down's syndrome and fragile-x syndrome in a single patient
TRANSCRIPT
Journal of Menial Deficiency Research., 1990, 34, 81-86
CASE REPORT
Down's syndrome and fragile-X syndrome in asingle patient
R. A. COLLACOTT,' D. P. DUCKETT,^ D. MATHEWS/J. S. WARRINGTON' AND I. D. YOUNG^
'The Frilh Hospital, and Departments of ^Cytogenetics and ^Child Health, The RoyalInfirmary, Leicester, England
ABSTRACT. A profoundly menially handicapped patient is described with thekaryotype 47,X, fra (X) (q27), + 21. Her phenoiype demonstrates features of bothDown's Syndrome and fragile-X syndrome. The authors believe only one other similarcase has been described.
I N T R O D U C T I O N
Arinami et al. (1987) have recently described a female mentally handicapped patientin whose karyotype trisomy 21 was associated with the fragile-X chromosome. Mostof the facial characteristics of their patient were those observed in Down's syndrome,but other features such as the large ears, long face with prominent forehead and lowerjaws, related closely to the fragile-X syndrome. They suggested that there wasprobably no aetiological relationship between the two chromosomal abnormalities,since the maternal age at delivery was 40 years. The present authors describe a secondcase of a young female in which Down's syndrome is associated with fragile-X syn-drome, in a family with familial mental retardation. Aspects of this patient's pheno-type reflect both chromosome disorders (Fig. 1).
CASE R E P O R T
The patient is the eighth child of parents of Afro-Caribbean origin, who emigratedfrom Montserrat in 1961. She was born at home as the product of a normal full-termpregnancy. Little antenatal care had been received. This patient's birth weight was4-56 kg and her condition at birth was described as excellent. Maternal and paternalages at the birth of the patient were 41 and 47 years, respectively. The patient had no
Correspondence: Dr Richard A. CoUacotty Consultant in Mental Handicap, The Frith Hospital,Groby Road, Leicester LE3 9QF, England.
81

82 R. A. Collacolt et al.
'-Or O
d
•a
Down's and fragile-X syndromes 83
serious illnesses in infancy or later childhood, and she continues to enjoy goodphysical health.
An elder brother (111,1) had died in Montserrat aged 5 months of an unknowncause. A second brother (111,3) attended a school for the mentally handicapped andcurrently attends an adult training centre. Another brother (111,5) also attended aschool for the mentally handicapped. Now aged 27, he is unemployed and stays athome with his unemployed father and mother.
Two sons of our patient's half-sister (IV,6 and IV,8) have also attended E.S.N.-Mschools, of whom one (TV,6) currently attends an adult training centre. Otherrelatives (1,6; 1,7; 111,9; 111,11; 111,13; 111,14; 111,17; and 111,18), still hving in theWest Indies, are considered to be educationally backward.
The patient is now aged 21 years. She was considered to be mentally handicappedduring infancy on account of marked developmental delay. On the Vineland AdaptiveBehaviour Scales, she obtained an Adaptive Behaviour Composite standard score of20. This translates into an age equivalent of 21 months. Her age equivalents withinthe communication, daily living skills and socialization domains are 21, 26 and 15months, respectively. Her age equivalent for motor skills is 23 months. She is unableto read or write. She speaks in short indistinct phrases only. She does not understandthe value of money. She is unable to dress, undress, wash or clean her teethindependently. She feeds with a knife, fork and spoon. She is regularly incontinent ofurine both by day and night. She is only partially mobile, being unable to walkdownstairs alternating her feet. She is limited in her affective responses. There is no
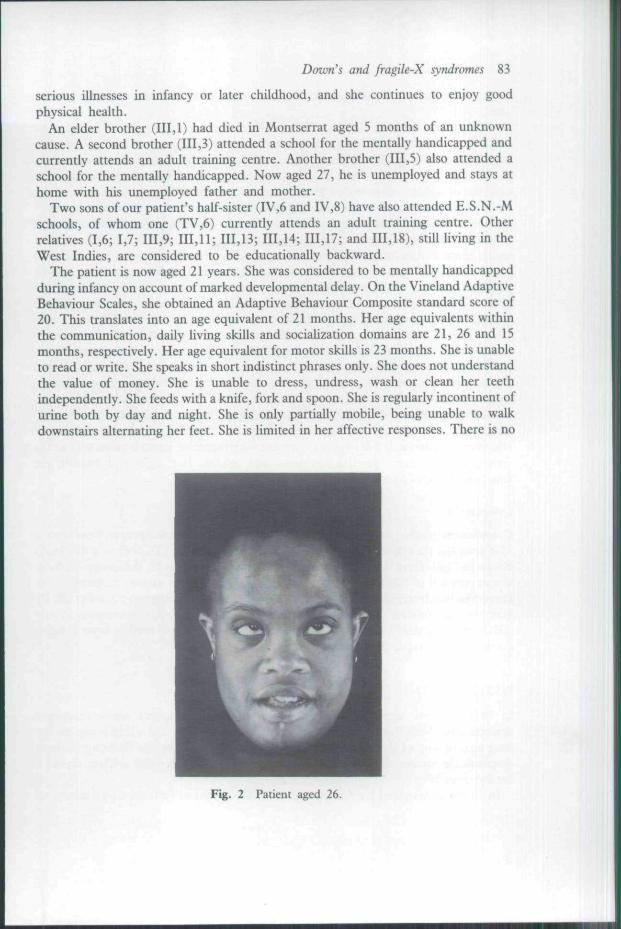
Fig. 2 Patient aged 26.

84 R. A. Collacott et al.
object attachment, obsessive desire for sameness, gaze avoidance or other autistictraits.
The patient has a psychiatric history which includes a variety of maladaptivebehaviours, such as stereotypic movements, over-activity, screaming and self-injurious behaviour. These include body rocking, biting her hands and wrists, tearingat the skin of the neck, head-banging, eye-poking and hair pulling. In addition,episodes of sudden uncontrolled physical aggression against people and property andencopresis have occurred. These maladaptive behaviours have largely subsided sincethe introduction of Carbamazepine 18 months ago, but recur when it is withdrawn.
Clinical examination shows the patient to be of Afro-Caribbean extraction and ofshort, obese stature (height 140-5 cm). Her head is of brachycephaiic appearance witha circumference of 52-0 cm. She has marked epicanthic folds, upwardly slopingpalpebral fissures and a convergent concomitant strabismus. Brushfield spots areabsent. The tongue is protruding, with marked dribbling. The jaw shows pronouncedmandibular prognathism. The lips are thick and the lower lip everted. The forehead ishigh (Fig. 2). The ears are normally positioned and small. The secondarydevelopment of the left ear, which protrudes, is poor. Secondary sexual characteristicsare normally developed. The hands show short stubby fmgers with a left bridgedsimian palmar crease. Dermatoglyphic studies show whorls on the ring and littlefingers bilaterally with ulnar loops on all other digits. The toes are short and fat, witha wider space between the first and second toes. The fourth toes are overlapping.There are no abormalities to be found with the chest, cardiovascular system orabdomen. Evidence of joint laxity is present with increased passive movement at thewrists, fingers, hips, patellar hgaments and ankles. Her sight and hearing arefunctionally satisfactory.
Cytogenetics
Chromosome studies on unbanded and sequentially GTG banded preparations from a72-h lymphocyte culture grown in a low folic acid medium (TC 199 -f 2-5% FCS)showed all cells from the patient to have an extra chromosome 21. Additionally, therewas expression of the fragile-X in eight (16%) of the 50 metaphases examined. Herkaryotype was interpreted as 47,X, fra (X) (q27), + 21. Investigation of other familymembers has to date confirmed the presence of the fragile-X chromosome in one(111,3) of the patient's two retarded brothers. Therefore, their mother is an obligatecarrier of the fragile-X chromosome.
D I S C U S S I O N
In 1987, Arinami and his colleagues described a female patient whose karyotypedemonstrated both the presence of an extra chromosome 21 and a fragile site on thelong arm of one of the X chromosomes. A recent search of the literature fails todemonstrate further descriptions of this association. The present authors report asecond case here.
In the case described by Arinami et al. (1987), physical features characteristic of
Down's and fragile-X syndromes 85
Down's syndrome were present. In addition, features suggestive of the fragile-Xsyndrome, namely a long face with prominent forehead, large ears, and a prominentlower jaw were also noted (Jennings et al., 1980). Although the facial features of thefragile-X syndrome have not yet been fully established, such features and mentalretardation are sometimes noted in carrier females (Fryns, 1986; Loesch & Hay,1988). Whereas most features are those of Down's syndrome, characteristics offragile-X syndrome, namely prominent forehead and prognathism are also present inthis patient. However, the ears are small, and the left side poorly developed andprominent (bat-ear).
The pedigrees of both cases show several family members in whom intellectualretardation is present. Cytogenetic studies of one of our patients mentallyhandicapped brothers also demonstrates the presence of a fragile site on the Xchromosome.
Both the patient described by Arinami et al. (1987) and the one presented here areprofoundly mentally handicapped. In other patients who have been described inwhom fragile-X syndrome has been associated with an additional chromosomalabnormality such as Klinefelter's syndrome, intellectual performance has been shownto be very severely impaired (Dunn et al, 1963: Fryns et al, 1984). This patient'sintellectual functioning is well below that of most patients with Down's syndrome.Additionally, she functions at a much lower level than her other handicapped malesiblings.
Watson et al. (1986) suggested that there was an increased risk of aneuploidyamongst the offspring of female carriers of the fragile-X syndrome. Although thepresent authors cannot ignore this suggested association, the maternal age at birth was41 in our patient. It is suggested that the non-disjunctional event in this case was,therefore, related to maternal age rather than to an interchromosomal effect involvingthe fragile-X chromosome carried by the mother. Further reports are necessary, assuggested by Arinami et al. (1987), to determine whether such increased risks ofaneuploidy exist.
A C K N O W L E D G E M E N T S
The authors wish to acknowledge the considerable assistance received from ourpatient's parents. In addition, we wish to thank the community nursing staff for theirassistance in examining the patient, Mrs Liliane McManus for her skill in decipheringthe original manuscript and Mrs Angela Pollard, Librarian, Frith Hospital, forconducting the literature search.
REFERENCES
Arinami T. et al (1987) A fragile X female with Down's syndrome. Human Genetics 11, 92-A.Dunn H. G. et al (1963) Mental retardation as a sex-linked defect. American Journal of Mental
Deficiency 67, 827-^8.Fryns J. P., Kleczkowska A., Wolfs I. & van den Berghe H. (1984) Kleinfelter syndrome and
two fragile X chromosome. Clinical Genetics 21, 445-7.

86 R. A. Collacott et al.
Fryns J. P. (1986) The female and fragile X. A study of 144 obligate female carriers. AmericanJournal of Medical Genetics 23, 157-^9.
Jennings M., Hall J. G. & Hoehn H. (1980) Significance of phenotypic and chromosomalabnormalities in X-linked mental retardation. American Journal of Medical Genetics 7,417-32.
Loesch D. Z. & Hay D. A. (1988) Clinical features and reproductive patterns in fragile Xfemale heterozygotes. Journal of Medical Genetics 25, 407-14.
Watson M. S. et al. (1986) Increased risk trisomy 21 offspring to fragile X carrier females?American Journal of Human Genetics 39, A137.
Received 2 August 1988; revised 13 October 1988
