dr rob palmer - gpwsi gastroenterology - c&h gastro ccg lead miss tamzin cuming - consultant...
TRANSCRIPT
Rectal Bleeding pathway
Dr Rob Palmer - GPwSI Gastroenterology- C&H Gastro CCG lead
Miss Tamzin Cuming- Consultant Colorectal Surgeon, Homerton

Rectal Bleeding
Up to 38% of people will experience rectal bleeding at some point in their lives
Only 13-40% of these will consult a doctor about it
The majority of cases are benign and caused by minor problems that can be managed in primary care

CausesCommon Rarer
Benign anorectal disease: o Haemorrhoidso Anal fissureo Fistula-in-ano
Diverticular disease Inflammatory bowel disease:
o Crohn’s diseaseo Ulcerative colitis
Polyps Malignancy
Coagulopathies Arteriovenous malformation Massive upper GI bleeding Radiation proctitis Ischaemic colitis (mesenteric
vascular insufficiency) Solitary rectal ulcer syndrome. Dieulafoy's lesion of small or
large bowel. Endometriosis Meckel’s diverticulum Rectal varices GI tract invasion of non-GI tract
malignancy Henoch-Schonlein purpura Trauma (possible sexual abuse).
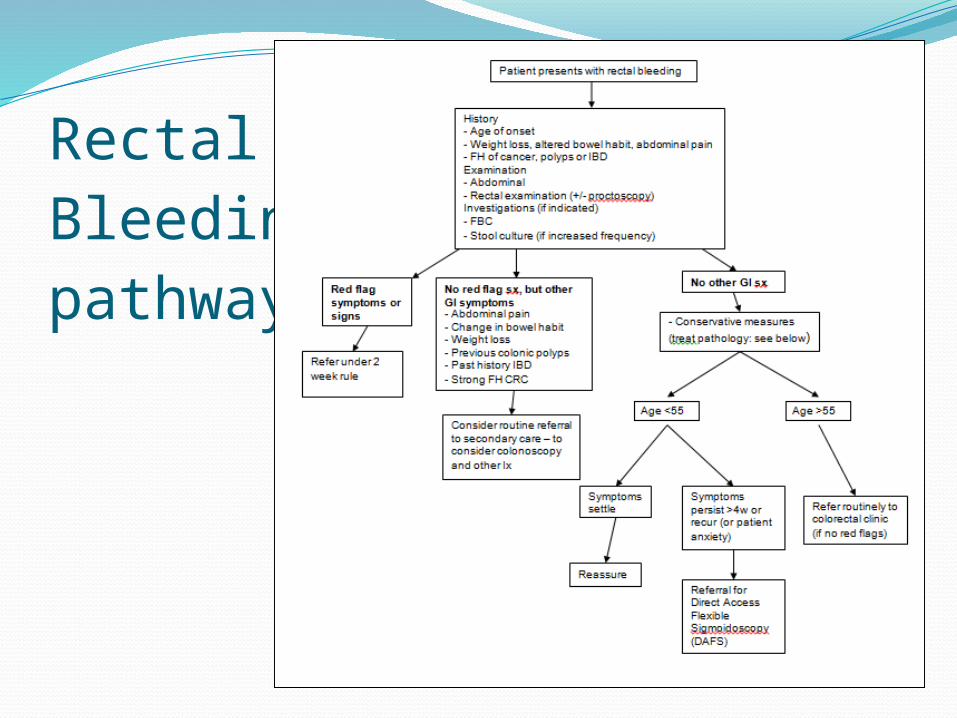
RectalBleeding pathway

History & Examination
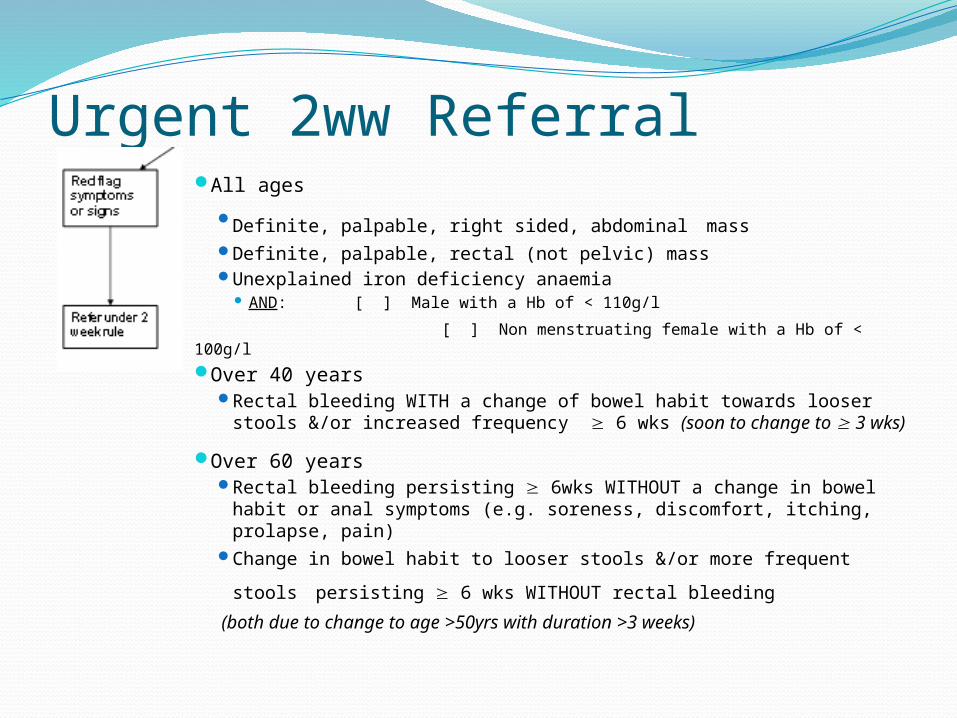
Urgent 2ww Referral All ages
Definite, palpable, right sided, abdominal mass Definite, palpable, rectal (not pelvic) mass Unexplained iron deficiency anaemia
AND: [ ] Male with a Hb of < 110g/l
[ ] Non menstruating female with a Hb of < 100g/l
Over 40 years Rectal bleeding WITH a change of bowel habit towards looser stools
&/or increased frequency 6 wks (soon to change to 3 wks)
Over 60 years Rectal bleeding persisting 6wks WITHOUT a change in bowel habit
or anal symptoms (e.g. soreness, discomfort, itching, prolapse, pain)
Change in bowel habit to looser stools &/or more frequent stools persisting 6 wks WITHOUT rectal bleeding
(both due to change to age >50yrs with duration >3 weeks)

Routine Referral to Secondary CareNo red flag sx, but other GI symptoms
Abdominal pain Change in bowel habit Weight loss Previous colonic adenomatous polyps or
malignancy Past history IBD Strong family history colorectal cancer
1 First Degree Relative (FDRs) <50 2 FDR of any age
Age >55yrs (not meeting 2ww criteria)
These patients may need investigation with colonoscopy (rather than flexi sig) to exclude other pathology

Referral for Direct Access Flexible Sigmoidoscopy (DAFS)
If no other GI symptoms and aged <55:Conservative management
Refer for direct access flexible sigmoidoscopy if:Symptoms not settling within
4 weeks (or recurring)High level of patient anxiety

Results of DAFS174 patients attended so farColonic pathology found in 39/174
22%16 hyperplastic polyps
Significant pathology in 23/17413%3 cancers10 adenomatous polyps10 new diagnoses of IBD proctitis

DAFS Patient SatisfactionProcedure done quickly enough:
78% yes, 22% noHelpful to have test on one visit to hospital:
87% - yes, prefer one visit4% - no, prefer to see dr in OPD first (9%
don’t mind)Overall satisafaction:
Very satisfied 61%, Satisfied 13%, Neutral 9%, Dissatisfied 9%, Very dissatisfied 9%

Referral for DAFSChoose and Book
Under Diagnostic Endoscopy – Flexible Sigmoidoscopy – Homerton (only available if <55yrs)
Directly bookable appointmentAppointments available on Tuesday morningsComplete referral form and send
electronically with CABGive patient information leaflet to patient


Information for patients - medicationsAspirin & Clopidogrel:
ContinueNo contraindication to diagnostic procedure +/- biopsies on
aspirin or clopidogrel
Warfarin: ContinueGP to check INR 1 week before endoscopy dateIf INR within therapeutic range, continue usual daily doseIf INR above therapeutic range but <5, reduce daily dose until
INR returns to therapeutic range
Iron tablets:Stop 1 week before procedure

Information for patients – the procedure
Bowel prepConsentProcedure

Unsuitable PatientsAcute anal pain suggestive of anal fissure
(procedure unlikely to be tolerated)Recent MI or CVA within 6wObesity (overall weight >135kg)DementiaPoor mobility (need to be able to transfer
from chair to bed)

Follow-upAll patients will be discharged back to
primary care following this procedure unless diagnosis of serious pathology found:malignancyIBDadenomatous polyps
The report will include detailed advice on management

Anal FissureA tear of the squamous lining of the distal anal canal.
Clinical Features:Sharp searing perianal pain, worse after defaecation.Bleeding is common, usually bright red on tissue
paper.Pruritus and irritation.Examination (gently part buttocks) may reveal linear
split, usually in midline posteriorly (90%), or anterior midline 10%. Fissure may not be seen, but may be palpated or be tender on palpation of the anal margin.

Anal Fissure

Anal Fissure - ManagementAcute: <6 weeks - conservative management:
Increase fluid intake High fibre diet to achieve
soft stools?Bulk forming laxatives (fybogel)
Topical creams –1w course of lignocaine gelSitz baths
pain reliefOral Analgesia

Anal Fissure - ManagementChronic: >6 weeksContinue conservative measuresCombination of bulk forming laxative (Fybogel BD) and softening
laxative (Lactulose BD) for the full 8 weeks Prescribe topical 0.4% Glyceryl Trinitrate (GTN) BD for 8 weeks
course N.B. 40% develop headaches as side effect 2 tubes of 30g should be sufficient to cover the 8 week course. Cost £34.80 for 30g tube
If fissure fails to heal (after 8 weeks of GTN) or if side-effects on GTN ointment switch to diltiazem 2% ointment (Anoheal®) Applied topically BD for 8 weeks. Cost of Anoheal® is approx £45 per tube
If not settling – refer to secondary care

Internal HaemorrhoidsAbnormally swollen vascular mucosal
cushions that are present in the anal canal originating from above the dentate line.
first degree Project into lumen of anal canal but do not prolapse
second degree
Prolapse on straining then reduce spontaneously
third degree Prolapse on straining but require manual reduction
fourth degree
Prolapsed and incarcerated; cannot be reduced

Internal Haemorrhoids

Internal HaemorrhoidsClinical Features:
rectal bleedingmucus dischargeitching and irritationoften painless (unless thrombosed or strangulated)
Causes:StrainingIncreasing ageRaised intra-abdominal pressureHereditary factors

Internal Haemorrhoids- ManagementIncrease oral fluid intakeDietary adviceConsider laxatives
Bulk forming (ispaghula husk) Lactulose (osmotic) or docusate (stimulant laxative with stool
softening properties, avoid in pregnancy)Topical anaesthetics with corticosteroids - use for up to 7 daysOral analgesics
Referral if: fail to respond to conservative management persistent bleeding, severe prolapse, affecting daily living fourth degree haemorrhoids
Urgent referral if: thrombosis with severe pain, incarceration, gangrene or sepsis

External Haemorrhoids (Perianal haematoma)A thrombosis of the external haemorrhoid
plexus, arising from below the dentate line
Clinical Features:acute severe pain, peaks 48-72hrs after onsetusually self-limiting to 7-10 daysbleedingdiscomfortitch

External Haemorrhoids (Perianal haematoma)

Internal piles: Management Analgesia Topical anaesthetics and corticosteroids Cold compresses
(If pt not tolerating pain in first 72hrs, consider referral for I&D)

Skin tagsGrowths of excess skin in the anal region, which
are often a remnant following the resolution of a thrombosed external haemorrhoid or other perianal trauma or inflammation, though they can be an isolated finding.
Clinical features:pruritus usually the biggest problemusually skin-coloured lesions arising from the rim
of the anal canal, which don’t contain dilated blood vessels

Skin tags

Skin tags - ManagementAnal hygiene
Wash after defaecationThorough attention to anal washing in bath or
showerAvoid perfumed soaps, biological washing
powders, fabric conditioners Use cotton underwear, avoid tight fitting
trousersManagement of constipationRefer for removal if large and
troublesome

Thank you!