drug toxicity & reproductive toxicology
TRANSCRIPT
Drug Toxicity & Reproductive Toxicology
byDr. Willis Ochieng
Toxicologist 0733871261

Outline of the Course
Drug Toxicosis Toxicoepidemiology Toxicity, Safety and efficacy of drugs Adverse drug reactions and their causes Adverse drug reactions and their prevention
Developmental Toxicosis
Toxicoepidemiology
Toxicoepidemiology Toxicoepidemiology is application of epidemiological
methods to the problem of acute poisoning› The best in addressing deficiencies in knowledge of poisoning
There is little hypothesis-testing clinical research in toxicology. Randomised clinical trials are rare for ethical reasons › Most observational studies are performed on highly selected
patients and are subject to marked bias› The approach is based almost entirely on deduction from
Known pharmacological and toxicological effects Generalisations from drugs within the same therapeutic class The collection of data on human poisoning is facilitated–
By non-fatal overdoses admitted in hospitals By legal requirements that deaths due to poisoning be reported to police
Fatal and clinical data obtained from reasonably defined populations makes it possible to identify differences in the severity and spectrum of toxicity between and within drug classes
Iatrogenesis
Iatrogenesis Poisoning is either by an overdose or as a
manifestation of excessive toxic side effects Prior to 1930, there were very few efficacious and
specific drugs available to a physician. Safe treatment was therefore difficult
Around 1930 the philosophy of the "magic bullet" of Ehrlich led to the concept of selective toxicity leading to the proliferation of many and safe drugs
The number in market has led to other toxicological problems necessitating need for a safety/efficacy evaluation prior to licensure of new drugs
Even with this safety evaluation effort, drug toxicity is still an issue
Safety & Efficacy of Medicines
Safety and Efficacy of Medicine
Most drugs are selectively-toxic chemicals and only a few drugs exhibit a single pharmacological or physiological effect
Adverse side-effects are properties of drug - patient- environment interactions and therefore no drug can be absolutely safe for all patients.
Drugs confer benefit. But, the benefit/risk ratio should be acceptable to the individual patient but not for all
Side-effects of drugs are therefore the result of many complex interactions between the drug, the patient and the patient's environment.
Drugs which are perfectly safe for most patients may not be quite as safe for certain individual patients
Drug Toxicity-Metabolism
Drug toxicity
Most drugs and other chemicals undergo metabolism in the body; basically a detoxification.
This may lead to formation of toxic intermediates with adverse drug reactions and also activate chemicals to form toxic derivatives
Well-nourished tissues have a highly effective chemical defence system which protects against the toxicity of these intermediates such as oxygen radicals› Toxicity results only from major overdose, or prolonged
exposure at lower dosage, or from nutritional deficiency Toxicity may be manifested in any different ways
including-- Acute effects that may lead to necrosis of the liver and kidney, Subacute effects leading to gastrointestinal ulceration, Chronic effects may lead to malignancy, effects on reproduction
and other organs in the bodyIdentification of Adverse Drug Effects
Adverse drug reactions and their causes-1
Adverse reactions may be identified by Clinical trials Doctor’s observations Hospital drug surveillance programmes (toxicovigillance) Cohort studies including post-marketing surveillance and
monitoring Case-control studies (study of disease cases for drug association) Epidemiological studies of disease statistics
Of the adverse reactions known many are the result of the intrinsic toxicity
Where the therapeutic ratio is low, adverse side-effects are common
The adverse reactions in these cases are the results of an extension of their therapeutic activities, and might also be considered as a consequence of overdose
Causes of Drug Effects-Homosapiens
Adverse drug reactions and their causes-2
It is generally assumed that all patients are the same and require identical dosage regimes for any given drug
Homo sapiens are genetically one of the most heterogeneous animal species
The efficacious dose for a given human population is taken as the dose producing the desired therapeutic response in the least responsive patients
This means generally, that all patients receive an efficacious dose, but a substantial number of patients receive an unnecessarily excessive amount of the drug
Most drugs, the higher the blood concentration, the greater the therapeutic benefit but the probability of adverse side-effects is also increased.
Causes of Drug Effects-Individual Metabolic Variations
Adverse drug reactions and their causes-3
The rates of metabolic deactivation, detoxification, and excretion of drugs vary widely from individual to individual
Some individuals may be particularly sensitive to certain medicines because they are deficient in the enzymes that normally effect deactivation.
As genetically-determined variations in drug response (pharmacogenetics) can be assessed by a variety of methods, adverse drug reactions due to such factors may now be averted
Causes of Drug Effects-Age
Adverse drug reactions and their causes-4
Over the age of 70, the enzymes that metabolically deactivate and detoxify drugs, and the various physiological processes involved in the excretion of drugs in the urine and bile are less efficient
There is a general tendency for aged patients to exhibit an increased pharmacological response from a given dose of a drug, and also to show an increased incidence of adverse side-effects.
Causes of Drug Effects-Interactions
Adverse drug reactions and their causes-5
There is a complex series of interactions between one drug and another and between environmental chemicals, etc, which may alter the metabolic deactivation of drugs and lead to—
To a heightened or diminished pharmacological effect, and to alterations in therapeutic activity
Many patients receive several drugs simultaneously as many as eight different drugs during hospitalisation
In addition, many patients are smoking, taking alcohol, and eating foods that contain substances, which might interact with the drugs prescribed
Causes of Drug Effects-Enterohepatic Circulation
Adverse drug reactions and their causes-6
Most drugs are rapidly metabolised and the unchanged drug and its metabolites are excreted in the urine or bile
Some of these drugs may undergo enterohepatic circulation
Elderly patients, with impaired detoxification and excretory functions, and prone to constipation are at most risk of accumulation of drugs in the liver by enterohepatic circulation
Causes of Drug Effects-Malnutrition
Adverse drug reactions and their causes-7
Repeated administration of many drugs makes excessive demands on the body's reserves and especially on its nutrition.
Malnutrition decreases the activities of the drug-metabolising enzymes and the concentration of intracellular protective materials, such as glutathione, with concomitant increases in the toxicity of many drugs
Causes of Drug Effects-Empirical
Adverse drug reactions and their causes-8
The safety evaluation of drugs is still largely an empirical procedure, with most of the toxicity evaluation being carried out in experimental animals
It is extremely difficult to make any scientifically-based risk assessment for man from animal toxicity studies
Prevention-1

Adverse Drug Reactions and their prevention-1
The obvious ways to minimise the adverse side-effects of drugs is-
Extend the pre-marketing human studies, to comprise clinical and pharmacokinetic investigations in a wider patient population including the elderly.
Phase out the marketing of new drugs, with appropriate monitoring of safety and efficacy,
Prescribe drugs for a finite period, and review a patient's drug prescriptions periodically to ensure no unnecessary prescription, and no obvious dangers from drug interactions
Prevention-2
Adverse Drug Reactions and their prevention-2
Individualise dosage, especially for elderly patients
The great majority of adverse drug reactions are dose-related and occur in patients taking standard doses of medications
These facts suggest that for many patients, standard drug doses may be excessive
Prevention-3
Adverse Drug Reactions and their prevention-3
Pharmacotherapy in the elderly should be based on age-dependent changes in function and composition of the body
Aging is characterised by a progressive loss of— Functional capacities of most if not all organs Reduction in response to receptor stimulation and homeostatic
mechanisms Loss of water content and an increase of fat content in the body.
The most important pharmacokinetic change in old age is a decrease in the excretory capacity of the kidney
The elderly is considered as renally insufficient patients The decline in the rate of drug metabolism with advancing age
is less marked
Developmental Toxicosis-History
Developmental ToxicosisHistory
In 1920s some defects were already known which had associations with-
Anophthalmia with hypovitaminosis Teratorata in rodents due to hypervitaminosis
Before the thalidomide disaster of the 1950s, people believed that congenital malformations were due to genetic causes only
This disaster proved that there was a part played by the environmental chemicals
With increasing foetal exposure to environmental chemicals and drugs and other xenobiotics during pregnancy teratogenic association became clear
Principles of Teratology-Definition
Basic Principles of Teratology-1
Developmental toxicology encompasses the fields of teratology “teras and logos” and transplacental carcinogenesis. There are six basic principles of teratology-› Genotype of the embryo or foetus interacts with the
environment influences teratogenicity› Stage of development of the embryo or foetus, at the time of
exposure, determines its susceptibility to teratogenic agents› Teratogens induce abnormal development according to specific
mechanisms› Death, malformation, deformation, intrauterine growth
retardation, and postnatal functional abnormalities are manifestations of teratogenesis
› Physiological properties of teratogens determine the access to the embryo or foetus
› Teratogenicity shows a dose-response relationship
Incidence of Congenital Anomalies
Incidence of Congenital Anomalies
Congenital defects are the main cause of perinatal mortality and postnatal morbidity in humans
The fifth leading cause of death before the age of 65 years
Incidence of human morphological abnormalities is 2-3% of births per year in most western countries
Only 30%-40% have known aetiology If stillbirths are included the incidence may be as big as 15-18% If we include neonates with functional defects, the incidence of
such abnormal function may approach 6-7% in 3-4 year old kids The overall incidence of abnormal development in
humans is very high
Impact on Morphological Developments
Drugs effects on Morphological Development
A process of morphogenesis includes morphogenetic movements, cell contacts, tissue interactions (inductions), and cell differentiation
Despite of rapid changes occurring during fertilization and blastocyst formation, teratogenesis cannot occur
Since the cells are totipotent, the blastocyst either dies or replenishes its compliment of cells following injury by chemicals
Gastrulation is the earliest stage of embryo development Teratogenic insult on this embryo is still very low Response to toxic insult is embryonic death and resorption, not all cells are
totipotent Organogenesis is most complex stage of development and most
adversely affected by exposures to exogenous chemicals Restriction is the loss of developmental plasticity that takes place when
cells have undergone determination or commitments to a final pathway of differentiation culminating into histogenesis
This is the maturation of differentiated cells into a fully functional condition Time of functional maturation depends on the organ system Pertubation of these maturation processes will not lead to morphological
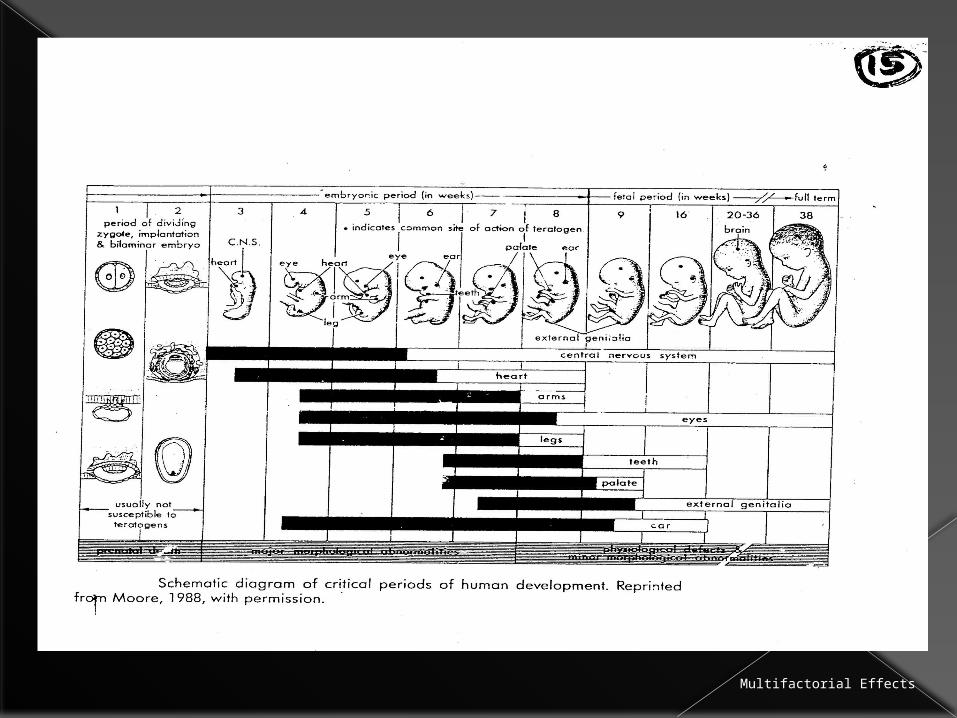
abnormalities BUT may manifest as functional aberrations.Fig. Showing Most Critical phase
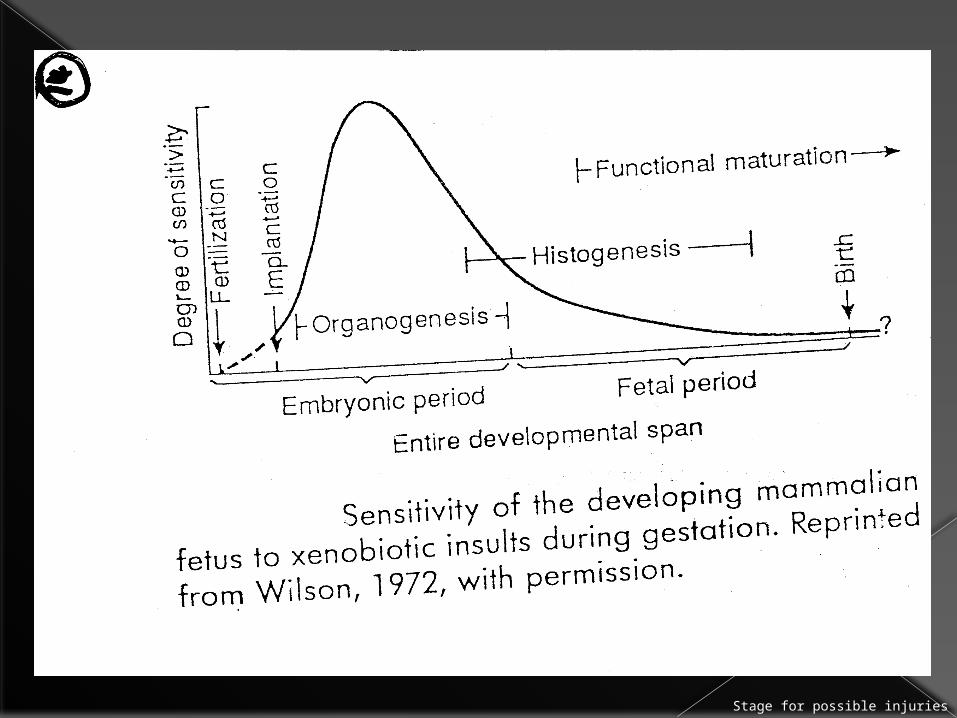
Stage for possible injuries

Predisposing Factors-1 Developmental toxicity depends on the stage of
embryonic development and factors that modify the toxicity of the xenobiotic.
These factors are: › Foetal genotype › Parental and genotype› Critical time is that time when embryo or foetus has the
greatest sensitivity to toxic influences Each organ or organ system has its specific critical
time. › A malformed organ cannot result from an exposure to a
toxic agent occurring after an organ has been fully formed at the time of exposure.
› One cannot make above statement in the case of a deformation Fig. Showing Critical Times
Multifactorial Effects
Predisposing Factors-2 Multifactorial threshold Concept: Cleft lip, cleft palate, spina bifida,
hypertrophic pyloric stenosis, clubfoot, congenital hip dislocation and certain cardiac malformations have mulfactorial causes
The action of teratogens require the embryo or foetus to be genetically predisposed to a malformation. Teratogens act only as modifying factors in the expression of the defect
For each organ the threshold for abnormal organogenesis exists, surpassing which will result in a malformation (dose response)
Embryonic and foetal pharmacokinetics: Hepatic enzyme activities are approximately the same as in the adult on a body weight basis
Foetal drug metabolism produces either toxic or nontoxic metabolites Since these metabolites are water soluble, they may accumulate in the foetal
compartment due to its higher water content Fortunately detoxification reactions tend to predominate over activation reactions Enzyme induction may occur in the foetus and alter the drug effect in the foetus
Foetal renal excretion aids elimination of xenobiotics especially the later stage of gestation
GFR increases with a concomitant increase in foetal drug clearance Preferential tissue binding of some teratogens (thalidomide) to
embryonic and foetal tissue may occur resulting into higher concentrations of the teratogen in foetus than in maternal blood
Sequestration is due to relative high water content and immature blood-brain barrier which may allow entry of neurotoxic agents in foetal brain Maternal Physiological State Effects
Predisposing Factors-3 Maternal physiological state may alter
homeostasis between the mother and the foetus
The impact must be severe enough to affect the foetus since the needs of the foetus are usually met at the expense of the mother
Hyperthyroidism in the mother may be severe enough to cause foetal goiter and tracheal obstruction
Hypothyroidism may lead to foetal cretinism, deafness and mental retardation
Malnutrition may lead to nonspecific abnormal development resulting in abortion, stillbirths, neonatal deaths and neural tube defects
Protective Pharmacokinetics
Predisposing Factors-4Maternal pharmacokinetics may have protective effect in the foetus following an exposure to a xenobiotic for the following reasons—› Absorption decreases during pregnancy partly due
to reduced GIT motility and decreased GIT metabolism of substances
› Vd increases during pregnancy due to increased total body water and body fat
› Renal clearence increases with pregnancy due to increased renal blood flow leading to increased GFR
Reasons above lead to decreases in the concentration of blood-borne xenobiotics and hence act as safe guard against foetal toxicosis
Toxcic pharmacokinetics
Predisposing Factors-5 Maternal pharmacokinetics may also cause
toxicosis in the foetus for the following reasons—› Progressive decrease in plasma albumin
concentration due to increasing plasma volume may affect plasma protein binding as a result of the increasing endogenous binding displacers such as non-esterified fatty acids.
This may raise up the blood levels of the available poisons or xenobiotic with a consequent foetal toxicosis.
› Maternal hepatic enzymes increases during pregnancy perhaps to cope up with excreted foetal waste.
However, oestrogen inhibits some pathway of the synthesis of some of these enzymes and may reduce the metabolic capacity
whereas progesterone may induce their biosynthesis. It thus depends very much on the agent in exposure.
Response to Foetal Toxicity
1.0 Response to foetal toxic injuries
Cytotoxicity can lead to Death, Malformation and Growth retardation
Focal or diffuse cell death results in focal or diffuse lesions
Inflammatory response to necrosis is unlikely to occur until the later half of gestation
Before this time the immune system is still immature. Plasticity of the early embryo allows for
compensatory growth after nonlethal exposure Attempts at repair often follows which ends in
congenital anomalies—deformations DEFORMATIONS exemplified by intestinal atresia as a
result of fibrosis following ischaemic bowel injury
Embryonic Faetal Death

1.1 Embryonic/Foetal Death Embryonic death--
Approximately 50-70% of all conceptuses are lost during the first 3 weeks of pregnancy
By the end of pregnancy 78% will die due to severe morphological abnormalities
Ten times more malformed foetuses are born dead than alive
Chromosomal anomalies are apparent in 60% of abortuses at less than 12 weeks of gestation
Terathanasia-- Riddance of dead or deformed nonviable embryos and
fetuses Mortality does not stop at birth--
Human babies (8%) with major malformations die during the neonatal period and early childhood
Mechanism of Defect Formation
1.2. Mechanism of Defect Formation
Cytotoxicity is a mechanism of defect formation› The most susceptible cell populations are those with high
proliferative rate and those beginning to differentiate› DNA sensitivity is due to genome exposure and is most likely to
be damaged by xenobiotic injury› Correlation between incidence of embryonic death and cytotocity
is not always apparent Because cytotoxic effect may be counterbalanced by embryonic
regeneration
› Eg., excessive cell death has a dramatic effect on limb development–
May lead to too few cells with a consequent limb reduction eg. cyclophosphamide exposure.
May lead to limb defect (thalidomide) because it affects mesonephric mesenchyme which is the inducer of limb tissue hormone
Cell death
1.3 Mechanism of Defect Formation cont--
Cell death (PCD) is needed for– Separation of digits Limiting size of digits Decreasing superfluous neurons Degeneration of primitive structures
PCD may be induced by lysosomal activity or altered nuclear activity through local, hormonal or chemical messages
Eg., Apical ectodermal maintenance factor, released by necrotic mesodermal cells may cause polydactyly in offsprings
Reduced Proliferative Rate
1.4 Reduced Proliferative Rate Reduced proliferative rate can occur
following a dose of a teratogen lower than that which induces cytotoxicity allowing regeneration to occur causing only growth retardation of the structure
Growth retardation of organ may have severe consequences(Eg. If dental anlagen is not of sufficient mass, teeth may
not develop)
Reduced proliferative tissues during histogenesis may cause abnormal differential growth rates, with later defective development
Failed Cellular Interactions
1.5 Failed Cellular Interactions
Cause may be genetic or toxic or both › Toxic agent in the absence of abnormal gene
may lead to absence cell induction to recognize other cells (Actinomycin D)
› Hypovitaminosis A causes disruption of spatial orientation of messenchymal cell condensation through altered cell adhesion molecule characteristics with the consequent malformed cartilage
A genetic anomaly may lead to aberration in the mobilization of the factors needed in cell interactions
Impeded Morphogenetic Movements
1.6 Impeded Morphogenetic Movements
Cellular migration can be impeded by decreased mobility of cells, altered quantity or quality of the extracellular matrix (ECM)
ECM is composed of glycoaminoglycans—hyaluronic acid, chondroitin, chondroitin sulphate, heparin sulphate, keratin sulphate and heparin—and collagen.
All these interact with integrins allowing movement or adhesions among tissues in directional planes.
Higher levels of hyaluronic acid during morphogenesis encourage cell migration by increasing cell proliferation, inhibiting aggregation which increase fluidity of ECM
During differentiation hyluronic acid levels decrease after increased aggregation of cells due to chondroitin production
Teratogens (cortisone) disrupts glycoaminoglycans and collagen synthesis resulting in reduction and sulphation of ECM components
Microtubules and microfilaments function can be affected through alterations in synthesis and turnover. Colchicine, etc do that
Calcium is an essential cation for the function of microtubules and microfilament function chelation (EDTA) of which may induce heart malformations if done during critical period of organogenesis Reduced Biosynthesis

1.7 Reduced Biosynthesis of Essential Components
Alterations in the biosynthesis of DNA, RNA, proteins, and energy sources such as NAD, NADP and ATP can have profound effects on normal growth and development—
Cytotoxicity is often accompanied with inhibition of DNA synthesis which may lead to teratogenesis
Cytosine arabinoside and hydroxyurea both depress DNA synthesis by DNA polymerase inhibition and ribonucleoside diphosphate reductase respectively
Since cytosine arabinoside exerts the more prolonged depression of DNA synthesis, there is less time available for repair before the initiation of anomalous development.
RNA synthesis inhibition results in the interference of proteins essential for growth
Lack of ATP, NAD, NADP can have serious effects on glycolysis, respiration and electron transport during critical period of organogenesis
Intracellular pH changes
1.8 Intracellular pH
Alterations of foetal pH can lead to anomalous development
A decreased pH interferes with cellular processes such as proliferation, intracellular communications, enzyme activities, and cytoskeletal protein polymerization.
All can lead to formation of malformed foetal tissue or death
Mechanical Disruptions
1.9 Mechanical Disruption
Mechanical disruption may-- Destroy cell interactions Impede morphogenetic movements Cause decreased cell proliferation through
pressure necrosis Change fluid balance within cells and fluid
filled organs such as eyes, brain, spinal cord disrupting them
Extrinsic pressure and prolonged uterine contractions can lead to mechanical pressure on the developing foetus by decreasing blood supply leading to anomalous foetal tissue Conclusion-1
Conclusion-1 Drugs and Chemicals have harmful effects on the
embryo or foetus at any time during pregnancy Can produce congenital malformations or deformities
during the first semester Greatest risk period is from the third to the eleventh week
During the second and third trimester drugs can—
Affect the growth or functional development of the foetus Have toxic effects on foetal tissues
Drugs given shortly before term or during labour can have adverse effects on labour or on the neonate after delivery
Not all the damaging effects of the uterine exposure to drugs are obvious at birth, some may manifest later in life Conclusion-2
Conclusion-2
Drugs should be prescribed in pregnancy- Only if the expected benefit to the mother is thought
to be greater than the risk to the foetus All drugs should be avoided if possible during
the first semester Drugs which have been extensively used in
pregnancy and appear to be usually safe— Should be prescribed in preference to new drugs The smallest effective dose should be used
Few drugs have been shown conclusively to be teratogenic in man, but no drug is safe beyond all doubt in early pregnancy
The End