmful effects of RA. 2. Ulnar deviation of the hand is present

*** Bilateral Hands on the Film ***1. Involvement of the Carpals and MCP --- Classically the MCP and carpals are affected. The carpals no longer show
the 8 bones. 2. Carpal coalition (ankylosis of the carpals) -- This is a congealed mass of bone with loss of joint space. Carpal
coalition is an early feature of RA. The index finger is primary target of RA and middle MCP joint.
*** View of the R Hand ***1. Indentation/Granulation Tissue on the Scaphoid -- This is an early sign of RA.
We need to manage the condition between excacerbations. As chiropractors we can change their diet and give them activities for mobility. We need to keep the joint moving to give them the best chance for long term success.
*** Another view of the hand ***1. The 1 st MCP joint space is decreasing 2. The Metacarpal head intrudes into the base of the phalanx – PENCIL IN A CUP APPEARANCE occurs at the base of the phalanx and the head of the metacarpal.
*** View of the Upper C-spine *** Increased ADI with RA -- Growth of pannus tissue affects the ADI.
1/5th of all patient’s with RA develop an increased ADI. If they have hand pain, headaches and have RA, you must get flexion and extension cervical films to document stability. In the presence of significant RA disease, obtain films every 6 months to a year as a good recommendation to check ADI. We should recognize that the patient’s cord may be in danger. Regardless of treatment choice, we need to document stability for the patient’s own good. We may need to consult a spine surgeon if instability is present that could compromise the cord.
Another common set of circumstances is that the suboccipital muscles tighten. The muscles are not designed to hold C1-C2 and therefore fatigue triggering pain and headaches. .
*** Neutral lateral Film of the C-spine, Flexion View and Extension View ***1. Increased ADI -- The patient gaps further in a flexed view. The patient gets back to normal with extension. This is a startling finding, meaning that the motion is so increased that the transverse ligament is compromised but still holding. This person may be catastrophic injury away from quadriplegia. There is urgency in this situation to see a surgeon.
*** View of the lateral C-Spine ***Increased distance of the ADI -- In this patient, the only thing keeping C1 from going far forward is the cord. In this
patient, you won’t need a flexion film, because the gap is so pronounced it may cause problems.
This patient has Le Hermitte’s sign upon physical presentation. They have shocks going down both arms. Think central canal stenosis right off the bat. Le Hermitte’s sign is associated with central canal stenosis and increased ADI.
*** MRI of the same patient as above ***Posterior Tubercle is touching the cordPannus tissue in the ADI space with increased space -- When the ADI is that big, the only thing keeping the post. Tubercle
in check is the cord There is not much left of the odontoid space.
*** AP View of the Pelvis with RA **Bilateral Symmetrical Decreased Joint Space – The condition causes Protrusio Acetabuli (bilaterally). We base our
diagnosis of RA with checking both joint spaces. Since both joint spaces are gone, we can confidently say bilateral, symmetric presentation and RA.
Disuse Osteoporosis – Lack of bone density due to disuse. The patient experiences pain with activity and cannot be active to stimulate bone development. They are at risk for disuse osteoporosis.
Fracture/Discontinous Cortex at the Femoral Acetabular Joint – The discontinous cortex indicates a fracture. The bone has failed because of protrusio acetabuli. RA and disuse osteoporosis have contributed to the fracture. The patient may need a hip replacement to help with pain and restore some function.
*** View of both knees ***Bilateral, symmetrical presentation of medial and lateral joint space narrowing -- There is such loss of joint space
narrowing, that the tibial spines are almost rounded over. Pan compartment, bilateral symmetrical joint space narrowing indicates RA.
Bad bone density – Typically, there is 40% cortical and 60% trabecular bone. In RA patients, we see more trabecular fibers (80%) and less cortical (20%).
Periarticular Osteoporosis -- Disuse osteoporosis, coupled with hyperemia lead to decreased density of bone.
*** Athrogram of the Lateral View of the Knee ***1. Baker’s Cyst -- Contrast has leaked into a new chamber in the popliteal fossa indicating Baker’s Cyst. Baker’s cyst
is commonly seen in RA and described as a golf ball like lesion with pain. It is a tear in the capsule that allows protrusion of the synovial lining. Contrast has filled the Baker’s cyst due to defect in the capsule. The cyst can be disabling and require draining of synovial fluid. These conditions may be surgical if the person has lost significant function.
*** View of the chest ***1. Lung Bases Appear More Dense -- Interstitial Fibrosus…RA is a systemic process involving multiple systems, including the lungs. In this view, the lungs show fibrosus. Fibrosus is the result of RA that can cause hardening of the lungs and joints. The fibrosus, if uncontrolled, can lead to respiratory problems and death.
JUVENILE RA (Inflammatory Arthritide)*** Picture of a Juvenile RA case ***
1. Irregular Contour of the Surface of the Humerus2. An osteophyte is present
This patient is 35 years old. We don’t expect this patient to have DJD (wrong category and age demographic). So, upon taking a history we found that the patient had Juvenile RA with secondary DJD.
DX. IMAGING #2 – 6/16/08
*** C-Spine Picture Overhead ***1. Posterior Elements all appear as 1 -- It is difficult to determine individual levels in the view.2. Lack of Recognizable Facet Joints, Anomalous IVF’s, and Posterior Elements appearing as one (Ankylosis), Short AP
Dimension with Tall Height Vertically-- The bodies of the vertebra don’t mature properly.
This patient has juvenile arthritis. They have the sero + form. The sero + category shows the most involvement in the spine. Inflammatory arthritides produce ankylosis and premature maturation. Premature maturation involves a growth plate that has closed.
Hyperemia stimulates a variety of tissues including provoking closure of the growth plate. We see a vertebra trapped as the posterior elements couldn’t migrate. This patient is at risk for ADI instability. We need some flexion and extension films to document stability in the best interest of the patient.
*** View of B Feet…STILL’S DIEASE ***Still’s Disease is sero negative arthritis. The patient in the above film has bilateral, asymmetrical RA and they are younger than 20. They have Junvenile RA. Generally speaking, Still’s patients have less involvement than other patients with inflammatory arthritides. The #1 sero negative form of RA is Still’s Disease. Still’s Disease is idiopathic. Some patients benefit from presception drugs to treat this condition. There are also people that don’t do well with the drugs and drug protocols. A dietary change to a less inflammatory diet can help this patient
*** Lateral View of the C-Spine *** 1. Calcified Soft tissues 2. United Posterior Elementes 3. Anomalous IVF ( due to incomplete migration of pedicles).
4. Disc space whiteness (calcification) 5. Underdeveloped Mandible (not at the correct angle) with Underdeveloped maxilla --
Still’s like all other RA is a systemic condition.
*** View of the Wrist and Hands ***1. Severe degeneration of the hands is present -- 2. You cannot discriminate the 8 carpals . 3. Pencil in a cup appearance -- Metacarpal head destroyed (pencil), with deepend end of the phalanx (cup). The
pencil in a cup appearance takes a long time to present (chronic severe degeneration into a deformity over time)
They had onset of RA (inflammatory arthritis) since they were a child. This is a juvenile chronic arthritis condition (JCA). This is definitely a sero + till proven otherwise. If you do get a – test, repeat the test. The test may have failed, rather than it not being sero +. ANKYLOSING SPONDYLITIS (Inflammatory Arthritide)Description and View of the Spine*** View of the Spine – Railroad Track Sign***
1. Vertically Oriented white lines running down the lumbar spine – RAILROAD TRACK SIGN. Railroad track sign involves ossification of ligamentous structures with pencil thin margins in the upper lumbar spine spine.
2. We also do not see the SI joints – AS affects both SI joints and can induce bony fusion.
AS is an inflammatory arthritide that restricts motion. AS patients have disuse osteoporosis of the vertebra. They carry loads on the outside because ossification of soft tissue and they will lose internal bone as support. There will be thinning of the end plates over time.
SI may present as a “ghost joint.” The anterior and posterior interosseus ligaments have ossified and masked visualization. You need to do a specialty study increasing KVP to view the SI joints to somewhat improve visualization. Taking a CT scan of this patient will be more beneficial than a plain film study for SI joints.
*** Another view of the L-spine and SI joints – Dagger Sign & Carrot Fracture***1. Interspinous ligament and supraspinous ligament calcification .-- Dagger Sign is present. Dagger sign involves lack
of joint spacing with pencil thin ossification of the interspinous and supraspinous ligaments between both joint surfaces.
2. Decreased Bone Density and Disuse Osteoporosis -- This is a patient with too little bone density (disuse osteoporosis due to their inflammatory condition.
3. Carrot Fracture – A horizontally oriented fracture of the spine into the disc space.
Women and men get AS (ankylosing spondylitis) at the same rate.
*** Lateral View of Lumbar spine ***1. Dystrophic calcification of the disc space in the upper lumbar spine
***Another view of Lumbar Spine ***1. Density of the disc space is greater than bone is this X-ray -- AS is a frequent producer of disk space calcification. Syndesmophytes (calcification of outer annular fibers) causes thining. The syndesmophytes run from joint margin to joint margin. The syndesmophytes carry the weight of the body. We are lose the ability to exchange nutrients by imbibition.
*** PA view of Lumbar Spine – Bilateral Sacral Ilitis ***1. Bilateral Sacral Ilitis -- This is an inflammatory process of the sacrum and ilia (SI joints) that can produce bony
fusion of the SI joints.
Review of AS Findings1. Railroad Track Sign – Ossification of the Ligamentous strctures with pencil thin margins2. SI as a “Ghost Joint – SI Jiont fusion from interosseus ligament ossification that makes visualization difficult3. Dagger sign – Lack of Joint Spacing with pencil thin ossification ofhe interspinous and suprspinous ligaments4. Disuse Osteoporosis5. Carrot Fracture – Horizontal fracture of the spine running into the disc space6. Syndesmophutes – Calcification of the annular fibers as a response to stress. The syndesmophytes now bear weight.7. Bilateral Sacral Ilitis – Inflammation of the SI joints than can lead to bony fusion

Dx. Imaging #2 – 6/23/08
Table 10.53 Differential Diagnoisis of Psoriatic Arthritis*** Study and Know the Table ***All inflammatory arthropathies can give transitory widening. Ankylosis: AS presents with the most ankylosisSoft Tissue Swelling: More common in RA (++), also common in Psoriatic (+) and Reiter’s (+)ESR = Psoriatic +, Reiter’s ++, RA +++, AS +++…ESR levels are up indicates inflammatory stage and if they are down it indicates minimal to no inflammatory processRheumatoid Factor = RA +++HLA 27 = AS (90% have elevation of this) – Most common found with SI joint problems. RA affects the SI joints infrequently; however, AS typically affects the SI joints. Reiter’s shows 75% chance for HLA 27. Psoriasis shows 60% HLA 27. CALCIFIC TENDONITIS (Inflammatory Arthritide)*** Bilateral Feet on the Screen ***
1. Calcification of the Peroneus Brevies tendon proximal to the styloid of the 5th metatarsal – There is a cortical margin with trabecular interior, indicating bony formation.
This patient suffered several inversion injuries to the ankle. The injuries produced an environment of alkaline pH change allowing calcium to precipitate in this environment. Tendon calcification is called calcific tendonitis. There is a higher rate of spontaneous rupture in calcific tendonitis.For example, cortisone injections cause pH changes that can lead to rupture (ex., spontaneous rupture in athletes due to pH changes from cortisone).
Calcific tendonitis has repeated history of trauma to the area. The area is painful to palpation. You can treat the area with underwater ultrasound, iontophoresis and acupuncture. The medication used for iontophoresis is weak acids like salicylic acid or acetic acid.
*** Picture of the AC joint ***1. Rotator Cuff Calcification is present -- The rotator cuff is a common site for dystrophic calcification (particularly the
supraspinatus tendon). The sharpey fiber attachment site is supplied by the circumflex arteries. The belly and tendon are supplied by another vessel. There is a critical zone with very little blood supply. Overhead sports wrings out the tendon and causes repeated microtrauma leading to dystrophic calcification.
METABOLIC ARTHRITIDES Gout*** Picture of the Ear – Not an X-ray ***1. Growth off the top of the ear with shiny white areas -- Tophi in the ear. The tophi are very tender. Squeezing it will cause crackles. The most common location for gout/tophi is the great toe.
*** Picture of bilateral feet – Overhang Sign***1. Overhang Sign is Present – This is joint line hanging/deposition of crystals. The overhang sign in this film is at the
1st Metatarsal Joint. Metabolic arthritides take a long time to show up on plain film. Often a lot of damage occurs before they appear on plain film
DX. IMAGING #2 – 6/25/08
*** Bilateral Feet…Gout is present. It is a metabolic arthritide. We have a crystal we are worried about, uric acid. This is an aberration of the purine pathway with too much circulating uric acid. This is a transient process. They have excess levels of uric acid in the bloodd exceeding the bility to excrete by the kidneys and depositing the crystals all over the body. There are periods of exccerbation and relaxation. The foot is a common area because blood supply slows distally at the end of the system and the crystals can be deposited. Wherever blood flows, uric acid can go. In this X-ray, the lesions at the great toe is a classic sign with the overhang lesion. A hallmark feature of metabllic arthriedes is that for quite somet time they leavle joint space and bone density alone. At the distal end of the 5th metatarsal, crystal depostis are made, some edema is present, and some swelling is present. The vasculature has been impacted at the 5th metatarsal. ***
*** Another picture of Bilateral Feet…The L foot and great toe appears gouged out. Superimposed on the anatomy should be 2 sesamoid bones. This is called the overhang sign, resulting from a break in - pattern of destruction. Another classic sign, is soft tissue swelling over the great toe. You check the aposing joint surface and . This patient is very red and swollen
over the great toe. 2 classic break in patterns present, prominent soft tissue swelling present. A biopsy of soft tissue will find UA crystals, but the blodd has transient rise and fall of uric acid based on kidney function. IN gout patients, the kidney’s get behind and can’t keep up leading to uric acid distribution. ***
*** Picture of Bilateral Hands…There is calcification of sfot tissue. 3 (physioligcal, dystrophic, metastatic)…Dystrophic calcification is present. UA crystals are invisible on plain film. Uric acid does the dmage leading to local pH change and depositioing of crystals/calcification. Tophaceous gout is present. Tophaceous gout. At the thumb, there is a calcification presne.t ***
*** Picture of the great toe…The classic joint is the metatarsal-phalangelal joint and in the hand metacarpal-phalangeal joint. This has to do with caliber of vessesl with the vessel abile to dump of uric acid. The dystrophic pattern is based on damage. Damage causes local pH change and calcium deposition. There is big soft tissue swelling present in the great toe. A bad effect of the Atkin’s diet was the creation of nitrogenous wastes without the ability to clear the waste leading to “gout like symptoms.”
*** Picture of the Proximal Tib-Fib Joint…***
*** CT scan of the Knee – There is a lucency in the tibia…The rim looks sclerotic. Bone is a slow adapter to stress. The lucency has been here for awhile. This eliminates the concept of aggressive processes. This uric acid crystals in a granulation tissue. This is intraosseous gout. Wherever blood flows, UA crystals can go. Sometimes they can preceptiate. Blood flow through bone is slow, ”swamp like.” The fix is often surgery, digging out the crystal deposition. ***
Pseudo-Gout (CPPD)The poster child for the metabolic category. This is a crystal that usually doesn’t produce bone change. The key to the finding is to look at the soft tissues of the joint space. The joint space should be black on plain film. In this picture of the knee joint the joint space is not very black indicating decreased joint space. There is a white stripe in the jont space. The white space is indicateive of crystal deposition. Classic, is decrased joint space with white stripe in the middle. Chondrocalcinosis is present and CPPD until proven otherwise (most common for older patient with knee pain with decrased joint space and chondrocalcinosis).
*** Pictuer of the Shld…The joint space is decreased between the glenoid and the humerus. Thiere is something laying on the bone as it leads to the joint space. There is calcification f the articular cartilage and possible thickening of the labrum. ***
***Picture of the Shld…There is small calcification of the humerus…This is articular cartilage calcification. Chondrla tissue follows the bone vs. calcific tendonitis that does not follow the bone structure and presents above the involved structure. ***
*** Picture of the Ear…There is increased pigementation in the cheek and a “ditry ear.” This is Homogenticic Acid deptiosn. When the acid oxidizes, it turns black. When it accumulates, the person is missing an enzyme. This is homogenticic acid oxidase. Alcaptneuria or ocranosis are the most common names. The patient never had the ability to produce the enzume and have been accuummulating this over a lifetime. On a daily basis, we don’t produce much. Overtime the accumulation becomes pathologic (ex. Over 30 eyars). ***
*** AP view of Lumbar Spine…The patient looks old but is 32 years old. This pattern does not fit the DJD category because it is too many levels. The differential is DJD in the wrong age and distribution (but it isnn’t), so it must be something else like ocranosis or alcaptneuria. This patient complains of lots of back pain. This pain is often written off. The urinary system spills the acid. Pee in a cup and have the urine sit there and it will turn balck. The air-fluid interface induces oxygen and causes the change to black. Homogentisic acid will turn black the longer it is exposed to oxygen. ***
*** Ocranosis/Alcaptonuria…Picture of the Spine with multiple level involvement…There is not pendil thin syndesmophutes, so no evidence of AS. The patient is young (mid 30’s) and not the right age for AS. This is wrong age and distribution for DJD. There are no osteophytes or bone change. ***
Osteoitis Condensis Ilia (OCI)** Picture of Both ilium and sacrum…The hallmark feature is multiple full term pregnancies. The ratio is over 10:1 for females as compared to males. CT studies show some thicking on the sacrum, but more pronounced on the ilium The sacrum is already a dense bony structure and is able to distribute the weight. The iliac part of the joint (Si joint)¸shows the sign of increased stess as it is not designed to bear the load. Elastase, relaxin, and other hormones peak just before child before and allow childbirth. It takes time to return them to normal. Then another short spian and pregnancy and the levels can’t get back

to normal. Over time the ligaments stiffen and the joint moves less. The increased bone may retreat. As the ligaments become more capable and joint movement lessens, the distribution of weight becomes more typical. Also, there is weight loss flowing the pregnancy (typically) and the stresses decrease leading to OCI bone formation decreasing. This is a mechanical stress response. It is found in the SI joint. It is not crystal deposition, not inflammatory, not degenerative, and is a special case. We don’t’ find fibriatlltion of the aritcualr surface. This is a miscellaneous category of pathology. It is an arthritide but is separate/miscellenous ***
*** Another Case of OCI…This person had several full term pregnancy. They don’t have to be vaginal delieveries because the vagina and pelvis have already received hormones to help with delivery. You need to still check for AS (ankylosing spondylitis since the pattern is differnte with females). ***
*** another pricture of OCI…The condition is present on both sides. This is due mechanical steres through Shrapey fibers to liamentous attachments ***
*** Picture of the Tib-Fib…We are looking at the cortico-medullary junction…We see periosteum on the film, and we shouldn’t see it as it should be black. This is a solid periosteal density. This is a patient in their history has bronchogenic carcinoma, with lobectomy. The patient has decreased ability of the remaning lung to exchange oxygen and CO2. The extremities are very sensitive to hypoxia. Our vasomotor system shunts blood to the interior over the exterior. This is a survival mehcniasm. This is chronic hypoxia that changes local pH at the periostem. The periosteum lays down near bone. This HPOA (hypertrophic pulmonary osteoarthrophaty). This is lung disease that set this condition for the reaction. Kids can also demonstrate HPOA. Kids get this because of a primary bone condition like Ewing’s sarcoma or osteosarcoma that sends metastasis to the lungs. The lung is a common site for bone mestastatis. The periphery becomes hypoxic and the periosteal irritation summates. You need systemic hypoxia. Some other conditions that cause this are emphysema.
*** Another picture of HPOA... in the Chest film…The picture also shows lung cancer ***
*** Pictuer of Clubbed Fingers…Clubbed fingers can occur with HPOA ***]
*** Miscelannous diseases…There is a picture of a lady with shinny areas at the fignertips that is truncated and retracted. The patient can have scleroderma. This is connective tissue that shrkins restricting the capillary bed and blood flow to and from the capillary. Truncated pattern is a narrow. There is squeezing of the blood vessel and we lose the distal phalanx. The situation is acroosteolysis. Acroosteolysis is the breaking or loss of the distal parts of the body. ***
*** X-ray of the Fingers…There is truncated appearance and narrowing. This person has scleroderma ***
SLE*** SLE changes soft tissues and not bone. The hands of an SLE person may look deviated. Radiograph of that patient and they will be able to put their hand flat on the film. This is called reversible subluxation, where the appearance physically is different than that radiographically. The reversible subluxation is classic. ***
*** Pictuer of the wrist and hand…There is a lucent area over the styloid of the ulna. There is a break in pattern (break in is common to gout). That is our radiographic though…this was a case of gout ***
*** Picture of the first metacrpala…There is a break in pattern (the best feature for break in pattern is. The white line is the interface between bone and pannus tissue. An aggressive pattern to break cortex leaves ragged trabecular bone. Break in the body tries to resist (slow steady push and the body can mount a response) vs breaking out (it has violated the cortex). The white line is the body’s reaction to the pressure. This is a break in pattern. Break out incluces infection and tumors ***
*** Pcicture of bilateral hands ***
*** Pictures of hand ***
*** The Right Hip joint is polka-dotted…This many be a sclerosing dysplasia (osteopoikylocis). Osteopoikylosis is a though, but it is outside the bone (a sclerosing dyspalsia of bone. THIS IS INTRACAPSULAR, EXTRACORTICAL PROCESS CALLED SYNOVIOCHONDRO METAPLASIA. Somtiems you see this with a fabella. Multiple joint mice indicates synoviochondrometaplasia. There is ossification in the synovial fluid with multiple joint mice. This is a primary condition where the genetic code is such that there is overprolifeation with ossification. These patients almost always have
problems of joint locking and they can’t straighten up. Jiont locking is common for joint mice, but with this mangintude it creates a great opportunity for this. JIOnt mice is not often a surgical condition. The surgery to fix this is worse than the dealing with the locking (minor annoyance) ***
*** another picture of the above condtion…pctire of the knee…It is intracapsular but extracortical…Priamry is synoviochondrometaplasia.***
*** Another picture of same condition of the knee…The joint mice have affected the jont capsule. Synoviochondrometaplasia is present in the joint capsuelf of the knee…This patient aslso has calcification of the suprapatellar burseae ***
*** Tunnel View of the Knee…Usually the best view to see joint mice of the knee. ***
*** Shoulder Tomogram…The image appears streaky because of dystrophic clacification of the glenoid labru. The labrum is caldifiec due to repeat tramatic events. B***
*** A picture of the Sholder…Dystrophic Calcificaiton of the Surpaspinatus ***
*** Distal Femur X-ray…In the interior of the bone there is an area of lucency. Lateral X-ray of Same patient…There is a break out pattern and some missing cortex. This is a young patient. PIGMENTED VILLONODULAR SYNOVITIS…The villus tissue should filter blood to produce snovoal fluid hypertrophies. It attacts hemosiderin and gives it a dark look. Pigemented Villonodular synovites. Pressure erodes bone. Thisi s a break in pattern ***
DX. IMAGING #2 – 6/30/08
Case Examples:1.DISH
Usually greater 50 years of ageCalcification and ossification of ALLCriteria for DISH
4 contiguous levelsPreservation of disc spaceAbsence of apophyseal ankylosis
Extraspinal enthesophatyMay have OPLL
Exuberant Hyperostosis..There can be ossifcaiton of the ALL and/or PLL
2. RAUsually 20-50 eyars of ageInfalmamtory arthritis of synovial articulationsHallmoark = bilateral and symmetric
Uniform joint space narrowingMarginal erosisionsDeformitiesADI instability (greater than 3 mm in adults)Protursion AcetabluOsteopeniaRTC tears
Pannus formation can erode tranversie ligament. Cranial Settling can occur decreasing cord space
3. DJD of C/SIVD naorrowingSubchondrla sclerosisUncovertebral and
Unvoveertberal joints can hypertohpy and scleross. A mock band is not a fracture but is sclerosis (unoverbreal osteoarthroiss). The IVF anc b enarrowed.Apophysieal joints arthroiss can be present.
4. Juevenile Rheuamatoid ARhtiries
ADI isntbailitApophysieal anklylosisHypoplasia of veretreal bodies and disascsOsteoporosis
5.Ossiciafcaiton of PLL: can compromise cord space
6.ASDecrased lordosis and anterior head carriageMarginal synsdepmphteysApophysial ankylosisADI instabilityOsteoporosisDisuse atrophy in chornic casesSpinous process erosionsCarroti stick pathologic fractures
7.Infectious discitisWidened retropharyngeal and retortracheal soft tissuesCortical destructionIVD narrowing
6.ASMarignal SyndesmophyteBamboo spine Trolley Track Sign IVD calcificationDagger Sign (ossification os SS and IS ligamets)
7.REithersMale to females is 50:1Classic triad (Can’t see, pee or dance with me)
Lover’sheelNonmarginal sysndesmplhtesBilteral Symmetric
10. Apophysieal Jiont ArhtorsisiIncrease the pedicle facte angle and cause degerneartve spondylolysthiese -- Non spondylolytic spondylolisthesis
11.Discogenic spondyloissOn one side predominatly
12.ASBilateral SI ankylosis (a hallmoark for AS)…starts in the SI and fuses them…The next site is the TL junction…Non-
marginal syndesmophytes…Dagger sign, Trolley track sign
13.Psoriatic ArhtitisAge 20-50, males = femlesPsoriatic skin lesions commonPressnec of nail changes seen in 8-%of arhtitis patientsAffected areas
Si jointsBilteral
“Sausage” digit deformity
14.RABilaterand Symmetrical, Ulnar deviation of figners, Flexin of PIP an dExtension of DP (Boutinneir’es)…Unirgogrm
joint space narrowing,
15.Psoriatic ArhtitisFusinform swelling, Tappering of middle phalanx compared to distal pahalnx (Pendip in cup deformiety)
16. GoutDisorder of puring metaboilismMale:F 20:1Usually 4th or 5th decadeHyperuricemiaComon sites
Foot1st MTP joint
Hand17. Scleroderma
Sof titususe cange: tapedred conical finertips, rtratciotnof fignerip, soft ftissue calicifationBone changes: repsirtion of distal tuts AKA acor-ostellyeisJionts normal
Soft tissue calcification is seen. Soft tissue distal to tufts is resorder
18. SynoviochonndrometaplasiaBening arhtorphaty characterizied formation of intracticlarlloose bodiesThird to fifth decases70% involves
19. Neuropathit ArhtopahtyDebirs, density, Destruction, Dislocation, Disorganization, Distenstion (6 D’s)
20. Pigmented Villnoduelar SynovitisUncommon inflammatory lesion of the synovial tissue liningn the jointsYoung to middle aged adults Male greate thanfemaleMonoartiulcar Radiographic findings
Dense lobulated masses and effusion“apple core”
21.Hydroxyapatitie deptiosition diseaseMale = female40-70 yearsMC = single joint ivnovledPain, tendernss, localized swelling and reduced rang eof motinTendon Ca++
22. Calcium Pyrosphosphate Dihydrate DepositionMale = Geamleusually grater than 30 with peak at 60
Acute presentation 20%, sweloen, hote tender jiotnsChronic presentation 60% stimulates osteoarhtrosis
23. JRAChronic polyarhtitis resmbing RABeigns before age 16
Radiogrpahic gindignsSoft tisuew swelling, osteoporosis, epristitis, balloneed epipyses, unofrm joint spac eloos, inta-articular ankylosis
24. SLEGeneralized concnectiv tissue disorder affecting ulitple organ systemsWomen of child-bearing age
Onset with fevere, malaise, skin rash and arthralgiasMost prominenet feature in hands
Reversible subluxations, dislocations
25. Primary OsteoarthritisInflmamtory variant of ostearhtotis involving the IP joint sof the handsCnetral erosisoinof the head of rpixmal pahalnsx and peripheral eroiss of the distal phalancx produece “gull” wing
signs.
DX. IMAGING #2 – 7/2/08
PVSBreak in pattern with “apple core.” More villonodular tissue that wrapped around, spreading to the head. Normal caliber and compressed in an apple core lesion. The lesion is more likely in the femur. This is villi formation that occur. It has an effect on bone, can cause ischemic compression.
Neuropathic ArthropathiesTertiary syphilis, Diabetes Mellitus, Syringomyelia can all be causes. CSF is intended to flow. Syrinx formation can cause compressive myleophaty with anatomic damage to the cord (called syringomyelia).
Nueurologic Injury that disruputs the proprioceptive function. The joint surfaces aren’t in relationship to the other. The joint surfaces bang off each other. The surfaces aren’t met to strike other surfaces. The chondral tissue is injured frequenctly and can’t rejuvenate. The underlying bone is now exposed. Aon with loss of ropiroception is loss of sensory. They can’t fully feel the magniftued of pain (they feel it, but not the extent of it). They walk into your office. “Bag of bones”…There is unccoridaanted proprioceptve finction. The person does not feel the full extent of the pain.
Syringomyelia picture
*** Picture of Woman With Diabetes Mellitus (lateral view of mortise joint of ankle)…The tallus and calcaneus are hard to view. We’ve got neurotorphic joint disease. The more common of the two forms is hypertrophic. The 6 D’s of neurotrohpic joint disease: 1). Destruction (boney destruction) 2).Debris (bone fragments) 3).Distention (bony bleeding into the capsule) 4).Disorganization 5).Dislocated (a lot of joint motion with the feeling of dislocation) 6). Density (dead bone gets more dense)…The most likely contributor is diabetes. This patient walked in. The foot is swollen, discolored and can be unstable. They do walk into your office.
The second version is atrophic. A common descriptor is surgical amputation. *** Picture of the foot…The 3rd metatarsal shows a candy lick appearance/sign. ****** Picture of the hip…Surgically amputated appearance is present…There is a great gap near the intertrochanteric line. The patient has minimal discomfort despite the shocking plain film sign. X-rays can’t fully predict amount of pain and dysfunction ***Note the missing/absent part of the bone
The 3 causes: 1). Diabetes mellitus 2). Syringomyelia 3). Tabes Dorsalis (tertiary syphilis)…#1 cause is diabetes mellitus. #2 and and #3 are debatable.
**** Ppicture of the shoulder…Syringomyelina is present. Typically a car accident in the past (months ago) with whiplash or cervical spine surgyer (considered trauma) can lead to syringomyelia. Spinal fixation surgery (discectomies) are linked with syringomyelia. New surgeries are attempting to decrease the risk of syringomyelia. Diabetics have poor vascular supply and weakned immune response. A typical diabetic may have callous, blisters that burst (taking away skin protection), diminished foot sensations (dermatitis – infection of the skin that respects nobody and no boundaries), lack of proprioceptive function ***
*** Know the 3 causes and know it is atrophic vs. neurotrophic. Know that if RA or psoriasis where present they would look like (pencil in cup) that favors the atrophic form. The mutilating arthritides favor presenting more like the atrophic form of this condition ***
SLE

The distinguishing feature is clinical. The problem is a small joint diseae (hand or foot). The hands are deformed. They present with reversible subluxation (clinically and radiographically). This is a functional problem. You work the tendons, use paraffin baths and others to treat them. If they can keep holding a fist (without it opening), that is a good sign. You cannot cure SLE, but you can manage symptoms. Most times patients are happy to have mobility back ***
Enteropathic ArthrtisThe primary problem is inflammatory bowel diseae with an arthritis that looks like the twin (AS). We cannot tell the difference between the two radiographically. The way to tell the difference is all in the history. They have bowel disease in their history. IN practice, you’ll see a couple of these cases in practice.
The AS patient will show SI joint fusion that jumps up to the T/L junction. The pattern is genetic related. The spine disease is accented vs. the bowel disease. The lab marker used to spearte the two is HLA B27. Over 90% of AS patients have the elevation. A lesser amount have this problem with enteropathic arthritis.
Psoriatic ArthropathyAlmost all the patients present with skin disease. 1-2% don’t have concurrent skin disease, but they get it soon after. Most everyone has skin diseae first and arthritis second. The twin is Reiter’s (Reactive arthritis). We are trying to tuse the word REACTIVE more than Reiter’s.
Reactive Arthritis damage in the hand
We tell the difference between reactive and psoriatic by history. We recognize the reactive arthritis patient with the history. The history would include a clinical triad: Can’t see, can’t pee, can’t dance with me (clinically: 1). Polyarthritis 2). Conjunctivitis 3). Urethritis…They can contract “lover’s heel” by an STD. The condition can occur at the calcaneal bursa, calcaneus, Achilles, or plantar fascia. This is a condition with many sexual partners. Reactive arthritis affects the spine and large joints (not small joints). Psoriatic arthritis affects small joints, along with RA. Psoriasis has a Ray pattern. This involves multiple knuckles (equal opportunity destroyer of small joitns).
A picture of “lover’s heel”…Ostoephyte in the calcaneus-achilles-plantar fascia area.
The most significant problem of inflammatory joint disease is ADI instability. We need to document stability at this joint by a cervical series that includes flexion and extension.
Reiter’s affects the spine and hips vs. psoriatic which can and does affect the small joints.
Inflammatory ConditionsBony fusion/ankylosis can present with inflammatory condition. We can prevent ankylosis for a long time with movement. It is a potential end product and if we do nothing they will get their more quickly. With treatment, they can postpone or prolong the bony ankylosis. RA affects both hands (bilateral symmetrical presentation). RA typically doesn’t affect the SI joints, and if it does it only affects one side (unilateral).
RA is the greatest threat to fusion of the hands (the most frequent diagnosis that can lead to fusion). The highest percentage of ankylosis is psoriasis (turns the greatest % to fusion, even though it is in the least amount of people).
EX. We have 100 patietns for each arhtopathy and what % of the subgroups develop ankylosis? Psoriases will develop ankylosis the most over the other conditions.
Ex. If we have 100 people that can present with inflammatory arthritis what will be the most common? RA
Periarticular blood flow in the small joints increases. Hyperemia can pressure erode/wash away bone. The most predictable change in bone density is down as hyperemia is more common in RA.
Disuse Osteoporosis with Psoriatic Arhtiris?
EOAErosive Osteoarhtirtis Arthritis
Scleroderma

Can’t close their mouth because of induration of soft tissue. The skin and conncctive tissue tighten. The fingers and toes are taken away (Acroosteolysis).
Sclerodemra patient that can’t closer their mouth.
SI Jiont Diseae that is silent and biased to females (OCI). This is osteitis condensans ili. The shape is triangular shaped and on the iliac side. The classic OCI patient has multiple full term berths. Relaxin, elastase, and other hormones affect the women during pregnancy. Ofthen the body respons to laxity by bony hardening of the area. C-section does not matter as the women still produces the hormones during the pregnancy. This condition may/may not go away.
Crystal Deposition Diseases1. Gout: Uric Acid crystals present (also called sodium mono-urate). Samples of the soft tissue swelling can show he
crystals within it. 2. CPPD: This is another crystal deposition problem. It stands for calcium pyrophosphate dehydrate deposition.3. Ocranosis/Alcaptneuria: The crystal is found in urine. The urine finding is black urine due to oxygen. It oxidizes
based on room oxdiaiton and occurs at the top of the cup. The crystal is homogeniticic acid. The accumulation is because of lack of enzyme (homogenticic acid oxidase).
4. Hydroxyapetite Deposition (HAD): This fits in the degenerative conditions. It is a degenerative condition that presents with DJD with tendonpathy or bursopathy overlay (calcific tendonitis orbursitis). This is dystrophic calcification. Ex.—Rolling ankle causes peroneal tendon calcium depotision….Multiple trauma is the culptir leading to the dystrophic calcification.
Tophaceious Gout: Presnet with soft tissue calcifications. What you see is calcium based, but the sodium monourate is invisible (radiolucent) on X-ray changing the pH and damaging the tissues. The pH is changed to alkaline and leads to the deposition.