dr françois habersetzer hôpitaux universitaire de ... · dr françois habersetzer hôpitaux...
TRANSCRIPT

Dr François Habersetzer
Hôpitaux universitaire de Strasbourg
Inserm 1110
Vaccins thérapeutiques et VHC

Spontaneous Clearance
(1% ??)
Primary Infection
Spontaneous Clearance
(15-50%)
Chronic CarrierState
(50-85%)
Healthy Carriers(30%)
Acute phase (< 6 months) Chronic phase (>6 months)
HCV: natural course of infection

Components of the adaptative anti-hepatitis C virus immune responses
CD81, SRBI,
Occludine, Claudine
Adapted from Freeman AJ et al. Immunology and Cell Biology 2001: 79: 515-536.Rehermann et al. JCI, 2009
Spontaneous Clearance of HCV infection requires :
•Early and multispecific class 1 restricted CD8+ T cell and class II restricted CD4+ T cell responses directed to S and NS HCV proteins
• The quality of HCV clearance and protection from reinfection is determined by the functional potency and cytotoxic potential of HCV-specific CD8+cells
•NS3 is a key viral protein for HCV elimination
NAb responses to epitopes in E1 and E2 are associated with resolution of infection and protection against reinfection

●●●●●●●●● 4
Weeks after infection
HCVHCV
2 4 6 8 10 12 14 16 18
Active
replication
T cell T cell inductioninduction
66--8 weeks8 weeks
1
10
100
Vir
ion
s 1
06
/ m
l
Sustained Sustained
Adaptive Adaptive
responsesresponses
HCVHCV %tet.+CD8+ T cells
1
10
100V
irio
ns
10
6/
ml
0.4
0.8 % H
CV
tet .+
/ CD
8
Weeks after infection2 4 6 8 10 12 14 16 18 20
% IFNg+/CD8HCVHCV
Weeks after infection
1
10
100
Vir
ion
s 1
04
/ m
l
200
300
100
0
IFN
-g E
LISP
OT
CHIMPANZEE INFECTION
HUMAN INFECTION
0 8 16 24 32 40
Thimme, R. et al, J Exp Med 2001 Shoukry, N. et al, J Exp Med 2003
NS3 is a keytarget
Importance of HCV-Specific Intra-Hepatic CD8+ T Cell Immune Responses (IFN-γγγγ) in Control of HCV Replication

Mechanism of HCV Clearance and Persistance
Spontaneous Clearance of HCV infection
Persistance of HCV infection
Strong and wide CD8+ and CD4+ T –cell
responses to HCV epitopes
Limited T-cell responses and limited
reactivity to HCV epitopes;
Viral CD4+ and CD8+ escape mutants
Lack of memory T-cell maturation
Persistence of dysfunctional T-cells
Strong cytotoxic T cell responses Negative costimulators of T cells : PD-
1/PDL1 receptors-ligand;
Immunoregulatory cytokines IL10
Neutralising Ab to E1/E2 Escape Mutants
IL28B gene polymorphisms
C/C genotype
IL28B gene polymorphisms
T/T genotype
Impairment of DC maturation
Ferrari C. Gastroenterology 2008; 134: 1601-1604; Rehermann B et al. Nat Rev Immunol 2005; 5: 215-229;
Thomas DL et al. Nature 2009; 461: 798-801; Wherry EJ et al. J Virol 2004; 78: 5535-5545

For Preventing HCV infection: need of strong cross-reactive
neutralising (Ab) responses
To reconstitute efficient immune control in chronically
infected patients : by restoring functional T-cell responses
similar to those patients who resolve the HCV infection
spontaneously : le vaccin thérapeutique
Need to develop vaccine strategies

Therapeutic Vaccines for chronic hepatitis C
• Different strategies for immunization
� Peptides
� Proteins
� DNA-immunization
� Virus-like particules
� Tarmogens
� Life attenatued carriers : recombinant viruses and bacteria
Recombinant viruses are an efficient way to deliver heterologous DNA that can mediate a
large amount of HCV antigens potentially increasing the immunogenicity of the vaccine in
comparison with peptides and proteins

HCV Treatment: TG4040 Therapeutic Vaccine
Based on non-replicative, poxvirus MVA (Modified Viral Ankara strain) was choice because he was successfully administered to immunize high risk patients against smoll pox without any significant side effects in the primary vaccination of over 150 000 humans
T cell-based therapeutic vaccine: expressing 3 of the major non-structural HCV proteins (NS3, NS4, NS5B) that are prominant targets of host induced immune responses during clearance / control of infection
First viral-based vaccine in the field of HCV therapies having entered clinical development
Objective: to prime HCV specific functional CD4+ and CD8+ T lymphocytes capable to produce IFN-γ and lyse infected cells

Induction d’une réponse immunitaire cellulaire après injection de TG4040
www.cancer-info.com
Migration
+
Administration s.c. de TG4040 (Mécanisme d’induction de la réponse immunitaire)
Hépatocytes Infectés
Élimination VHC via les cytokines
Lyse des hépatocytes par les cellules CD8 spécifique anti-VHC
NK
CD8
DC
CD4
LT cytotoxique
Migration Au Foie
Voie non cytolytique
●●●●●●●●● 9
Infection et capture
TG4040
Mécanisme d’action supposé de TG4040

Etude de phase 1 - TG4040.01 - d’escalade de dose chez des patients ayant une hépatite chronique C minime
• Dose escalating study � Cohort 1: 106 pfu, 3 patients
� Cohort 2: 107 pfu, 3 patients
� Cohort 3: 108 pfu, 9 patients + boost at month 6
All patients: Prime injection (3 weekly injections)
8 12 16 20 40 44 4828 32 360
TG4040 inj (cohort 3, 4)
weeks4 24
TG4040 inj (cohort 5)TG4040 inj (cohort 6)
TG4040 injection
●●●●●●●●● 10
Habersetzer F et coll. Gastroenterology, 2011.

Étude de phase 1 d’escalade de dose: Evolution de la virémie
11
Change in HCV RNA from baseline
D22 D37 M2 M3 M4 M5 M6 M6+8 M6+22 M9D15D8D1
TG4040 injections
1,0
0,5
0,0
- 0,5
- 1,0
Ch
ange
in H
CV
RN
A (
log1
0)
106 pfu (n = 3)
107 pfu (n=3)
108 pfu (n=6)
� Pas d’effet sur charge virale 108 pfu
� Nadir après 37 j
� Diminution prolongée de la virémie de 37 à 6 mois 106 pfu
Rappel (108 pfu)
Habersetzer F et coll. Gastroenterology, 2011.

Patient 3 Corrélation réponse T et virémie C
-2 0neg
Pt 31
-1.5
-1
-0.5
0
0.5D1
D22 M6
2850
100
150
200
250
ND ND
NS4B NS5/1 NS5/2NS3/1 NS3/2 VL measurements
M2
D37M-1
Corrélation entre la diminution de la virémie et la réponse immunitaire spécifique au TG4040
ELISpot : Réponse augmentée contre NS3/1 et NS4B (> moy pré -thérapeutique + 2SD) et induction de réponse contr e NS3/2
Habersetzer F et coll. Gastroenterology, 2011.

Résultats étude de phase 1 : preuve de concept
Chez des patients ayant une hépatite C chronique
� Vaccin thérapeutique TG4040 bien toléré
� Baisse transitoire de la virémie chez 50% des patients
� Permet d’induire une réponse immunitaire chez 33% des patients
Nécessité d’envisager des combinaisons pour permettre une élimination
virale
Habersetzer F et coll. Gastroenterology, 2011.

●●●●●●●●● 14
4 80 16 20 24 40 44 48 52 56 60 64 68 7228 32 36
4 8 12 16 200 40 44 48 52 56 60 64 68 7228 32 36 76 80 84
TG4040, 107 pfu(subcutaneous injection)
Initiation of SOC
Second stopping rule
if viral load detectable after 24
weeks of SOC (all Arms)
Control Arm(n=31)
Primary endpoint: improvement of cEVR rates
First stopping rule if viral load decrease is inferior to
2 log10 IU/mL (Control Arm only)
4 80 16 20 24 40 44 48 52 56 60 64 68 7228 32 36
SOC: PegIFN/ribavirin(Pegasys®/Copegus®)
SOC Lead-In Arm(n=63)
TG4040 Lead-In Arm (n=59)
Weeks
TG4040 monotherapy
12
12
24
Randomized Open Label Phase II Trial
1:2:2Randomization
2 experimental arms
Treatment-naïve
Non-cirrhotic
Genotype 1
Patients
Evaluable population: ITT population excluding patients
who left study before cEVR evaluation
Wedemeyer H et al. EASL 2013
Résultats étude de phase 1 : preuve de concept

●●●●●●●●● 15
Control(n=31)
SOC Lead-In (n=63)
TG4040 Lead-In(n=59)
Mean Age in years 41 44 43.6
Gender, n females / n males 15/16 27/36 27/32
Caucasian, n (%) 30 (96.8) 60 (95.2) 59 (100)
Mean Baseline HCV RNA in log10 IU/mL (SD) 5.96 (0.68) 5.74 (0.81) 5.71 (0.81)
HCV genotype, n (%)
1a
1b
1a/b
6 (19.4)
25 (80.6)
0
12 (19)
50 (79.4)
1 (1.6)
15 (25.4)
44 (74.6)
0
IL28B n C-C / n non C-C(All data are not yet available)
7/17 14/33 16/32
F3 Fibrosis, n (%) (Biopsy or FibroScan®) 1 (3.2) 6 (9.5) 7 (11.8)
High Baseline ALT (≥ 2 ULN), n (%) 5 (16.1) 15 (23.8) 16 (27.1)
� Good balance between arms, including IL28B polymorphism and genotype 1a/1b
distributionWedemeyer H et al. EASL 2013
� Stratification by age (>vs≤50 years) and baseline viral load (>vs≤400 000 IU/mL)
Demographic and baseline characteristics
●●●●●●●●● 16
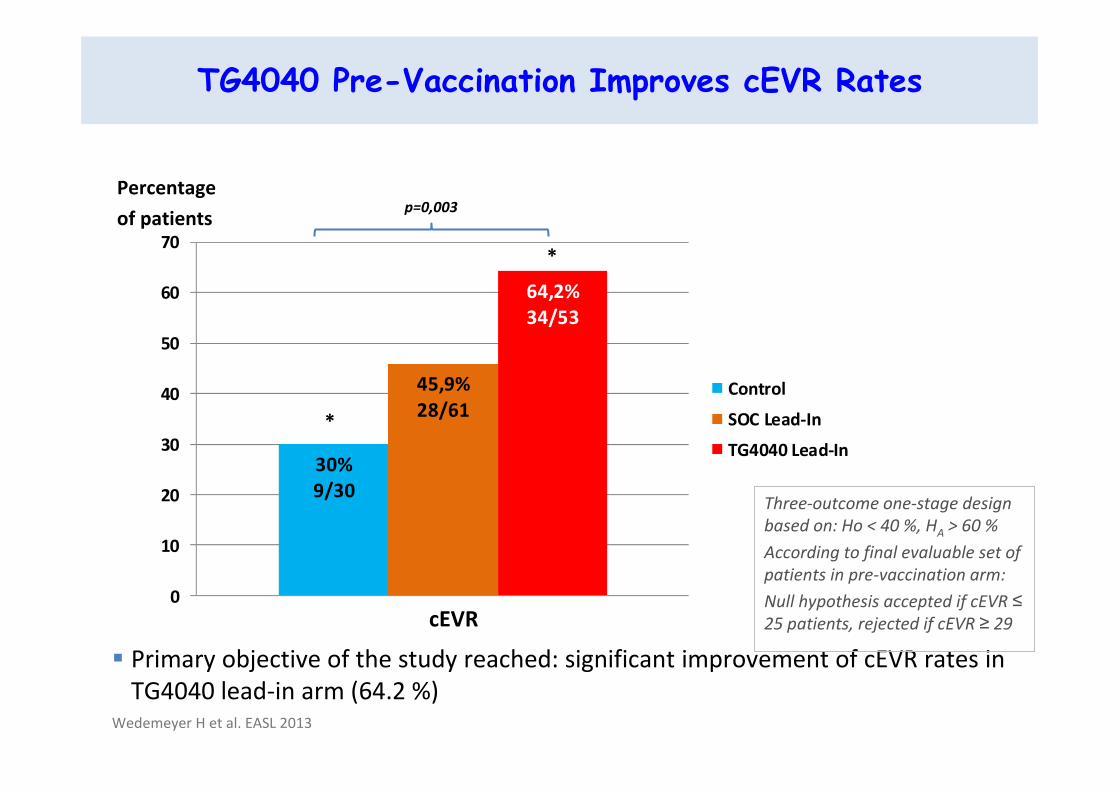
TG4040 Pre-Vaccination Improves cEVR Rates
� Primary objective of the study reached: significant improvement of cEVR rates in
TG4040 lead-in arm (64.2 %)
30%9/30
45,9%28/61
64,2%34/53
0
10
20
30
40
50
60
70
Control
SOC Lead-In
TG4040 Lead-In
cEVR
Percentage
of patients
*
*
p=0,003
Three-outcome one-stage design
based on: Ho < 40 %, HA > 60 %
According to final evaluable set of
patients in pre-vaccination arm:
Null hypothesis accepted if cEVR ≤
25 patients, rejected if cEVR ≥ 29
Wedemeyer H et al. EASL 2013

●●●●●●●●● 17
SVR24 Response Relapse and Viral BreakthroughP
erc
en
t o
f p
ati
en
ts
- ITT: at least one PR
administration
- LOD<10IU/mL
� Viral breakthrough (defined as greater than or equal 100IU/mL increase in HCV
RNA after drop to BLOD) occurred in 5% (3/63) and 2% (1/55) in PR lead-in and
TG4040 pre-treatment arms vs 0% in control arm
n/N = 15/31 32/63 32/55 6/31 6/63 7/55
SVR24 Relapse
Wedemeyer H et al. EASL 2013

TG4040 Induces HCV Specific T-Cell Responses
●●●●●●●●● 18
� NS3 specific ELISpot IFN-γ responses: 46% of patients
� Overall, 71% of patients had TG4040 specific T-cell responses
Baseline TG4040 pre-treatment
W9
W1
2
M-1
D1
TG4040 Pre-Treatment Arm (n=55)
No SFC/106 PBMC < 50 SFC/106 PBMC50-100 SFC/106 PBMC
150-200 SFC/106 PBMC> 200 SFC/106 PBMC
-SFC: Spot-forming cell-PBMC: Peripheral Blood Mononuclear Cells
100-150 SFC/106 PBMC
Representative ELISpot well
Negativecontrol
NS3M
ean
SFC
/10
6P
BM
C
Baseline(M-1; D1)
PegIFN/RBV +
TG4040(W14; W24)
End Of Study(W84)
TG4040 Pre-Treatment(W9; W12)
� Ex: NS3
Wedemeyer H et al. EASL 2013

●●●●●●●●● 19
Induction of Anti-MVA Humoral Immune Responses
� All TG4040 treated patients developed detectable anti-MVA humoral responses
� No significant correlation between neither total nor neutralizing antibodies and
virological response (cEVR and/or SVR24)
W2
W8
W9
W1
2
W1
4
W2
4
D1
Me
an F
old
Ch
ange
fro
m B
ase
line
(D
1)
Neutralizing anti-MVA antibodiesControl Arm
PegIFN/RBV lead-in Arm
TG4040 Pre-Treatment Arm
Wedemeyer H et al. EASL 2013

●●●●●●●●● 20
Cut-off: 24 weeks of PegIFN/riba. in each arm Control (n=31) SOC Lead-In (n=63) TG4040 Lead-In (n=59)
Any adverse events n (%) 27 (87.1%) 58 (92.1%) 57 (96.6%)
Adverse events related to PegIFN & ribavirin 25 (80.6%) 56 (88.9%) 51 (86.4%)
Adverse events related to TG4040 NA 21 (33.3%) 35 (59.3%)
Most common adverse events (more than 15%)(*; significant difference; p ≤ 0,05)
FatiguePyrexiaInjection site erythema*Influenza like illnessInjection site indurationInjection site pruritus
NeutropeniaAnaemiaLeukopenia
HeadacheInsomniaPruritusAlopeciaNauseaDecreased appetiteMyalgia
18 (58.1%)
6 (19.4%)
1 (3.2%) *8 (25.8%)
0
0
9 (29%)
8 (25.8%)
5 (16.1%)
7 (22.6%)
7 (22.6%)
6 (19.4%)
2 (6.5%)
5 (16.1%)
5 (16.1%)
4 (12.9%)
33 (52.4%)
15 (23.8%)
11 (17.5%)
11 (17.5%)
4 (6.3%)
4 (6.3%)
18 (28.6%)
8 (12.7%)
4 (6.3%)
13 (20.6%)
8 (12.7%)
9 (14.3%)
4 (6.3%)
5 (7.9%)
5 (7.9%)
12 (19%)
30 (50.8%)
21 (35.6%)
18 (30.5%) *8 (13.6%)
9 (15.3%)
9 (15.3%)
15 (25.4%)
16 (27.1%)
7 (11.9%)
17 (28.8%)
5 (8.5%)
9 (15.3%)
12 (20.3%)
7 (11.9%)
12 (20.3%)
9 (15.3%)
Grade 3/4 adverse events 7 (22.6%) 15 (23.8%) 13 (23.7%)
Safety

●●●●●●●●● 21
Safety
� As of today, 19 SAEs reported in 13 patients, none related to TG4040 alone
Control SOC Lead-In TG4040 Lead-In Total
Total SAEs (events) 4 11 4 19
Related to PegIFN/ribavirin only 2 5 0 7
Related to TG4040 only 0 0 0 0
Related to TG4040 & PegIFN/ribavirin - 2 3 5
SAEs unrelated to treatments 2 4 1 7
� SAEs related to PegIFN/ribavirin & TG4040 in 4 patients
� Three patients with severe peripheral thrombocytopenia (2 in SOC lead-in arm, 1 in vaccine lead-in
arm) and one patient with aplastic anemia in vaccine lead-in arm
� Recovery of blood parameters in 1 to 4 months, one recent case ongoing
� Common feature between the 3 patients with thrombocytopenia: HLA-DRB1*04 allele (statistical
association p=0.001)
Wedemeyer H et al. EASL 2013

●●●●●●●●● 22
�Pre-treatment with immunotherapeutic TG4040 followed by
PegIFNα2a/RBV significantly increased cEVR as compared to
PegIFNα2a/RBV alone, in treatment-naive patients with genotype 1
HCV: 64% compared to 30%
� In pre-treatment arm, higher SVR24 rate as compared to the
control arm: 58% vs 48%
� And lower relapse rate: 12% vs 19%
�TG4040 alone was generally well tolerated.
However, TG4040 treatment may be associated with exacerbation
of IFNa-related immune side effects in distinct HLA-backgrounds
Summary and Conclusions

●●●●●●●●● 23
�TG4040 induced HCV-specific T cell responses:
46% NS3-specific ELISpot IFN-gamma responses, 71% overall
�T cell and/or B cell responses against MVA were induced in all
patients
Summary and Conclusions
In Conclusion:
This study in chronic hepatitis C illustrates the potential value of viral vector-based immunotherapy for the treatment of chronic infections including viral hepatitis which warrants further evaluation

●●●●●●●●● 24
Acknowledgements
Poland•Robert Flisiak, Bialystok•Mazur Wlodzimierz, Chorzów•Maciej Jablkowski, Lodz•Ewa Janczewska-Kazek, CzeladzSpain•Vicente Carreno, Madrid•Moises Diago, Valencia•Manuel Romero Gomez, Sevilla•Ricardo Sola, Barcelona•Maria Trapero, MadridGermany•Frank Lammert, Hamburg•Ulrich Spengler, Bonn•Heiner Wedemeyer, Hannover•Stefan Zeuzem, Frankfurt
� The patients and their families� The HCVac investigators and their study staff
Romania•Mircea Calistru, Bucharest•Adrian Goldis, Timisoara•Ioan Sporea, Timisoara•Carol Stanciu, Iasi•Coman Tanasescu, BucharestFrance•Thomas Baumert•Cyrille Feray, Nantes•Véronique Grando, Créteil•François Habersetzer, Strasbourg
•Christian Trepo, Lyon•Jean-Pierre Vinel, Toulouse•Jean-Pierre Zarsky•Vicent Leroy
Israel•Yaacov Baruch, Haifa•Alexander Fich, Soroka•Ran Tur Kaspa, Petah Tikva•Yoav Lurie, Tel AvivUSA•Adrian Di Bisceglie, Saint Louis•Eugene Schiff, Miami
� Transgene �Geneviève Inchauspé�Jean Marc Limacher