dr : osama badry cardiology /anticogaulation coordinator incharge of anticoagulation service...
TRANSCRIPT

Dr : Osama BadryCardiology /Anticogaulation CoordinatorIncharge of Anticoagulation Service AWH-HMC/Qatar
Pharmacist - Directed Anticoagulation Service
: Quality Of care

“The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.”
Institute of Medicine. (2001). National Academy Press
Quality : Definition
“The provision of the necessary health care service to the appropriate person at appropriate time, and using the best means with the objectives of getting the best results for each individual patient, and the community at large.”
Qatar Supreme Council of Health

Effective Patient-centered
Timely Efficient
Quality of Care
Scientific Knowledg
e
Waiting Time
Patients’ Needs
Wasteful
Practices

Warfarin : Effective rat poison

Warfarin Therapy
Warfarin –Most widely used vitamin K antagonists(VKAs) worldwide in the prevention of treatment of blood clots. it’s used complicated by various factors
Ansell J .et.al 2004,Bungard TJ,et.al.2009,Hamby L ,et.al 2000
Utilizing the correct intensity and maintaining the patient in the therapeutic-determinant of its therapeutic effectiveness and safety
Ansell J .et.al 2004,Yi W.et.al.2008,kamali F.et.al,2010
3 primary models available for managing oral anticoagulant care are usual medical care, anticoagulation clinic, patient self management
Wilson SJ.et.al 2003

Question
Is the pharmacist managed anticoagulation more effective than usual care?

Anticoagulation Clinic (AC)
Anticoagulation management services(AMSs) (i.e.; anticoagulation clinics) is accepted as
gold standard and one of the approaches to improve anti Coagulant care
Ansell J et al. 2001Pharmacist Managed AMS in comparison to
other clinics (physician / Nurses) :Achieve superior anticoagulation control Favorable impact on hospitalization
Ruud KM. et al. 2010

Pharmacist Managed AC
Pharmacist-staffed Acs provided patient education, a more consistent monitoring and early recognition of risk factors.
Chamberlain MA. et.al .2001
Pharmacist –managed AC service demonstrated decreased advers events(39-47 % bleeding) and reduced hospital costs (USD 375-1620 per patient).
Saokaew S .2010, You JHS CA.et al .2008

Quality Team

Disadvantage of Usual Care
No systematic approach for tracking and scheduling INRs.No specific dosing nomogram or protocol are utilized ; only
individual physician knowledge and experience with management of warfarin is utilized.
Patients who are not getting their lab work done routinely may not discovered until a doctor’s appointment or a prescription renewal.
Long waiting time resulted in patient’ frustration and low satisfaction.
No structured education or counseling for patients and/or their families.
Unavailability of the treating physicians. No active participation for other health care providers e.g.
Pharmacists, Patient educators and dieticians. Follow-up appointment depends on physician’s scheduling.No structured evaluation of service e.g non adherence to warfarin
therapy.

Outpatient Management



Conclusion: The pharmacist-managed anticoagulation program within a family practice clinic compared to usual care by the physicians achieved significantly better INR control as measured by the percentage of time patients’ INR values were kept in both the therapeutic and expanded range. Based on the results of this study, a collaborative family practice clinic using pharmacists and physicians may be an effective model for anticoagulation management with these results verified in future prospective randomized studies.
Inpatient
Management

Impact of PDAS on Quality and Safety of HIT Management


Outcome with pharmacist – and physician- managed warfarin mediated anticoagulation

Efficacy with pharmacist –managed in-hospital anticoagulation

Garwood et al 2008

Pharmacist-Managed
Anticoagulation clinic
From Zero to star of
excellence

Process of implementation
Pharmacy Director Idea
Cardiology Champion
Multdisciplinary
Subcommittee
Pharmacy & Therapeutic Committee
Senior Executive Clinical
complexityProvision of
resources
and support

Challenges
Resources
Physician resistance
Patient satisfaction
Referral and first appointment

Anticoagulation clinic statisticsTotal Number of Patients May 2013- September 2014

Indication NoAF 59
MVR 9
AVR 8
DVR 5
L-V thrombus 7
Pulmonary hypertension 2
DVT 38
Pulmonary Embolism 28
Portal vein thrombosis 2
Stroke 3
APS 3
Sever AS,MR 1
Right portal vein thrombosis 1
Post MI , LV aneurysm 1
IVC 1
Low EF 1
Cerebral vein thrombosis 2
Total 171
Anticoagulation clinic statistic per Indication May 2013- September 2014

Month No
May /2013 11
June/2013 47
July/2013 79
August /2013 50
September/2013 85
October/2013 53
November/2013 74
December/2013 96
JANUARY /2014 86
February /2014 105
March/2014 101
April/2014 98
May/2014 97
June/2014 95
July/2014 104
August/2014 106
September/2014 123
TOTAL 1410
VISITS NO /MAY 2013-SEPTEMBER 2014
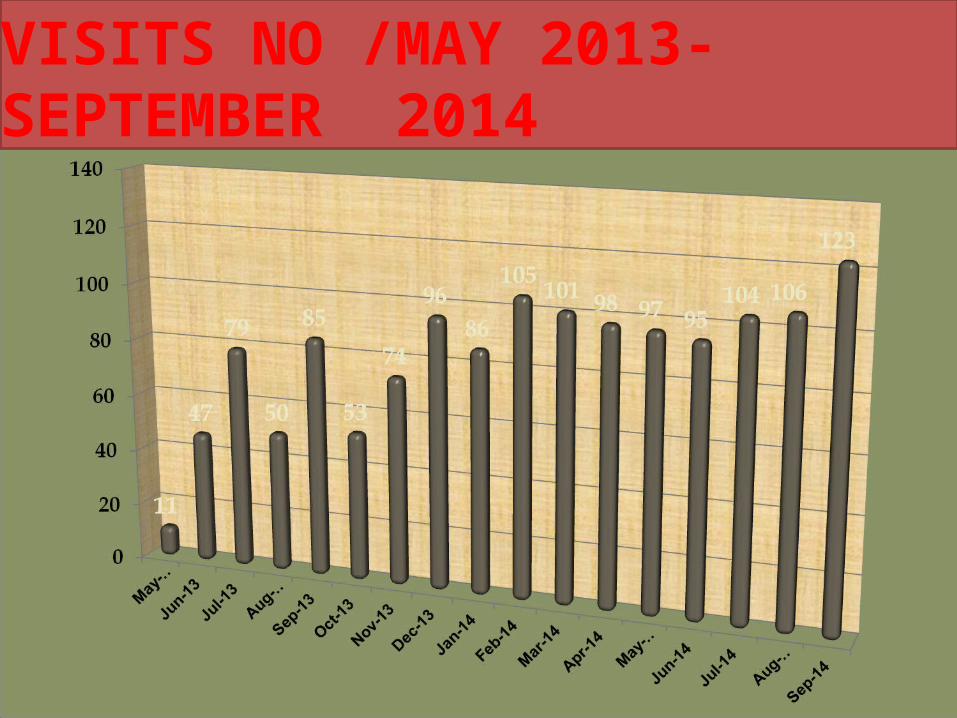
VISITS NO /MAY 2013-SEPTEMBER 2014

Month NoMay /2013 12
June/2013 11
July/2013 28
August /2013 27
September/2013 19
October/2013 21
November/2013 18
December/2013 22
JANUARY /2014 12
February /2014 20
March/2014 13
April/2014 27
May/2014 37
June/2014 53
July/2014 24
August/2014 36
September 45
TOTAL 425
INTERVENTIONS

Interventions

Research done in collaboration with Qatar university, ‘’Satisfaction and quality of life of patients attending an ambulatory pharmacist-managed anticoagulation clinic in Qatar’’, see the supporting evidence.
The quantitative improvement was done by calculation of TTR (time in therapeutic range) a metric of how well patients are managed on warfarin therapy by using software program, the result is 77.8
Another two ongoing researches were accepted by research center
1-‘’evaluation of clinical and economical outcomes at pharmacist versus physicians –based anticoagulation outpatient clinic and its impact on the cardiovascular disease management in Qatar””
2-‘’ The Effect of Genetic Variants on Warfarin Dosing and Its Impact on Cardiovascular Outcomes in Qatar’’
Quality Evidence

Why We Are Successful
Strong and effective leadership Multidisciplinary Team Quality Improvement First clinic run by a clinical pharmacist in
HMC/ QATAR

Progress does not involve replacing one
theory that is wrong with one that is right,
rather it involves replacing one theory that
is wrong with one that is more subtly wrong.
Hawkins Law
