
PROGRESS IN ENDOSCOPIC TREATMENT OF UROLITHIASISTREATMENT OF UROLITHIASIS
Olivier TraxerTenon Tenon HospitalHospital, Paris, France, Paris, France
Université Pierre & Marie CURIE (PARIS VI)Université Pierre & Marie CURIE (PARIS VI) [email protected]

FLEXIBLE URS
• Since 2001 recent development of newSince 2001, recent development of new flexible URS and the miniaturisation of i t t ll t d th di tinstruments allow today the direct diagnosis and treatment of upper urinary tract diseases
– Smallest caliber actively deflectable (7.5F)– Working channel is 3.6FWorking channel is 3.6F– 2-way active deflect°. : 270-270 degrees – Improved fiberoptics and digital technologyImproved fiberoptics and digital technology
Basillote JB et al. Urol Clin North Am. 31, 2004
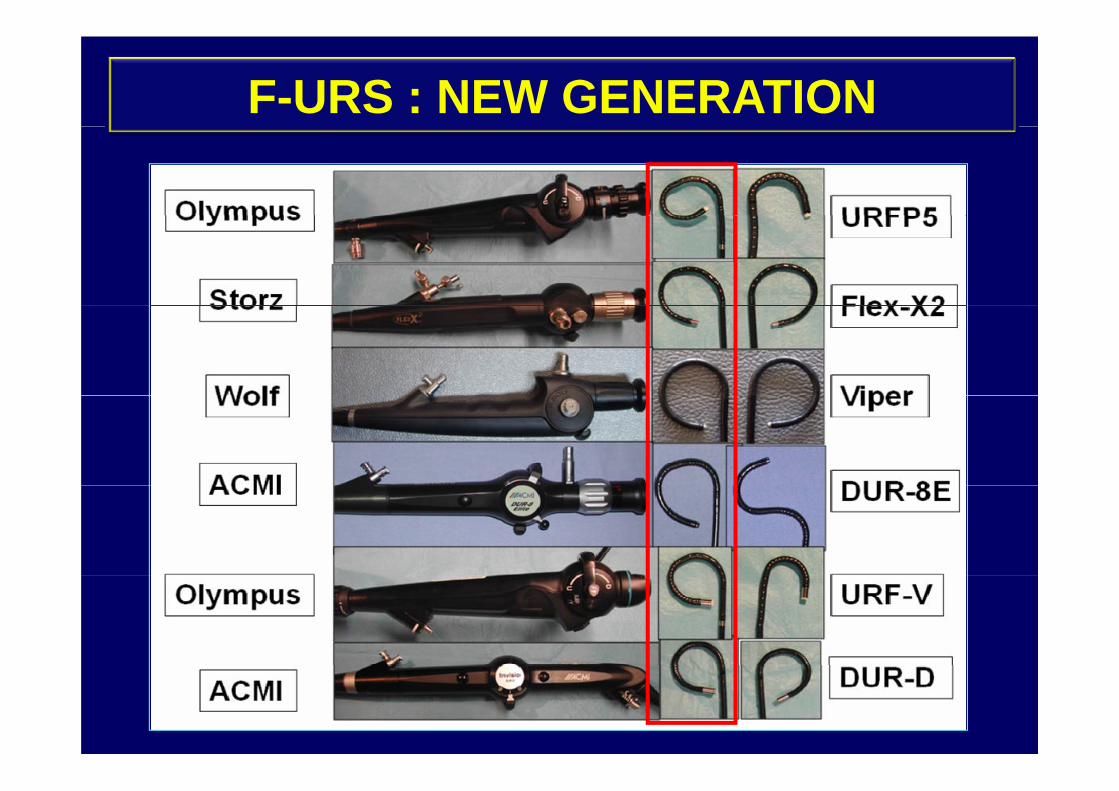
F-URS : NEW GENERATION

FLEXIBLE URS
Flex-X2 DUR-D
URF P5 URF VURF-P5 URF-V• Access to the entire
collecting system :collecting system : 95-100%
Busby & Low, 2004Beiko & Denstedt, 2007

Improvements in Ureteroscope Designp p g
FiberOptic Digital System

ELECTROMAGNETIC SPECTRUM NANOMETER
RAYON X MICRONDE-390
-514
32 7-63
0
5594 064
40 600
80 100
ONDE RADIO
190
-
488 53
577 7569 10 29 1069 21
UV VISIBLEINFRA-RED
400 700

HOLMIUM YAG LASER
• I t d ti f H l i YAG
CALCULASE 10W: Karl Storz
• Introduction of Holmium:YAGlaser wich can fragment any type of stone ablate and cut tissueof stone, ablate and cut tissue has expanded the role of FURS
Grasso et al, J Clin Laser Med Surg 1998

SPECIAL CIRCUMSTANCES
DJ INCRUSTATION
SPECIAL CIRCUMSTANCES
DJ INCRUSTATION

MATERIALS• WIRES
MATERIALS
• DLC & URETERAL ACCESS SHEATH • NITINOL BASKET• PORT SEAL / MANUAL HAND DEVICE• LASER FIBERS
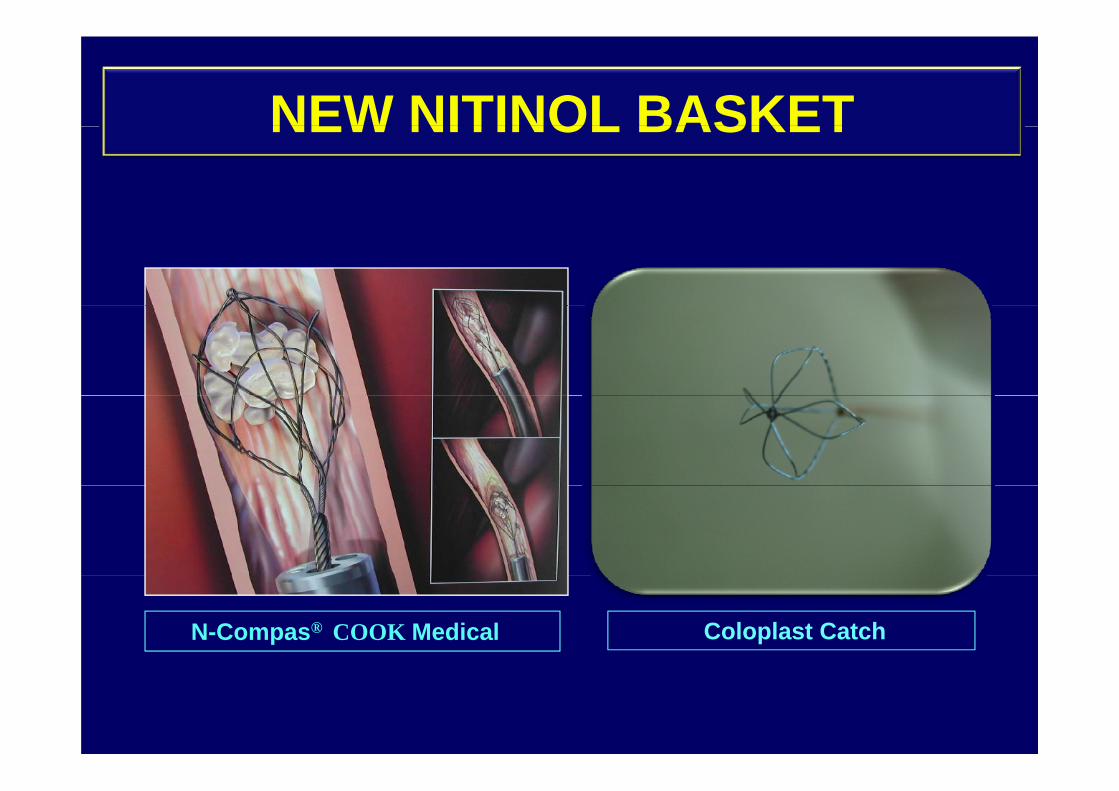
NEW NITINOL BASKETNEW NITINOL BASKET
N-Compas® COOK Medical Coloplast Catch

NITINOL RETRIEVING DEVICES

NEW NITINOL BASKETNEW NITINOL BASKET
N-Trap®N-Trap®
To prevent stone migration during Rigid URS

URETERAL ACCESS SHEATHURETERAL ACCESS SHEATH
• Facilitate multiple entries/exitsFacilitate multiple entries/exits
• Avoid effects of ureteral edemaAvoid effects of ureteral edema
• Maintain low intrarenal press.p
• Limit operating time
• Facilitate irrigation
• Protect Flexible URS
Kourambas, J Urol 2001

ADEQUATE FLOW OF IRRIGANTADEQUATE FLOW OF IRRIGANT
SPECIFIC PORT SEAL & IRRIGATION DEVICESTo Preserve & Increase irrigation
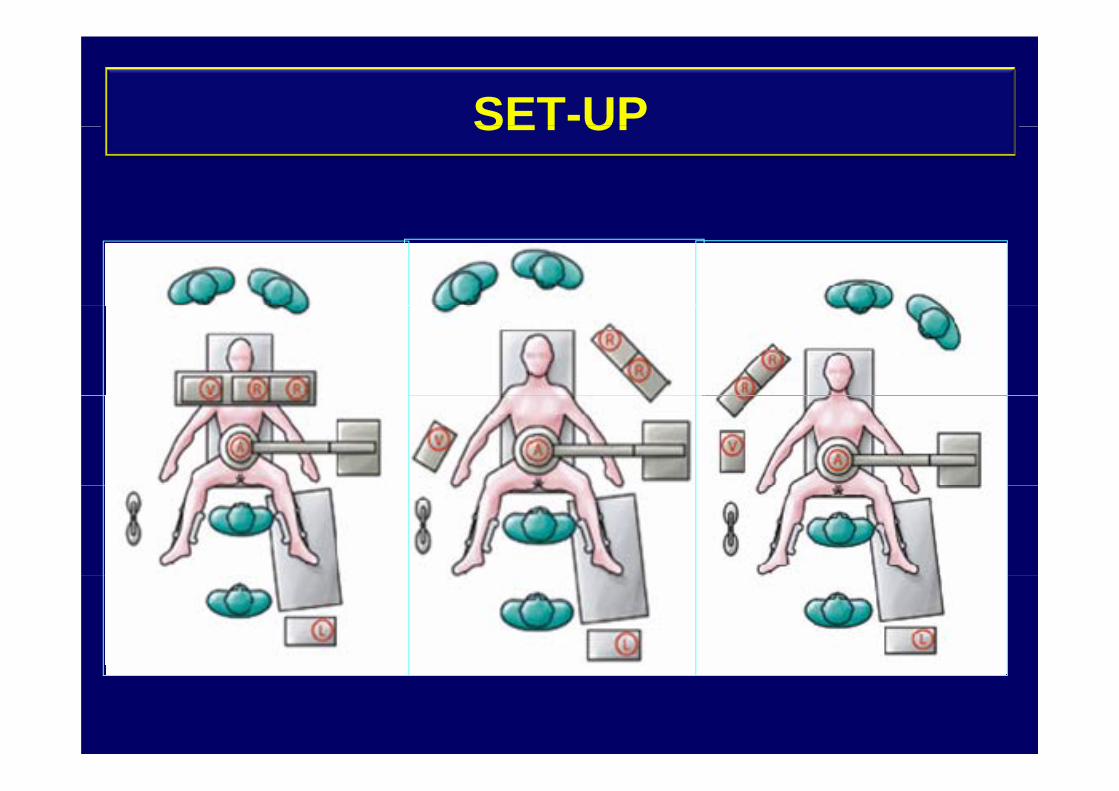
SET-UPSET UP

SET-UPSET UP

LASER AND FIBERSLASER AND FIBERS

PATIENT POSITIONPATIENT POSITION

INSPECT EACH CALYXWITH C-ARM CONTROL

INDICATIONS• THERAPEUTIC (90%)• DIAGNOSTIC (10%)
- STONES (75%)- Kidney-Ureter
Lower Calyx
DIAGNOSTIC (10%)- Obstructions
D f t IVP - Lower Calyx- Cystine- Anatomic abnormal.
- Defect on IVP- Unexplained
- Obesity- Coagulopathy
Hematuria- Positive Cytology
- Associat° FURS-Perc- Strictures (5%)
Ureter UPJO
y gy- Reccurent uroth. tumor - Ureter - UPJO
- Urothelial Tumors (10%)- Foreign body : stent, …
tumor
g y ,
Beiko, Urol Clin N Am 2007

EAU GUIDELINES 2009
URETERAL STONESURETERAL STONES
EAU Guidelines 2009

EAU GUIDELINES 2009
RENAL STONES <= 2 cmsRENAL STONES <= 2 cms
EAU Guidelines 2009
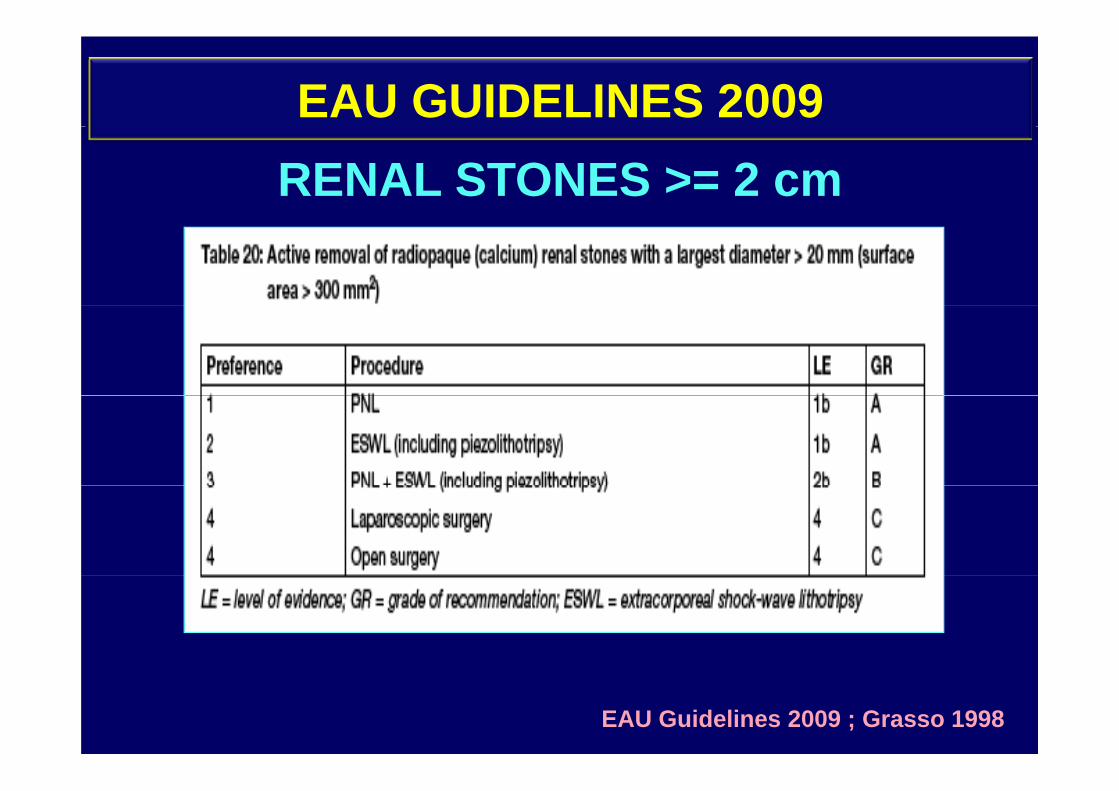
EAU GUIDELINES 2009RENAL STONES >= 2 cm
EAU Guidelines 2009 ; Grasso 1998

F-URS F-URS success rate was defined as stone free (SF)
or remaining fragments (RF) less than 3 mmor remaining fragments (RF) less than 3 mm
Post operative evaluation:– Second look : 1-3 weeks
KUB t D 1 d RUS t D 30– KUB at Day 1 and RUS at Day 30– KUB Day 1 and NCCT at Day 30

RESULTS (>2 CM)RESULTS ( 2 CM)
First session
SF Rate : 55,6%TRAXER et al, WCE 2009
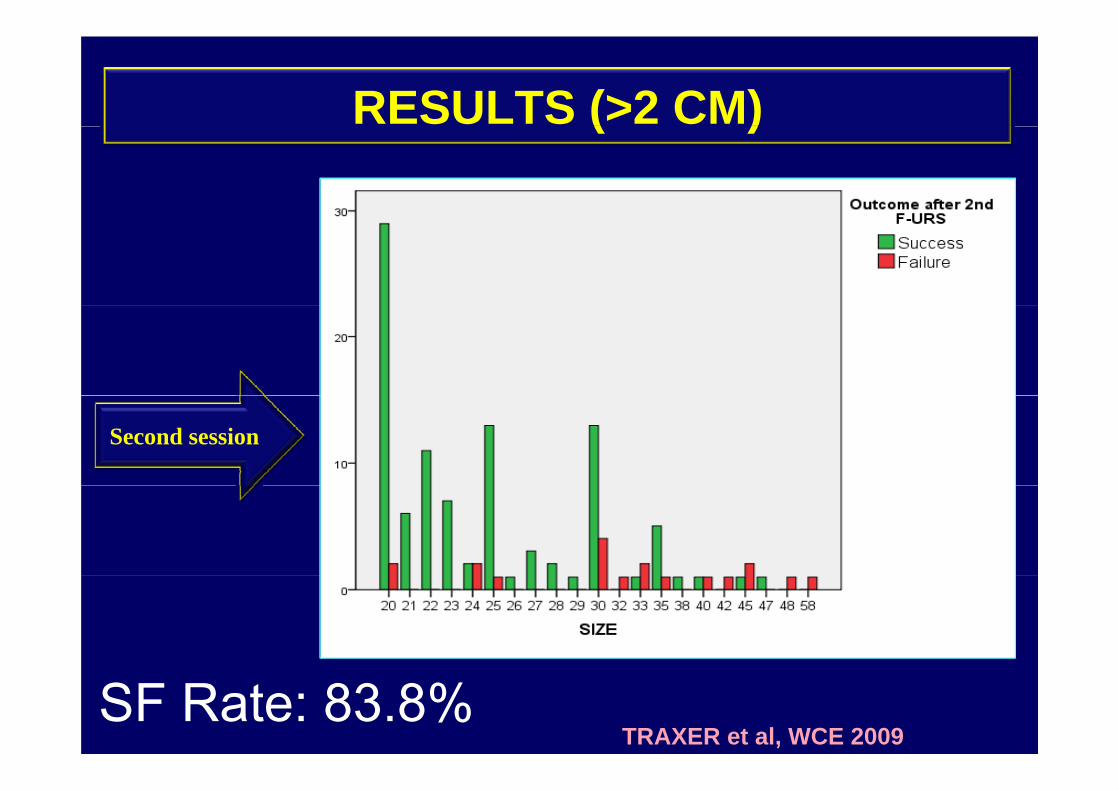
RESULTS (>2 CM)( )
Second session
SF Rate: 83.8%TRAXER et al, WCE 2009
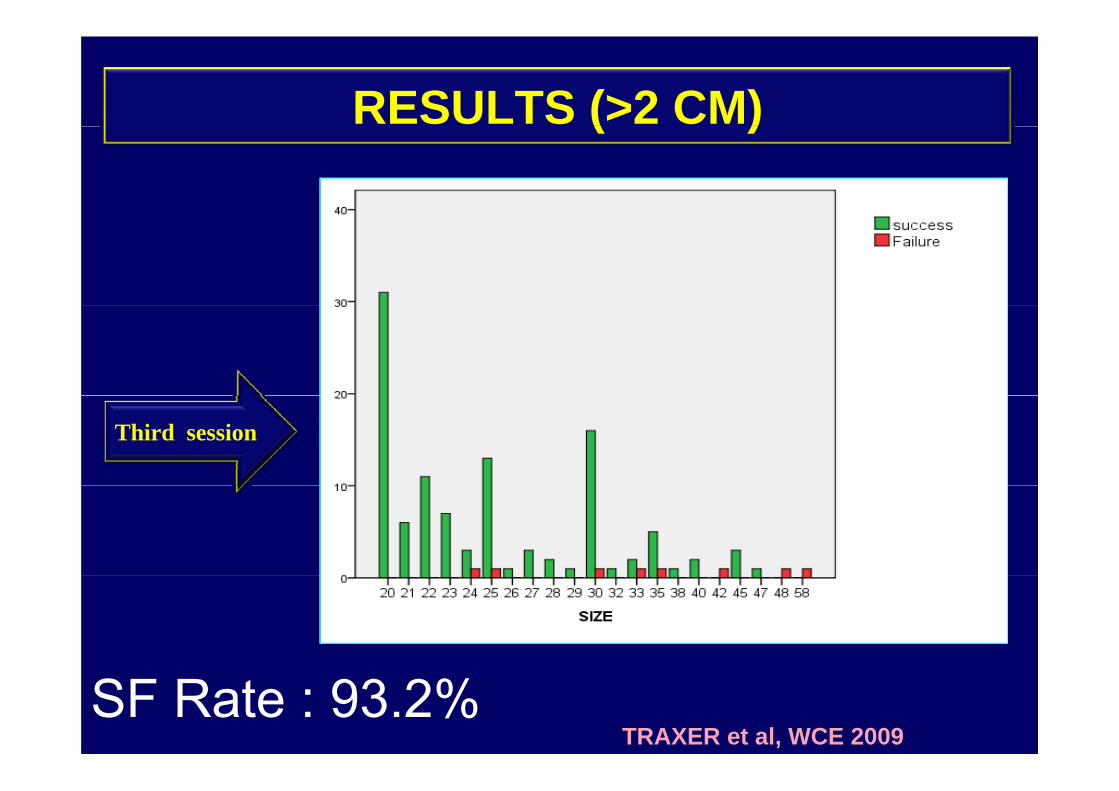
RESULTS (>2 CM)( )
Third session
SF Rate : 93.2%TRAXER et al, WCE 2009

RESULTS ( >2 CM)
1st F‐URS 2nd F‐URS 3rd F‐URS 4th F‐URS
( )
89.80%97.90%
63% 73.60%78.90%
52.60%
10.50%0.00%
2 ‐ 3 cm> 3 cm> 3 cm

LARGE RENAL PELVIC STONE

COMPLETE LASER FRAGMENTATION IN ONE SESSIONSESSION

Large Renal stone (multiple) fragmentation with one isession

TREATMENT OF SOLITARY KIDNEY STONE TOTAL VOLUME : 25 mm (1 session)
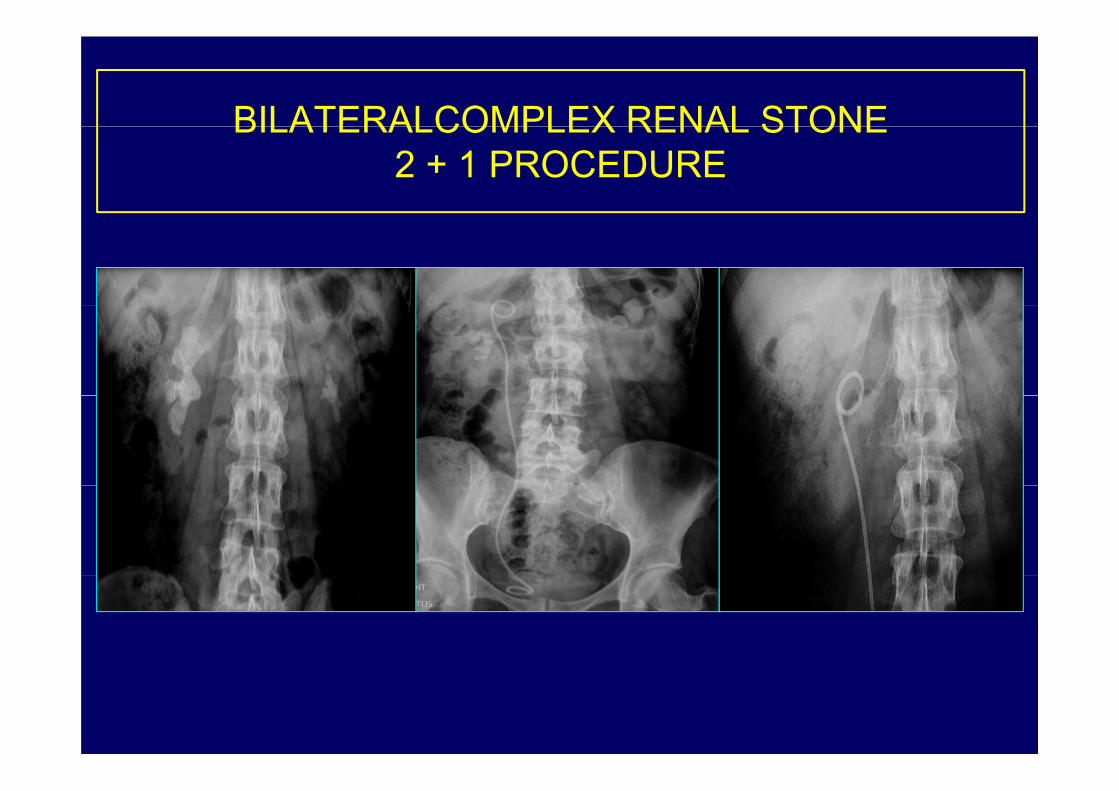
BILATERALCOMPLEX RENAL STONEBILATERALCOMPLEX RENAL STONE2 + 1 PROCEDURE

RESULTS

LOWER POLE STONELOWER POLE STONE REPOSITIONING
Tipless Nitinol BasketTipless Nitinol Basket
S h t 2002 K b 2000LP Stone < 15 mm
Schuster, 2002, Kourambas 2000EAU Guidelines 2009

LOWER POLE STONE REPOSITIONING• Kourambas et al (Urol 56, 2000):
St di l d / iti l b k t– Stone displaced w/ nitinol basket or grasper– 90% SF for displaced – 83% for in situ stones
S h t t l (J U l 168 2002)
I Sit Di l d
• Schuster et al (J Urol 168, 2002):
In SituN=59
DisplacedN=19
P-value
O ll 71% 94% 0 058Overall 71% 94% 0.0581 cm 77% 77% ns>1 cm 29% 100% 0.005

LP STONE REPOSITIONING
α
n Wattsn-x Watts
Fiber laser in deflected URS : important loss of energy through out the way
n Watts
Fiber laser in deflected URS : important loss of energy through out the way

LOWER POLE STONE STUDY IIO O S O S U
Group 1 (1 cm)(n=67)( 6 )
SWL URSSWL(n=32)
URS(n=35)
Stone Free: 1ºoutcome parameter 35 vs 52% (ns)
Pearle MS et al. J Urol, 2005

Stone-Bearing caliceal diverticulumg

TECHNIQUE (BLUE)

Stone-Bearing caliceal diverticulumStone Bearing caliceal diverticulum

Stone-Bearing caliceal diverticulum
We successfully treated caliceal diverticulunm stone in lower pole while others calim difficulties of obtaining success ratepole while others calim difficulties of obtaining success rate
Glenn M Preminger J endourol 2002; 16:557-563Glenn M. Preminger. J endourol. 2002; 16:557-563Batter S, Dretler S: J Urol 1997; 158

Stone-Bearing caliceal diverticulum

SPECIAL CIRCUMSTANCES
HORSESHOE AND PELVIC KIDNEYHORSESHOE AND PELVIC KIDNEY
• Preminger G. J Endourol 2005Preminger G. J Endourol 20058 patients : SFR 85% (1 session)

SPECIAL CIRCUMSTANCES
COMBINED BODY DEFORMITIESCOMBINED TREATMENT
BODY DEFORMITIES
Wi ll U l Cli N A 2008Wignall, Urol Clin N Am. 2008
Scarpa & Scofone, Eur Urol 2008
SPECIAL CIRCUMSTANCES
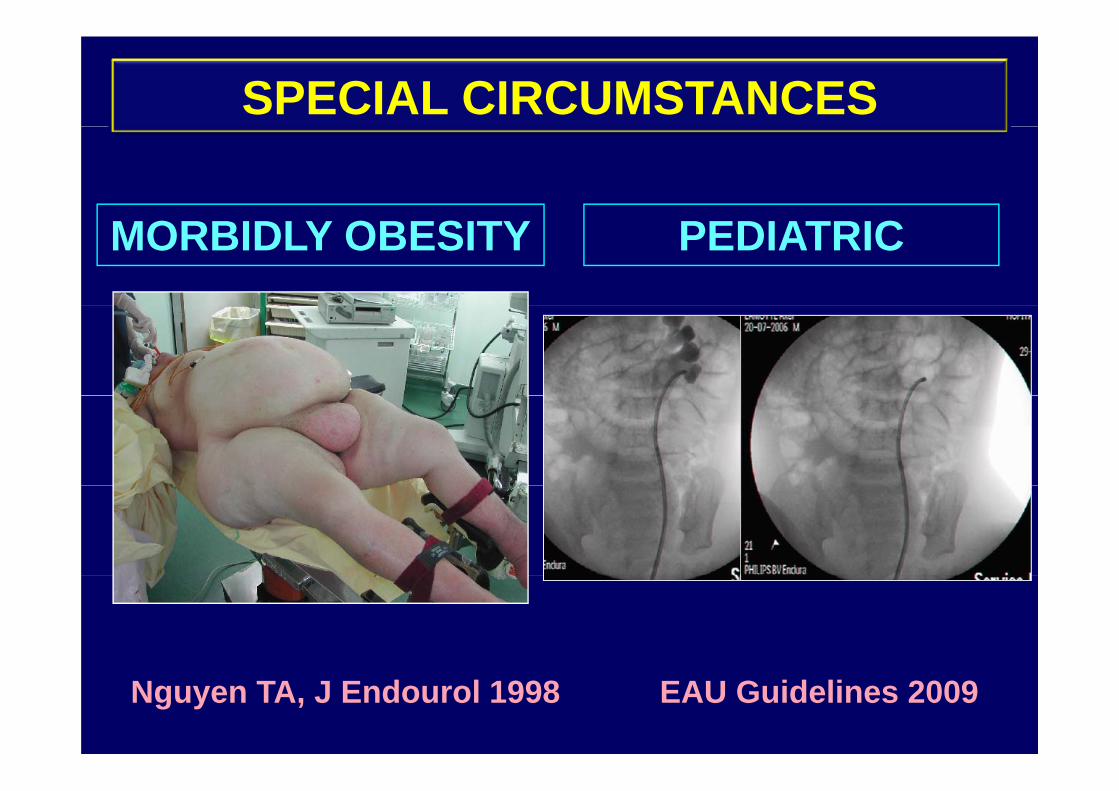
MORBIDLY OBESITY PEDIATRIC
Nguyen TA, J Endourol 1998 EAU Guidelines 2009

SPECIAL CIRCUMSTANCES
INTERNAL / EXTERNAL URINARYINTERNAL / EXTERNAL URINARY DIVERSION

SPECIAL CIRCUMSTANCES
JJ INCRUSTATION MIGRATIONJJ INCRUSTATION-MIGRATION

RESIDUAL FRAGMENTS
< 4 mm….. < 2mm…. ?!
Streem J Urol 1995 ; MS Pearle, J. EndoUrol 2009
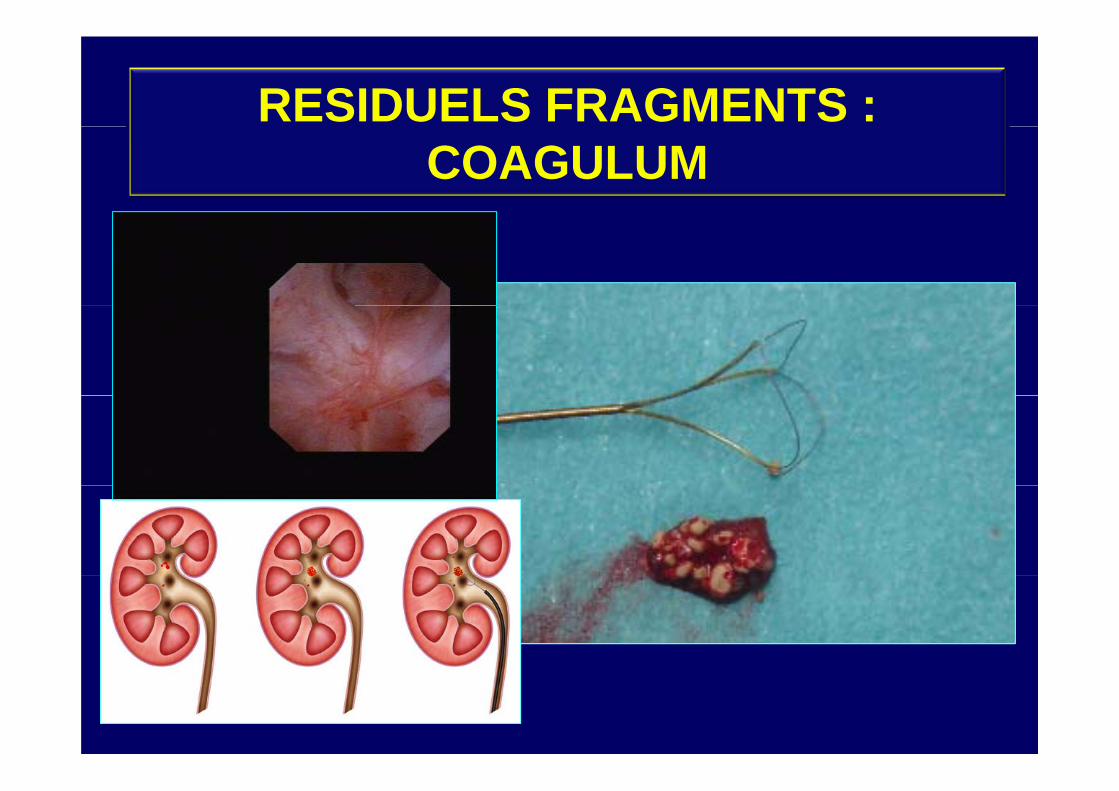
RESIDUELS FRAGMENTS : COAGULUM
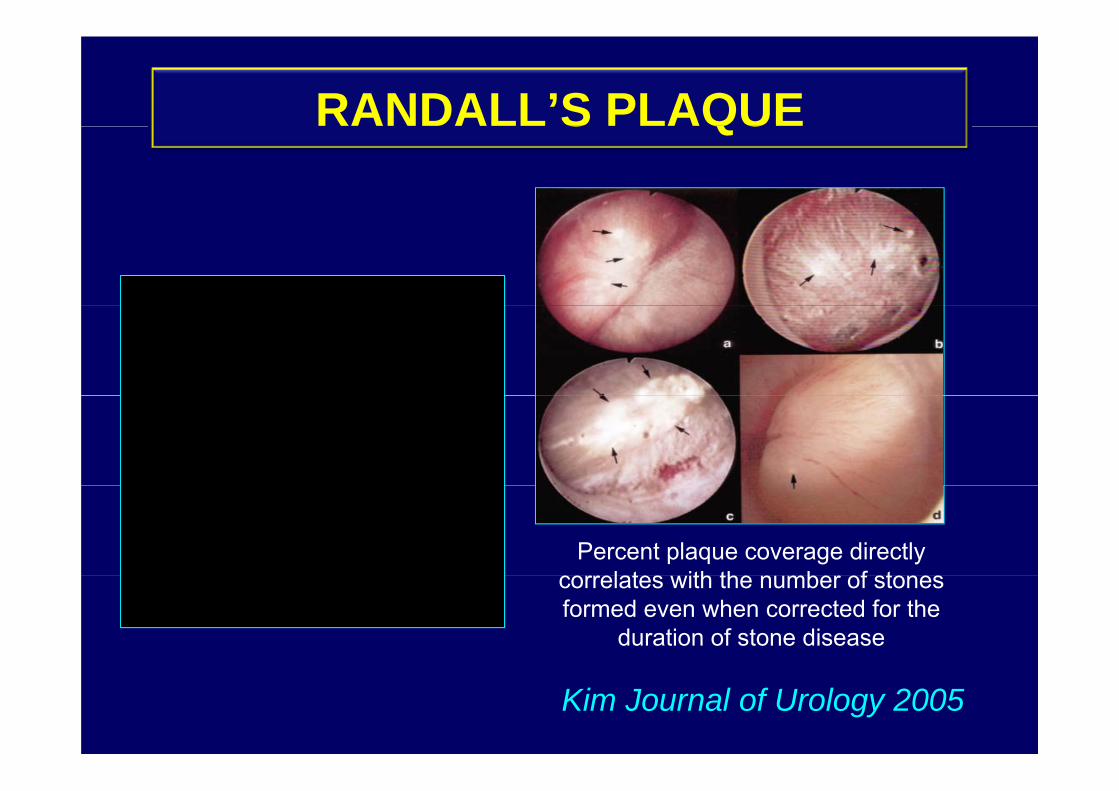
RANDALL’S PLAQUES QU
Percent plaque coverage directly l t ith th b f tcorrelates with the number of stones
formed even when corrected for the duration of stone disease
Kim Journal of Urology 2005

RANDALL’S PLAQUE
Submucosal calcifications erode
S QU
Submucosal calcifications erode to papillary surface whereby exposure to urine results inexposure to urine results in salt deposition an papillary
stone formation.

RANDALL’S PLAQUES QU
Matlaga et al J of UrologyMatlaga et al, J. of UrologyMay 2006

ADVANTAGES-DIS OF FLEXIBLE URS• Stone removed entirely / outpatient procedure• ? waiting for fragments to pass• ? waiting for fragments to pass• Ho-Laser : universally effective /all stones types• Radiolucent stones definitively treated with URSRadiolucent stones definitively treated with URS• Low complication rate (infection, pain, stricture)
Bagley 2008Bagley, 2008• Special circumstances :
• Patient Obesity Dash 2002y• Scoliosis & body deformities Busby 2004• Bleeding diatheses Watterson 2002
R l b liti (HK)• Renal abnormalities (HK) Gupta 2007• Patient preferences
• DIS:DIS:- COST, Time-Consuming, Durability,

CONCLUSIONS
• RIRS: Reliable, Safe & Effective/ kidney stone ttt, y• Technique of RIRS is now well established due to
Development of effective F URS– Development of effective F-URS– Specific Instrumentat° (new grasping devices)– Efficient laser
• Lower Pole Stone is a special indicationp• The challenge in the ensuing years is to refine
technique and patient selection for the growing listtechnique and patient selection for the growing listof endourologic options
• Multicenter Prospective Randomized Studies are• Multicenter Prospective Randomized Studies are needed

oli ier tra er@tnn aphp [email protected]@yahoo.comq @y







