
Upper Cross Syndrome: Assessment & Management in Family PracticeHKDU Symposium Dec 2014
Dr. Ngai Ho Yin AllenFamily Medicine SpecialistPGDipMusculoskeletal Medicine MBBS(HK), DCH(London), DFM(CUHK), DipClinDerm(London), FRACGP, FHKCFP, FHKAM(Family Medicine)

Muscle imbalances can spread through the muscular system in a predictable manner
Janda (1987, 1988) has classified these patterns as:1. Upper crossed syndrome
2. Lower Crossed syndrome &
3. Layer syndrome
The crossed syndromes are characterized by alternating sides of inhibition and facilitation in the upper quarter and lower quarter
Janda’s Crossed Syndromes

The Upper Crossed Syndrome
Facilitation of: Suboccipital muscles
Upper trapezius,
Levator scapulae,
Sternocleidomastoid, and
Pectoralis muscles
Inhibition of: Deep cervical flexors
Lower trapezius,
Serratus anterior, and
Rhomboid muscles

The Upper Crossed Syndrome
Weak deep cervical flexors
Weak lower trapezius,
rhomboids, serratusanterior
Tight suboccipitals, upper trapezius, levator scapulae
Tight sternocleidomastoid, pectoralis muscles

Muscles Inhibited in UCS
Deep neck flexorsLower trapezius
Serratus
anterior
Rhomboid muscles

Forward head posture increases stress on upper cervical segments
Cervicogenic headache occured more often in people with anterior head positioning (J Manipulative Physiol Ther. 2004)
According to Travell & Simons trigger point theories, anterior head positioning has significant contributions to the perpetuation of myofascial TrPs in the head, neck and shoulder muscles, as well as TMJ disorders
Anterior Head Positioning

Suboccipital, posterior cervical, upper trapezius and splenius capitis muscles contract and shorten to bring the head into extension to allow the eyes to gaze forward
Consequences of UCS (1)
Loss of cervical
lordosis & flattening
of cervical curve
TrPs development
causing headache and
neck pain
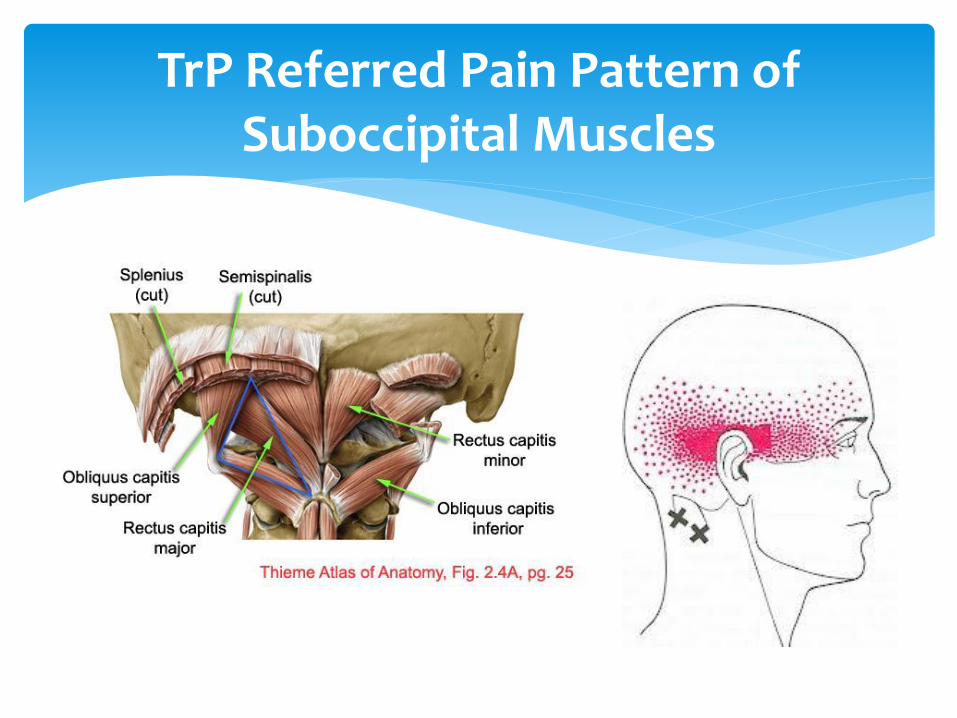
TrP Referred Pain Pattern of Suboccipital Muscles

TrP Referred Pain Pattern of Posterior Cervical Muscles
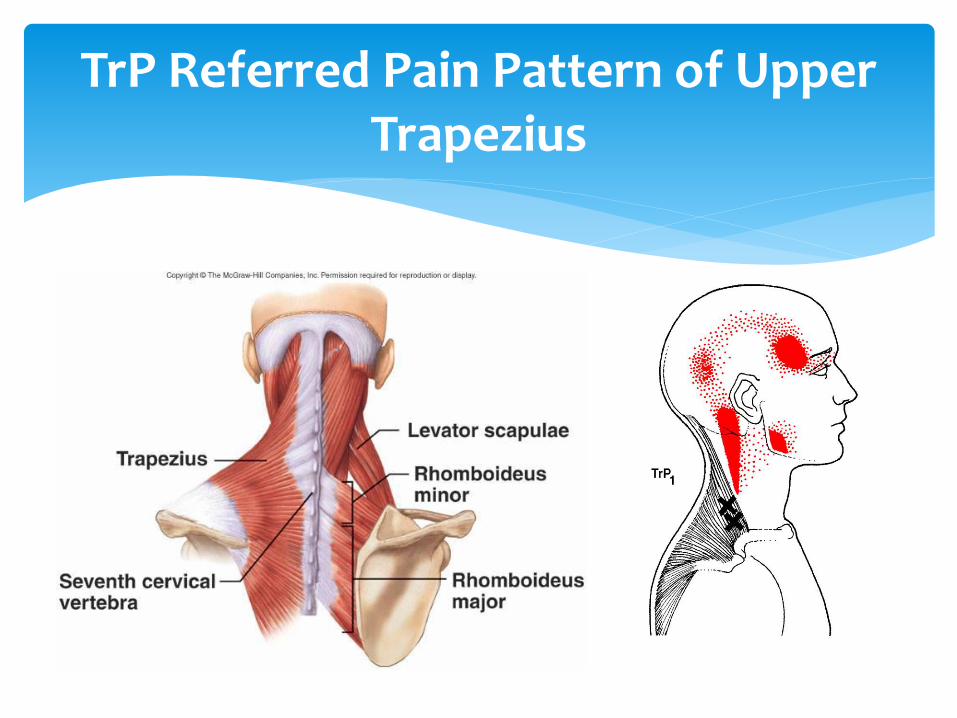
TrP Referred Pain Pattern of Upper Trapezius

TrP Referred Pain Pattern of Splenius Capitis

Sternocleidomastoid and splenius cervicis placed in a mechanical disadvantaged position as a result of reduced cervical lordosis
Consequences of UCS (2)
Muscle overloading & TrP
development causing headache and
neck pain

TrP Referred Pain Pattern of Sternocleidomastoid
Sternal division Clavicular division

TrP Referred Pain Pattern of Splenius Cervicis

Suprahyoid and infrahyoid muscles placed in stretched position
Consequences of UCS (3)
Counteracting force of
mandibular elevating
muscles
Increased intra-articular
pressure of TMJ
Muscle TrP
development
causing ear pain,
facial pain and
jaw pain
TMJ Dysfunction

TrP Referred Pain Pattern of Digastric Muscle
Posterior belly TrP Anterior belly TrP
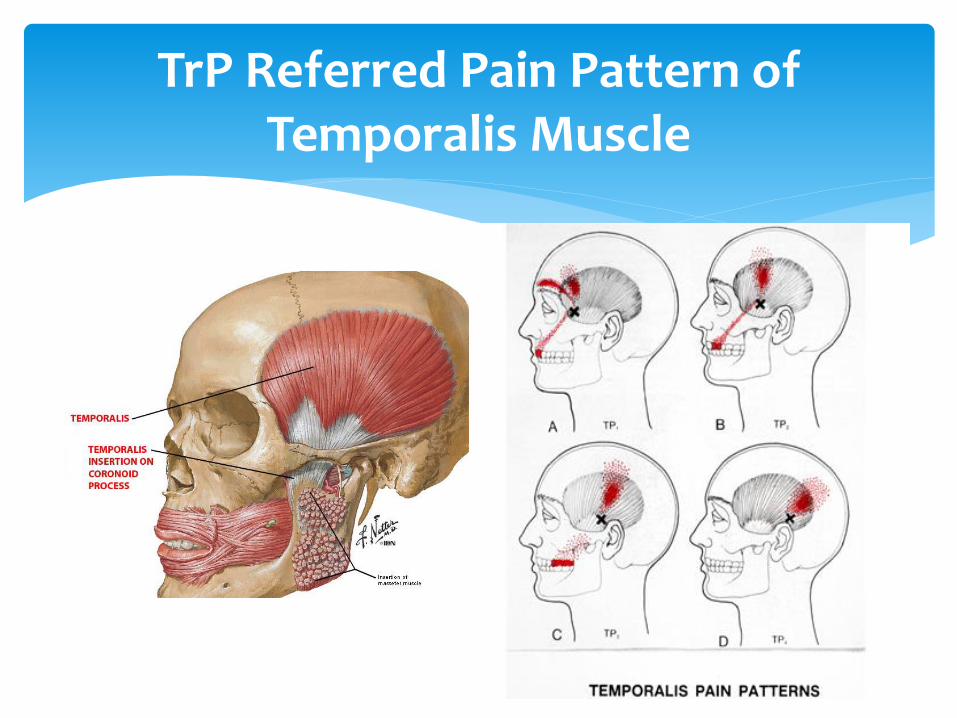
TrP Referred Pain Pattern of Temporalis Muscle
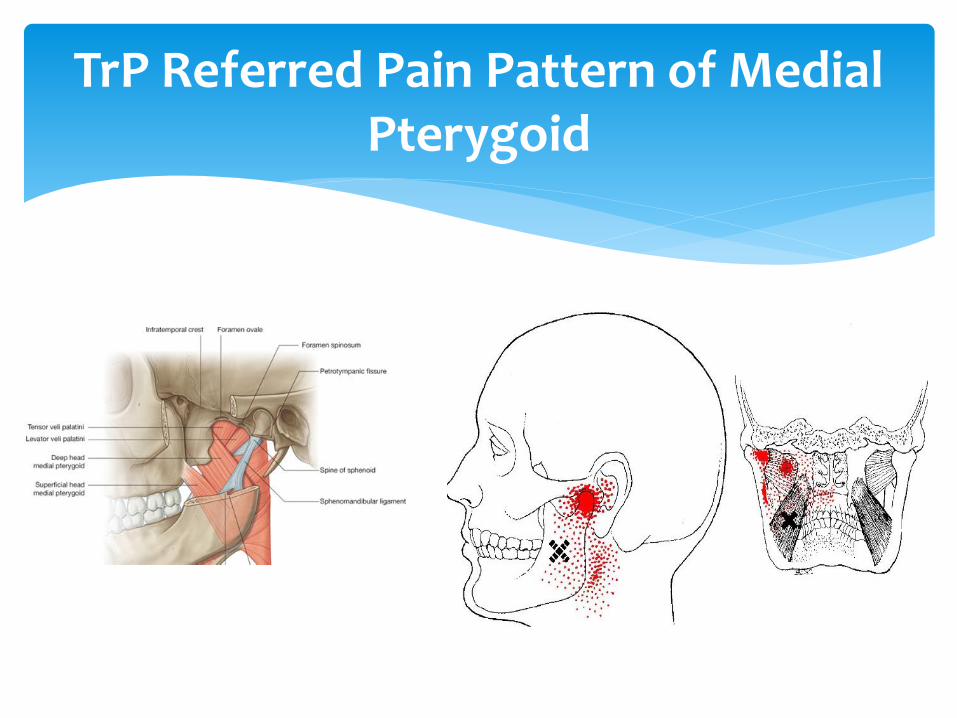
TrP Referred Pain Pattern of Medial Pterygoid

TrP Referred Pain Pattern of Lateral Pterygoid
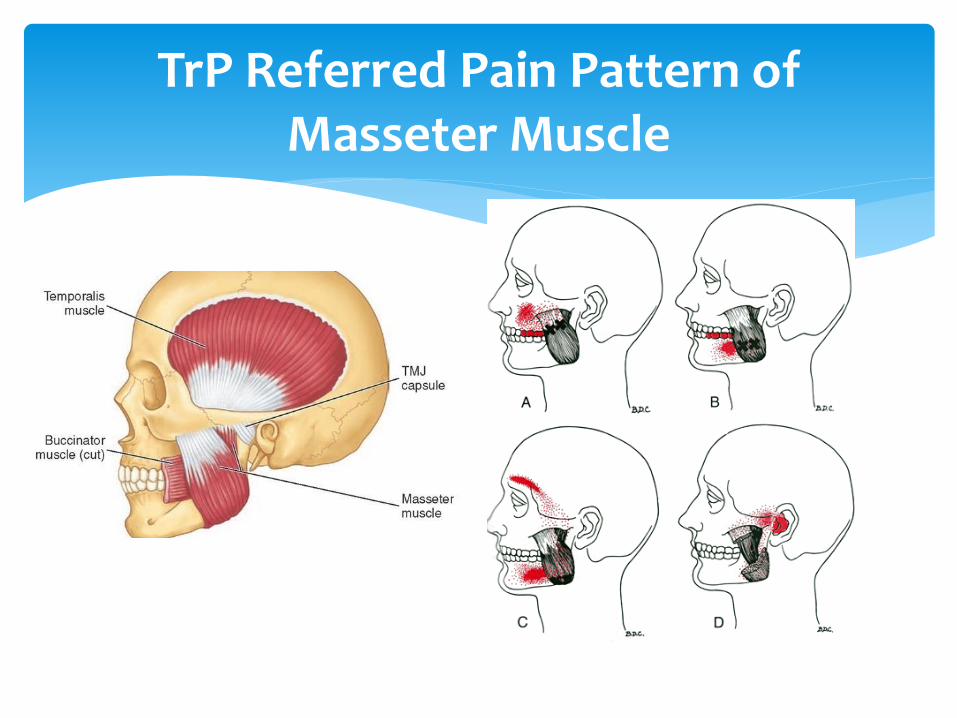
TrP Referred Pain Pattern of Masseter Muscle

Increased cervical extension compression of C0/1, zygapophyseal joints and nerve roots
Consequences of UCS (4)
Compression of C0/1, zygapophyseal joints
and nerve roots
Degenerative changes of zygapophyseal
joints and cervical nerve root impingement


Tightness of pectoralis and upper trapezius creates an anterior force on glenohumeral joint and limits scapular upward rotation, external rotation and posterior tilt
Consequences of UCS (5)
Reduction in subacromial space
Subacromial impingement syndrome,
rotator cuff tendinosis and tear

Assessment of Upper Crossed Syndrome

Patient is observed from:
1) In front
2) Behind
3) From the side
Concentrate on head position and any asymmetry
Inspection

Inspection From Front
Observe:
1) Eye levels
2) Chin position
3) Shoulder elevation

Inspection From Side
Observe:
1) Ear lobe position
2) Exaggerated or reduced lordosis
Ideal position from side: straight line passing through earlobe and AC joint of shoulder

Clinically, assessment of anterior head position is probably the single most useful postural parameter in a patient with head and neck pain complaints
A simple test: 1. Looking at the patient from the side and
place a real or imaginary plumb line on a tangent to the crest of the thoracic spine kyphotic curve
2. Then measure the distance from this line to the depth of the cervical curve
3. This distance should be ~6cm
Measurements > 6cm indicate anterior head positioning
Anterior Head Positioning

Inspection From Behind
Observe:
1) Head position
2) Shoulder elevation
3) Scoliosis of thoracic spine

Other examination directed by patient’s symptoms. These may include:
1. Cervical spine palpation and range of motion examination
2. Neurological examination of upper limb
3. Shoulder palpation and range of motion examination
4.Shoulder impingement tests
5. Temporomandibular joint examination
6.Head and neck, shoulder trigger point palpation
Other Examinations

Management

Depends on clinical expertise. These may include:
1. Office and daily activities ergonomic assessment
2. Medications: simple analgesics and second-line analgesics as temporary pain control
3. Trigger point injections or dry-needling
4. Manual therapies
5. Home exercise prescription and postural correction (most important for long-term management)
Management in Family Practice

Different approaches:
Local anesthetic without corticosteroid and adrenaline, e.g.
0.5% procaine (less myotoxic), 1% lidocaine
Dry needling (more post-injection soreness)
One MUST know the anatomical danger zones before injection.
E.g. rhomboid injection can cause pneumothorax
Trigger Point Injection
Sternomastoid trigger point injection

Manual Therapy
Randomized controlled studies showed that spinal manipulative therapy (SMT) is effective for cervicogenic headaches, particularly those focused on treatment of the upper cervical segments (Spine 2002)
Systematic reviews of randomized control trials using manual therapy in cervicogenic headache patients suggest better outcomes compared to no treatment (Man Ther. 2010 )
Direct and indirect techniques. Generally post-isometric relaxation is much safer than high-velocity low amplitude (HVLA) techniques

Muscle energy technique for releasing
the left levator scapuae
HVLA thrust technique for treating a
C5 FRS Left dysfunction

Sternocleidomastoid and Upper Trapezius stretching exercises
Exercise Prescription (1)

Pectoralis stretching exercises
Home Exercise Prescription (2)

Levator scapulae stretching exercises
Home Exercise Prescription (3)

Deep neck flexor strengthening exercises
Home Exercise Prescription (4)
Eccentric deep neck
flexor exercises

Lower trapezius strengthening exercises
Home Exercise Prescription (5)

Rhomboid strengthening exercises
Home Exercise Prescription (6)

Serratus anterior strengthening exercises
Home Exercise Prescription (7)

Simple Shoulder Postural Exercise
Stand with feet ~4 inches apart, arms at the sides and thumbs pointing outward
Tighten the buttocks to stabilize the lower back Rotate the thumbs, arms and shoulders out and back while inhaling,
squeezing the shoulder blades together in back Maintain this position while pulling the shoulders down and exhaling Hold this position while breathing normally and correct the head
posture (see following slide)

Simple Head Postural Exercise
Perform the shoulder postural exercise first
Once the shoulder posture has been corrected, gently move the head backward to bring the ears in line with the shoulders
This must be accomplished without moving the nose up or down and without opening the mouth

Postural Avoidance (1)
Positioning of the pillow to produce relief of the sternocleidomastoid:
1. Patient supine with the corners of the pillow tucked between the chin and shoulders. NOT to place pillow under the shoulders
2. Patient side-lying with the pillow between the head and shoulder. NOT to place pillow under the shoulder so that the chin lies in the hollow of the shoulder placing the SCM and scalenes in shortened positions

Postural Avoidance (2)
Support for short upper arms: when the patient’s upper arms are short in relation to torso height, they do not reach the armrests of most chairs. This imposes sustained gravity stress on the trapezius
Select chairs with armrests of the correct height to provide elbow support
Hands-in-pockets posture can also help to relieve strain on upper trapezius

Postural Avoidance (3)
Avoid working at a desk with the head turned to one side and projected forward to see documents or a display screen
Avoid the so-called “bird-watching” posture for prolonged period
The above postures place the splenius cervicis in sustained contraction

THE END







