drug/application - university of arizonaajgulbis/medlinks/pharmacology/... · web...
TRANSCRIPT

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Cholinergic Agonists Direct Acting Cause vasodilation by stimulating muscarinic type receptors on arteries
Increase Low viscosity saliva
CONTRAINDICTIONS: Bradycardia, hypotension, asthma, and peptic ulcer
All acetylcholine receptors are nicotinic except parasympathetic end organ receptors which are muscarinic
1st adrenergic receptor is nicotinic
Acetylcholine Eye surgery - topical Coronary angiography -
Coronary vasodilatation
Nicotinic and Muscurinic agonist
Broken down by AchE - Brief duration of action
No CNS
NT as sympathetic ganglia, pre and post- parasympathetic ganglia, adrenal medulla, and NMJ
Carbachol Nicotinic and Muscarinic agonist
NOT broken down by AchE No CNS
Bethanechol Used to stimulate intestine and bladder - increase contraction and tone
Muscarinic agonist Long duration of action NOT broken down by AchE No CNS
Decrease HR , decrease pupil diameter, increased secretions, bronchospasms, and increase GI and urinary function
In high does - causes vasodilatation and decreased BP due to activation of M3 receptors that release NO
Pilocarpine Glaucoma management - topical
Dry mouth - oral
Muscarinic agonist 2 - 3 hr duration of action NOT broken down by AchE CNS
Cholinergic crisis - salvation, lacrimination, urination, defecation, emesis (SLUDE syndrome)
Nicotine Smoking cessation - patch or gum
Nicotine receptor agonist CNS stimulant - respiration
stimulant and emetic effects
Nicotine poisoning causes depolarization block
Epinephrine Effects Bowel activity increase
Acetylcholinesterase reversible inhibitors
Indirect acting - temporarily blocks esteratic site of AchE
Physostigmine Antidote for atropine poisoning
Wide angle glaucoma
CNS - restlessness and agitation
Neostigmine Peripheral symptoms Treat myasthenia gravisNon-obstructive
intestinal/bladder atony
No CNS - due to positive charge
1

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Edrophonium Diagnosis myasthenia gravis
Same as neostigmine, but shorter acting (less potent)
Acetylcholinesterase irreversible inhibitor
Indirect actine - permanently bind
Depolarization block causing respiratory failure
Antidote is Pralidoxime(peripheral) / Atropine (central)
Sarin – Nerve gas
Malathion (organophosphates) – pesticide
Treat lice
Penetrate CNS Humans break
Isoflourophate Glaucoma - not a first line drug
Duration of action - 1 week Overuse leads to toxicity (SLUD)
Acetylcholinesterase reactivator
Pralidoxime Antidote for AchE inhibitor
Reactivates AchE - only effective if given early
No CNS - positive charge
Peripheral antidote
Acetylcholine receptor antagonist
Muscarinic antagonist side effects:
Atropine - from belladonna or jimson weed plants
Treat Parkinson Treat intestinal spasms Best treatment for
organophosphate poisoning
Decrease nasal secretions Dilate eye to examine the
retina
CNS Muscarinic antagonist
Dry mouth Constipation Decreased sweating Mydriasis Urinary retention Tachycardia Decreased tears Precipitation of glaucoma
2

Acute iritis Physostgimine poisoning Bronchodilation (no
longer used)
Decreased respiratory secretions
Scopolamine - from belladonna plant
Treats motion sickness Increase CNS effect Muscarinic antagonist
Drowsiness Amnesia
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
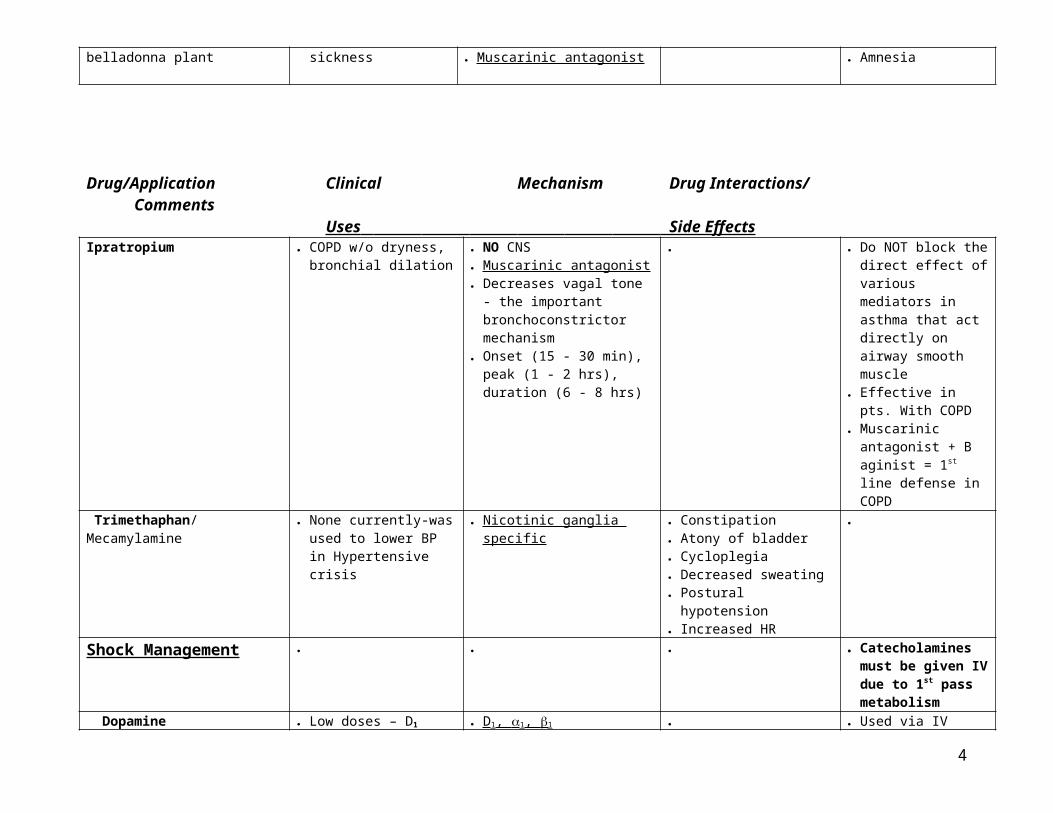
Ipratropium COPD w/o dryness, bronchial dilation
NO CNS Muscarinic antagonist Decreases vagal tone - the
important bronchoconstrictor mechanism
Onset (15 - 30 min), peak (1 - 2 hrs), duration (6 - 8 hrs)
Do NOT block the direct effect of various mediators in asthma that act directly on airway smooth muscle
Effective in pts. With COPD
Muscarinic antagonist + B aginist = 1st line defense in COPD
Trimethaphan/ Mecamylamine None currently-was used to lower BP in Hypertensive crisis
Nicotinic ganglia specific Constipation Atony of bladder Cycloplegia Decreased sweating Postural hypotension Increased HR
Shock Management Catecholamines must be given IV due to 1st pass metabolism
Dopamine Low doses – D1
Moderate - 1
High - 1
D 1, 1, 1
Brief duration - inactivated by liver MAO
Used via IV
Epinephrine Dose dependent Cardiac stimulant (B1) Bronchodilator (B2) Glaucoma (A1) Given IV, topical,
inhalation
1 2 1 2 Agonist Vasoconstrictor - do NOT use at terminal arteries
Norepinephrine Infrequently used - increases BP and contractility
1 2 1 Agonist NO CNS
Constricts renal blood flow
3
Given IV
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Phenylephrine To treat paroxysmal super ventricular tachycardia
Induces vagally mediated reflex
Decrease nasal secretions - topical
Induce mydriasis - does NOT effect accommodation
1 Agonist - vasocontriction
Indirect acting Sympathomimetics
Ephedrine Used orally Weight loss Performance enhancement
Release of NE B2 receptor agonist (minimum) CNS stimulant
Relax bronchial muscle Vasoconstriction of vessels
in nasal mucose Increased HR and BP Actions blocked by: cocaine
(block uptake), TCA (block uptake, and respirine (deplete NE content)
Herbal supplement
Amphetamine Narcolepsy Hyperactivity in children Appetite control
Catecholamine release CNS stimulant
Increased BP and HR
Cocaine Vasoconstriction Local anesthetic in surgical
procedures
2 adrenergic agonist-blocks re-uptake of serotonin, dopamine, and Norepinephrine
CNS stimulant Produces a massive release of
DA
Increase BP and HR Highly Addictive
Diuretics HTN Nephrogenic diabetes
insipidus Hypercalcemia Hypercalciuria
Fluid and electrolyte imbalance
Mannitol Transiently control Osmotic diuretic (inert sugar) Dehydration Used in IV
4

cerebral edema during neurosurgery
Maintain renal blood flow during major vessel surgery
Manage drug interactions
Loop of Henle Increases delivery of Na and
water out of the loop into the blood - decreases viscosity
Expands ECF volume Decreases renin release
Hypernatremia Temporary volume
expansion CONTRAINDICTIONS:
Pulmonary edema, anuria, dehydration
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Acetazolamide Glaucoma Antiepileptic Prevention of altitude
sickness
Inhibits carbonic anhydrase - both membrane bound and cytoplasmic CA
Increase urinary HCO3 excretion
Increased Na and Cl delivery to the loop of Henle
Causes metabolic acidosis CONTRAINDICTION:
Sulfa drug allergy
Rarely used as a diuretic
Thiazides (Hydrochlorothiazide) Edema states HTN Nephrogenic diabetes
insipidus
Inhibits the Na, Cl symport Distal tubule
Chronic use decreases Ca excretion
Less efficacious than loop diuretic
Loop Diuretics Furosemide Ethacrynic acid
Mobilize edema fluid Via IV - pulmonary edema Hypercalcemia
Ascending loop Inhibits the Na-K-2Cl transport Increase excreation of Ca, Mg,
Na, Cl
Dehydration Hyponatremia Hypernatremia Hyopkalemia Ototoxicity (deafness) CONTRAINDICTION:
Sulfa drug allergy, hypercalciuria, calcium kidney stones
K+ Wasting (does not require supplement)
Spironlactone Refractory edema associated with secondary hyperaldosteronism
HTN and edema Primary
hyperaldosteronism Co-administered with loop
diuretics and thiazides
Aldosterone receptor antagonist Late distal and collecting ducts
Hyperkalemia K sparing
Triamterene Used with loop diuretics and thiazides
Inhibit Na channels Late distal and collecting ducts
Hyperkalemia K sparing
B agonist Dobutamine Stimulate heart in
cardiogenic shock Short term - cardiac
decomensation
1 Agonist
5

Abuterol (metaproterenol) Dilate bronchial airways - used to manage asthma, COPD
2 Agonist Given orally - decrease BP and increase HR
Given via inhalation - jitters and tremors
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Isoproterenol Mild or transient episodes of heart block
For cardiac arrest until cardioversion can be performed
Bronchodilator (minimum)
1 2 Agonist Tachycardia
-Blockers (Sympatholytic drugs)
HTN Cardiac arrhythmias (AF -
after cardiac inversion) Angina
Chronic use (months) - Increased ejection fraction, contractility, and improvement in systolic performance with decrease in systolic and diastolic volumes and left ventricular mass
DO NOT use with asthma patients, COPD, unstable CHF, Occlusive peripheral vascular disease
Can cause AV Heart block High Doses With Ca+ blockers With Digoxin
Gradual removal due to upregulation of receptors
In persons with mild, moderate, or severe heart failure - reduces morbidity (40%) and mortality (30%)
Use with ACE inhibitor when treating CHF
Propanolol Management of Hypertension Angina Cardiac arrhythmias Migraine headaches Anxiety
1 2 –Antagonist (non-selective) - Decrease cardiac work and CO
Blocks renal 1 receptors to inhibit renin release - decrease angiotensin
No ISA
Bad dreams Depression Sexual dysfunction Aggravation of severe
congestive heart failure and occlusive peripheral vascular disease
Bronchospasms in asthma and COPD
INTERACTION: Calcium channel blockers and
6

Digoxin - causes AV blockMetoprolol Hypertension 1 –Antagonist - selective
No ISA Decreases CO and renin
SEE ABOVE SEE ABOVE
Timolol Glaucoma (major use) Antiarrythmia Treat hypertension
1 2 –Antagonist Decrease IOP by decreasing
aqueous humor production
topical
Central -Agonists Clonidine Centrally acting Anti-
Hypertensive (oral) 2-Agonists Inhibits release of NE - acts
pre-synaptically Decreased sympathetic outflow
to the heart- Decreased CO CNS
Sedation Withdrawal hypertension Decrease libido
Rebound hypertension
If given IV can cause direct vasoconstriction via A2 receptors
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
1-Blockers Phentolamine (Regitine) Lowers BP and HR of
pheochromacytoma Raynaud's diseases
(vasospasms) Erectile dysfunction
Competitive antagonist for both 1 2 receptors
Tachycardia
Prazosin Lowers BP - not widely used
BPH - relax bladder smooth muscle
1-Antagonist Decrease on total peripheral
resistance Increase in venous capacitance
Postural Hypotension Syncope - 1st full dose Favorable lipid shifts
Initiate with lower dose Give at night
Vasodilators Hydralazine Hypertension (not 1st line)
Reduce afterload in the treatment of heart failure when ACE inhibitors cannot be used
Direct SM relaxation by decrease in Ca and increase in NO
Decrease in TPR
Baroreceptors may cause tackycardia and increase oxygen usage (Blocked by B-blockers)
Immunogenic - Slow acetylators develop lupus like symptoms
Minoxidil Hypertension - drug resistant
Activates ATP dependent K channels resulting in hype-polarization and relaxation of SM
Decrease in TPR
Barrow receptors may cause tackycardia and increase oxygen usage
Tachycardia Pericardial effusion Fluid retention Hypertrichosis (xs. hair)
USE in combination with -Blockers and diuretics
Sodium Nitroprusside Hypertension Crisis - via IV
Fe-cyanide complex Increases release of NO -
Hypotension Cyanide and thiocyanate
Use only in patients with NORMAL liver
7

activates guanylcyclase cGMP relax SM
Decrease in cardiac preload and afterload
poisoning and kidney function so toxins can be metabolized and eliminated
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Nitroglycerin Sublingual - venodilatation in the peripheral, splanchic, and pulmonary vascular beds
IV or high dose –decrease afterload
Abort acute angina attacks Angian prophylaxis
Releases NO upon contact Decreased venous return
(preload) decrease volume decreased contractility decreased oxygen consumption
Slight arteriolar dilatation Dilatation of epicardial
coronary a. and of the collaterals blood flow shifts to ischemic areas even though there is a decline in overall flow
Hypotension Decrease cardiac output Syncope Headache Possible dependence CONTRAINDICTION-
Sildenafil (Viagra) - increased vasodilation effect due to increased amount of cGMP
Develop tolerance Use: sublingual,
topical, buccal, oral spray, IV
Short duration of action
Isosorbide dinitrate Angina prophylaxis Heart failure - decreases
preload
Releases NO - long acting CONTRAINDICTION- Sildenafil (Viagra) - increased vasodilation effect due to increased amount of cGMP
Sublingual, chewed, or swallowed
Sildenafil (Viagra) Erectile dysfunction Inhibits phosphodiesterase-type 5
Inhibits the degradation of cGMP - vasodilation
Increases effects of NO Hypotension
ACE Inhibitors Captopril Management of
hypertension CHF Postmyocardial infarction
not treated with thrombolytics
Ejection fraction is <40% Delay renal insufficiency
Inhibits ACE Inhibits ACE from degrading
vasodilator bradykinin Indirectly inhibits Angiotensin
II from activating PIP pathway that causes the expression of protooncogene and growth factors
Hypotension on first dose Renal insufficiency
w/arterial stenosis due to efferent arteriole relaxation, therefore decrease in GFR
Cough due to kinin concentration
Proteinuria
Reduces mortality by 25%
8

w/type I diabetes and proteinuria (Unknown)
Decreases TPR (afterload) - w/o changes to heart rate
Decreases preload
Angioedema due to increased kinin
Hyperkalemia w/renal insuffiency, w/hypo aldosteronism (occurs with patients using K sparing diuretics)
CONTRAINDICTION: Do not give to pregnant, K-sparing diuretic
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Angiotensin II Receptor Blockers
Losartan Diuretic Hypertension
Blocs binding of AII to its receptors
Vasodilator Decreases preload and after
load
CONTRAINDICTION: Do not give to pregnant
Does not cause cough Reduces mortality and
morbidity by 30% when combined with Spironolactone
Calcium Channel Blockers Hypertension (not a 1st line drug)
Arrhythmias - slows AV conduction and prolongs refractory period
Anti-Anginal
AV Block Hypotension Constipation, nausea,
vomiting Associated with
cardiovascular morbidity and mortality in hypertensive pts.
Contraindication: B-blocker (A-V block with Verapamil), Digoxin (A-V block and increased serum digoxin levels with Verapamil)
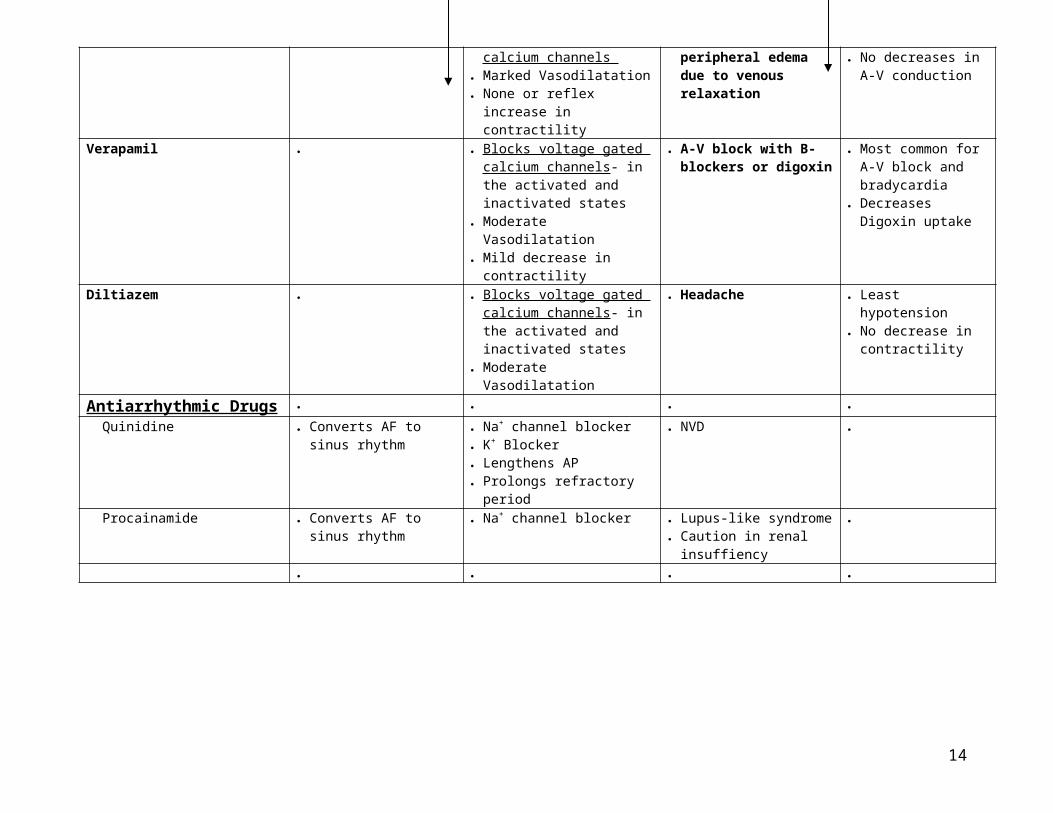
Nifedipine Blocks voltage gated calcium channels
Noncardiogenic peripheral edema due to venous
Most hypotension No decreases in A-V
9

Marked Vasodilatation None or reflex increase in
contractility
relaxation conduction
Verapamil Blocks voltage gated calcium channels- in the activated and inactivated states
Moderate Vasodilatation Mild decrease in contractility
A-V block with B-blockers or digoxin
Most common for A-V block and bradycardia
Decreases Digoxin uptake
Diltiazem Blocks voltage gated calcium channels- in the activated and inactivated states
Moderate Vasodilatation
Headache Least hypotension No decrease in
contractility
Antiarrhythmic Drugs Quinidine Converts AF to sinus
rhythm Na+ channel blocker K+ Blocker Lengthens AP Prolongs refractory period
NVD
Procainamide Converts AF to sinus rhythm
Na+ channel blocker Lupus-like syndrome Caution in renal insuffiency
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Lidocaine Ventricular ectopy Converts VT to sinus
rhythm - associated with hemodynamic instability
NOTE: not preferred over cardiac inversion
Na + channel blocker - esp. in depolarized cardiac tissue
Little effect on normal cardiac tissue - suppresses electrical activity of tissue causing arrhythmia
CNS stimulation
Toxicity - least cardiotoxic Extracardaic - Tremor and
seizures
Given IV because of extensive first pass hepatic clearance
- Blockers AF rate control Limits A-V conduction Do not use in asthma Depression
Verapamil AF rate control Ca channel blocker Limits A-V conduction
LV dysfunction AV block
Digoxin Atrial fibrillation - slows ventricular rate and increases CO (does NOT convert to sinus rhythm)
CHF
Inhibits membrane Na-K- ATPase activity - results in increase intracellular Ca
Increased myocardial contractility
Decreased intracellular K Use leads to a decrease in heart
Intoxication: Cardiac (arrhythmia) or extracardiac (fatigue, anorexia, naseua and vomiting, altered yellow-green vision, confusion, delerium and depression)
Does NOT reduce overall mortality, only morbidity
Small therapeutic index and long duration of action
Treatment of toxicity -
10

size, diuresis, decrease in blood volume and relief of edema
CNS stimulant Vagal stimulation, baroreceptor
sensitization, and sympathetic withdrawal
Encephalopathy Visual disturbances
hospitalization and monitoring - give IV K, stop digitalis, antiarrythmic drug, digoxin antibody (if severe)
Amiodarone Acute VT AND VF Long term treatment of AF
Blocks Na+ and some K+ channels
Sympatholytic Raises threshold for excitation Slows impulse conduction
Pulmonary fibrosis Liver dysfunction Thyroid dysfunction Corneal micro-deposits Skin color change
Adenosine (AMP) IV - Paroxysmal supraventricular tachycardia
Adenosine A 1 receptor agonist Directly inhibits AV nodal
conductance and increases AV nodal effective refractory period
Increase potassium conductance
Decreases cAMP induced Calcium influx
Flushing Inducing transient AV block INEFFECTIVE with the
drug theophylline - adenosine receptor antagonist
11

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
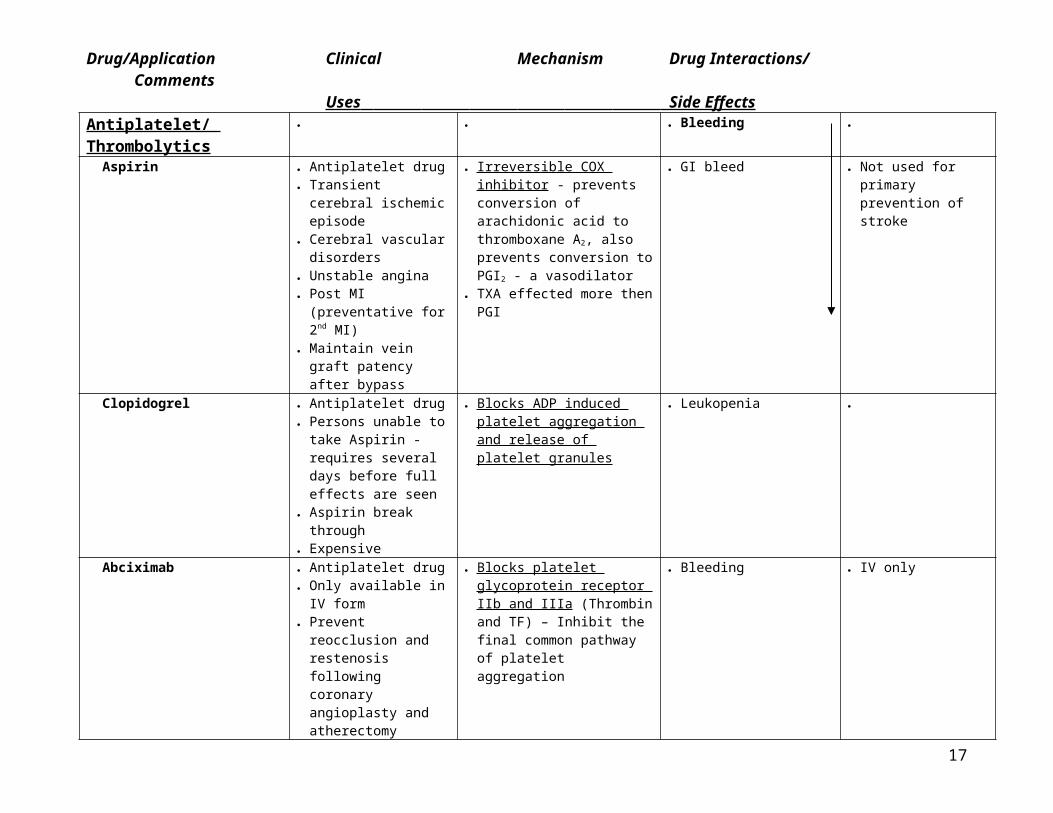
Antiplatelet/ Thrombolytics Bleeding
Aspirin Antiplatelet drug Transient cerebral
ischemic episode Cerebral vascular
disorders Unstable angina Post MI (preventative for
2nd MI) Maintain vein graft
patency after bypass
Irreversible COX inhibitor - prevents conversion of arachidonic acid to thromboxane A2, also prevents conversion to PGI2 - a vasodilator
TXA effected more then PGI
GI bleed Not used for primary prevention of stroke
Clopidogrel Antiplatelet drug Persons unable to take
Aspirin - requires several days before full effects are seen
Aspirin break through Expensive
Blocks ADP induced platelet aggregation and release of platelet granules
Leukopenia
Abciximab Antiplatelet drug Only available in IV form Prevent reocclusion and
restenosis following coronary angioplasty and atherectomy
Blocks platelet glycoprotein receptor IIb and IIIa (Thrombin and TF) – Inhibit the final common pathway of platelet aggregation
Bleeding IV only
Dipyridamole Antiplatelet drug Combined with aspirin
Inhibitor of adenosine uptake Weak inhibitor of
phosphodiesterase - increases cAMP
12

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Streptokinase Thrombolytic drug MI (w/in 6 hrs of pain) Stroke (w/in 3 hr of
symptoms) Arterial Thrombus Infused parenterally $200
Noon-enzymatic protein Activates the fibrinolytic system Forms Plasminogen-
streptokinase activating complex to convert plasminogen to plasmin. Plasmin break fibrin.
Risk of bleeding CONTRAINDICTIONS: hx
of peptic ulcers, IDDM, internal bleeding, CVA, recent surgery or trauma, brain tumor, aneurysm, bleeding diathesis, age over 70, or uncontrolled severe HNT
Prolongation of PT or APTT indicates lytic state
Follow by use of heparin
t-PA Thrombolytic drug $2000
Converts plasminogen to plasmin. Plasmin break fibrin
t-PA selectively binds to bound fibrin-plasminogen
Releases plasmin – systemic fibrinolytic
Not used to treat: DVT or PE
Prolongation of PT or APTT indicates lytic state
Must be followed up with Heparin
Anticoagulants Heparin - Injection Hemodialysis
Cardiopulmonary bypass DVT (IV) and DVT
prevention (subcu) PE and PE prevention
SEE BELOW Hemorrhage Thrombocyopenia Arterial thromboembolism Hypersensitivity Osteoporosis
Monitored by APTT of >50 sec and PTT - heparin plasma [0.2 - 0.4 U/ml)
IV Only Does NOT cross
placenta Unfractionated (UFH) Initial treatment for
DVT PE
Enhances antithrombin III and IIa, which deactivates Thrombin and Factors Xa and Iia
Short half-life (0.5 - 1 hour)
Heparin induced thrombocytopenia (HIT) - Activates antiplatelet Ab (IgG) that activate platelets via their Fc Iia receptors
OK for breast feeding or pregnancy
Widespread binding - unpredictable
Low molecular weight(LMWH)
Subcutaneous b.i.d DVT - prophylaxis Venous
thromboembolism
Enhances antithrombin IIIa only , which deactivates factor Xa more than Iia
Long half-life (4 - 6 hours) Eliminated in kidney
Spinal or epidural hematoma
Less likely: HIT, but if already HIT DON’T use
Predictable ↑ ½ life, ↑
bioavailability
13
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Warfarin - Oral DVT - begin during heparin treatment
PE - begin during heparin treatment
Atrial fibrillation Acute MI Valvular heart disease Recurrent systemic
embolism
Interferes with vit K therefore reducing factors VII, IX, X, and Thrombin
Long duration (35-45 hrs) Metabolized by cytochrome
P-450
Hemorrage Teratogenic - CROSSES
placenta CONTRAINDICTIONS:
Rifampin - increases metabolism; Nafcillin - loss of activity; alcohol - chronic: decrease activity, acute: increased; Metronidazole, trimethoprim, and sulfamethoxazole - decreases metabolism of S isomer; Amiodarone - decreases metabolism of S and R isomer; Aspirin - risk of bleeding
½ life 35-45 hrs Therapeutic delay (3-4
days) PT or INR 2-3 Treat OD with Vit K
Protamine Sulfate Reversal of Heparin's (LMWH) actions
Basic protein that binds the acidic heparin to for a stable compound
Partially reveses the anti-factor Xa activity
Vitamin K Reverse warfarin's anticoagulant effects
In the process of carboxylation of Factors Vii, IX, X and thrombin, vit. K is oxidized to am epoxide - a required step
Pulmonary All 2 agonists Palpitations 2 dilation
which leads to barrow receptors increasing HR
Tremor – caused by stimulation of 2 in skeletal muscles - Na-K ATPase causing hypokalemia
Asthma:o 1) Mild-Albuterolo 2) Low dose ICSo 3) Low - Med dose
ICS + LABAo 4) High dose ICS +
LABACOPD:o 1st line- B agonist +
anticholinergic bronchodilators
o Symptomatic -ICSo Acute exacerbation
-inhales B agonist and anticholinergic, plus systemic CS
14

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Abuterol (metaproterenol) Bronchodilator - inhalation
Acute attacks
2 Agonist Activates adenylyl cyclase
increased cAMP PKA relaxation of smooth muscle
Duration of action 3 - 6hr
Tremors - B2 receptors on skeletal muscle
Palpitations - B2 receptors on peripheral vasculature vasodilatation reflex- increased cardiac force and rate of contraction
Hypokalemia - stimulate K+ uptake by skeletal muscle via muscle Na-K-ATPase pump cardiac arrhythmias
Salmeterol Bronchodilator - prevention of attacks, b.i.d.
Long Lasting B2 Agonist Long duration >12 hrs
Should NOT be repeated for acute attacks
Theophylline (Caffeine) 2nd line therapy for COPD and asthma
Must be monitored 5-15 mcg/ml therapeutic
range; 30 mcg/ml toxic range
In elderly and pts. with COPD - max 12 mcg/ml
Methylxanthine compound Unclear mechanism - results in
smooth muscle relaxation, improved diaphragmatic contraction, and increased mucociliary clearance
Some anti-inflammatory effects Well absorbed for GI tract Volume of distribution: 0.5L/KG - 1mg/kg increases 2mcg/ml Clearance varies among and
within individuals - cleared by cytochrome p450 in liver
Common side effects- nausea, tremor, HA, agitation, and insomnia
Severe toxicity > 30 mcg -Seizures, arrhythmias
Conditions that decreased elimination: CHF Liver disease Cor pulmonale -
increased pulmonary a. pressure
Ciprofloxacin ErythromycinConditions that increase Elimination Smoking
Corticosteroids Asthma COPD Rhinitis - use topically See below for specifics
Binds to GC receptor in cytoplasm and enters nucleus
Forms homodimer and binds to GRE - results in transcriptional regulation of specific target genes
See below for specifics
15

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Prednisone COPD - acute excerbations
Asthma Give twice dailyGood on: Sneezing Rhinorrhea Pruritis Nasal Blockage
Oral corticosteroids - systemic Binds to GC receptor in
cytoplasm and enters nucleus Forms homodimer and binds to
GRE - results in transcriptional regulation of specific target genes
CHRONIC EFFFECTS Adrenal insufficiency Glucose intolerance Osteoporosis?Compression
fractures Myopathy - esp. quads Osteonecrosis Cataracts Glaucoma Psychosis Cushingoid appearance Obesity Hypokalemia Immune Suppression/
infection Purpura Delayed wound healing In children - stunted growth
Inhaled w/precautions avoid most if not all side effects
20% reaches respiratory tract when inhaled
Osteoporosis is treated by bisphosphonate /Ca+
+
Beclomethasone 1st line therapy in asthma Symptomatic COPD -
chronic use <800 micro g / day no
problems <1600micro g/day no
adrenal problems
Inhaled corticosteroid - same mechanism as above
20% of inhaled steroid reaches lung and absorbed into body
Limited systemic effects Oropharyngeal candidias
(thrush) Dysphonia (hoarseness) In children - stunted growth
Use of spacer limits amount deposited in the oropharynx (nl. up to 80% deposited) or with rinsing mouth
Chromolyn and Nedochromil Inhalation ProphylacticOK on: Sneezing Rhinorrhea Pruritis Nasal Blockage
Not well defined - prevents degranulation of mast cells, t-lymphocytes, eosinophils, and macrophages
Anti-inflammatory effects Improve bronchial
hyperresponsiveness Protects against
bronchoconstrictive stimuli
None
16
Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Ipratropium COPD w/o dryness, bronchial dilation
Rhinitis
NO CNS Muscarinic antagonist Decreases vagal tone - the
important bronchoconstrictor mechanism
Onset (15 - 30 min), peak (1 - 2 hrs), duration (6 - 8 hrs)
Nasal administration - blocks rich parasympathetic innervation of mucosa - decrease secretion
Do NOT block the direct effect of various mediators in asthma that act directly on airway smooth muscle
Effective in pts. With COPD
Muscarinic antagonist + B aginist = 1st line defense in COPD
Montelukast (Accolate) Leukotriene receptor antagonist Antihistamines Good on:
Sneezing Rhinorrhea Pruritis NOT nasal congestion
H1 receptor antagonist 1st generation blocked muscarinic receptors causing sedation and anticholinergic effects (dry mouth, urinary retention)
2nd generation selective w/o sedation of sedation
Diphenhydramine (1st Gen) Benadryl Blocks rhinitis, uticaria,
eczema
H1 blocker Muscarinic receptors blocker CNS
Sedation Anticholinergic side effects
Terfenadine (2nd Gen) Relief of allergic rhinitis Blocks H1 receptors Blocks delayed rectifiers –
voltage gated K channels Metabolized By CTY450 3A4 to
fexophenadine (the H1 active metabolite - Allegra)
NO CNS
Torsades de pointes - due to blocked delayed rectifier channels (prolonged QT interval and Ventricular Tachycardia)
Block metabolism: Ketoconazole Itraconazole Erythromycin Clarithromycin
Decongestions Good on: Nasal Blockage
1 2 Agonist
Phenylephrine 1 2 Agonist Increase BP due to fluid retention
Insomnia Not used w/MAO
inhibitors Caution w/BPH
Pseudoephedrine Common in OTC oral Vasoconstrictor 1 2 agonist
Not used w/MAO inhibitors
17

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Oxymetazoline (Afrin) Nasal sprays 1 2 agonist topical vasoconstriction
Rebound congestion with prolonged use
Rhinitis medicamentosa - Chronic rhinitis, secondary hyperemia, tachyphylaxis, and mucosal irritability
GI Drugs Erythromycin Increase intestine motility
Antibiotic Motilin agonist - prokinetic
effects Diarrhea
Kaolin/ Pectin (Kaopectate) Makes solid stool Forms clay in lumen Does not stop fluid loss Cimetidine (Tagamet) Decrease acid secretion
Peptic ulcer disease (no longer used)
Parietal cell H2 Blocker - inhibits both basal and meal induced acid secretion
Short duration of action (4 -6 hrs)
Mental confusin Antiandrogenic effects -
decreased libido, gynecomastia
Metabolized by CYP450 - decreases metabolism of other drugs inc. coumadin and diazepam
Ranitidine (Zantac) Peptic ulcer disease Decrease acid secretion Stage I and II GERD
H2 Blocker Long duration of action - Lasts
12hrs
No significant side effects
Loperamide (Imodium AD) Diarrhea Opioid receptor agonist Poor CNS penetration Increases mixing contractions Decreases motility
Do NOT give to treat diarrhea induced by infections with invasive organisms
Metoclopramide Diabetic gastroparesis Antiemetic For constipation
Dopamine Antagonist (D 2) Seratonin Agonist (5-HT 4)
Misoprostol Adjunct therapy for peptic ulcer disease
NSAID gastric ulcers
Prostaglandin receptor agonist - In parietal cells (opp. happens elsewhere) inhibit adenyl cyclase stimulated by histamine indirectly acid secretion
Also, protect mucosa damage induced by acid, alcohol, and NSAIDS (aspirin)
Diarrhea - secretory Uterine stimulation (avoid
during pregnancy) Do NOT give - IBS pts.
Marked for co-administration with anti-inflammatory - prevent side effects
18

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Sucralfate (Carafate) Stress/ Peptic ulcers Mucoprotective
Basic aluminum salt - 3 actions:- Complexes with proteins and forms a protective layer over ulcer site
- Decreases back-diffusion of H+ ions - Binds pepsin and bile salts
Non-toxic Constipation, diarrhea,
nausea, dry mouth, etc.
Omeprazole (Prilosec R and S isomer /Nexium - S isomer)
Peptic ulcer disease - inhibits both basal and meal induced acid secretion
Esophagitis Stage II and III GERD
Proton pump inhibitor Irreversible H+, K+ pump
inhibitor - inhibits gastric secretion
Need low pH to be active 24-48 hour action Metabolized by CYP2C and
CYP3A
Gastric hyperplasia due to oversecretion of gastrin (?) (linked to gastric cancer in animals)
Given with Amoxicillin to treat H. Pylori - 80% effective
Bismuth (Pepto Bismol) Diarrhea - esp. microorganism caused
Inhibit toxin-induced formation of prostanoid substances in intestinal mucosa
Prophylactic Treat
Diphenoxylate Diarrhea Opioid agonist CNS
Overdose- respiratory deprssion
Treat OD with naloxone Do NOT give to treat
diarrhea induced by infections with invasive organisms
Mixed with Atropine to deter abuse
Magnesium Hydroxide Antacid - Stage 1 GERD Laxative Pro osmotic
Weak base that neutralizes acid Non-systemic Rapid onset Raises intragastric pH to 8 - 9
Increased acid secretion Laxative (con when used as
an antacid) Xs. can induce muscle
weakness and fatigue
Propantheline Decrease acid secretion Anticholinergic Cholestyramine Diarrhea Binds osmotically active agents Endocrine Drugs Lispro Insulin Injected prior to meal Insulin analog - with penultimate
and antepenultimate (pro-lys) AA at carboxy-termainal end have been reversed (lys-pro)
Fast acting, high peak, and short duration
Subcutaneous
19

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Tolbutamine Type 2 diabetes Sulfonyureas - promote first phase insulin releas
Potentiate the effects of insulin in target tissues (action at post-receptor level)
Decrease hepatic glucose output Half-life = 6 hrs Liver metabolism
Hypoglycemia From sulfa antibacterial drugs
Oral
Metformin Hyperglycemia Biguanide drug Reduces hyperglycemia by
decreasing hepatic glucose output - blocks hepatic glucose production
Increases peripheral uptake and metabolism of glucose
Takes 1 -2 weeks to decrease hyperglycemia
Renal excretion
Diarrhea Loss of appetite Nausea Rare - lactic acidosis
Oral
Acarbose Reduce sugar absorption Inhibits intestinal disaccharidase enzymes
Retards absorption of sucrose and starch in the intestine
Gas productin Oral
Rosiglitazone Type 2 diabetes Anti-hyperglycemic agent
Thiazolidinediones - sensitizes peripheral tissues to insulin
Enter nucleus, and bind the gamma subunit of the portein regulator PPAR, which modifies gene transcription of the glucose transporter
Also decrease hepatic glucose production
Weight gain Liver function abnormalities
- check
Oral
Propylthiouracil Overactive thyroid gland Antithyroid - block the organification of iodide
Decreases the peripheral conversion of T4T3
I-131 radioiodine Persistent hyperthyroidism
Induces radiation injury to the cells - occurs gradually over wks - mo
Hypothyroidism - give thyroid
CONTRAINDICATION: pregnancy - destroy fetus thyroid
20

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Parahormone Diagnostic test - distinguish pseudohypoparathyroidism from hypoparathyrodism
Increase bone density in osteoporosis (not yet in US)
Acts like parathyroid hormone - promotes intestinal and renal absorption of Calcium, and Ca resorption from bone
Injection
Calcitonin Hypercalcemia Paget's disease Osteoporosis
Decreases calcium and phosphorus resorption from bone
Subcutaneous Nasal spray
Dihydroxycholecaciferol Renal enzyme deficiency to convert vit. To active form
Convert vit. D to active form
Etidronate Paget's disease Osteoporosis -
intermittent treatment (2 wks q 3 mo)
Diphosphonate - decreases bone resorption
Oral
Alendronate Osteoporosis - qd before breakfast with water
Diphosphonate - decreases bone loss
Gastrointestinal Epigastric pain
Clomiphene Citrate Anovulation - given 5 day courses to induce ovulation
Estrogenantagonist - causes reflex stimulation of GnRH that leads to LH surge ovulation
Bromocriptine Prolactin tumors Prolactine overscretion Acromegaly
Dopamine superagonist - suppresses secretion and growth of prolactin secreting cells
InhibitingGH secretion
Nausea
Raloxifene (Evista) Osteoporosis Estrogen receptor modulator - inhibits bone resportion and turnover
Do NOT use - hx. of DVT
Mifepristone (RU 486) Postcoital contraception Abortion in early
pregnancy
Synthetic steroid - inhibits progesterone receptors
For abortion - follow with prostaglandin after 48 hours
Hydrocortisone 1 or 2 adrenal insufficiency
Congenital adrenal hyperplasia
Cortisol - increase gluconeogenesis, potentiation of effects of lipolytic agents, improve stress response
Cushing like symptoms Oral or parenterally
Prednisone Treat diseases with strong inflammatory reactions
Glucocorticoids - potent glucorticoid effects
Longish duration of action Very potent
HTN Hypokalemia Edema
21

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Dexamethasone Decrease cerebral edema Diagnostic agent to
suppress endogenous secretion of mineralcorticoid activity
Potent glucocorticoid Long duration of action
See above
9-fluorohydrocortisone Aldosterone replacement Very potent mineralcorticoid - adrenocorticoid analog
125 times more active than hydrocortisone
Metyrapone Diagnostic test of pituitary, eliciting a compensatory ACTH release, which is reflected in increased 11-deoxycortisol in plasma and urine
Inhibits 11-beta-hydroxylation in adrenocortical cells
Decreases hydrocortisone production
Cholestyramine an Colestipol Decrease plasma LPL High molecular weight Ion- exchange resins that bind bile acids in intestine
Forces the formation of new bile acids from cholesterol
Nausea, vomiting, constipation, and steatorrhea
Reduced absorption of compounds that depend on bile acids - fat soluble vit, thyroid hormone, iron, digitalis, thiazide diuretics, tetracycline, and anticoagulants
Mix with water or fruit juice - give before meal
Atorvastatin (Lipitor) Lower LDL levels Lower VLDL
HMG-CoA reductase inhibitor Increased synthesis of the LDL
receptor - esp. in liver
Liver and muscle enzyme elevations
Side effects increase with Cyclosporin, nicotinic acid, an fibric acid derivatives
Gemfibrozil Decreased VLDL production
Not known -lipid regulating drug Decreases hepatic uptake of FFA
and decreases synthesis of triglyceride and of VLDL carrier apoprotein
Increases plasma HDL
Gastrointestinal Liver function abnormalities
- check
22

Drug/Application Clinical Mechanism Drug Interactions/ CommentsUses Side Effects
Nicotinic acid Familial hypercholesterolemia elevated VLDL and IDL levels
Unknown - B- group vitamin Lipid lowering properties Decreases hepatic synthesis of
triglycerides Augments fecal excreting of
neutral sterols (cholesterol end-products)
Decreases adipose tissue lipolysis
Enhanced lipoprotein lipase activity
Incresed HDL levels Decreases VLDL, LDL and
TAG
Cutaneous flushing Pruritis Side effects treated with
NSAIDS Provoke cardiac
arrhythmias Liver function abnormalities GI - heartburn, nausea, and
diarrhea Increased serum uric acid gout
Impaired glucose tolerance
Overall lipoprotein reduction is 10 - 15 %
Combine with resins treatment
23