1
What is non-Hodgkin lymphoma, how is it treated, and what is the
unmet need?
Tim Illidge BSc PhD MRCP FRCR FRCPathInstitute of Cancer Sciences,
University of ManchesterManchester Cancer Research Centre,
Manchester, UK
2
Professor Tim Illidge
• Professor of Targeted Therapy and Oncology at the Institute of Cancer Sciences, the Christie NHS Foundation Trust in Manchester, UK
• Fellow of the Royal College of Radiologists and the Royal College of Pathologists, and Member of the Royal College of Physicians
• Researches new antibody-based therapies for lymphoma
• Has led many early- and late-phase clinical trials
• Author of >100 publications
• Co-Chair of Nordic Nanovector's Scientific Advisory Board
2
3
Non-Hodgkin lymphoma
3
4
Non-Hodgkin lymphoma
• Approximately 1.5 million people worldwide are living with non-Hodgkin lymphoma (NHL)
• 81% increase in incidence of NHL between 1973–1990
• NHL is the third fastest growing cancer in the world (excluding the US) in terms of population
• An estimated 300,000 people die each year from NHL and it is the leading cause of death due to cancer in men aged 20–40 years
Based on US statistics4
5
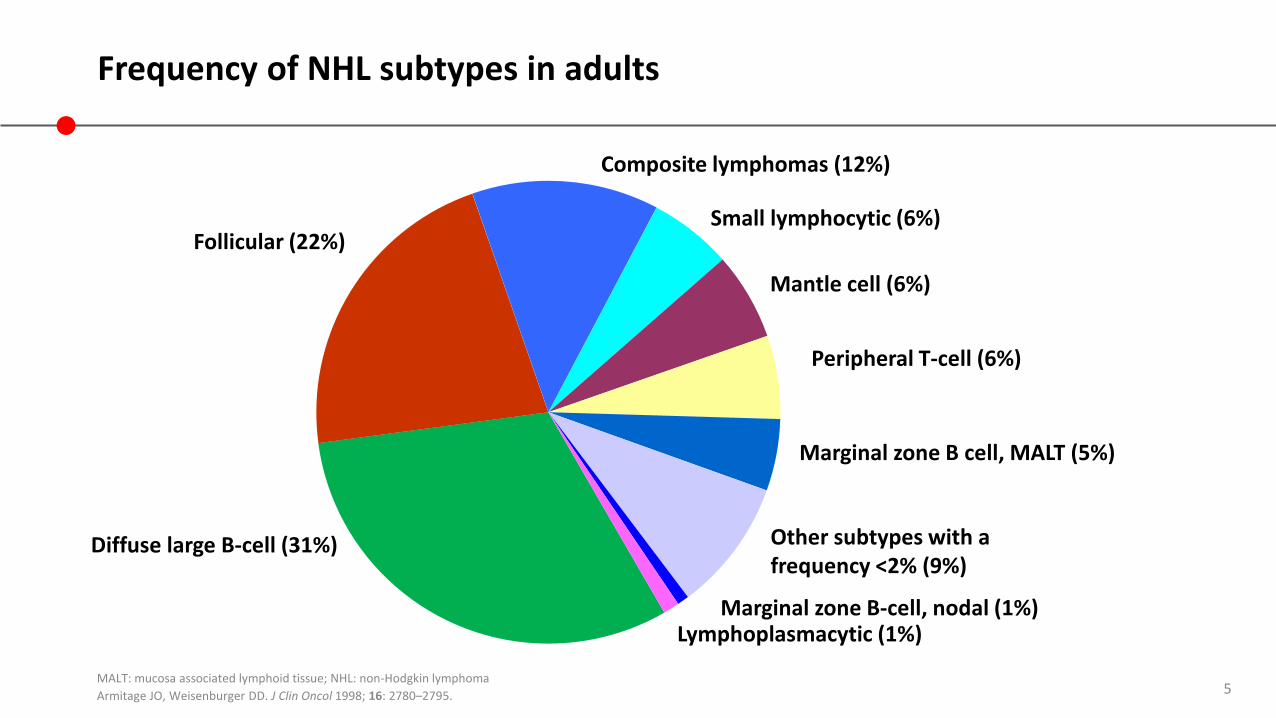
Frequency of NHL subtypes in adults
MALT: mucosa associated lymphoid tissue; NHL: non-Hodgkin lymphoma
Armitage JO, Weisenburger DD. J Clin Oncol 1998; 16: 2780–2795.
Follicular (22%)
Diffuse large B-cell (31%)
Small lymphocytic (6%)
Mantle cell (6%)
Peripheral T-cell (6%)
Marginal zone B cell, MALT (5%)
Other subtypes with a frequency <2% (9%)
Marginal zone B-cell, nodal (1%)Lymphoplasmacytic (1%)
Composite lymphomas (12%)
6
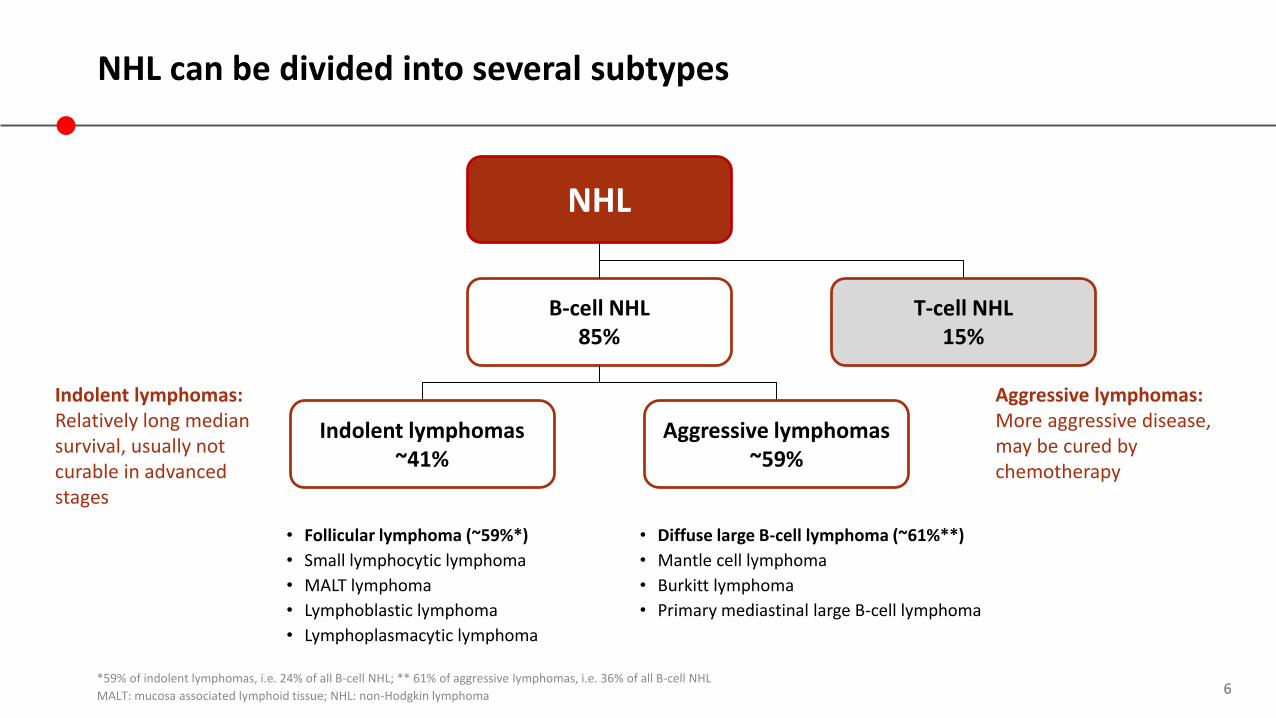
B-cell NHL85%
NHL can be divided into several subtypes
*59% of indolent lymphomas, i.e. 24% of all B-cell NHL; ** 61% of aggressive lymphomas, i.e. 36% of all B-cell NHL
MALT: mucosa associated lymphoid tissue; NHL: non-Hodgkin lymphoma 6
• Follicular lymphoma (~59%*)
• Small lymphocytic lymphoma
• MALT lymphoma
• Lymphoblastic lymphoma
• Lymphoplasmacytic lymphoma
• Diffuse large B-cell lymphoma (~61%**)
• Mantle cell lymphoma
• Burkitt lymphoma
• Primary mediastinal large B-cell lymphoma
Aggressive lymphomas: More aggressive disease, may be cured by chemotherapy
Indolent lymphomas: Relatively long median survival, usually not curable in advanced stages
Indolent lymphomas~41%
Aggressive lymphomas~59%
NHL
T-cell NHL15%
7
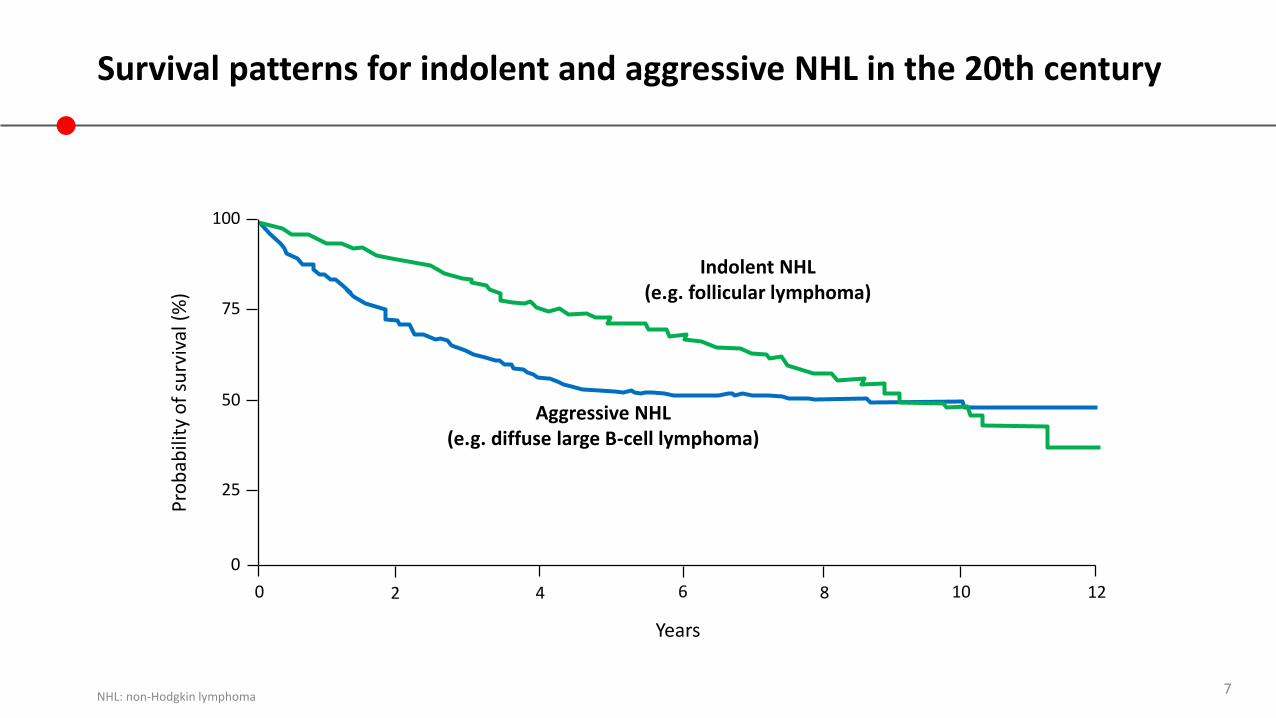
0 2 4 8 126 10
0
25
50
75
100
Pro
bab
ility
of
surv
ival
(%
)
Years
Indolent NHL(e.g. follicular lymphoma)
Aggressive NHL(e.g. diffuse large B-cell lymphoma)
Survival patterns for indolent and aggressive NHL in the 20th century
NHL: non-Hodgkin lymphoma
8
Follicular lymphoma and diffuse large B-cell lymphoma are two NHL subtypes of interest
Follicular lymphoma
• Low-grade/indolent
• 20–30% of NHL cases
• 80–85% of patients are diagnosed in a late stage (stage III or IV) due to its slow growth
• Average age of diagnosis is 60 years
• May not always require treatment and for those who are asymptomatic with low disease burden - Watch-and-wait may be used.
NHL: non-Hodgkin lymphoma8
Diffuse large B-cell lymphoma
• High-grade / Aggressive
• Most common NHL; 31% of all cases
• Occurs most frequently in those aged >50 years ( average age 62 years)
• Immediate combination chemotherapy treatment is essential and potentially curable
9
Treating non-Hodgkin lymphoma
9
10
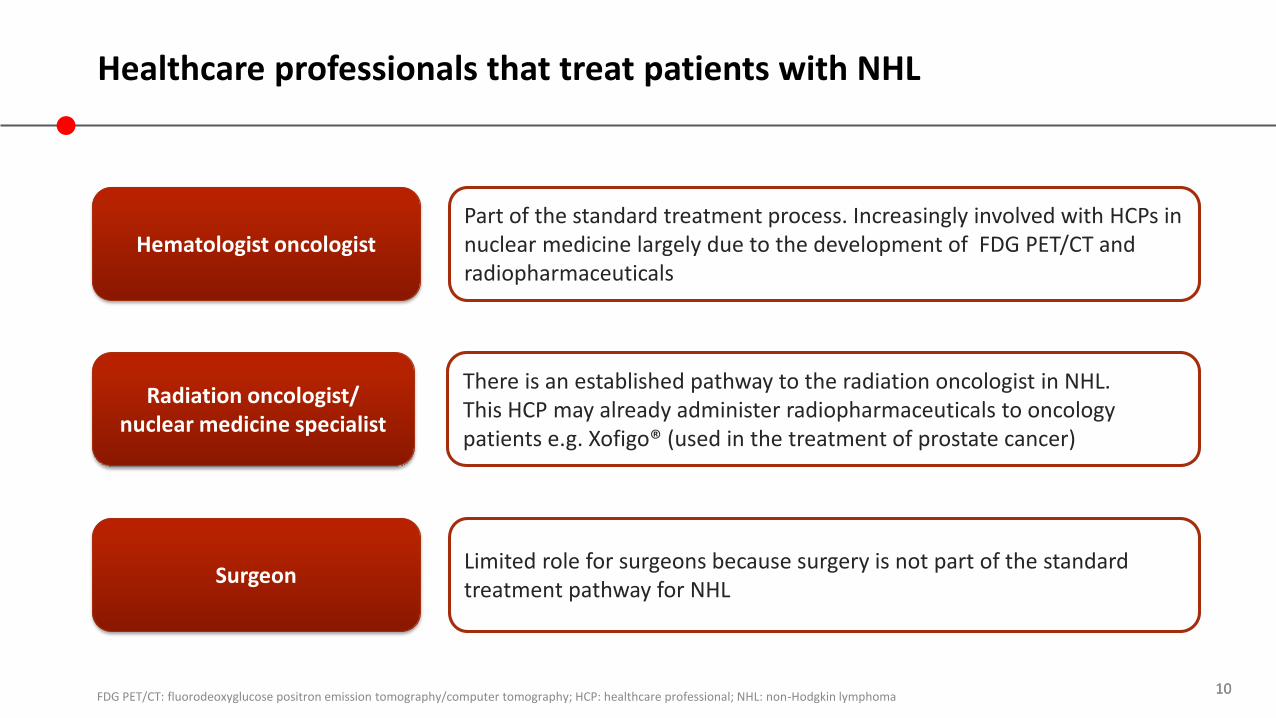
Healthcare professionals that treat patients with NHL
FDG PET/CT: fluorodeoxyglucose positron emission tomography/computer tomography; HCP: healthcare professional; NHL: non-Hodgkin lymphoma10
Radiation oncologist/ nuclear medicine specialist
There is an established pathway to the radiation oncologist in NHL.This HCP may already administer radiopharmaceuticals to oncology patients e.g. Xofigo® (used in the treatment of prostate cancer)
Hematologist oncologistPart of the standard treatment process. Increasingly involved with HCPs in nuclear medicine largely due to the development of FDG PET/CT and radiopharmaceuticals
SurgeonLimited role for surgeons because surgery is not part of the standard treatment pathway for NHL
11
Therapies used for NHL
• Cytotoxic chemotherapy e.g. CHOP (cyclophosphamide, adriamycin, vincristine, prednisolone)
• Cell surface receptor-targeted therapies e.g. antibody therapies
• Includes drugs such as rituximab that target cell-surface proteins such as CD20
• Molecularly targeted therapies e.g. therapies targeting downstream signal transduction pathways—block cancer growth and spread by interfering with specific molecules involved in tumor growth and progression
• Targeted agents act on the tumor-specific genes, proteins or the tissue environment that contribute to growth and survival
• Targeted agents have several advantages over chemotherapy:
• Greater tumor specificity
• Potentially more favorable toxicity profile
NHL: non-Hodgkin lymphomaCancer.net, accessed October2015
11
12
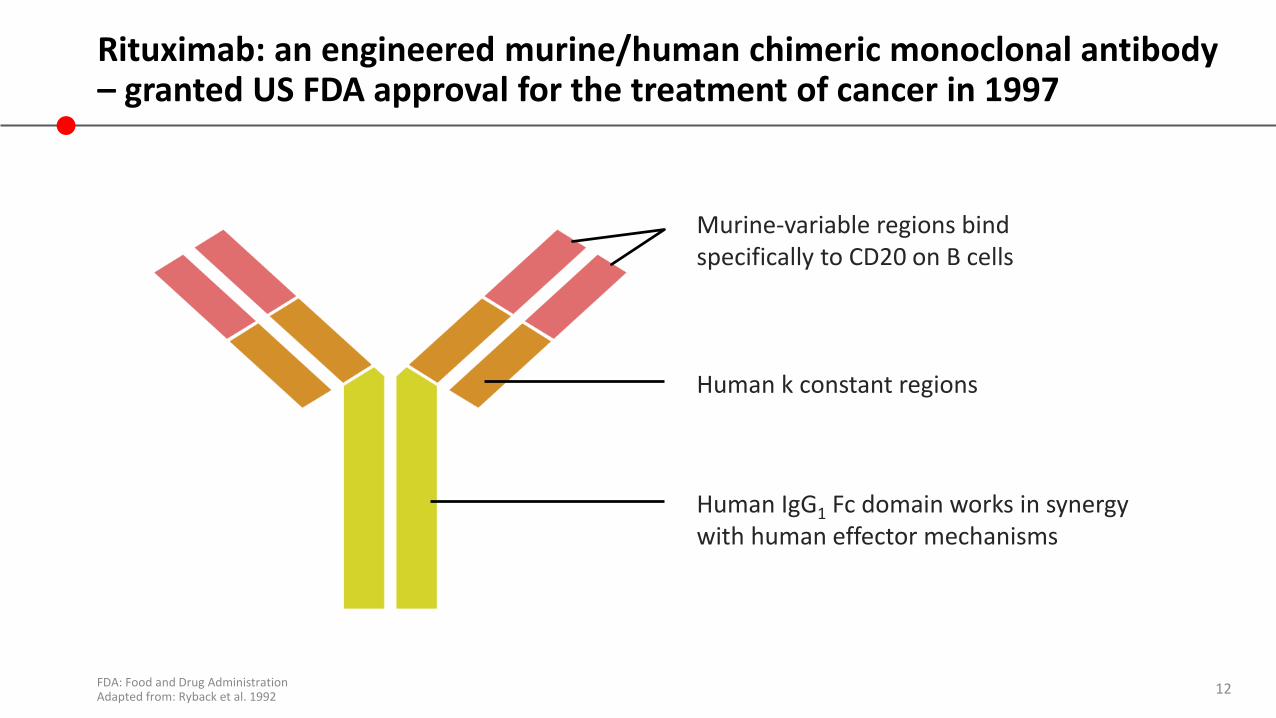
Rituximab: an engineered murine/human chimeric monoclonal antibody – granted US FDA approval for the treatment of cancer in 1997
FDA: Food and Drug AdministrationAdapted from: Ryback et al. 1992
Murine-variable regions bindspecifically to CD20 on B cells
Human k constant regions
Human IgG1 Fc domain works in synergywith human effector mechanisms
13
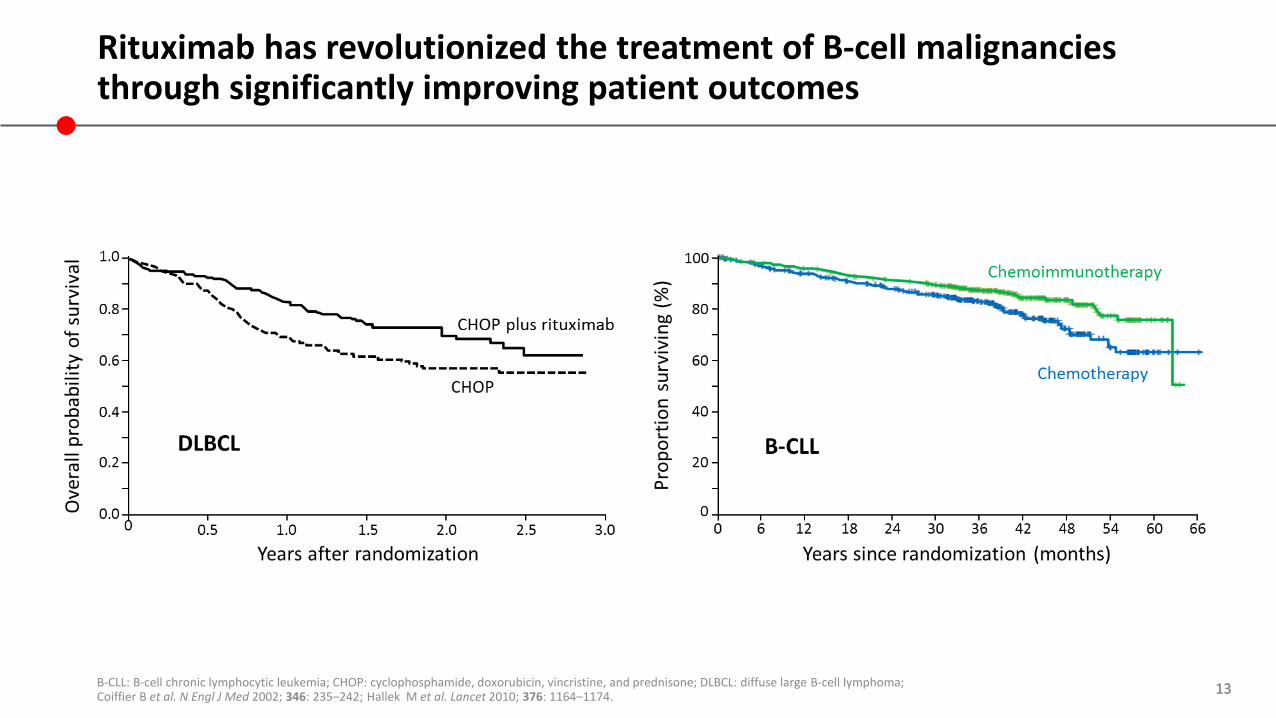
Rituximab has revolutionized the treatment of B-cell malignancies through significantly improving patient outcomes
B-CLL: B-cell chronic lymphocytic leukemia; CHOP: cyclophosphamide, doxorubicin, vincristine, and prednisone; DLBCL: diffuse large B-cell lymphoma; Coiffier B et al. N Engl J Med 2002; 346: 235–242; Hallek M et al. Lancet 2010; 376: 1164–1174.
13
14
Therapies used for NHL
• Cytotoxic chemotherapy e.g. CHOP (cyclophosphamide, adriamycin, vincristine, prednisolone)
• Cell surface receptors e.g. antibody therapies
• Includes drugs such as rituximab that target cell-surface proteins, e.g. CD20
• Molecularly-targeted therapies e.g. therapies targeting downstream signal transduction pathways—block cancer growth and spread by interfering with specific molecules involved in tumor growth and progression
• Targeted agents act on the tumor-specific genes, proteins or the tissue environment that contribute to growth and survival
• Targeted agents have several advantages over chemotherapy:
• Greater tumor specificity
• Potentially more favorable toxicity profile
• Not all tumors express the same targets
NHL: non-Hodgkin lymphomaCancer.net, accessed October2015
14

15
Immunochemotherapy has become the mainstay of NHL treatment
• Immunochemotherapy, combining rituximab and chemotherapy, is used in both indolent and aggressive disease +/- radiotherapy
• Specific treatments vary depending on the patient, disease subtype, and stage of disease
• Several common immunochemotherapy regimens include:
ARA-C: cytarabine; R: rituximab15
R-CHOPcyclophosphamide,
hydroxydaunomycin (doxorubicin), Oncovin® (vincristine), prednisone
R-CVPcyclophosphamiode, vincrostine,
prenisone
R-ICEifosfamide, carboplatin,
etoposide
R-EPOCHetoposide, prednisone, Oncovin®,
cyclophosphamide, halotestin
R-ESHAPetoposide, adiramycin
(doxorubicin), Ara-C, platinum
R-DHAPdexamethasone, cytarabine,
cisplatin
16
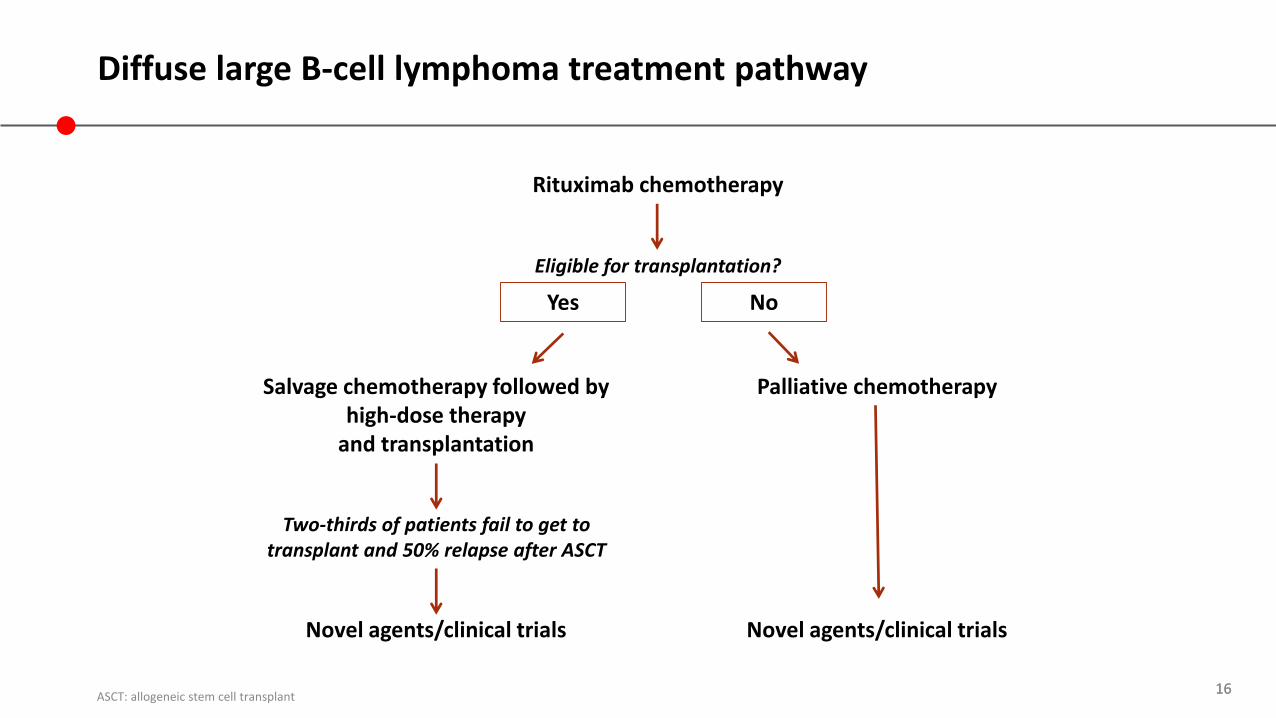
Diffuse large B-cell lymphoma treatment pathway
16ASCT: allogeneic stem cell transplant
Rituximab chemotherapy
Eligible for transplantation?
Salvage chemotherapy followed by high-dose therapy
and transplantation
Palliative chemotherapy
Novel agents/clinical trialsNovel agents/clinical trials
Yes No
Two-thirds of patients fail to get to transplant and 50% relapse after ASCT

17
Follicular lymphoma treatment pathway proposed at ASH 2004
*Symptoms, cytopenias, rapid growth of disease, potential organ compromise (e.g. hydronephrosis); **Consider collection of peripheral blood progenitor cells for future transplantation. ASH; American Society of HematologyWinter JN et al. Hematology Am Soc Hematol Educ Program 2004: 203–220.
17
Stage I–II disease
Involved field radiotherapy
Stage III–IV diseaseIndications to treat*
Watch and wait
Rituximab chemotherapy
Rituximab maintenanceIndications to treat
Radioimmunotherapy
Transplantation (age/fitness limitation!)
**
Yes No
18
The unmet clinical need: Patients who ‘fail’ rituximab-chemotherapy treatment or are unfit for multi-agent treatment
• Rituximab has been successful in improving patient outcomes
• Rituximab-chemotherapy regimens have become the standard of care in first- and second-line
• Although there is a substantial number of patients with DLBCL can be cured by these treatments, many are refractory or relapse
• In follicular lymphoma, many patients eventually relapse and become refractory to rituximab
• Novel agents are required and targeting the cell surface receptors with improved antibodies and antibody conjugates allows the majority of lymphomas to be targeted
DLBCL, diffuse large B-cell lymphoma18
19
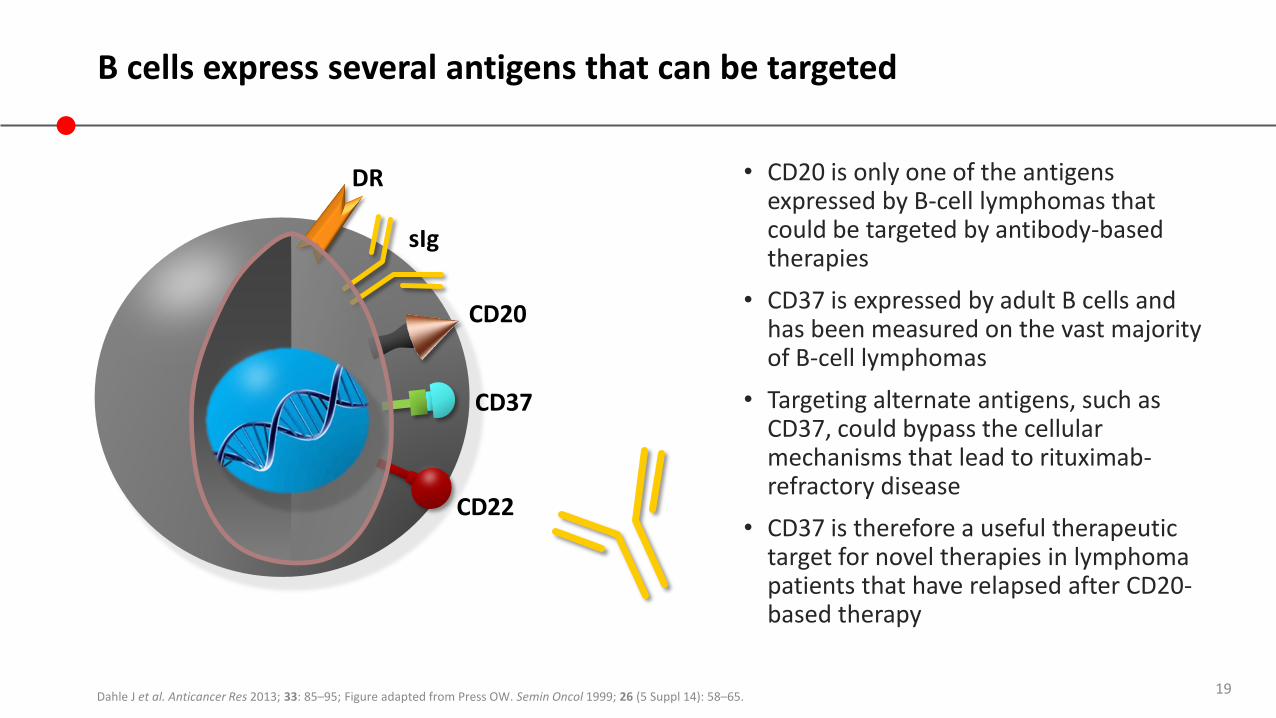
B cells express several antigens that can be targeted
• CD20 is only one of the antigens expressed by B-cell lymphomas that could be targeted by antibody-based therapies
• CD37 is expressed by adult B cells and has been measured on the vast majority of B-cell lymphomas
• Targeting alternate antigens, such as CD37, could bypass the cellular mechanisms that lead to rituximab-refractory disease
• CD37 is therefore a useful therapeutic target for novel therapies in lymphoma patients that have relapsed after CD20-based therapy
Dahle J et al. Anticancer Res 2013; 33: 85–95; Figure adapted from Press OW. Semin Oncol 1999; 26 (5 Suppl 14): 58–65.
DR
sIg
CD20
CD37
CD22
20
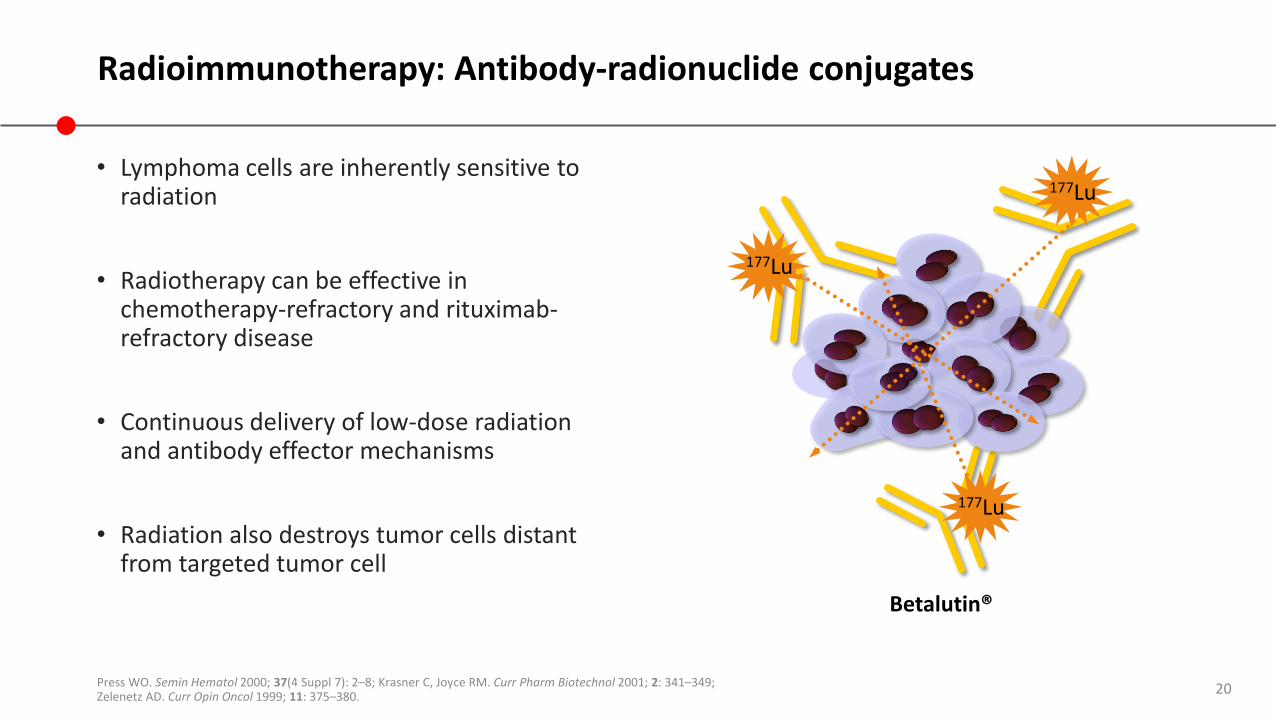
Radioimmunotherapy: Antibody-radionuclide conjugates
• Lymphoma cells are inherently sensitive to radiation
• Radiotherapy can be effective in chemotherapy-refractory and rituximab-refractory disease
• Continuous delivery of low-dose radiation and antibody effector mechanisms
• Radiation also destroys tumor cells distant from targeted tumor cell
Press WO. Semin Hematol 2000; 37(4 Suppl 7): 2–8; Krasner C, Joyce RM. Curr Pharm Biotechnol 2001; 2: 341–349; Zelenetz AD. Curr Opin Oncol 1999; 11: 375–380.
Betalutin®
177Lu
177Lu
177Lu
21
Defining features of single treatment antibody-radionuclide conjugate in relapsed follicular lymphoma
• High response rates (ORR and CR)
• Durable long-term responses
• Simple and effective treatment; high quality-of-life for both older and younger patients
• Limited uptake and availability
CR: complete response; ORR: overall response rate
22
The unmet need innon-Hodgkin lymphoma
22
23
Where is the unmet need in NHL?
NHL: non-Hodgkin lymphoma23
Relapsed NHL No standard therapy past second-line
Rituximab resistance Patients who have developed resistance to the CD20-targeted antibody
Older patientsPatients aged >65 years might not be able to tolerate some chemotherapies
Comorbidities Some comorbidities can impact tolerability of treatment
Lack of response Patients with a poor response to first- or second-line treatment
24
What features should we look for in a novel therapy to help us meet these unmet needs?
• Antibody-radionuclide conjugate therapy (radioimmunotherapy) that has a strong efficacy and safety profile in relapsed and refractory patient populations, including:
• Patients who have failed previous therapies
• Patients who are have relapsed or are refractory to rituximab
• Patients who are considered ‘frail’ that might not be eligible for current therapies, e.g. older patients, those with comorbidities
• A treatment that does not have strict compliance requirements
24
25
Summary
• NHL has several subtypes; the most common are follicular lymphoma and diffuse large B-cell lymphoma
• Chemotherapy, rituximab, radiotherapy and targeted treatments are commonly used to treat NHL
• There is no standard treatment beyond second line, and there is an unmet need for new therapeutic options for patients who have failed previous therapies
• A novel antibody-radionuclide conjugate treatment could be a future option for second- or third-line therapy in patients with follicular lymphoma or diffuse large B-cell lymphoma, who are unable to tolerate transplantation or chemotherapy
NHL: non-Hodgkin lymphoma25







