drs. loader, kift, straig, rapaport ... - plus...
TRANSCRIPT
SPRING 1996
EDGELINES
© 1996 Two Swan Advertising Agency
TIP-EDGE GRAPHIC
Published Quarterly In The USA
APPLIANCE UPDATES — Q’S & A’S — CASE REPORTS — TECHNIQUE TIPS — REVIEWS
Continued on page 2
No Monkey Business —the Tippytriplets let the world know what theythink of friction in orthodontics.
DRS. LOADER, KIFT, STRAIG, RAPAPORT(STANDING) PLUS HAWKINS ANDPARKHOUSE (SEATED) PONDER SIDE-WINDER TORQUE IN AUSTRALIA—PAGE 3.
DR. GILDA RUBIANO OF BOGOTA, COLOMBIAVISITS WITH MEMBERS OF THE KESLING ANDROCKE ORTHODONTIC GROUP DURING TIP-EDGE REFRESHER COURSE—PAGE 4.
®
ith the recent intro-duction of pretorqued.0215" x .028" arch-
wires (TP 381-195 maxillary,381-196 mandibular), setting upfor rectangular Stage III has sud-denly become easier, quicker andmore accurate. No longer shouldit be necessary to manipulate
torque set-tings intothe anteriorsegments ofarchwires inthe majorityof cases.
The pas-sive set ofthe rectan-gular cross
section is of course relevant,serving as a “reference plane”for the final torque angulationsthat will be achieved by theSide-Winder springs. Comple-tion of both torque and tip areself-limiting and stop simulta-neously. If the rectangular crosssectional angle is flat, parallelwith the occlusal plane (referredto as a “zero torque” setting),each bracket will express the
torque value built into itsrespective base.
Generally, a zerotorque setting is ap-propriate. However,there are occasions withadverse skeletal dis-crepancies, when stan-
dard incisor torque angu-lations will be inappropriate,
particularly in Class III cases.Indications for AnteriorTorque Compensation
The most common indica-
“Pretorqued” Rectangular ArchwiresBy: Dr. Richard Parkhouse, Consultant Orthodontist, Glan Clwyd Hospital, WALES
Dr. R.C. Parkhouse
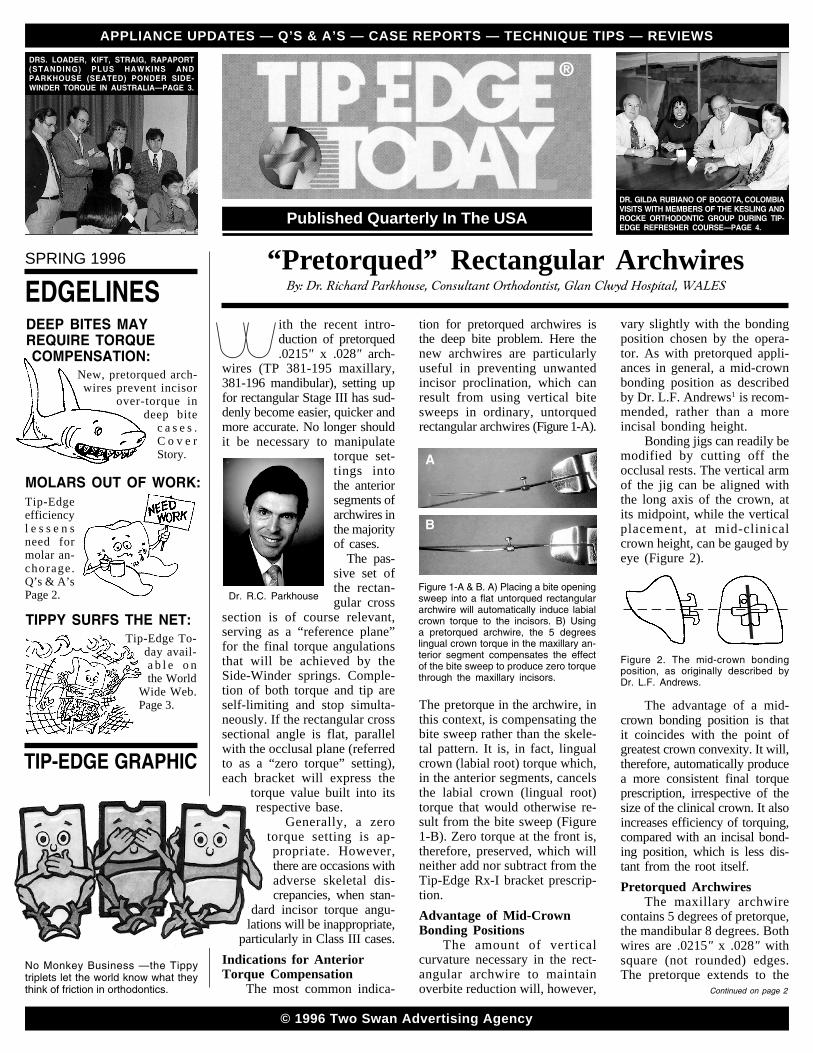
tion for pretorqued archwires isthe deep bite problem. Here thenew archwires are particularlyuseful in preventing unwantedincisor proclination, which canresult from using vertical bitesweeps in ordinary, untorquedrectangular archwires (Figure 1-A).
vary slightly with the bondingposition chosen by the opera-tor. As with pretorqued appli-ances in general, a mid-crownbonding position as describedby Dr. L.F. Andrews1 is recom-mended, rather than a moreincisal bonding height.
Bonding jigs can readily bemodified by cutting off theocclusal rests. The vertical armof the jig can be aligned withthe long axis of the crown, atits midpoint, while the verticalplacement, at mid-clinicalcrown height, can be gauged byeye (Figure 2).
Figure 2. The mid-crown bondingposition, as originally described byDr. L.F. Andrews.
The advantage of a mid-crown bonding position is thatit coincides with the point ofgreatest crown convexity. It will,therefore, automatically producea more consistent final torqueprescription, irrespective of thesize of the clinical crown. It alsoincreases efficiency of torquing,compared with an incisal bond-ing position, which is less dis-tant from the root itself.Pretorqued Archwires
The maxillary archwirecontains 5 degrees of pretorque,the mandibular 8 degrees. Bothwires are .0215" x .028" withsquare (not rounded) edges.The pretorque extends to the
Figure 1-A & B. A) Placing a bite openingsweep into a flat untorqued rectangulararchwire will automatically induce labialcrown torque to the incisors. B) Usinga pretorqued archwire, the 5 degreeslingual crown torque in the maxillary an-terior segment compensates the effectof the bite sweep to produce zero torquethrough the maxillary incisors.
The pretorque in the archwire, inthis context, is compensating thebite sweep rather than the skele-tal pattern. It is, in fact, lingualcrown (labial root) torque which,in the anterior segments, cancelsthe labial crown (lingual root)torque that would otherwise re-sult from the bite sweep (Figure1-B). Zero torque at the front is,therefore, preserved, which willneither add nor subtract from theTip-Edge Rx-I bracket prescrip-tion.Advantage of Mid-CrownBonding Positions
The amount of verticalcurvature necessary in the rect-angular archwire to maintainoverbite reduction will, however,
A
B
DEEP BITES MAYREQUIRE TORQUE COMPENSATION:
TIPPY SURFS THE NET:Tip-Edge To-
day avail-a b l e o nthe World
Wide Web.Page 3.
New, pretorqued arch-wires prevent incisor
over-torque indeep bite
c a s e s .C o v e rStory.
MOLARS OUT OF WORK:Tip-Edgeefficiencyl e s s e n sneed formolar an-chorage.Q’s & A’sPage 2.

Pg 2 COVER STORY — QUESTIONS & ANSWERS
“Pretorqued” Rectangular Archwires... Continued from page 1
distal of the archwires. By meansof a few simple adjustment stepsby the operator, it is therefore pos-sible to accommodate to varia-tions of tooth width and arch formwithout stocking a range of dif-ferent sized archwires.
Centerline markings (singlefor maxillary, double for man-dibular) appear on what will nor-mally be the gingival surface ofthe maxillary archwire and theincisal surface of the mandibular(Figure 3).
Q’s and A’s
addition, to accommodate someproclination of the maxillaryincisors. For this purpose, amaxillary pretorqued archwirecan also be placed upside down.In this instance, the centerlinemarking will not be visible tothe operator on insertion. Withno bite sweep, 5 degrees of pro-clination will automatically beprovided to the maxillary inci-sors (Figure 6-A). Again, the
be necessary. In such instances,plain rectangular arches (TP 381-197/8) can be fitted without bitesweeps and, except in cases ofsevere skeletal discrepancy, noadjustment to anterior torque val-ues will be necessary, with “zerotorque” throughout.Detorquing theBuccal Segments
Due to the continuity of thewire, the pretorque in the ante-rior segment extends to thedistal ends. Therefore, it is ne-cessary to return the posteriorsegments of the archwire to“zero torque.” This is a simpleadjustment, made by graspingthe archwire with two pairs oftorquing pliers (TP 100-142P)immediately adjacent (one oneach side) to each traction hookin turn (Figure 4). A small twist
Figure 5. Verifying zero torque in thebuccal segment.
cal segments, all that remains isto wipe in the bite sweep withthumb and finger, steadying thearchwire in a torque plier im-mediately mesial to each hookin turn. To check that the sweephas compensated the pretorqueto zero, hold the archwire at itsmidpoint and eye along theinterspace between the plierbeaks, as illustrated in the Tip-Edge Guide.2
Small alterations in anteriortorque can easily be made byholding the archwire firmly atits centerline in a plier. Gentleupward pressure with fingers be-neath the distal ends will slightlyincrease palatal root torque inthe maxillary anterior segment,while depressing the ends willreduce it, and vice versa in themandibular. Recheck for zerotorque in the posterior segments.Skeletal Variations
The most common needfor a modified anterior torqueprescription arises in severeClass III cases. Since the ma-jority of Class III cases have araised mandibular angle withreduced overbite, bite sweepswill not normally be necessary.In these circumstances, pre-torqued rectangular archwirescan be fitted flat and the pre-torque across the anterior seg-ment can be used to compensatethe skeletal pattern.
It is frequently necessary, in
Figure 3. Pretorqued archwires — 5 de-grees of lingual crown torque (maxil-lary) and 8 degrees (mandibular). Thecenterline markings, on the uppersurfaces, should both be visible to theoperator on insertion.
In increased overbite cases,where bite sweeps are required tomaintain overbite reduction, bothcenterline markings should, there-fore, be visible to the operatorwhen fitted. This is to ensure thatneither arch will inadvertently beplaced upside down. The lingualcrown pretorque across the inci-sors thus compensates the labialcrown torque that occurs in theincisor region when placing avertical bite sweep, so preserving“zero torque.”
Of course, pretorqued arch-wires are not required for everycase. Where anterior openbite orminimal overbite existed initial-ly, bite sweeps will obviously not
Figure 6-A & B. Compensating aClass III skeletal pattern, without in-creased overbite. A) The maxillary arch-wire must be fitted upside down to allow5 degrees of maxillary incisor proclin-ation. B) Pretorqued archwire can befitted flat to produce 8 degrees of retro-clination of the mandibular incisors.
posterior segments will normallybe adjusted to zero torque.
It is usually necessary tofinish the mandibular incisorsto a retroclined position, in or-der to maintain a positive over-jet. A mandibular pretorquedarchwire used without a bitesweep will give 8 degrees ofretroclination to the mandibularincisors (Figure 6-B). All thatis required is to adjust the seg-ments distal to the hooks to zerotorque, as described above.References1. Andrews LF. The straight wire appliance
explained and compared. J Clin Orthod1976;10:174-195.
2. Kesling PC. Tip-Edge Guide, 2nd ed.1992, Two Swan Advertising pp. TE-39.
at this point can return the un-wanted lingual crown torquealong the posterior segments to“zero torque,” similarly on theopposite side, without alteringthe pretorque in the anterior seg-ment. Verify the zero torque byholding one posterior segmentof the archwire in a torque plierand sighting across to the op-posite leg, as described in theTip-Edge Guide2 (Figure 5).Bite Sweeps AchieveZero Anterior Torque
Having detorqued the buc-
Figure 4. Eliminating undesired pos-terior crown torque.
5°
-8°
A
B
Q. When using Tip-Edge brackets and the Differential Straight-Arch Technique, are the second molars routinely banded?
WYNCOTE, PENNSYLVANIAA. Because of the unique Tip-Edge archwire slot, there is no
need for more than one molar in each quadrant for anchorage. Usu-ally second molars are only banded if they need leveling, rotation orare in crossbite.
Q. Is it possible to substitute an accentuated bite sweep for ananchor bend during bite opening? MANILA, PHILIPPINES
A. Yes. The important thing is the distance the anterior portionof the wire is displaced gingivally from the archwire slots in the
brackets. However, if the wire slides distally through the molar tubes(posterior space closure), the amount of anterior gingival displace-ment (bite opening forces) may become reduced. This might not berecognized as readily as when using localized, bite opening bends.
Q. In Stage III, when using a .022" x .018" nickel titaniumTorque Bar, how many degrees of change in angulation can onereasonably expect and in how much time? Do you use 20° or 30°bars routinely? Is it possible to achieve 10° of torque?
PIKETON, OHIO
A. The average rate of torque is approximately 2° per monthand the 30° Torque Bar is preferred. With proper insertion it shoulddeliver 10° of torque within six months.
COURSE NEWS — TECHNIQUE TIP — CASE REPORT Pg 3
CASE REPORT
Indonesian Tip-Edge Course
Tip-Edge in Japan
H.K. .............................. Female, 15 YearsExtractions ............................... U55, L55Archwires Used ..................... 6 (3U, 3L)Adjustments ......... 17, Time: 25 MonthsRetention .................................. Perfector
Cephalometric Changes:Start-Dotted Finish-Solid–
1-APo +1.5 mm +1.0 mmWits +1.5 mm 0.0 mmSN-MP 32.5o 33.0o
ANB 4.5o 4.0o
SNA 79.5o 78.5o
SNB 75.0o 74.5o
–1-SN 91.0o 92.0o
A two-day basic course was held in October 1995 at LadokgiR.E. Martadinata, Jakarta. The course leader (sixth from left) wasCommander Dr. A. Betny Sumantri of the Indonesian Navy.
All the participants in the course were enthusiastic and dili-gently went through all the stages on their typodonts. Tip-EdgeGuides, translated into Indonesian by Dr. Sumantri, helped makethe course a success.
In October of 1995 Dr. R.C. Parkhouse (front row center) spoketo the members of the Japanese Tip-Edge Society in Nagoya. Histopic was “The Vertical Dimension.” The Society is only three yearsold but already has held nine meetings and has over 120 members.He also gave a 3-day typodont course in Tokyo.
TP Orthodontics Goes Online andFeatures Tip-Edge Today—http://www.tportho.com.
This 15 year old female exhibited a Class II, Division 1 malocclusion witha Wits value of +1.5 millimeters. While the extraction of teeth was clearlyrequired to correct her malocclusion (total discrepancy of -7.0 mm) second,rather than first, premolars were extracted to prevent flattening the profile.
Tip-Edge appliances with .016" Wil-cock stainless steel archwires wereplaced in both arches. Zing® Stringwas used to tip the maxillary rightfirst premolar distally just enough toallow for alignment of the canine.
Stage II began using the original.016" Wilcock archwires with biteopening curves. At the next appoint-ment, maxillary and mandibular .022"archwires were placed to maximizemolar rotational control during finalspace closure.
After all extraction sites were closed,Stage III was initiated with squareedged .0215" x .028" stainless steelarchwires in both arches. Side-Winder springs were placed on allteeth to upright and torque themto their final inclinations.
Tip-Edge Today is thefirst orthodontic publica-tion available on the WorldWide Web. The WWWTip-Edge pages will allowfor instantaneous world-wide computer access tothe latest developments inthe Tip-Edge appliance andtechnique.
When fully construct-ed, the Tip-Edge Web sitewill include most articles aswell as graphics and pho-tos from current and past is-sues of Tip-Edge Today.The online version of Tip-
Edge Today will also allow for faster answers to technique questionsthrough an electronic bulletin board feature. Information will also beprovided on upcoming Tip-Edge courses and lectures as well as thelatest information on new product developments and technique tips.In response to popular demand the latest “Tippy” cartoon adventureswill also be posted on this Web site.
Through the use of an attached printer, hard copies of any itemsposted on the Tip-Edge pages can easily be printed (in full color withappropriate printers) for use in research or teaching. Although the firstTip-Edge pages may be a little “rough” in appearance please be patientas they will be continuously updated and improved in quality. Tip-EdgeToday Online can be accessed at: http://www.tportho.com.

®Pg 4 COURSE / LECTURE NEWS
100 Center PlazaLaPorte, Indiana 46350
Bulk Rate
U.S. Postage
PAIDLaPorte, Ind.
PERMIT NO. 79
Graduate Orthodontics and Tip-Edgein Colombia, S.A.
Starting second from left: Dr. Eduardo Galvis, Dr. Gilda Rubiano, Dr. Elsa Arango,Dr. Guiomar Cely and third semester students of the CIEO Military University.
For Subscription orCustomer Service
Call1-800-348-8856
219-785-2591Fax 219-324-3029
As a way to expand new horizons, the CIEO* Military Univer-sity in Bogota, Colombia has been teaching the Differential Straight-Arch® Technique for over 5 years.
The course begins with a semester which covers theory andpractice. The students bond brackets on typodonts which have beenset in different malocclusions and go through the three stages of thetechnique. The next semester the students start many Tip-Edge caseswhich are easily finished before they graduate because it is a threeyear orthodontic program.
The Tip-Edge technique is taught by Dr. Gilda Rubiano whoattended a course at the Orthodontic Center in 1989 and returned fora Refresher in 1995. Chairman of the Department, Dr. Eduardo Galvis,and Dr. Guiomar Cely also assist with Tip-Edge patients in the clinic.Both attended a Tip-Edge course a few years ago. The Universityhas many records of patients treated with the technique that prove itsspeed, ease and effectiveness.*Center of Investigation and Education of Orthodontics
Graduate Students’ Tip-Edge CourseOn November
17th-18th, first yeargraduate students ofsome of the ortho-dontic programs thatteach Tip-Edge took acourse at the Ortho-dontic Center. Begunin 1994, these courseshave proved to be aneffective springboardfor students to diveinto Tip-Edge. Participating schools included Columbia University,Montefiore Medical Center, Saint Louis University, State Universityof New York at Stony Brook and University of North Carolina.
Students from Saint Louis University examine patientat the Orthodontic Center.
Tip-Edge in Australia
In October of 1995 Dr. R.C. Parkhouse (seated, third from left)gave an advanced course in Sydney, New South Wales. Over 40orthodontists, including some post graduate students, attended thelectures at the Swiss Grand Hotel.