dr. elizabeth bryce vancouver coastal health making sense out of medical microbiology reports
TRANSCRIPT

Dr. Elizabeth BryceVancouver Coastal Health
Making Sense out of Medical Microbiology Reports

1. Understand what specimens are considered “acceptable”
2. Learn how to interpret a medical microbiology gram stain report
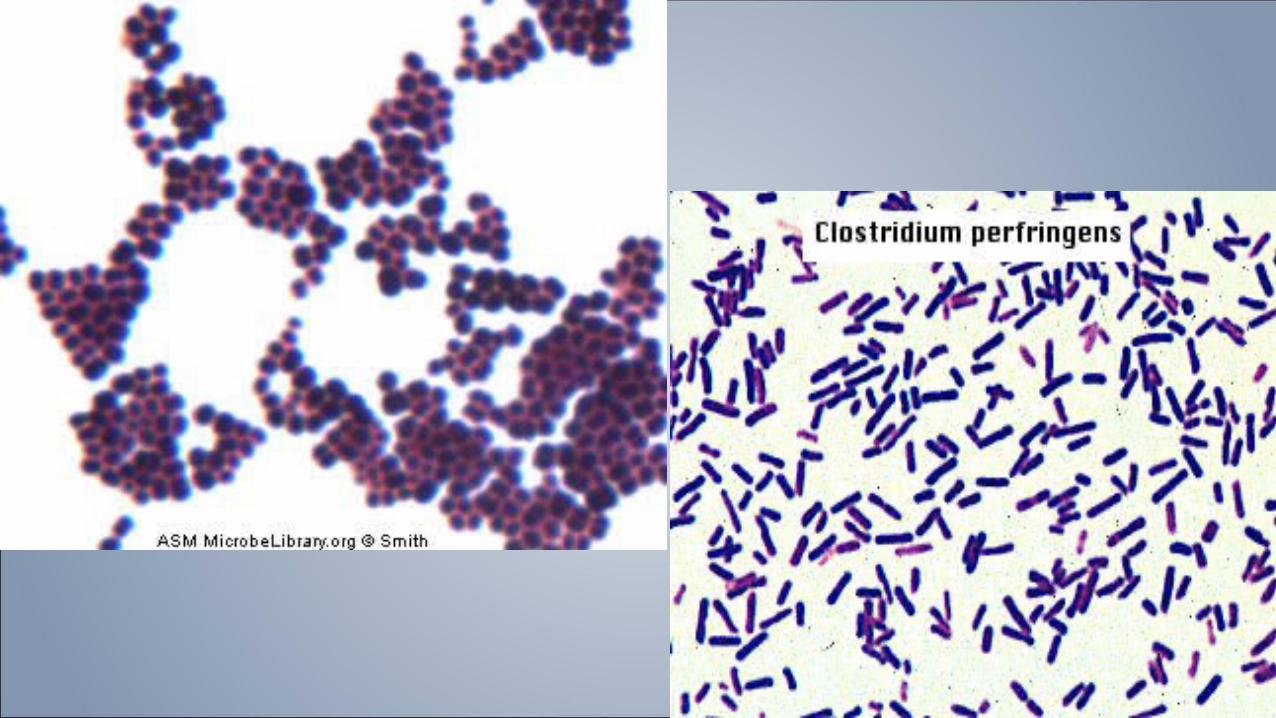
3. Know what the common pathogens are
4. Putting the gram stain and culture report together
5. Using other laboratory reports to help in the decision making
Objectives

› Best if collected prior to antibiotic administration
› Best if collected early in the course of disease
› Swabs generally poor specimens compared to actual body fluids or tissues which are quite reliable
› “Deep” specimens always best e.g. sputum vs spit, deep wound vs superficial, etc…
General concepts for specimen collection
Tip One: Look at the description of the specimen

› Anaerobic cultures for urine, respiratory samples, most GI samples, most perirectal samples
› Cultures of objects/devices e.g. contact lens cases, urine from bedpans, urinary catheters, drainage bags, drain tips, trach tubes Exceptions: central line tips
› Broken, damaged, leaking specimen container
› Too long in transit or wrong temperature (e.g. CSF)
Unacceptable specimens

Contaminants versus Pathogens› Some organisms more associated with colonization
E.g. coagulase negative staphylococci, diphtheroids
› Others are always pathogenic E.g. Legionella, Shigella, Listeria
› But most fall in between so:
1.Consider the body site: sterile body site versus mucous membrane
2.Look to see if there are multiple specimens with same organism
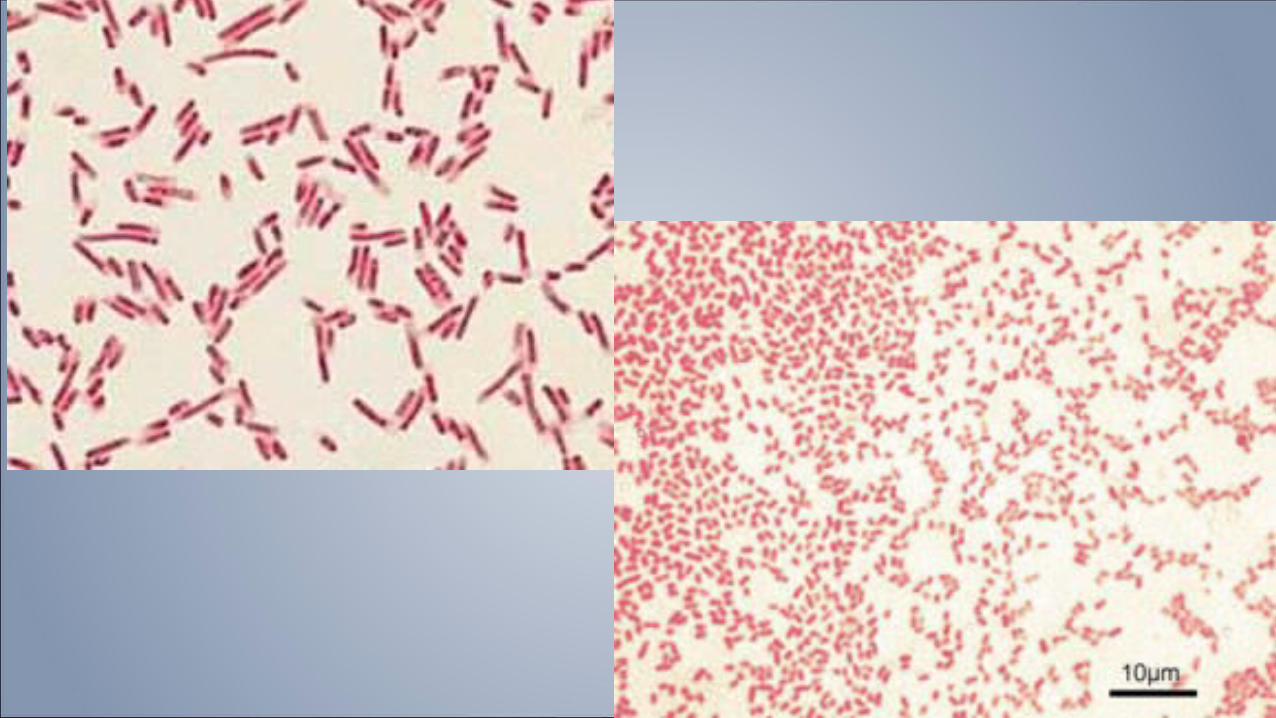
3.Look at the gram stain …….

› Assesses the quality of the specimen
› Gives an early indication of degree of inflammation
› Gives an early indication of possible pathogens
› Guides the workup of the specimen
The all-important Gram Stain
Tip 2: Always compare the gram stain to what grows in culture. Do they correspond?



Fraught with interpretive problems because– Specimen request not fully completed and lab treats as a
superficial wound– Inappropriate sample sent (e.g. swab rather than
fluid,tissue)– Specimen placed directly into a broth media and lab has no
gram stain to guide them (problematic for radiology specimens)
–Medical Microbiologists and lab techs may differ in their opinion as to what is a “significant” amount or type of organism to report
– Sometimes “normal flora” can cause infection
Wound Specimens

Unable to interpret or poor quality specimens

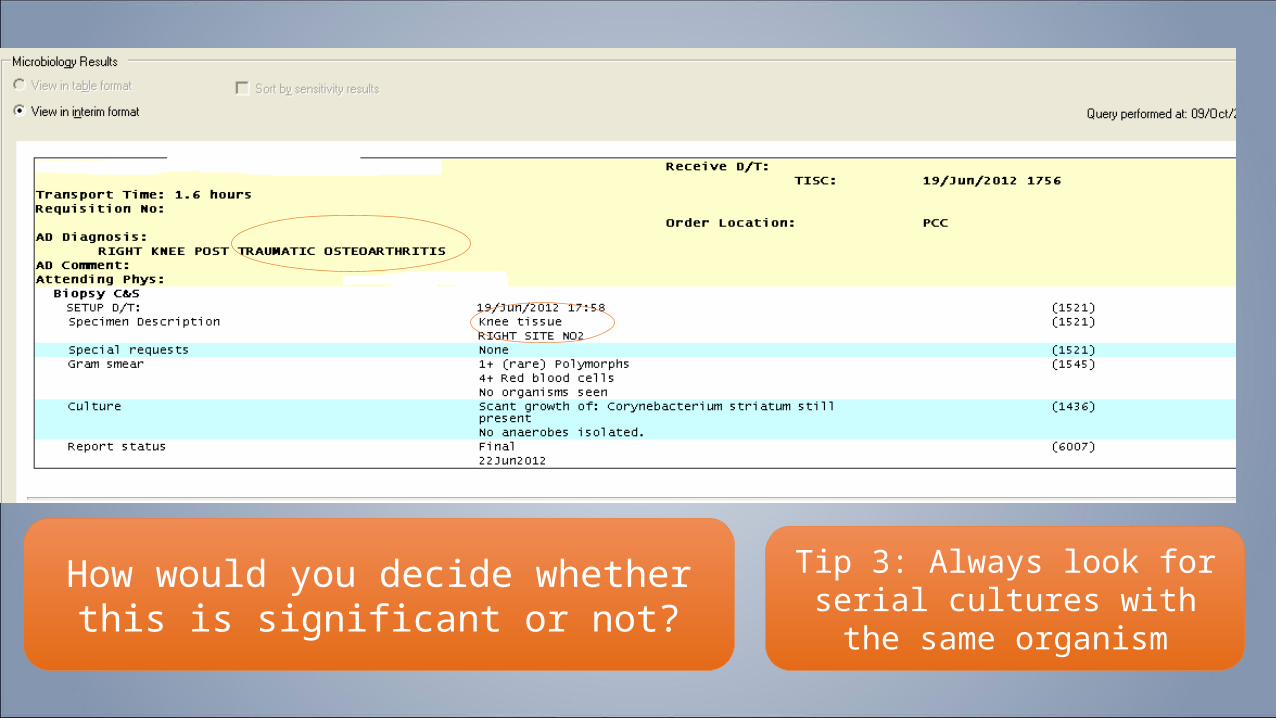
How would you decide whether this is significant or not?
Tip 3: Always look for serial cultures with the same organism


› Large spectrum of disease and types of samples: sinuses, ears, tracheal aspirates, sputum, bronchoscopy specimens, biopsies…..
› Complicated by presence of normal respiratory flora from the mouth AND the fact that sometimes normal flora can cause disease AND because sometimes “pathogens” just represent colonization in chronic lung disease
› Gram stain very important in interpretation of the quality of the specimen
Respiratory samples

Is it a good specimen – why or why not?If it is Haemophilus – are all species pathogenic?

A good quality specimenA diagnosis that points to clinical significance
Why isn’t there a pathogen described?What could this represent?
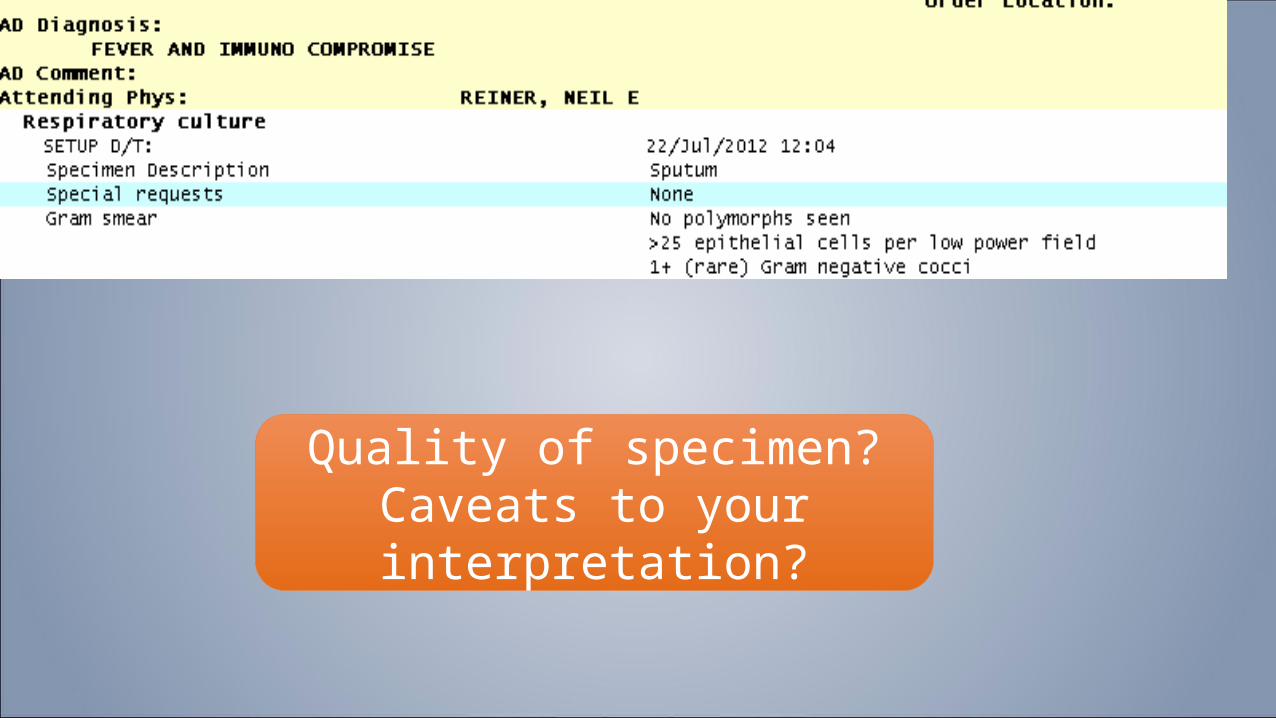
Quality of specimen?Caveats to your interpretation?
Symptoms PLUS radiology PLUS
› BAL with intracellular bacteria on gram stain
› Pos Blood culture without another source
› Pos culture of pleural fluid
› Pos LRT specimen (BAL or protected brush)
NSQIP definition
Uncommon to see intracellular bacteria
Even from a drain?
Still can get a contaminant
Missing: good quality specimen (+++ polys, 0 epithelial cells, 3-4+ organisms)

And now for something completely different: ……Urines

Significant colony counts
>108 CFU/L but…. Catheter vs voided
specimen differ
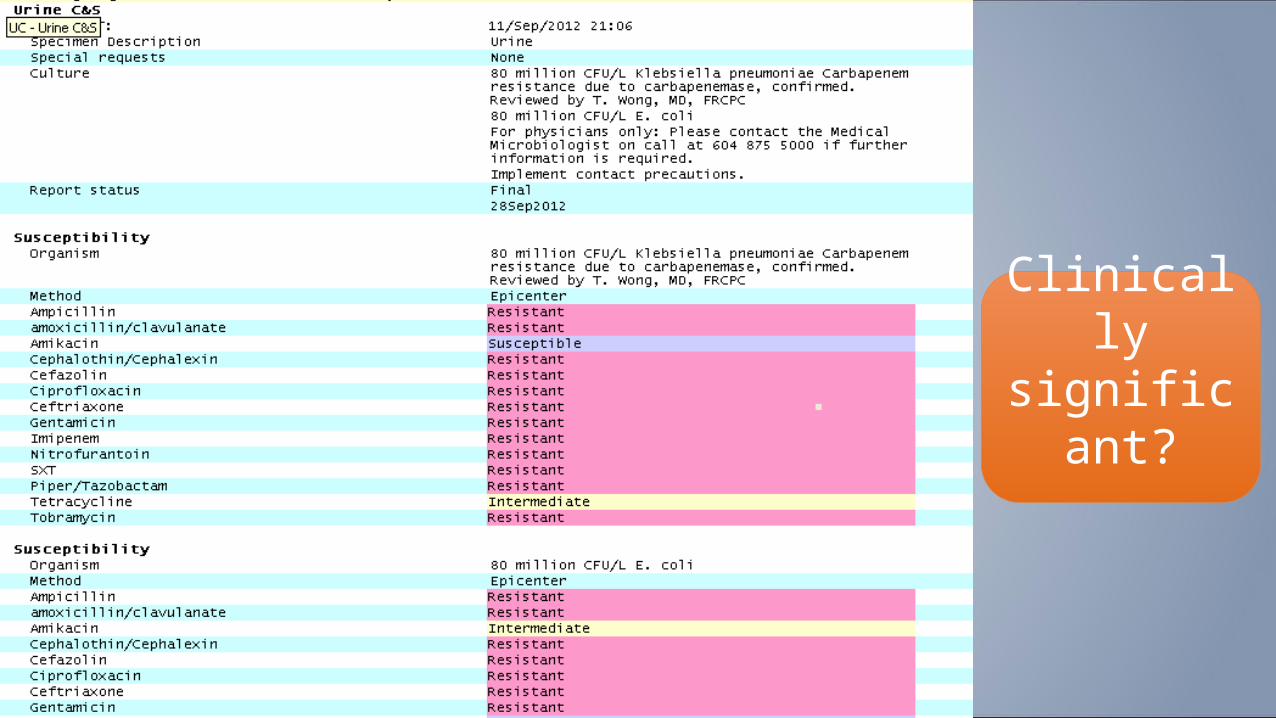
Clinically significant?

The importance of the urinalysis
IMPORTANT:Urinalysis much more reliable than dipstick because:1)Dipstick has a finite lifespan2)Must be kept in a closed container (not exposed to air
Testing with outdated and improperly stored materials leads to erroneous results.

Helpful:Nitrites (not Nitrates):
very specificBacteria in Gram Stain (but not usually done)
Maybe helpful:Leukocyte Esterase
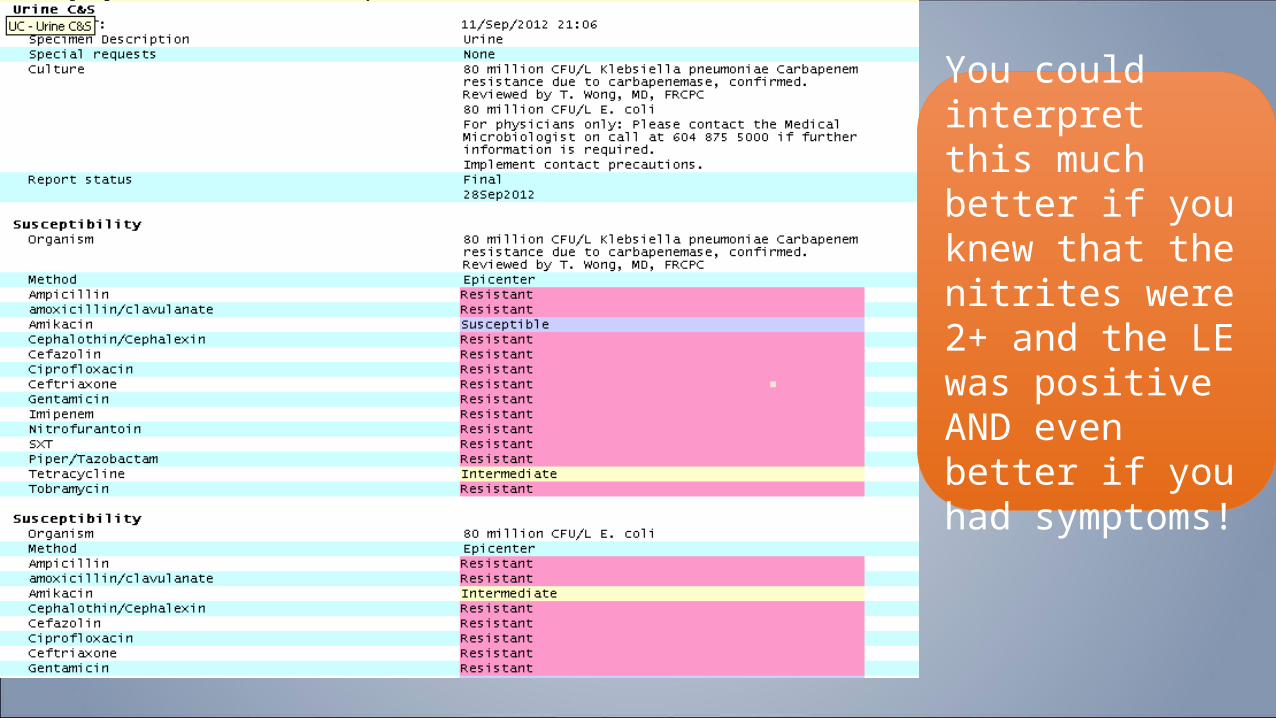
You could interpret this much better if you knew that the nitrites were 2+ and the LE was positive AND even better if you had symptoms!
NSQIP - UTISymptoms PLUS
› Urine culture > 108/L with no more than two species
OR Symptoms Plus
› Pos dipstick for LES and/or nitrate
› Pyruria or positive direct gram stain
› 105/L in non-voided specimen x 2, same pathogen
Lab doesn’t do this
No specification as to skin contaminants
Often these are not clinically
significant

Blood cultures
Interpretation not always easy….
a)Contamination from HCWs skin/poor techniqueb)Normal skin flora and only one blood culture set drawnc)Samples drawn from a compromised site

CDC Recognized pathogen from one or more blood cultures. Pathogen not related to an infection at another site OR patient with at least one:
fever, chills, and/or hypotension
and positive laboratory cultures from two or more blood samples drawn on separate occasions not related to infection at another site and do not reflect contamination.
CLABSI: One of the following must be met:
• Same organism from both the catheter tip and at least one percutaneous blood culture.
• Same organism from at least two blood samples (one from a catheter hub and the other from a
peripheral vein or second lumen) meeting criteria for quantitative blood cultures or differential time to positivity
• Quantitative Culture-colony count from catheter ≥3 fold the peripheral sample
Defining Central Line Blood Stream Infections

SIRS symptoms PLUS
› Positive blood culture
› Clinical documentation of purulence or positive culture from any site…..documenting cause of sepsis
NSQIP definition
Number of positive bottles orSkin contaminants
Differential time to positivityBlood cultures matching clinical culture elsewhere
Catheter growth < 2 hrs before growth from peripheral sample.
• Sensitivity 85% and specificity 91%Is available on request (machines can calculate the DTP)Underutilized
Differential time to positivity

How do you decide whether clinically significant or not?

Conclusions› The lab is only as good as the information it receives and the
quality of specimen sent
“Garbage in – Garbage out”
› There are “clues” a) gram stain with lots of polymorphs b) the type of organism and the body site c) presence of organism on multiple specimens and/or sites d) helpful ancillary tests (urinalysis) e) symptoms (if they are recorded)
› If in doubt – give us a call!