drug interactions between anti-hcv antivirals ledipasvir...
TRANSCRIPT

Drug Interactions between Anti-HCV Antivirals Ledipasvir/Sofosbuvir and Integrase Strand Transfer Inhibitor-Based Regimens
Kimberly Garrison, Joseph M. Custodio, Damian McColl,Phillip S Pang, Moupali Das, FuChih Cheng, Grace Ma, and Anita Mathias
Gilead Sciences, Foster City, CA
2nd Asia Pacific AIDS and Co-infections Conference (APACC), 1-3 June 2017, Hong Kong Presentation # 14

Disclosures
▪ Damian McColl, K.L. Garrison, J.M. Custodio, P.S. Pang, M. Das, F. Cheng, G. Ma, and A. Mathias: Gilead (employment; equity ownership).
2Garrison, APACC 2017, Presentation # 14

Background
▪ The introduction of antiretrovirals (ARVs) has significantly reduced acquired immunodeficiency syndrome (AIDS)-related deaths in human immunodeficiency virus (HIV)-infected individuals
– However, as HIV-related morbidity and mortality have decreased, liver-related complications associated with viral hepatitis have become a leading cause of death in this population1
▪ It is estimated that there are over 4 million HIV/hepatitis C virus (HCV) coinfected individuals globally
▪ It is a high priority to address this unmet medical need by identifying well-tolerated treatment options for HIV/HCV coinfected patients
3Garrison, APACC 2017, Presentation # 14
1. Bica I, et al. Clin Infect Dis 2001;32:492-7
Background
▪ Ledipasvir
– Once-daily, oral, 90-mg NS5A inhibitor
▪ Sofosbuvir
‒ Once-daily, oral, 400-mg NS5B inhibitor
‒ GS-331007, predominant circulating metabolite
▪ Ledipasvir/Sofosbuvir FDC
– Once-daily, oral, fixed-dose (90/400 mg) combination tablet for chronic hepatitis C for genotype 1 or 42
4
SOF nucleotide
polymerase
inhibitor
LDVNS5A
inhibitor
SOF nucleotide
polymerase
inhibitor
SOF nucleotide
polymerase
inhibitor
LDV
NS5A
inhibitor
SOF
nucleotide
polymerase
inhibitor
LDV
NS5A
inhibitor
SOF
nucleotide
polymerase
inhibitor
FDC, fixed-dose combination; genotype 4: LDV/SOF SPC
Garrison, APACC 2017, Presentation # 14
2. Harvoni [summary of product characteristics]. Cambridge, UK: Gilead Sciences International Ltd.; 2014

Background (cont’d)
▪ Preclinical data suggest LDV/SOF exhibits limited potential for clinically significant drug-drug interactions (DDIs)3
5
Transporters/Enzymes Substrate Inhibitor
P-gp/BCRPLDV
SOF (not GS-331007)LDV
Slow Oxidative Metabolism* LDV
P-glycoprotein (P-gp); breast cancer resistance protein (BCRP)
*unknown pathway
▪ LDV and SOF are not substrates for or clinically relevant inhibitors of organic cation transporter (OCT)-1 or -2, organic anion transporter polypeptide (OATP)-1B1 or -1B3, bile salt export pump (BSEP), or organic anion transporter (OAT)-1 or -3
▪ GS-331007 is not a substrate for OAT1, OAT3, or OCT2
▪ LDV or SOF are not turned over by major CYP isoforms in vitro
▪ LDV, SOF and GS-331007 are not substrates or clinically relevant inhibitors of UGT1A1
Garrison, APACC 2017, Presentation # 14
3. Harvoni [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2015;

Potential of Clinically Significant DDIs by ARVs4-8
▪ Emtricitabine (FTC) and TAF (and TFV as a major metabolite of TAF) exhibit limited clinically relevant DDI potential
▪ TAF is not an inhibitor/inducer of CYP3A4 in vivo, nor a substrate of OAT1 or 3; TDF does not inhibit major CYP isoforms
▪ DTG is not a clinically relevant inhibitor of OAT1 or 3, and is not expected to impact the pharmacokinetics (PK) of drugs that are substrates of CYPs, UGT1A1/2B7, P-gp, BCRP, BSEP, OATP1B1/1B3, OCT1, and multidrug-resistance‒associated proteins 2/4
6
Transporters/Enzymes Substrate Inhibitor (or Inducer‡)
P-gp/BCRP/
OATP1B1/1B3TAF, DTG†, TDF† COBI
OCT2/MATE1 DTG
CYP3A4 EVG, COBI, DTG COBI
CYP2D6 COBI
CYP2C9 EVG‡
UGTs* EVG, DTG
*Elvategravir (EVG) is a substrate for UGT1A1/1A3; dolutegravir (DTG) is a substrate for UGT1A1/1A3/1A9;
†DTG and tenofovir (TFV) disoproxilfumarate (TDF) are substrates for P-gp and BCRP;
‡EVG is a modest inducer; COBI, cobicistat; MATE1, multidrug and toxin extrusion protein 1;
TAF, tenofovir alafenamide fumarate
Garrison, APACC 2017, Presentation # 14
4. Bam RA, et al. Antivir Ther 2014;19:687-92;
5. Lepist EI, et al. Antimicrob Agents Chemother 2012;56:5409-13;
6. Murakami E, et al. Antimicrob Agents Chemother 2015;59:3563-9;
7. Stribild [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2014;
8. Tivicay [package insert]. Research Triangle Park, NC: ViiV
9. Healthcare; 2014;

Objectives
Primary
▪ To evaluate the DDIs between LDV/SOF and integrase strand transfer inhibitor‒based regimens: EVG/COBI/FTC/TAF (E/C/F/TAF; 150/150/200/10 mg) and DTG+FTC/TDF (50 mg + 200/300 mg)
Secondary
▪ To evaluate the safety and tolerability of co-administration of LDV/SOF and ARVs
7Garrison, APACC 2017, Presentation # 14
Methods
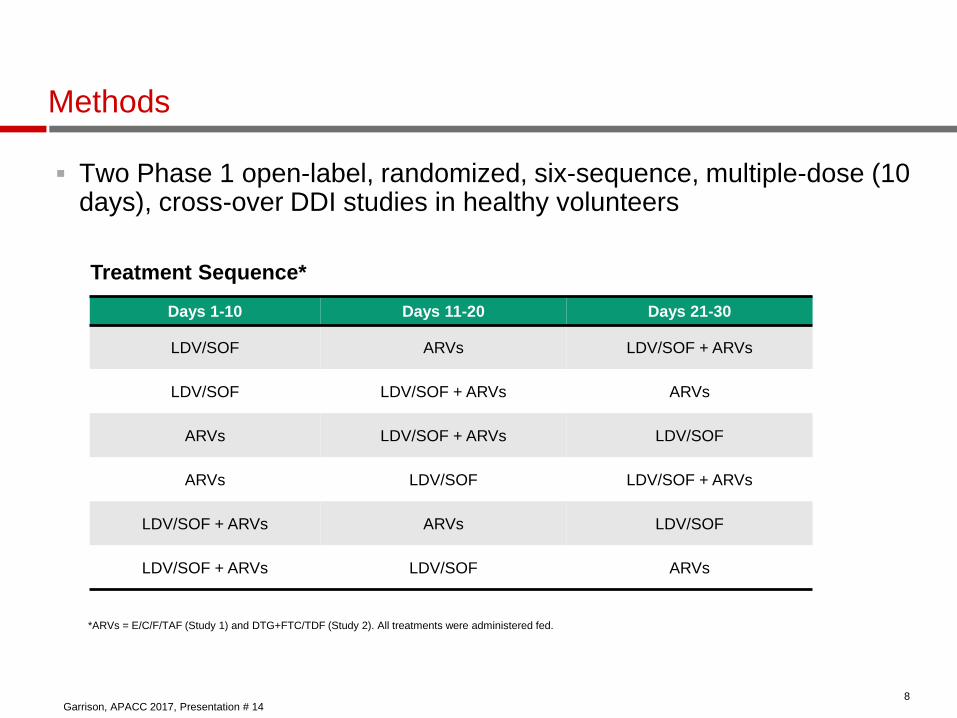
▪ Two Phase 1 open-label, randomized, six-sequence, multiple-dose (10 days), cross-over DDI studies in healthy volunteers
8
Treatment Sequence*
Days 1-10 Days 11-20 Days 21-30
LDV/SOF ARVs LDV/SOF + ARVs
LDV/SOF LDV/SOF + ARVs ARVs
ARVs LDV/SOF + ARVs LDV/SOF
ARVs LDV/SOF LDV/SOF + ARVs
LDV/SOF + ARVs ARVs LDV/SOF
LDV/SOF + ARVs LDV/SOF ARVs
*ARVs = E/C/F/TAF (Study 1) and DTG+FTC/TDF (Study 2). All treatments were administered fed.
Garrison, APACC 2017, Presentation # 14

Methods
▪ Steady-state PK sampling was performed over 24 hours for LDV, SOF, GS-331007, FTC, and TFV (Studies 1 and 2); EVG, COBI, and TAF (Study 1); and DTG (Study 2)Plasma concentrations were determined using validated LC/MS/MS assays
▪ Plasma concentrations were determined using validated liquid chromatography‒tandem mass spectrometry assays
▪ PK parameters—including area under the plasma concentration-time curve over the dosing interval (AUC), maximum plasma concentration (Cmax), and plasma concentration at the end of a dosing interval (C)— were estimated using noncompartmental methods (WinNonlin® 6.3, Pharsight Corp., St Louis, Missouri, USA)
▪ Geometric least-squares mean ratios (GMRs) and 90% confidence intervals (CI) were estimated using analysis of variance for AUC, Cmax, and C
(test vs reference), and compared against lack of PK alteration boundaries of 70‒143%
▪ Adverse event (AE) monitoring, and clinical laboratory, physical examination, and electrocardiographic evaluations were performed throughout study
9Garrison, APACC 2017, Presentation # 14

Subjects Study 1 Study 2
Enrolled/completed, n 30/30 30/29*
Mean age, y (range) 33 (22, 44) 32 (19, 45)
Mean weight, kg (range) 75 (60, 98) 76 (55, 109)
Sex (male/female), n 20/10 22/8
Race, n (%)
White 20 (67) 17 (57)
Non-white 10 (33) 13 (43)
Ethnicity n (%)
Hispanic/Latino 4 (13) 17 (57)
Non-Hispanic/Latino 26 (87) 13 (43)
Subject Enrollment and Demographics
10
*1 subject discontinued due to abnormal liver function test, which resolved within 2 weeks of treatment discontinuation.
Garrison, APACC 2017, Presentation # 14

Safety: Adverse Events in ≥2 Subjects
11
Subjects, n (%)
Study 1
(n= 30)
Study 2
(n=30)
Treatment-emergent AEs* 14 (47) 15 (50)
Nausea 5 (17) 5 (17)
Headache 5 (17) 5 (17)
Diarrhoea 3 (10) --
Dyspepsia 3 (10) --
Constipation 2 (7) 3 (10)
Vomiting 2 (7) 2 (7)
Pain in extremity 2 (7) --
Back Pain -- 2 (7)
Dizziness -- 2 (7)
AEs leading to discontinuation -- 1 (3)
*By system organ class and preferred term; all AEs reported were Grade 1 or 2 in severity;
no Grade 3 or 4 AEs were reported in either study.
Garrison, APACC 2017, Presentation # 14

Effect of Antiretrovirals on LDV/SOF PK
12
LDV
Mean
(%CV)
LDV/SOF +
E/C/F/TAF
N = 30
LDV/SOF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)
22,900
(35.7)
12,700
(36.3)
1.79
(1.63, 1.96)
Cmax
(ng/mL)1140 (32.1) 684 (32.3)
1.65
(1.53, 1.78)
Ctau (ng/mL) 896 (37.7) 459 (40.3)1.93
(1.74, 2.15)
Data presented to 3 significant figures.
%CV, Percent coefficient of variation
Study 1: LDV
Garrison, APACC 2017, Presentation # 14

Mean
(%CV)*
LDV/SOF
+
E/C/F/TAF
N = 30
LDV/SOF
N = 30
GMR
(90% CI)
SOF
AUCtau
(ng·hr/mL)
3310
(24.8)
2340
(37.4)
1.47
(1.35, 1.59)
Cmax (ng/mL)1570
(34.9)
1220
(37.9)
1.28
(1.13, 1.47)
GS-331007
AUCtau
(ng·hr/mL)
18,740
(22.6)
12,600
(20.9)
1.48
(1.44, 1.53)
Cmax (ng/mL)1230
(18.6)
951
(18.7)
1.29
(1.24, 1.35)
Ctau (ng/mL) 600. (27.4)359
(24.7)
1.66
(1.60, 1.73)
Effect of Antiretrovirals on LDV/SOF PK (cont’d)
Study 1: SOF and GS-331007
Garrison, APACC 2017, Presentation # 14

Effect of Antiretrovirals on LDV/SOF PK (cont’d)
LDV
Mean (%CV)
LDV/SOF+
DTG+FTC/TDF
N = 29
LDV/SOF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)8940 (35.1) 10,300 (37.4) 0.89 (0.84, 0.95)
Cmax
(ng/mL)523 (33.9) 626 (33.6) 0.85 (0.81, 0.90)
Ctau (ng/mL) 316 (39.2) 365 (41.2) 0.89 (0.84, 0.95)
Study 2: LDV
Garrison, APACC 2017, Presentation # 14

Effect of Antiretrovirals on LDV/SOF PK (cont’d)
15
Mean (%CV)*
LDV/SOF+
DTG+FTC/T
DF
N = 29
LDV/SOF
N = 30
GMR
(90% CI)
SOF
AUCtau
(ng·hr/mL)3220 (28.0)
2960
(27.0)
1.09
(1.00, 1.19)
Cmax (ng/mL) 1740 (33.2)1640
(35.0)
1.06
(0.92, 1.21)
GS-331007
AUCtau
(ng·hr/mL)
11,600
(18.4)
11,000
(18.5)
1.06
(1.03, 1.09)
Cmax (ng/mL) 824 (18.4) 836 (17.6)0.99
(0.95, 1.03)
Ctau (ng/mL) 344 (19.8) 328 (20.9)1.06
(1.03, 1.10)
Study 2: SOF and GS-331007
Garrison, APACC 2017, Presentation # 14
*Data presented to 3 significant figures. %CV, % coefficient of variation.

EVG
Mean (%CV)
LDV/SOF +
E/C/F/TAF
N = 30
E/C/F/TAF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)29,800 (23.3) 26,900 (22.7) 1.11 (1.02, 1.20)
Cmax (ng/mL) 2160 (27.5) 2180 (23.3) 0.98 (0.90, 1.07)
Ctau (ng/mL) 731 (35.6) 513 (40.0) 1.46 (1.28, 1.66)
COBI
Mean (%CV)
LDV/SOF +
E/C/F/TAF
N = 30
E/C/F/TAF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)17,000 (30.4) 11,400 (36.3) 1.53 (1.45, 1.62)
Cmax (ng/mL) 1670 (17.1) 1380 (26.0) 1.23 (1.15, 1.32)
Ctau (ng/mL) 175 (90.4) 56.1 (99.6) 3.25 (2.88, 3.67)
Effect of LDV/SOF on EVG and COBI PK: Study 1
Garrison, APACC 2017, Presentation # 14
*Data presented to 3 significant figures.

DTG
Mean (%CV)
LDV/SOF+
DTG+FTC/TDF
+LDV/SOF
N = 29
DTG+FTC/TDF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)73,700 (28.8) 65,900 (30.5) 1.13 (1.06, 1.20)
Cmax (ng/mL) 5520 (34.8) 4830 (28.3) 1.15 (1.07, 1.23)
Ctau (ng/mL) 31,890 (40.5) 1680 (38.3) 1.13 (1.06, 1.21)
Effect of LDV/SOF on DTG PK: Study 2
Garrison, APACC 2017, Presentation # 14
*Data presented to 3 significant figures.

FTC
Mean (%CV)
LDV/SOF +
DTG+FTC/TDF
N = 29
DTG+FTC/TDF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)
10400 (17.3) 9800 (19.6) 1.07 (1.04, 1.10)
Cmax (ng/mL) 1650 (28.3) 1620 (23.2) 1.02 (0.95, 1.08)
Ctau (ng/mL) 91.6 (28.9) 87.1 (28.7) 1.05 (1.02, 1.09)
FTC
Mean (%CV)
LDV/SOF +
E/C/F/TAF
N = 30
E/C/F/TAF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)
11600 (15.5) 12000 (15.4) 0.97 (0.93, 1.00)
Cmax (ng/mL) 1840 (22.1) 1780 (18.4) 1.03 (0.96, 1.11)
Ctau (ng/mL) 98.5 (27.2) 104 (26.8) 0.95 (0.91, 0.99)
Effect of LDV/SOF on FTC PK
Study 1 Study 2
Garrison, APACC 2017, Presentation # 14

TFV
Mean (%CV)
LDV/SOF +
E/C/F/TAF
N = 30
E/C/F/TAF
N = 30GMR (90% CI)
AUCtau
(ng·hr/mL)397 (15.9) 315 (18.7) 1.27 (1.23, 1.31)
Cmax (ng/mL) 20.7 (16.1) 17.8 (20.4) 1.17 (1.12, 1.22)
Ctau (ng/mL) 15.5 (16.6) 11.7 (20.0) 1.33 (1.28, 1.38)
TAF
Mean (%CV)
AUClast
(ng·hr/mL)195 (29.2) 239 (45.9) 0.86 (0.78, 0.95)
Cmax (ng/mL) 148 (48.2) 166 (50.8) 0.90 (0.73, 1.11)
Effect of LDV/SOF on TFV and TAF PK: Study 1
Garrison, APACC 2017, Presentation # 14

TFV
Mean
(%CV)*
LDV/SOF +
DTG+FTC/TDF
N = 29
DTG+FTC/
TDF
N = 30
GMR (90% CI)
AUCtau
(ng·hr/mL)4900 (24.1) 3020 (26.6) 1.65 (1.59, 1.71)
Cmax (ng/mL) 495 (24.0) 310 (24.4) 1.61 (1.51, 1.72)
Ctau (ng/mL) 117 (23.2) 55.7 (28.7) 2.15 (2.05, 2.26)
Effect of LDV/SOF on TFV PK: Study 2
*Data presented to 3 significant figures.
Garrison, APACC 2017, Presentation # 14

Conclusions
▪ LDV/SOF was generally well-tolerated when given alone or in combination with E/C/F/TAF or DTG+FTC/TDF
▪ Effect of ARVs on LDV/SOF PK
– E/C/F/TAF increased LDV, SOF, and GS-331007 exposures
▪ Results are consistent with findings from DDI evaluations between LDV/SOF and boosted ARV regimens3,9
▪ The mechanism is consistent with intestinal P-gp and/or BCRP inhibition by COBI
▪ Increased LDV, SOF, and metabolite exposures were within the exposure-safety window, as defined by clinical safety data, and are not considered clinically relevant
– No alteration of LDV/SOF PK by DTG+FTC/TDF
21Garrison, APACC 2017, Presentation # 14
3. Harvoni [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2015;
4. Bam RA, et al. Antivir Ther 2014;19:687-92;
5. Lepist EI, et al. Antimicrob Agents Chemother 2012;56:5409-13;
6. Murakami E, et al. Antimicrob Agents Chemother 2015;59:3563-9;
7. Stribild [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2014;
8. Tivicay [package insert]. Research Triangle Park, NC: ViiV
9. Healthcare; 2014; 9. German P, et al. Seattle, WA; February 23-4, 2015, abstr 82

Conclusions (cont’d)
▪ Effect of LDV/SOF on ARVs
– LDV/SOF increased EVG and COBI exposures
▪ Increased COBI exposure (AUC) was not considered to be clinically relevant based on results from Phase 2/3 studies that showed no association between COBI exposure and the incidence of common AEs or renal function parameters
▪ Increased COBI exposure is not expected to introduce further drug interaction potential10
▪ No alteration of EVG AUC and Cmax; the modest increase in EVG C was not considered clinically meaningful as EVG trough concentrations were >10 fold above the 95% inhibitory concentration (45 ng/mL)
– No alteration of DTG, FTC, or TAF PK by LDV/SOF
– LDV/SOF increased TFV exposure within DTG+FTC/TDF, but not within E/C/F/TAF
▪ Higher TFV within DTG+FTC/TDF was consistent with finding from DDI evaluation between LDV/SOF and non-nucleoside reverse-transcriptase inhibitor-based regimens efavirenz/FTC/TDF and FTC/rilpivirine/TDF3
▪ The mechanism is likely due to inhibition of P-gp and BCRP-mediated efflux of TDF by LDV
22Garrison, APACC 2017, Presentation # 14
10. Mathias AA, et al. Clin Pharmacol Ther 2010;87:322-9
3. Harvoni [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2015;

Conclusions (cont’d)
▪ LDV/SOF may be coadministered with E/C/F/TAF without monitoring
▪ LDV/SOF may be coadministered with DTG+FTC/TDF with appropriate monitoring for TFV-associated AEs
23Garrison, APACC 2017, Presentation # 14

Acknowledgements
▪ The authors gratefully acknowledge all the study subjects and the research team. This study was funded by Gilead Sciences, Inc.
24Garrison, APACC 2017, Presentation # 14

Disclosures
▪ Damian McColl, K.L. Garrison, J.M. Custodio, P.S. Pang, M. Das, F. Cheng, G. Ma, and A. Mathias: Gilead (employment; equity ownership).
25Garrison, APACC 2017, Presentation # 14