drug abuse and overdose trends: what’s still out there and … · 2017-06-22 · drug abuse and...
TRANSCRIPT
Drug Abuse and Overdose Trends: What’s Still Out There and What’s New? Ernest Stremski, MD, MBA Children’s Hospital of WI – ED Trauma Medical College of WI – Pediatrics Concordia University School of Pharmacy and Physician Assistant Program
No Financial Disclosures

Today, Fond du Lac EMS will be responding to:
Apnea Arymo
Seizure from MDMA
Smoking “spice”
Bath salts
Skittles
1-800-222-1222
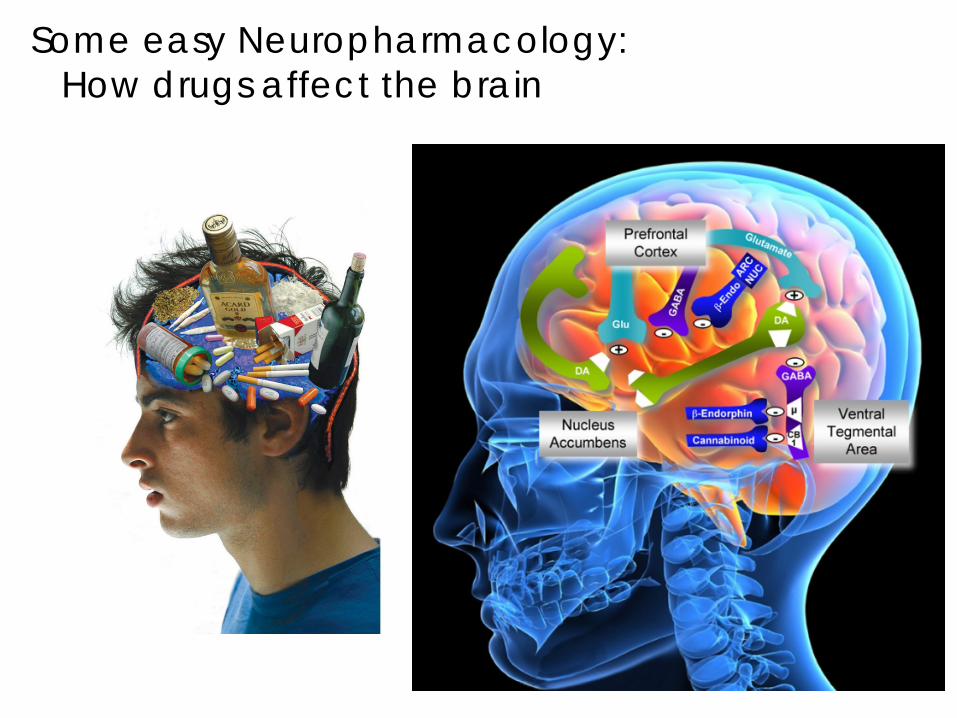
Some easy Neuropharmacology: How drugs affect the brain

Cerebral Cortex
Limbic System
MESOLIMBIC & VTA

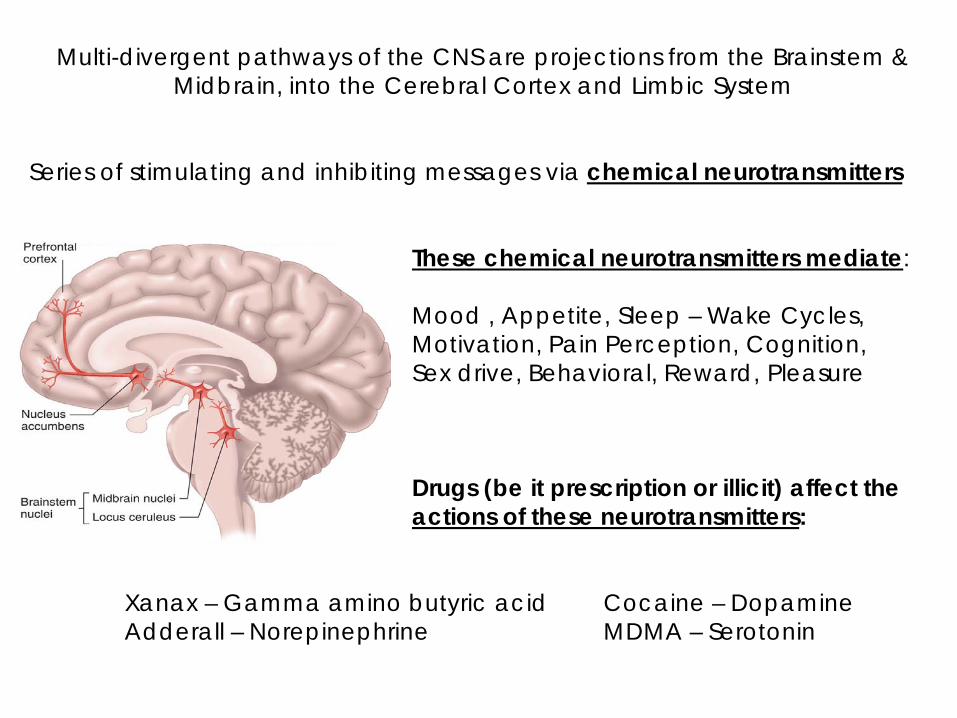
Multi-divergent pathways of the CNS are projections from the Brainstem & Midbrain, into the Cerebral Cortex and Limbic System
Series of stimulating and inhibiting messages via chemical neurotransmitters These chemical neurotransmitters mediate: Mood , Appetite, Sleep – Wake Cycles, Motivation, Pain Perception, Cognition, Sex drive, Behavioral, Reward, Pleasure Drugs (be it prescription or illicit) affect the actions of these neurotransmitters: Xanax – Gamma amino butyric acid Cocaine – Dopamine Adderall – Norepinephrine MDMA – Serotonin

NOREPINEPHRINE
DOPAMINE
SEROTONIN
ANANDAMIDE
Stimulant
Dissociative
Euphoria
Sedation & Anxiolytic

So many ways to get “High”
Many are provided by Mother Nature
Many neurotransmitters & receptors can mediate dissociative effects
Heroin & Opioids
Lysergol
Dextromethorphan
Psylocibin
Peyote
Salvinorin A
Muscimol
Scopolamine
MDMA MME 2C-B Ketamine
Myristicin
Synthetic Cannabinoid
Cathoniones
PCP
LSD
GHB
THC
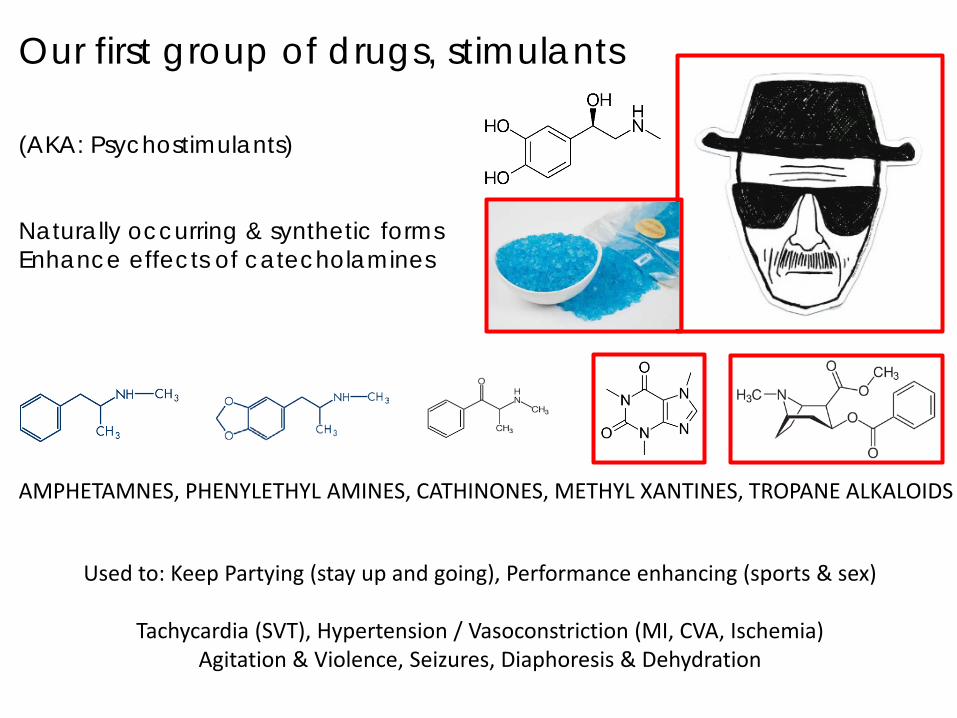
Our first group of drugs, stimulants (AKA: Psychostimulants) Naturally occurring & synthetic forms Enhance effects of catecholamines
Used to: Keep Partying (stay up and going), Performance enhancing (sports & sex)
Tachycardia (SVT), Hypertension / Vasoconstriction (MI, CVA, Ischemia) Agitation & Violence, Seizures, Diaphoresis & Dehydration
AMPHETAMNES, PHENYLETHYL AMINES, CATHINONES, METHYL XANTINES, TROPANE ALKALOIDS

Historical use of Amphetamines in the USA Increase work & productivity Treat Depression Weight loss / Appetite suppressant
Recreational Pharmaceutical Mood Elevator ADD / ADHD Arousal / Energy Narcolepsy Sexual stamina Weight loss Sport enhance Decongestant Should NOT be prescribing amphetamines for Depression, Chronic Fatigue, Asthma
5mg Methamphetamine
Military Weight Loss
Depression

Normally, we have a baseline amount of catecholamine stimulation of the brain Example: Water going into the sink (Epi releasing into the brain)
Keeps EPI in the brain for longer duration
Enhances amount of EPI released to the brain
Enhances and prolongs EPI in the brain

The “bath salts” (again, nothing to do with a relaxing spa)
Typically are synthetic cathinone products (Khat – natural source of Cathus edulis)
Mephedrone, Methylone, Methylenedioxypyrovalerone (MDPV)
Approach with Caution: CV & Neuro Support Benzodiazepines Cool Hydrate Not detected in standard drug screens
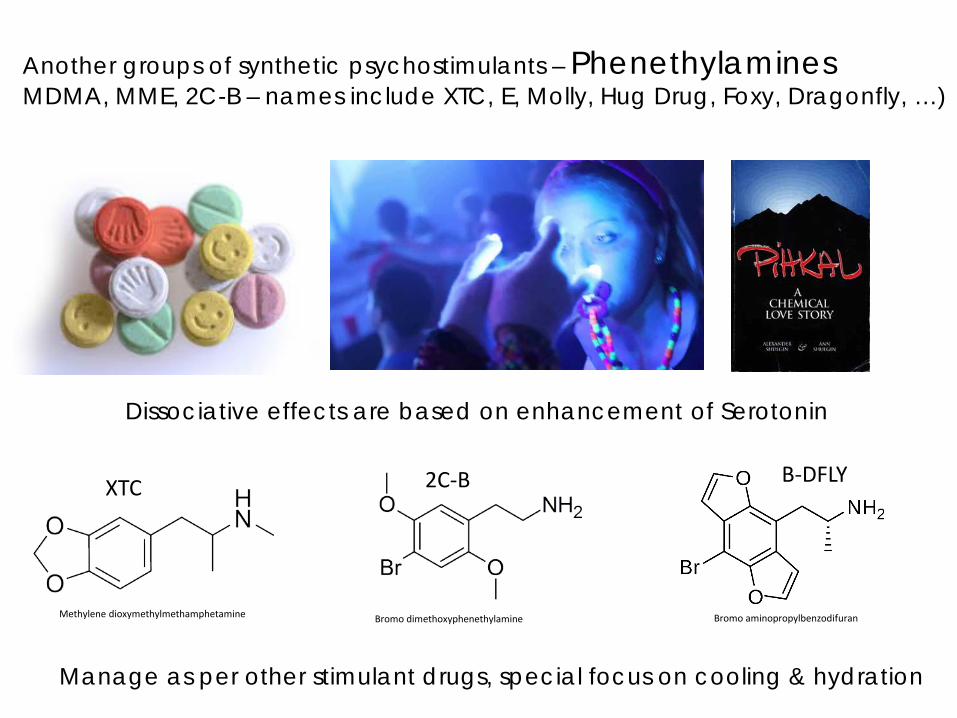
Another groups of synthetic psychostimulants – Phenethylamines MDMA, MME, 2C-B – names include XTC, E, Molly, Hug Drug, Foxy, Dragonfly, …)
Dissociative effects are based on enhancement of Serotonin
Manage as per other stimulant drugs, special focus on cooling & hydration
Methylene dioxymethylmethamphetamine Bromo dimethoxyphenethylamine Bromo aminopropylbenzodifuran
XTC 2C-B B-DFLY
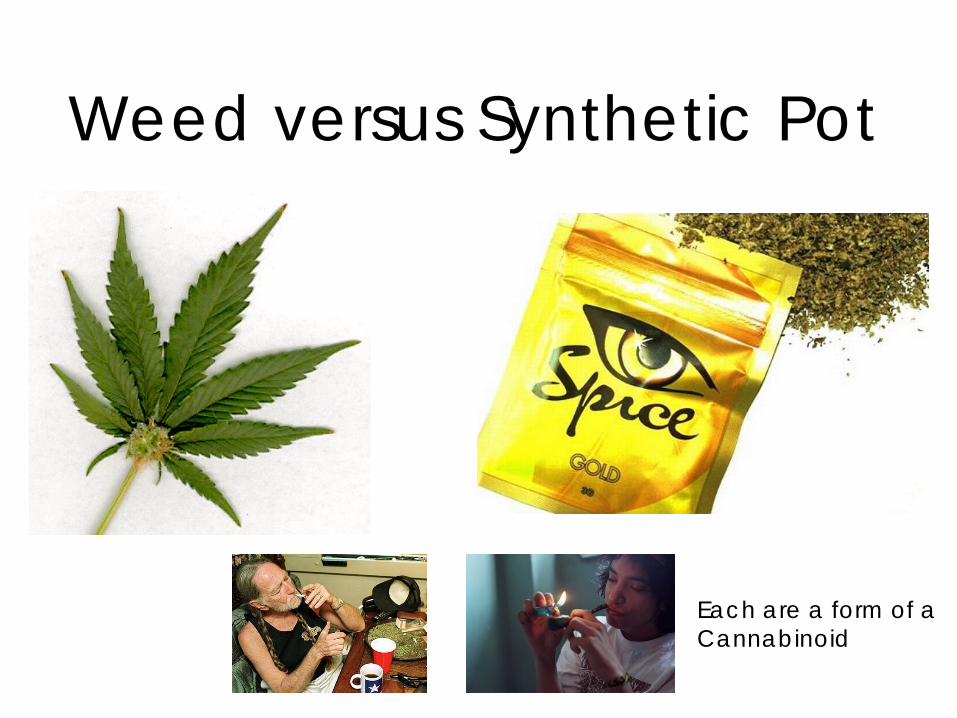
Weed versus Synthetic Pot
Each are a form of a Cannabinoid
We have 2 cannabinoid neurotransmitters They both act like THC (active component of marijuana) Anandamide and Arachadonyl glycerol There action is mediated at a receptor known as CB1
Marijuana (Sacred grass) – effects written B.C. Marijuana widely available OTC – pre 1910 Marijuana warnings – Refer Madness 1930s Marijuana Hippies – 1960s Marijuana – isolated THC as component 1964 Marijuana – discovered site of action at CB1 1992 Marijuana – medical & dispensaries begin 1998 New targets for CB1 – JWH compounds 2000s Marijuana – legalized recreational use ____ & ____ 2014


Where is the legitimate medicinal use of THC? Reduce intra-ocular pressure in certain forms of glaucoma Effective anti-emetic during chemotherapy Reduce pain of Multiple Sclerosis & peripheral neuropathy Minimize seizures in certain forms of refractory Epilepsy Appetite enhancing effects in HIV wasting Roles in: Cancer? Auto Immune Suppression? PTSD? ….. Is marijuana a “stepping stone” to drug abuse and Heroin? Would you rather have your kid doing marijuana versus ______? Are the motor & long term effects of THC less problematic than ETOH?

Medical marijuana legislation In February 2017, Sen. John Erpenbach and Rep. Chris Taylor introduced S 38/A 75, which would create a state-regulated program allowing access to medical cannabis for patients with serious medical conditions and their doctors’ recommendations. Meanwhile, two other proposals — SJR 10/ AJR 7 — would call for an advisory referendum on whether Wisconsin should create a medical marijuana program. Unfortunately, no action has been taken since the bills were referred to committee. However, there has been modest progress on improving Wisconsin’s CBD-focused medical cannabis law. On April 17, 2017, Gov. Scott Walker signed Act 4, which expands the state’s existing limited medical cannabis law, Lydia’s law, enacted in 2014. The original law allowed patients with documentation of a seizure disorder to possess CBD treatments, but it did not legalize the production of CBD products in the state. Act 4 expands the program to protect all patients who possess CBD and have a letter from their physician. Unfortunately, it remains illegal to produce or distribute CBD products. Sen. Chris Larson and Rep. Jimmy P. Anderson introduced legislation (S 104/A 158) that would allow state-licensed businesses to produce and dispense CBD treatment products.

delta 9, tetrahydrocannabinol (THC)
JWH 018 - 1-pentyl-3-(1-naphthoyl)indole
POT and SYNTHETIC POT are both activators of CB1 The synthetic forms are more profound in their ability to act on CB1 and other sites Leads to exaggerated effects (CV)
“pure THC” user “synthetic pot” user Tachycardic & Hypertensive Agitated Unresponsive Seizures
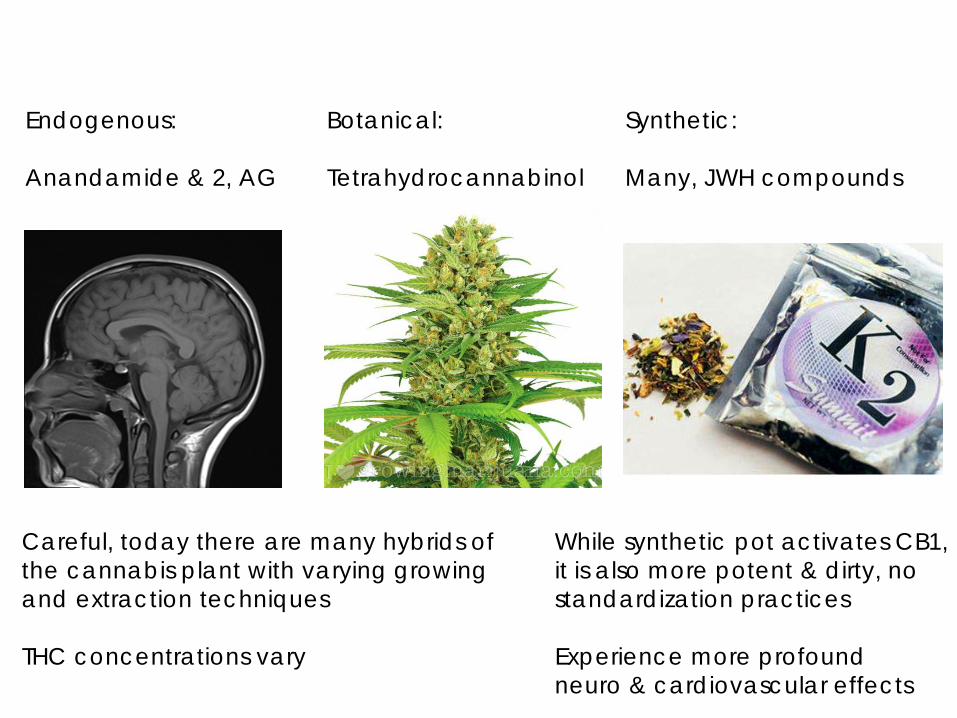
Careful, today there are many hybrids of the cannabis plant with varying growing and extraction techniques THC concentrations vary
Endogenous: Anandamide & 2, AG
Botanical: Tetrahydrocannabinol
Synthetic: Many, JWH compounds
While synthetic pot activates CB1, it is also more potent & dirty, no standardization practices Experience more profound neuro & cardiovascular effects

What did they take? Unresponsive, minimal to zero respiratory effort, pinpoint pupils, hypotonia
Crushed and insufflated tablets Ingested oral tablets Injected a powder

The Journal of the Pharmacy Society of Wisconsin, 2014: Volume 17
Prescription drug abuse affects > 6,000,000 US Citizens As many as 50 deaths / day due to Opioid Analgesic Overdose 80 % of heroin abusers have previously used Opioid analgesic medications

Opioid Analgesic Drugs Natural source is the opium poppy (Papaver somniferum)
Up to 10 % dry weight is Morphine
Actions of Opioid Drugs (Stimulate Mu, Kappa, Delta receptors of CNS) Stimulation of these 3 receptors blocks neural processing Primary effect on spinal cord / brain is to stop pain processing Problems: Slows and can fully inhibit respiratory processing Enhances Dopamine release in the Mesolimbic system Relaxes smooth muscle (drops BP, stops labor, slows peristalsis) Release histamine (warm flushed, pruritic, red skin)

Katzung, Basic and Clinical Pharmacology, 2012, 13th Ed.
Heroin
0.01 0.01
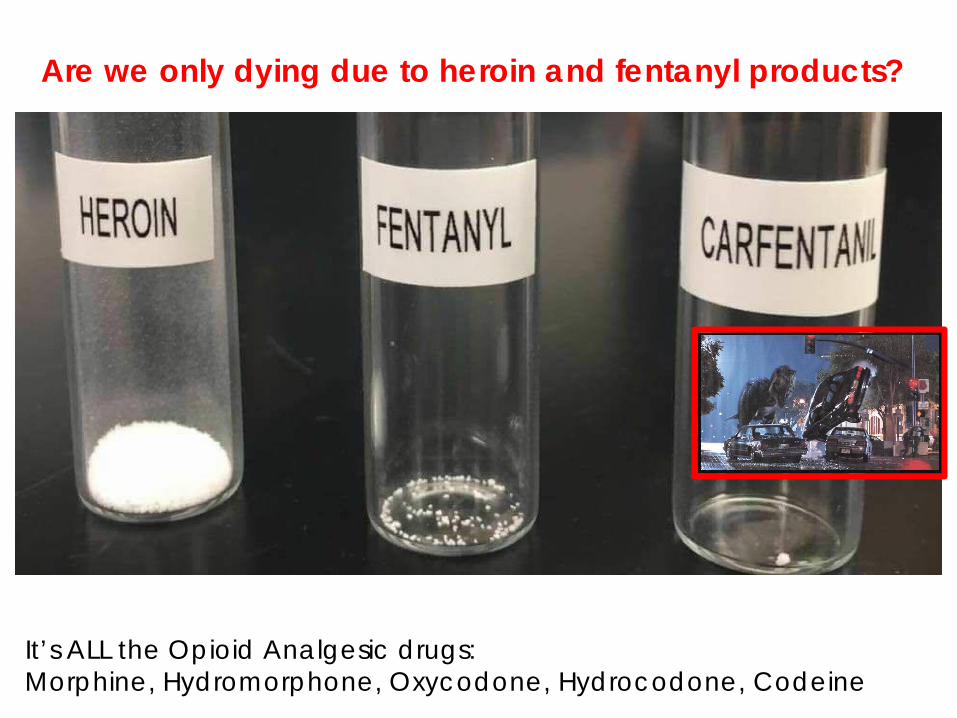
Are we only dying due to heroin and fentanyl products?
It’s ALL the Opioid Analgesic drugs: Morphine, Hydromorphone, Oxycodone, Hydrocodone, Codeine


Long acting opioid analgesic drugs, some of these are “newer”
Arymo
Avinza
Embeda
Kadian
Exalgo Palladone
Oxycodone
Oxymorphone Tapentadol Hydrocodone
Hydromorphone ?

Old OxyContin
ABUSE – DETERRANT TABLET TECHNOLOGY
New OxyContin
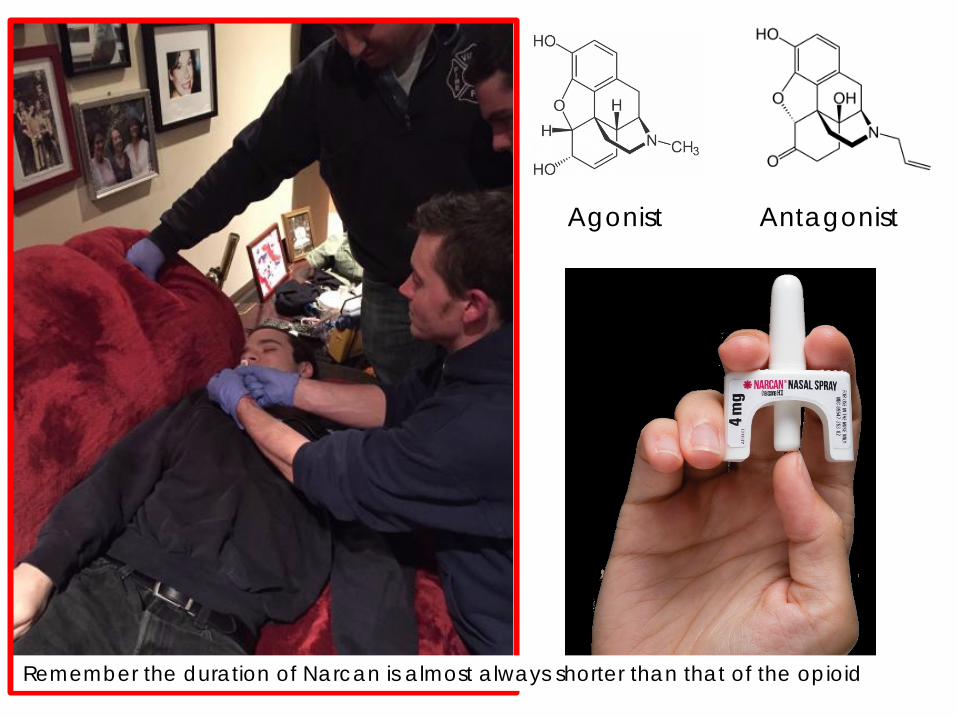
Agonist Antagonist
Remember the duration of Narcan is almost always shorter than that of the opioid

DXM looks like an opioid but has almost zero opioid effect. A metabolite (DXO) has Dissociative effects via Serotonin and NMDA SKITTLES – not going to be Narcan-reversible, let it wear off

Today, Fond du Lac EMS rescued:
Morphine
Phenethylamine
Smoking “JWH Compounds”
Cathinone stimulants
Dextromethorphan
1-800-222-1222
BENZO
BENZO BENZO
NARCAN
NO NARCAN