
www.england.nhs.uk
Safer Medication & Medical Devices
Medication Safety & Hospital Admissions Avoidance
30th June 2015
Dr Ahmed AmeerMedication Safety Officer

www.england.nhs.uk
Outline for Session
• How big is the issue?• Is the situation getting better or worse?• Medication Review taken seriously enough?• What should we all be doing about it?
www.england.nhs.uk
Important academic references
• 11.2% patients had adverse drug events (ADEs) causing hospital admission (47.6% preventable)
• Patient age , time since starting new medicine and total number of medicines independently predictors of admission
• Antiplatelets, anticoagulants , diuretics, ACE inhibitors and anti – epileptics major culprits
Kongkaew, C., Hann, M., Mandal, J., Williams, SD, Metcalfe, D., Noyce, P. & Ashcroft, D. Risk Factors for
Hospital Admissions Associated with Adverse Drug Events. Pharmacotherapy 2013; 33: 827-837
www.england.nhs.uk
Important academic references
• 6.5% UK hospital patients admitted due to Adverse Drug Reactions (ADRs)
(72% preventable) Pirmohamed et al BMJ 2004;329:15-19
• Preventable drug related problems accounted for 3.7% of hospital admissions. Antiplatelets, Diuretics, NSAID’s accounted for 50% of all admissions Howard et al BJCP 2007;63:136-4
• 20.8% patients readmitted to hospital due to ADR within 1 year of first admission.
Diuretics & Antiplatelets most frequent
culprits Davies EC et al BJCP 2010;70:749-55
www.england.nhs.uk
www.england.nhs.uk
BUT under recognised because under reported ?
• International Classification of Disease (ICD) coding from hospital databases are not reliable for identifying ADRs Hohl CM,Karpov A, Reddekopp Let al. ICD-10 codes used to identify
adverse drug events in administrative data: a systematic review J Am Med Inform Assoc 2014;21:547–557
• Only 9% of adult patients admitted to a UK hospital with a confirmed medication related harm (ADRs , medication errors, non-adherence) had a related ICD
code documented. Reynolds M et al. A descriptive exploratory study of how
admissions caused by medication-related harm are documented within inpatients’ medical records. BMC Health Service Research 2014; 14: 257
• Hohl CM,Karpov A, Reddekopp Let al. ICD-10 codes used to identify adverse drug events in
administrative data: a systematic review J Am Med Inform Assoc 2014;21:547–557

www.england.nhs.uk
BUT under recognised because under reported ? (2)
• 31.5% of children admitted to a UK hospital with a confirmed ADR had a related ICD code documented Bellis et al. BMC Pharmacology and Toxicology 2014, 15:72. Clinical coding of prospectively identified paediatric adverse drug reactions – a retrospective review of patient records

www.england.nhs.uk
And the situation is only getting (and will get even) worse

www.england.nhs.uk
www.england.nhs.uk
Polypharmacy meets Multi-morbidity
www.england.nhs.uk
Medication Reviews
www.england.nhs.uk
And there are plenty of tools to help
• NICE Medicines Optimisation guidance • Kings Fund , Scottish and Welsh Polypharmacy
documents (CPPE focus too 2016)• Seven steps to managing polypharmacy: Specialist
pharmacy Services document• Reducing Inappropriate Polypharmacy: The Process
of Deprescribing Scott IA et al JAMA Intern Med 2015.
doi:10.1001/jamainternmed.2015.0324
• STOPP START Gallagher P et al Int J Clin Pharmacol Thera 2008;46:72-83
• No Tears Using the NO TEARS tool for medication review. T Lewis. BMJ 2004;329:434
www.england.nhs.uk
Medication Review taken seriously enough?
Can we compare it with a routine Total Knee Replacement (TKR) ?
www.england.nhs.uk
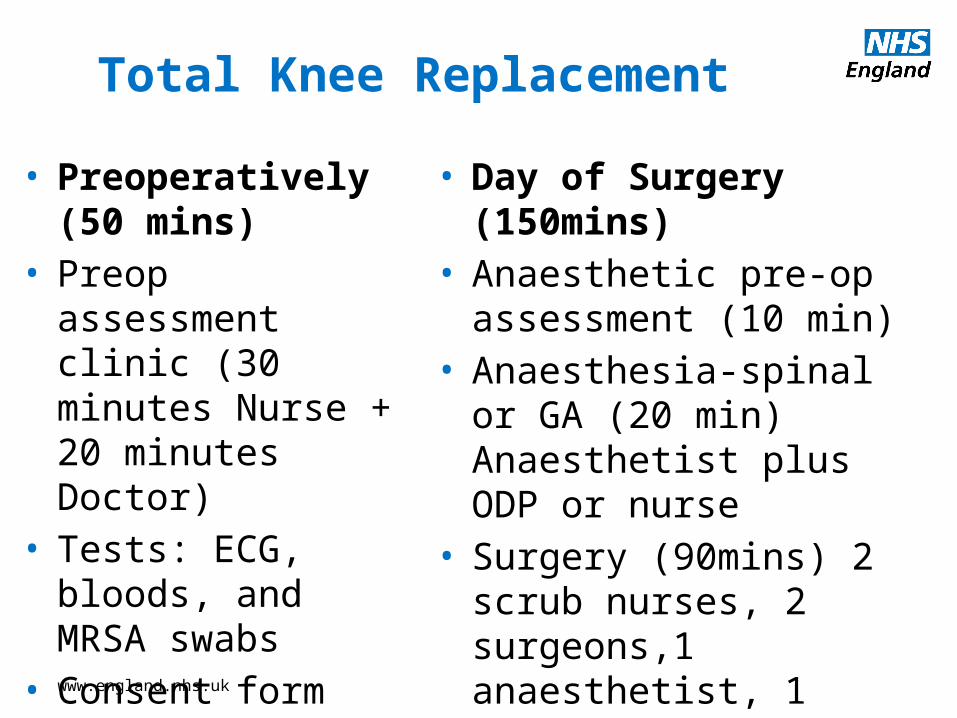
Total Knee Replacement
• Preoperatively (50 mins)
• Preop assessment clinic (30 minutes Nurse + 20 minutes Doctor)
• Tests: ECG, bloods, and MRSA swabs
• Consent form
• Day of Surgery (150mins)• Anaesthetic pre-op
assessment (10 min) • Anaesthesia-spinal or GA
(20 min) Anaesthetist plus ODP or nurse
• Surgery (90mins) 2 scrub nurses, 2 surgeons,1 anaesthetist, 1 runner
www.england.nhs.uk
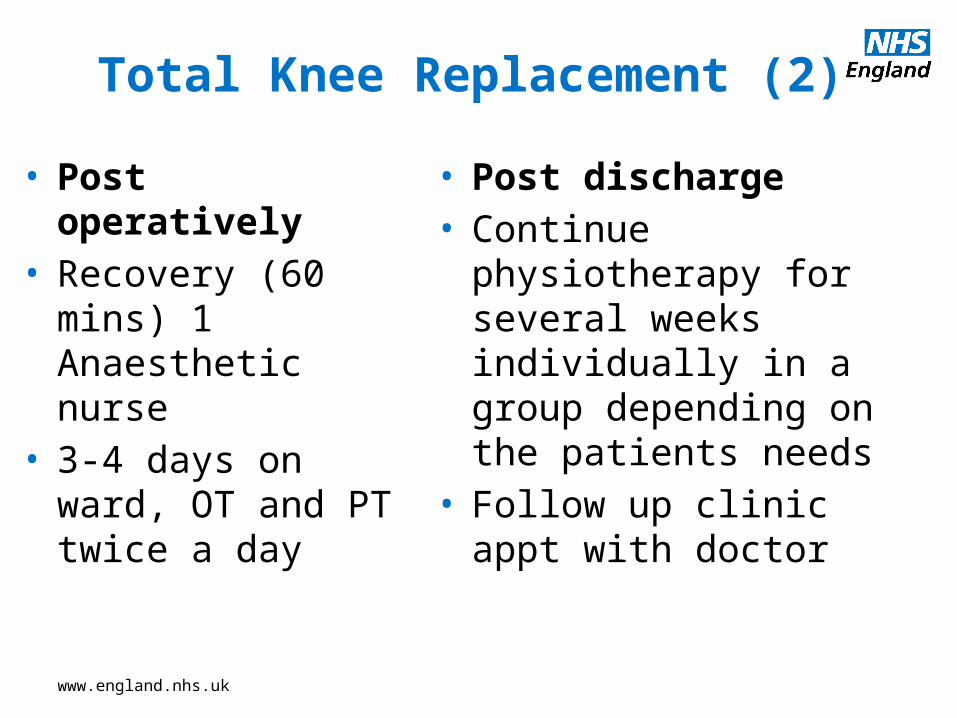
Total Knee Replacement (2)
• Post operatively• Recovery (60 mins)
1 Anaesthetic nurse• 3-4 days on ward,
OT and PT twice a day
• Post discharge • Continue physiotherapy for
several weeks individually in a group depending on the patients needs
• Follow up clinic appt with doctor
www.england.nhs.uk
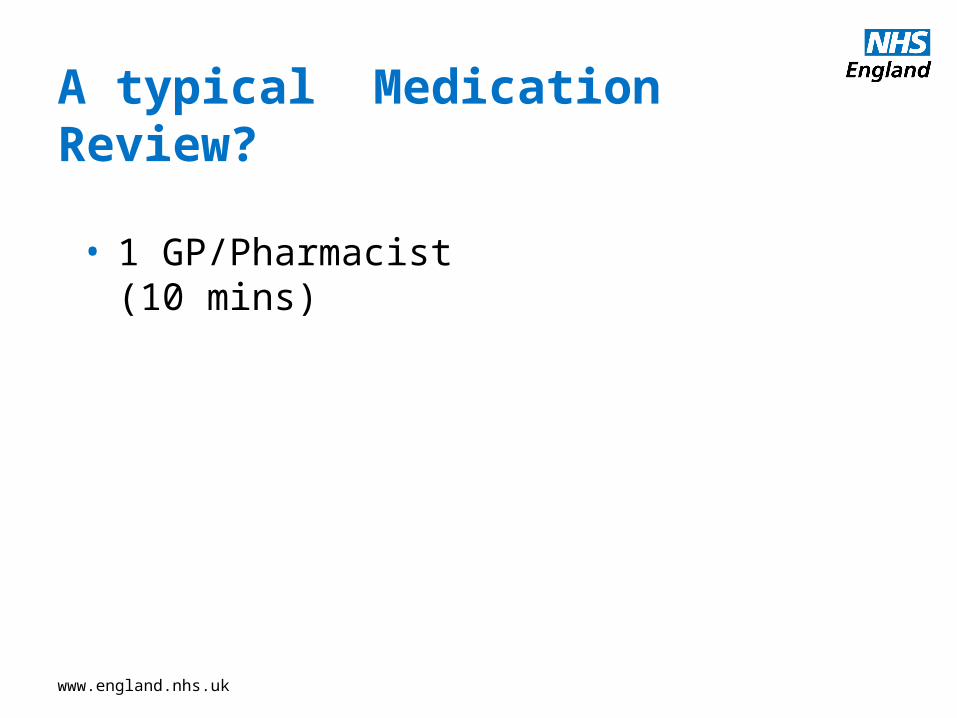
A typical Medication Review?
• 1 GP/Pharmacist (10 mins)
www.england.nhs.uk
So what could the NHS be doing about it ?
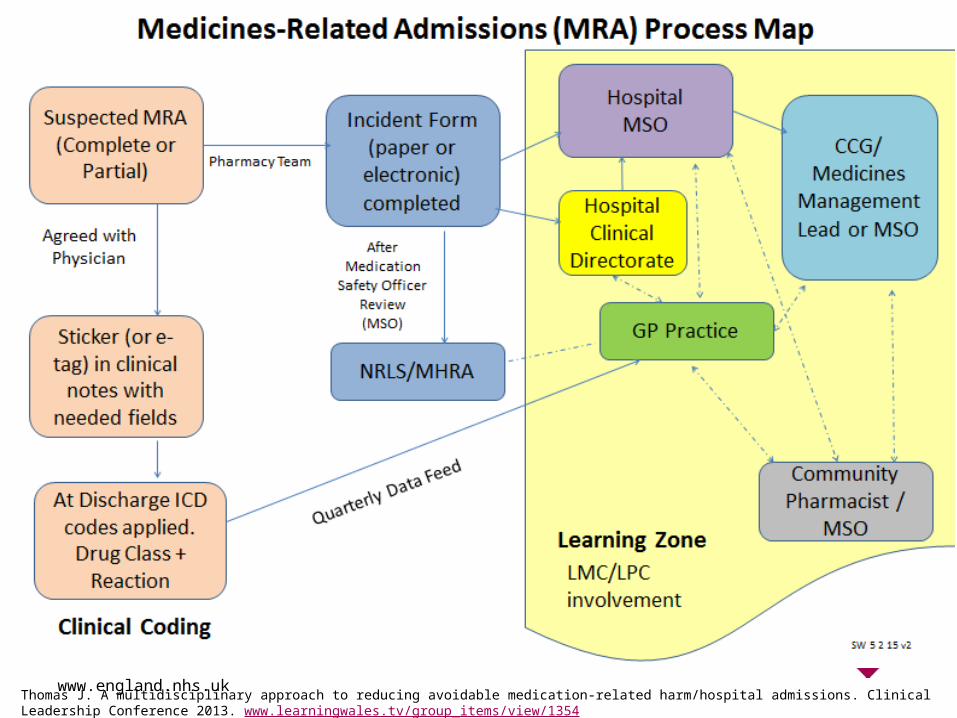
www.england.nhs.ukThomas J. A multidisciplinary approach to reducing avoidable medication-related harm/hospital admissions. Clinical Leadership Conference 2013. www.learningwales.tv/group_items/view/1354

www.england.nhs.uk
2020: NHSE Medicines Optimisation Dashboard to include Medication related admissions per CCG ?
www.england.nhs.uk
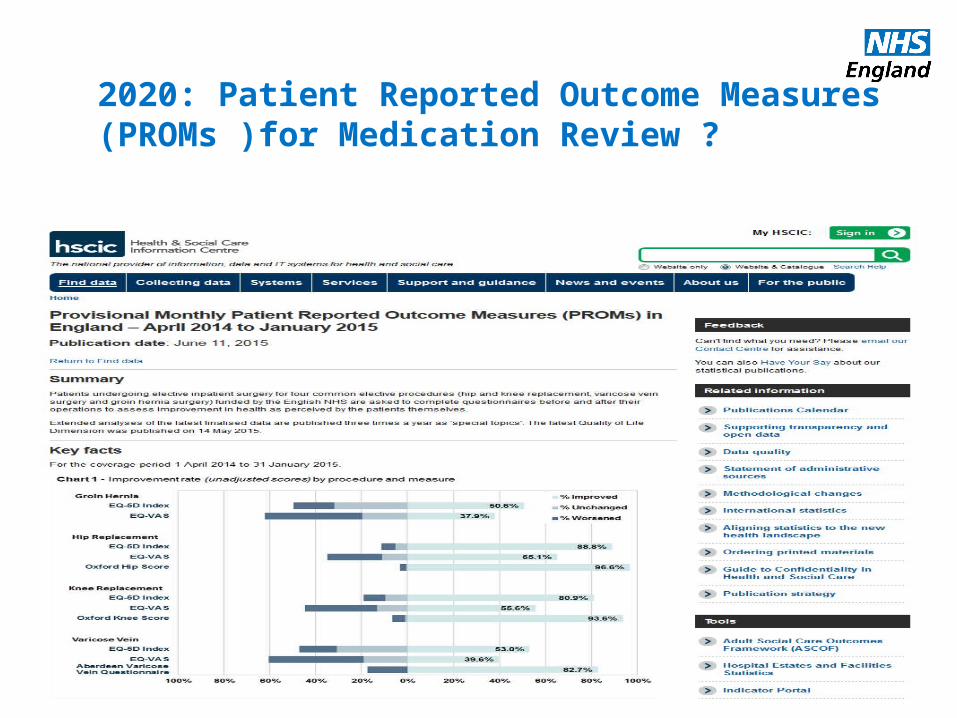
2020: Patient Reported Outcome Measures (PROMs )for Medication Review ?
www.england.nhs.uk
www.england.nhs.uk
www.england.nhs.uk
www.england.nhs.uk
But finally what could YOU be doing about it ?

www.england.nhs.uk
www.england.nhs.uk
Is balancing the Prescription Equation your key to medication related admissions avoidance?
“If we just keep adding, and not subtracting, we just multiply the medication problems”
www.england.nhs.uk
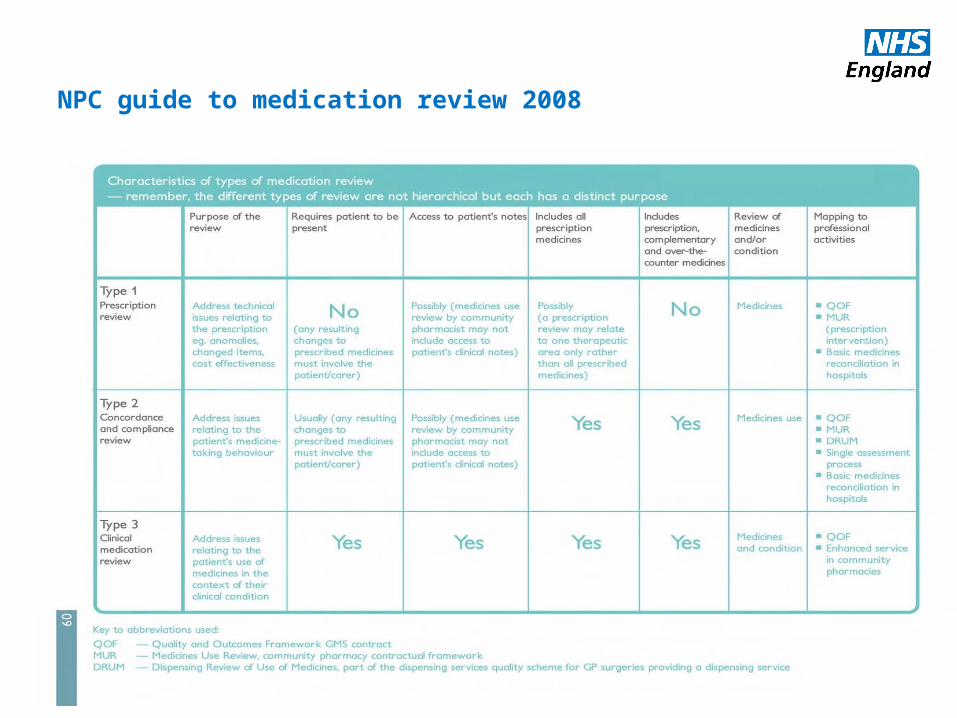
NPC guide to medication review 2008
www.england.nhs.uk
Important References

www.england.nhs.uk







