dwij physiology of bone
TRANSCRIPT

GOOD MORNING

PHYSIOLOGY OF
BONE
By- Dr. Dwij Kothari
1st year MDS

CONTENTS
Introduction
Definition
Functions of bone
Classification of bone
Types of bone
Structure of bone
Macroscopic
Microscopic
Bone ossification

Types of bone cells
Growth and development
Bone physiology
Calcium metabolism
Composition of bone
Bone remodeling
Effect of other hormones on bone
Prosthodontic considerations
Conclusion
References

INTRODUCTION
Bone is a highly vascular connective tissue.
They are rigid organs that support and protect the
various organs of body; produce red and white blood
cells and store minerals.
Bones come in a variety of shapes and have a
complex internal and external structure, are light
weight yet strong and hard, and serve multiple
functions.

Types of tissue found in bones are mineralized
osseous tissue, marrow, endosteum, periosteum,
nerves, blood vessels and cartilage.
At birth there are over 270 bones in an infant
human’s body. But many of these fuse together as the
child grows, leaving a total of 206 separate bones in
an adult.

DEFINITION Bone – is the hard portion of the connective tissue
which constitutes the majority of the skeleton;
It consists of an inorganic or mineral component and
an organic component (the matrix and cells);
The matrix is composed of collagenous fibers and is
impregnated with minerals, chiefly calcium phosphate
(approx 80%) and calcium carbonate (approx 10%),
thus imparting the quality of rigidity.
(GPT 8)

FUNCTIONS OF BONE
Bones provide the framework and protectthe soft tissues and vital organs of the body.
Acts as reservoir of minerals.
Is the site of productionof blood cells.
Helps in nerve muscle conduction.

Classification of bone
1) According to position
Axial skeleton
Appendicular skeleton
2) According to shape
Long bones
Short bones
Flat bones
Irregular bones
Pneumatic bones
Sesamoid bones
3) According to development
Membrane(dermal) bones
Cartilaginous bones
Membrano-cartilaginous
bones
4) Structural classificationCompact bones
Cancellous spongy or
trabecular bones

CLASSIFICATION OF BONES:
- According to Position :
Appendicular skeleton –bones forming
appendeges of body.
e.g Bones of the limbs, shoulder, and hip
Axial skeleton – bone forming axis of body.
e.g Skull, rib, sternum and vertebrae.

According to Shape :
1) LONG BONES-
• Longer than they are wide (e.g
Humerus)
• Consist of a long shaft with two
expanded ends - epiphyses
• Primarily compact bone but may
have a large amount of spongy
bone at the ends or extremities
• Typical , Miniature and Modified
long bones.

2) SHORT BONES-
• Shape – cuboidal ,trapezoid or
scaloped
• Carpal & tarsal bones

3) FLAT BONES-
• Thin, flattened and a bit curved
(e.g. sternum , scapula , & vault
of skull)

4) IRREGULAR BONES-
• Vertebra, hip bones, bones in the
base of the skull
5) PNEUMATIC BONES-
•Irregular bones contain large air
spaces lined by epithelium
•Maxilla, sphenoid, ethmoid
6) SESAMOID BONES-
•Bony nodules embedded in tendons
or joint capsules.
•Patella, fabella etc.

According to development of bone :
Membranous ( ectodermal) bone
Ossify in membrane – derived from intra membranous
ossification
Bones of vault of skull and facial bones
Cartilaginous ( endochondral ) bone
Endochondral ossification
Vertebral colums , thoracic cage bones of limbs
Membrano-cartilaginous bones
Clavicle, mandible, sphenoid, occipito temporal

Compact Bone
Solid bone,
Dense in texture but porous
Except for those
accommodating cells,
processes and blood vessels
Arms and legs
Adaptation to bending and
twisting forces
Spongy bone
Open in texture ,
meshwork of trabeculae
Usually interior of bone
Many spaces between
spicules (or trabeculae) of
bone
Marrow found within the
spaces
Spine, ribs, jaw, wrist
Adaptation of
compressive forces
According to structure of bone :

Compact bone morphology
Lacuna
Osteocyte home
Haversian canal
Central canal for blood
vessels, etc
Canaliculi
Osteocyte processes
Lamellae
Concentric circles
representing
appositional bone
deposition

Spongy (trabecular) bone
Consists of thin plates
between whom spaces are
present
Radiographically,
•TYPE 1 : Regular and horizontal
trabeculae.
• TYPE 2 : Irregularly arranged
numerous delicate trabeculae.

At microscopic level, there are 4 types of bone.
* Woven bone
* Lamellar bone
* Composite bone
* Bundle bone
( Contemporary implant dentistry , MISCH, 3rd
edition)

Woven bone
Relatively weak, disorganized, and poorly
mineralized.
Serves a crucial role in wound healing by
(1) Rapidly filling osseous defects,
(2) Providing initial continuity for fractures and
osteotomy segments,
(3) Strengthening a bone weakened by surgery or
trauma.

Lamellar bone
Strong, highly organized, well- mineralized tissue.
Makes up more than 99% of the adult human
skeleton.
Provides good strength.
The full strength lamellar bone that supports an
endosseous implant is not achieved until about 1 year
postoperatively. Contemporary implant dentistry, MISCH, 3rd edi.

Composite bone
Osseous tissue formed by the deposition of lamellar
bone within a woven bone lattice, a process called CANCELLOUS COMPACTION.
Quickest means of producing relatively strong bone.
When the bone is formed in the fine compaction
configuration, the resulting composite of woven and
lamellar bone form structures known as primary
osteons.

Bundle bone
It is a functional adaptation of lamellar structure to allow attachment of tendons and ligaments.
Perpendicular straitions, called Sharpey’s fibers, are the major distinguishing characteristics of bundle bone.
Distinct layers of bundle bone usually are seen adjacent to the PDL along physiologic bone- forming surfaces.

ANATOMY: STRUCTURE OF BONE
Diaphysis
Epiphysis
Metaphysis
Articular cartilage
Periosteum
Endosteum
Medullary or marrow
cavity
A typical long bone consist of following
(The anatomical basis of medicine and surgery, Gray’s anatomy, Peter.L.William, 39th edition)

Structure of Short, Irregular, and Flat Bones
Thin plates of periosteum-covered compact bone on the outside
with endosteum-covered spongy bone (diploë) on the inside
Have no diaphysis or epiphyses
Contain bone marrow between the trabeculae

Two fundamental factors which lead to strength of bone are
intimate combination of mineral salts and fibrous tissue and
the units of concentric microscopic tubular lamellae.
The bone substance forms trabeculae running in directions
suited to their functions.
The trabeculae are strongly developed in regions subjected to
compression or tensile stresses.

Microscopic structure of bone
Bone is composed of basic units called lamellae.
Lamellae are thin plates of bone.
Each lamellae has,
- gelatinous matrix
- ground substance of collagen fibres
- calcium salts deposited in matrix

Lamellae are placed one above
another with small spaces between
them. They are called lacunae.
Lacunae contains osteocytes.
Lamellae arranged as -concentric
plates around a small central canal.
• Called a haversian system or
osteon.
Volkman’s canals interconnecting
channels containing blood vessels &
the adjacent haversian canals

Lamellae are 3 types based on their placement.
a) circumferential lamellae – these enclose entire adult
bone, forming its outer perimeter.
b) concentric lamellae – these make up the bulk of
compact bone.
c) interstitial lamellae – are interspersed between
concentric lamellae and filling spaces between them.


PHYSIOLOGY OF BONE FORMATION:OSSIFICATION
• The process by which bone forms is called OSSIFICATION.
• The skeleton of a human embryo is composed of fibrous
connective tissue membrane formed by embryonic connective
tissue (mesenchyme) and hyaline cartilage that are loosely shaped
like bones.
• They provide supporting structure for ossification.
• Ossification begins around the 6th or 7th week of embryonic
life and continues throughout adulthood.

BONE OSSIFICATION
Involves both production of organic bone matrix and
calcification
This is NOT bone GROWTH!!!
Two types of ossification:
Intramembranous
Endochondral

Bone formation follows one of 2 patterns;
1. Intramembranous ossification- refers to the formation of bone
directly on or within the fibrous connective tissue membranes.
2. Endochondral ossification- refers to the formation of bone in
hyaline cartilage
•Maxilla forms by intramembranous ossification.
•Mandible forms partly by intramembranous and partly by
endochondral ossification.
•Greater part of body, ramus, condylar and coronoid process are
intramembranous in origin.
•Only the tip of condylar and coronoid process are of
endochondral origin.

INTRAMEMBRANOUS OSSIFICATION
1) At the site where bone will develop, mesenchymal cells become
vascularized, cluster and differentiate –
• First into osteoprogenitor cells and then into osteoblasts.
• The site of such a cluster is called a centre of ossification.
• Osteoblasts secrete the organic matrix of bone and gets
surrounded to become osteocytes.
• Later calcium & other minerals are deposited and tissue
calcifies.

2) As the bone matrix forms, it develops into trabeculae. As
trabeculae develop in various ossification centres, they fuse
with one another to create the open latticework appearance of
spongy bone. Connective tissue in trabecular spaces
differentiates into red bone marrow.
3) On the outside of bone, vascularized mesenchyme develops
into periosteum. Eventually, Some of the spongy bone is
replaced by the cortical bone. This will remodeled to reach its
adult size & shape.

ENDOCHONDRAL OSSIFICATION
1) Development of the cartilage model.
• Mesenchymal cells differentiate into
chondroblasts which form the
hyaline cartilage model
• A membrane called perichondrium
develops around the cartilage
2) Growth of the cartilage model
•Cartilage model grows by interstitial & appositional growth
•Chondrocytes in mid-region calcify the matrix
•Vacated lacunae forms small cavities
•Osteoblasts in perichondrium produce periosteal bone collar( once
perichondrium starts to form bone, it is known as periosteum)

3) Development of primary ossification center
•Near the middle of the model, capillaries of the periosteum grow into
the disintegrating calcified cartilage.
•These vessels and the osteoblasts, osteoclasts & red marrow cells, are
known as the periosteal bud.
•With the development of periosteal bud, primary ossification center
and medullary cavity forms.

4) Development of the diaphysis and epiphysis
•The diaphysis, which was once a solid mass of hyaline cartilage, is
replaced by compact bone.
•When blood vessels( epiphyseal arteries) enter the epiphysis,
secondary ossification centers develop. ( usually around the time of
birth)

Stages in formation of bony lamellae
After secondary ossifying center develops –
Osteogenic cells become osteoblasts
Lies along the surfaces of bars or plates of bone
Osteoblasts lay down a layer of ossein fibrils – osteoid.
Lamellus of bone formed
Osteoblasts now lay down another layer of osteoid over
first lamellus.

Types of bone cells*Osteoprogenitor – resting cell that can transform into
an osteoblast and secrete bone matrix
*OSTEOBLASTS – Produces new bone, derived from
bone marrow cells
*OSTEOCYTES – not clear, osteoblasts when they lose
their activity become osteocytes
*OSTEOCLASTS – lyse or eat away bone, derived from
precursors of monocyte in the bone marrow

Osteoprogenitar cells
* Appearance
pale staining,
small, spindle shaped
* Location
present on all non-
resorbing surface
* Function
give rise to osteoblasts in
vascularized regions
chondroblasts in avascular
regions

Osteoblasts
* Appearance
Large nondividing cells,
eccentric nucleus, basophilic
cytoplasm, negative Golgi
image, cytoplasmic processes.
* Function
Synthesize and secrete organic
constituents of bone matrix
(osteoid)
aid in calcification.

Osteocyte
Appearance
* smaller and less
basophilic than
osteoblast,
* have interconnecting
processes
Function
* forms bone matrix in
repair conditions.
* release calcium ions from
bone matrix when calcium
demands increase

Osteoclast
Appearance
multinucleated,
non-dividing cells,
very acidophilic.
Have a ruffled border
and clear zone
Origin
From blood monocytes/
macrophages

Function
move around on bone surfaces,
resorb bone matrix
Focal decalcification and extra cellular digestion by acid hydrolases and uptake of digested material
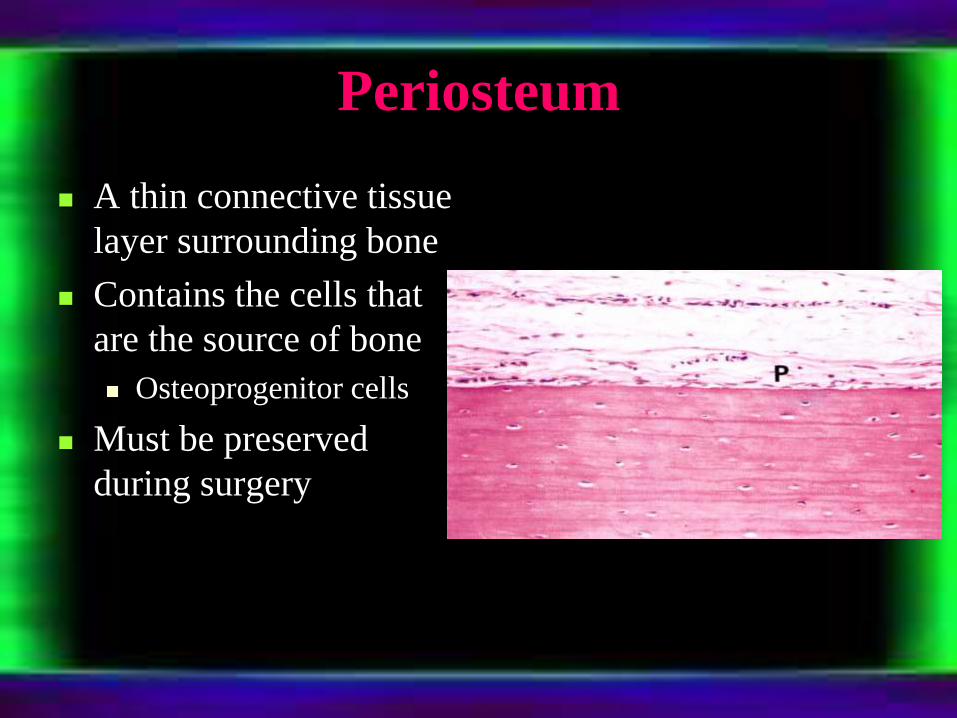
Periosteum
A thin connective tissue
layer surrounding bone
Contains the cells that
are the source of bone
Osteoprogenitor cells
Must be preserved
during surgery

Growth and development
GROWTH – An increase in size (TODD)
DEVELOPMENT – is progress towards maturity (TODD)
GROWTH SPURTS – sudden increase in growth.
a) Just before birth
b) 1 year after birth
c) Mixed dentition growth spurt – boys (8-9 years) girls (7-9 years)
d) Pre pubertal growth spurt – boys (14-16 years) girls (11-13 years)

Mechanism of bone growth
The changes that bone deposition and resorption can produce are,
a) Change in size
b) Change in shape
c) Change in proportion
d) Change in relationship of the bone with adjacent structures.
A combination of bone deposition and resorption resulting in a growth movement towards the depositing surface is “cortical drift”

Displacement –
movement of the
whole bone as a unit.
a) Primary displacement
b) Secondary
displacement

Theories of bone growth
GENETIC THEORY – growth is controlled by genetic
influence.
SUTURAL GROWTH THEORY (SICHER) – cranio facial
growth occurs at the suture
CARTILAGINOUS THEORY( JAMES SCOTT) – intrinsic
growth controlling factors are present in cartilage and
periosteum with sutures being only secondary.

THE FUNCTIONAL GROWTH MATRIX CONCEPT
(MELVIN MOSS) – claims that the origin, form, position,
growth and maintenance of all skeletal tissues and organs are
always secondary, compensatory and necesssary responces to
chronologically and morphologically prior events / processes
that occur in specifically related non skeletal tissues, organs /
functioning spaces.

VAN LIMBORG’S THEORY (1970) – suggested the
following 5 factors that he believed controlled growth.
a) Intrinsic genetic factor
b) Local epigenetic factors
c) General epigenetic factors
d) Local environmental factors
e) General environmental factors

ENLOW’S EXPANDING ‘V’
PRINCIPLE – the growth
movements and
enlargements of these bones
occurs towards the wide end
of ‘v’ as a result of
differential deposition and
selective resorption of bone.
Growth factor that regulate bone
remodelling
1. Insulin – like growth factors (IGF) I & II
2. Transforming growth factor –b (TGF – b) superfamily,
including the bone morphogenetic proteins (BMPs)
3. Fibroblast growth factors (FGF)
4. Selected cytokines of the interleukin (IL), tumour necrosis
factor (TNF), & colony – stimulating factor (CSF) families


Functions of growth hormone
It has effects:
1) On growth of skeleton, skeletal muscle
and viscera.
2) On metabolism of a) carbohydrate b)
protein c) fat d) electrolytes.
3) On milk production - lactogenic effect.
4) On erythropoisis.

Bone physiology
- CALCIUM METABOLISM
- BONE REMODELLING

Calcium metabolism
Daily intake - 1000mg
Intestinal absorption – 350
Secretion in gastrointestinal juices – 250
Net absorption over secretion – 100
Loss in feces – 900
Excretion in the urine – 100
* Sources of calcium:
Milk and milk products, egg, vegetables (phytic acid)

BONE’S ROLE IN CALCIUM METABOLISM
Decrease in ca2+level
Receptors
Parathyroid gland cells detect lowered ca2+ conc
Control center
PTH gene
turned on
INPUTcAMP
OUTPUT release of PTH
Effector
Osteoclast increase bone resorption
Kidney release ca2+ in blood, excrete phosphate in urine, and produce calcitriol
Response
Increase in blood ca2+ level
Return to homoestasis when response brings ca++ back to normal
Some stimulus disrupts homeostasis by causing

Calcium in the plasma and interstitial fluid
Average Plasma calcium concentration – 9.4mg/dl
Equivalent to 2.4 mmol of calcium per liter
Calcium in the plasma – 3 forms
1. 40% combined with plasma proteins - nondiffusible through
capillary membrane
2. 10% diffusible through capillary membrane but non ionized
3. 50% diffusible and ionized

Clinical manifestations
HYPOCALCEMIA
1) Concentration of serum calcium is low but calcium is normal, so no tetany results.
2) calcium is low, so tetany results.
Cause – PTH deficiency, vit-D deficiency, etc.
HYPERCALCEMIC STATES
When blood level of calcium rises above 12mg/dl
1) Drowsiness
2) Decreases the QT interval of heart – causes constipation.
3) Calcium deposits in soft tissues

TETANY
- Due to hyperirritability of motor nerve fibres supplying the skeletal muscle.
- Painful tetanic contraction of the muscles resulting in spasm.
- Trousseau’s sign

COMPOSITION OF BONE
Bone
Inorganic 65% Organic 35%
(Primarily calcium phosphate
which is present in form of
Highly insoluble crystals of Collagen 90-95 % Ground substance 5-10 %
Hydroxyapatite) •Glycoprotein
•Proteoglycan
•Sialoproteins
•Lipids
Bone and its relation to extracellular
calcium and phosphate

Organic matrix of bone
90-95 % is collagen fibres, which gives bone its powerful
tensile strength.
5-10 % is a homogeneous gelatinus medium called ground
substance.
Ground substance is composed of extracellular fluid plus
proteoglycans like chondroitin sulfate and hyaluronic acid
which helps to control the deposition of calcium salts.

Bone salts
Major crystalline salts, hydroxyapatite of bone are principally
composed of calcium and phosphate.
Ca10 (PO4) 6 (OH) 2
Each crystal – 400 Å long, 10-30 Å thick, 100 Å wide
Shape – long , flat plate
The relative Ca/P ratio on a weight basis is 1.3 -2
Magnesium, sodium, potassium and carbonate ions are also
present. They are believed to be conjugated
TENSILE AND COMPRESSIONAL STRENGTH OF BONE
Collagen fibers provide bone with great tensile strength while
Inorganic salts allow bone to withstand compression.

Calcium exchange between bone and
extracellular fluid
Whenever calcium salts are injected intravenously or removed from the circulating body fluids, the concentration returns to normal within 30 minutes to 1 hour due to exchangeable calcium present in bone, about 0.4-1% of the total bone calcium.
It provides a rapid buffering mechanism to keep the calcium ion concentration in equilibrium.

Bone remodelling
Deposition of bone by the Osteoblasts :
o Found on the outer surfaces of bone and in the bone cavities.
o Small amount of osteoblastic activity occurs continually - in all living bones
( on about 4% of all surfaces at any given time in an adult)

Absorption of bone by Osteoclasts:
oLarge phagocytic, multinucleated cells.
oNormally active on < 1% of bone surfaces in an adult
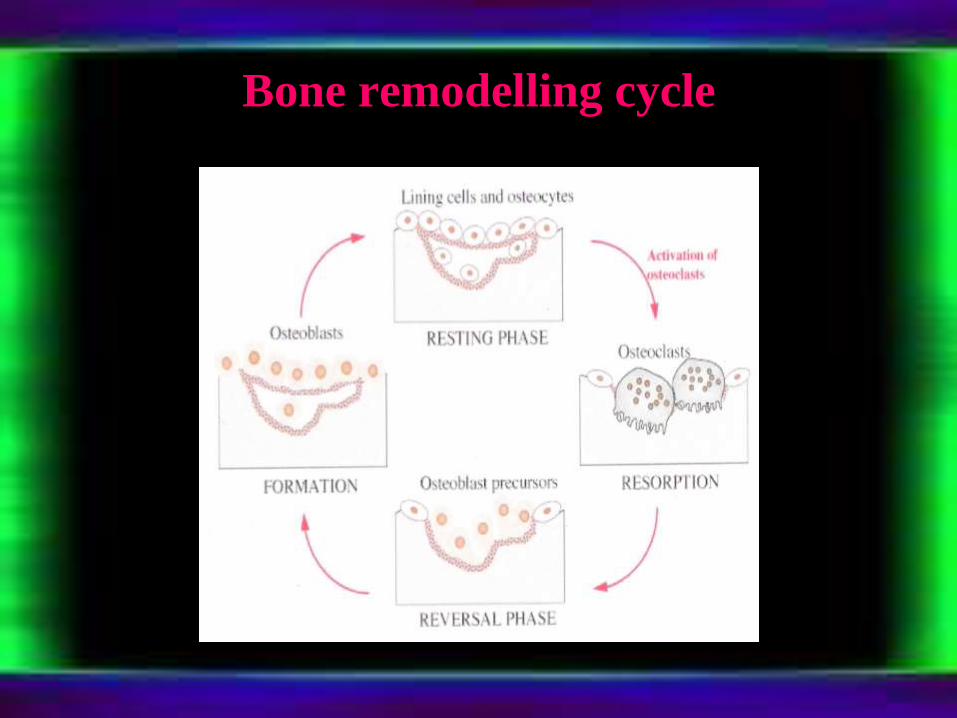
Bone remodelling cycle

Process of bone remodelling

Value of continual bone remodelling
Adjusts its strength in proportion to the degree of bone stress,
bone thickens when subjected to heavy loads.
Shape of the bone can be arranged for proper support of
mechanical forces
New organic matrix is needed as the old organic matrix
degenerates, thus normal toughness of bone is maintained.

Repair of a fracture activates all the periosteal and intraosseous
osteoblasts and also new osteoblasts are formed from
osteoprogenitor cells.
Within a short period of time osteoblastic tissue and new
organic bone matrix followed by deposition of calcium salts
develop between the two broken ends of the bone.
This is called a callus.
Bone remodelling and repair

HEALING OF EXTRACTION SOCKET
The removal of a tooth initiates the sequence of
inflammation, epithelization, fibroplasia & remodeling.
Socket heals by secondary intention & it takes
minimum of 6 months for healing of a socket to the degree to
which it becomes difficult to distinguish from the surrounding
bone when viewed radiographically
When a tooth is removed, the remaining empty
socket consists of cortical bone (radiographic lamina dura) &
a rim of oral epithelium left at the coronal portion.

In 30 minutes, the socket fills with blood, which coagulates &
seals the socket from the oral environment.
During the 1st week, inflammatory stage takes place.
All debris, bone fragments & contaminating bacteria will be
removed by leukocytes
Fibroplasia begins with the ingrowth of fibroblasts &
capillaries
Epithelium migrates along the inner surface until they meet
or till the bed of granulation tissue
At the end of 1st week osteoclasts accumulate along the
crestal bone.

During the 2nd week,
Large amount of granulation tissue fills the socket.
Osteoid deposition has begun along the alveolar bone lining
the socket
(In smaller sockets the epithelium may have become fully
intact by this point.)
During 3rd & 4th week,
The process started in 2nd week will continue & healing with
epithelization of most sockets complete at this time.
The cortical bone continues to resorb from crest & walls of the
socket & new trabecular bone is laid down across the socket.

During 4th – 6th month,
It is not until 4 – 6 months after extraction, the cortical bone
lining a socket is fully resorbed, which is radiographically evident
when there is loss of distinct lamina dura.
The epithelium moves towards the crest & eventually becomes
level with the adjacent crestal gingiva.
At Ist year, the only remnants visible after 1 year is the rim of
poorly vascularized fibrous tissue (scar) that remains on the
edentulous ridge.
During 2nd month,
Histologically the socket is filled with immature bone by
the end of second month and there is some quantitative loss when
healing is uneventful. This loss in quantity during normal healing
after extractions is one of the reasons of waiting period of 6 weeks
to 2 months is often advocated prior to the placement of the
dentures

Effects of other hormones on bone

Parathyroid hormone
4 parathyroid glands located
immediately behind the
thyroid gland – one behind
each of the upper & each of
the lower poles of the
thyroid.
Each gland is 6mm long,
3mm wide, & 2mm thick.

Contains mainly chief cells & moderate no. of oxyphilcells.
Chief cells secrete PTH & oxyphil cells are believed to be modified or depleted chief cells that no longer secrete hormone.
PTH is first synthesized on the ribosomes in the form of a preprohormone, a polypeptide chain of 110 amino acids.

Effect on bone
PTH accelerates removal of calcium from bone by 2 processes.
Its initial effect is to stimulate osteolysis.
A 2nd more slowly developing effect of constant exposure to
PTH is to stimulate the osteoclasts to resorb completely
mineralized mature bone.
PTH also has anabolic actions on bone.

Effects of glucocorticoids on bone
metabolism Bone formation
Most important
Bone resorption Probably only during 1st 6 – 12 months of Rx
OC production & postponed apoptosis
Long term, bone turnover
Intestinal absorption of calcium
Urinary phosphate & calcium loss Direct effect on kidney
Secondary Hyperparathyroidism
Bone loss
Early but temporary

Thyroid gland
Regulates metabolism and blood calcium levels.
On skeletal system. Thyroxineis required for the growth and maturation of epiphysealcartilage so that in the absence of this hormone, linear skeletal growth does not occur.
Excess thyroxine causes osteoporosis because of calcium drainage from the bone.

Calcitonin
A peptide hormone secreted by thyroid gland.
Tends to decrease plasma calcium concentration &, in general,
has effects opposite to those of PTH.
Synthesis & secretion of calcitonin occur in the parafollicular
cells, or C cells, lying in the interstitial fluid of the thyroid
gland.

Calcitonin actions
The major effects of calcitonin administration is a rapid fall in the plasma calcium concentration, caused by inhibition of bone resorption.
Calcitonin is a physiologic antagonist to PTH with respect to calcium. However, with respect to phosphate, it has the same net effect as PTH ; that is, it decreases the plasma phosphate level.

Bone disease in hyperparathyroidism
In mild hyperparathyroidism bone can be deposited rapidly
enough
In severe hyperparathyroidism the bone may be eaten away
almost entirely
Radiograph shows extensive decalcification and large punched
out cystic areas of the bone that are filled with osteoclasts in
the form of so called giant cell osteoclast tumors
Multiple fractures of the weakened bones from slight trauma
The cystic bone disease of hyperparathyroidism is called
osteitis fibrosa cystica
Large quantities of plasma alkaline phosphatase – due to
osteoblastic activity

Vitamin D
Source :-
1. Produced in the skin by ultraviolet radiation (D³)
2. Ingested in the diet (D² & D³)
Not a classic hormone
Minimum daily requirement is approximately 2.5μg, & the recommended daily intake is 10μg (400 units)
Most important diet sources are fish, plants, grains and milk.



Rickets
- In prolonged case , the compensatory increase in PTH secretion causes extreme osteoclasticabsorption of the bone
- Bone becomes weaker and imposes marked physical stress on the bone resulting in rapid osteoblastic activity
- These laid down large quantities of osteoid which does not become calcified

Osteomalacia
Deficiencies of vitamin D
and calcium occur as a
result of steatorrhea
Poor absorption of calcium
and phosphate
This almost never proceeds
to the stage of tetany but
often is a cause of severe
bone disability

Prosthodontic considerations
DEFINITION
Alveolar bone – “ The bony portion of the mandible or maxillae in which the roots of the teeth are held by fibres of the periodontal ligament ”.(GPT- 8)
Residual ridge resorption – A term used for the diminishing
quantity and quality of the residual ridge after teeth are
removed. (GPT – 8)
BONE SUBSTITUTES
I) Bone graft materials
AUTOGENOUS BONE GRAFTS
a) Bone from intra-oral sites: osseous coagulum, bone blend,
intra-oral cancellous bone marrow transplants,bone swaging.
b) Bone from extra-oral site: iliac autografts
ALLOGRAFTS
a) Undecalcified freeze-dried bone allograft (FDBA)
b) Decalcified freeze-dried bone allograft (DFDBA):
bone morphogenic proteins BMP, osteogenin

XENOGRAFTS
Calf bone ,keil bone, anorganic bone
II) Non-bone graft materials
• Sclera
• Cartilage
• Plaster of paris
• Calcium phosphate biomaterials
2 types of calcium phosphate ceramics have been used:
1) hydroxy apatite
2) Tricalcium phosphate
• Bioactive glass
• Coral derived materials

RESIDUAL BONE AND MAXILLOMANDIBULAR
RELATION
•It is generally agreed that residual edentulous alveolar ridges resorb;
however there remains some controversy regarding the effect of
dentures on the process.
•Some authorities discussed the concept of disuse atrophy and
recommended that dentures be constructed and worn to preserve the
alveolar ridge. In contrast, others have emphasized the mechanical
trauma that is associated with the wearing of complete dentures

CHANGE IN FUNCTION:
The reaction of the bone to a change in function is
subjected to the supreme test when the natural teeth are extracted
and replaced with dentures.
WOLFF’s LAW states that a change in form follows a change in
function owing to the alteration of the internal architecture and
external conformation of the bone, in accordance with
mathematical laws.
Intermittent Stimulation Bone Apposition
Constant stimulation (Irritation) Bone Resorption

REACTION TO PRESSURE
•Bone builds in response to tensile stimulation, like the pull of a
ligament or muscle. Once the teeth are removed, dentures cannot
provide such stimulation.
•A denture is potentially capable of exerting steady pressure and also
intermittent heavy pressure that can interrupt the blood supply,
resulting in resorption.
•For this reason the dentures should be removed at least 8 of every 24
hour

•CHANGES IN THE SIZE OF BASAL SEAT:
•Maxillary teeth generally flare downward and outward, so bone
reduction generally is upward and inward.
•Since the outer cortical plate is thinner than the inner cortical plate,
resorption from the outer cortex tends to be greater and more rapid.
•The anterior mandibular teeth generally incline upward and forward
to the occlusal plane, whereas the posterior teeth are inclined slightly
lingually.
•The outer cortex is generally thicker than the lingual cortex. Also,
the width of the mandible is greatest at its inferior border. As a result,
the mandibular residual ridge appears to migrate lingually and
inferiorly in the anterior region and to migrate buccally in the
posterior region.
• Consequently, the mandibular arch appears to become wider
posteriorly as resorption progresses

4 clinical factors related to resorption rate :
I. Anatomic factors comprise size, shape, and density of
ridges, thickness and character of mucosal tissue, the ridge
relationship, and number and depth of sockets. Resorption rate
of residual ridges depend on bone volume and bone density.
II. Metabolic factors - nutritional, hormonal, other metabolic
factors that influence the osteoblasts and osteoclasts activity.
III. Functional factors - consist of frequency, intensity,
duration, and direction of force which translated into biologic
cell activity.
Bone formation or bone resorption may result.

Atwood, DA. Some, clinical factors related to rate of resorption of residual
ridges. J Pros Dent 1962; 12:441-50.
IV. Prosthetic factors - technique, materials, concepts,
principles and practices .

Procedures used in complete denture service to minimize the
loss of alveolar bone include:
Recording the tissues in the impression at their rest position.
Decreasing the number of teeth.
Decreasing the size of food table
Developing an occlusion that eliminates, as much as possible,
horizontal forces and those that produces torque
Extending the denture bases for maximum coverage within
tissue limits.
Eating by placing small masses of food over the posterior
teeth where the supporting bone is best suited to resist force.
Removing the dentures for at least 8 of every 24 hours for
tissue rest.

OSTEOPOROSIS
It is the loss of bone mass & density throughout the body,
including the jaws.
The basic problem is that resorption outpaces bone formation.
The common causes are:
Lack of physical stress on bones.
Malnutrition
Lack of vitamin C
Postmenopausal lack of estrogen secretion
Old age
Cushing syndrome

Riggs & Ganguly (1991) distinguished two distinct syndromes of
involutional osteoporosis.
1. Type1/postmenopausal osteoporosis: in which a loss of
trabecular bone is predominant, resulting in fractures of
vertebrae and wrist.
2. Type2/senile osteoporosis: in which both cortical and cancellous
bone are lost, resulting in hip fractures as well.
B. LAWRENCE RIGGS , CONSTANTINOS D. CONSTANTINOU, LARISA SEREDA, ARUPA GANGULY,
, Mutation in a gene for type I procollagen (COL1A2) in a woman
with postmenopausal osteoporosis, Proc. Natl. Acad. Sci. USA
Vol. 88, pp. 5423-5427, June 1991

Prevention of senile osteoporosis
Men – physical activity, exposed to sun light, adequate amount
of calcium containing foods or medicinal forms of calcium.
Women – estrogen therapy, vitamin D supplements, use of
fluorides, increased calcium intake.
(H. Rico, M. Revilla, L. F. Villa, E. R. Hernandez, J. P. Fernandez, Crush fracture
syndrome in senile osteoporosis: A nutritional consequence?, journal of bone and
mineral research )

AGING AND BONE TISSUE
There are 2 principal effects of aging on bone tissue.
The first is the loss of calcium and other minerals from bone matrix
(demineralization). This loss usually begins after age 30 in females,
accelerates greatly around age 40 to 45 as levels of estrogen decrease,
and continues until as much as 30% of calcium is lost by age 70. In
males calcium loss does not begin until after age 60.
The second principal effect of aging on the skeletal system is a
decrease in the rate of protein synthesis. The bones become brittle and
susceptible to fractures.

CONCLUSION
Physiological principles govern all aspects of
prosthodontic treatment and long term function. An
understanding of the fundamental physiology, metabolism, and
biomechanics of bone is essential for clinicians placing and
restoring these devices.
With this knowledge of bone physiology, it is possible to
institute procedures in prosthodontics that will assure a prosthesis
which would be more acceptable to the patients.

References
Text book of medical physiology, Arthur.C.Guyton, 9th edition.
Essentials of medical physiology, K.Sembulingam, 3rd edition.
Physiology, Robert.M.Berne, 5th edition.
Orthodontics, current principles and techniques, Thomas.M.Graber, 3rd edition.

Orthodontics, the art and science, S.I.Bhalaji, 5th
edition.
The anatomical basis of medicine and surgery, Gray’s anatomy, Peter.L.William, 39th edition.
New atlas of human anatomy, Thomas.O.Mccracken. 2nd edition.
Robbins and cotran basic pathology, kumar, cotran, robbins, 7th edition.
Oral histology (development, structure and function) A.R.Ten cate, 6th edition.

Oral anatomy, histology and embryology, B.K.B.Berkovitz,G.R.Holland, B.J.Moxham 4th edition.
Clinical biochemistry , ALLAN GAW, ROBERT A. COWAN,
DENIS ST.J.O’REILLY, MICHAEL J. STEWART, JAMES SHEPHERD.
Human Embryology, Inderbir Singh, 7th edition.
Contemporary implant dentistry , misch, 3rd edition.
Douglas C. Wendt, The degenerative denture ridge-Care and
treatment,J. Prosthet Dent 1974;32,5:477-492.

Dr. AJAY GUPTA, Dr. BHAWANA TIWARI, Dr. HEMANT GOEL, Dr
HIMANSHU SHEKHAWAT, RESIDUAL RIDGE RESORPTION : A
REVIEW, Indian Journal of Dental Sciences, march 2010 , vol 2 issue 2.
H. Rico, M. Revilla, L. F. Villa, E. R. Hernandez, J. P.
Fernandez, Crush fracture syndrome in senile osteoporosis: A
nutritional consequence?, journal of bone and mineral research
David J. Baylink, Jon E. Wergedal, Kenji Yamamoto, and
Eberhard Manzke, Systemic factors in alveolar bone loss, J
Prosthet Dent. 1974;31,5:486-505.
Atwood, DA. Some, clinical factors related to rate of
resorption of residual ridges. J Pros Dent 1962; 12:441-50.

Charles H. Chesnut III, and Patricia J. Kribbs, Osteoporosis:
Some aspects of pathophysiology and therapy, jpd 1982 Jul;
48(1)4-7.
Physiology & anatomy , A Homeostatic approach, John
Clancy , Andrew j Mcvica.

THANK YOU ALL

NEXT SEMINAR IS ON : 3-08-2012
SPEECH MECHANISM
BY- Dr. Baxi Harsh
1st year M.D.S.