Download - Unit 2 biomedical

Cardiovascular Measurements
DEEPAK.P
UNIT 2
1

DEEPAK.P2
Objective At the end of this UnitYou will learn
Different Biomedical measurements such as ECG, Blood pressure measurement, Cardiac Measurements

DEEPAK.P3
Cardiac Function Measurements

Measuring Cardiac Function1. Blood Pressure
2. Electrocardiogram
3. Stress Test
4. Angiography
4 DEEPAK.P

Measuring Cardiac Function1. Blood Pressure
Measure of fluid pressure within system
a. Systolic Pressure: Pressure generated by contraction
b. Diastolic Pressure: Pressure achieved between contractions.
SBP reflects the amount of work the heart is performing
DBP indicates the amount of peripheral resistance encountered
5 DEEPAK.P

DEEPAK.P6
Blood Pressure Measurement

Blood Pressure MeasurementsAdequate blood pressure is essential to maintain the blood
supply and function of vital organs.
A history of blood pressure measurements has saved many person from death by providing warnings of dangerously high blood pressure (hypertension) in time to provide treatment.
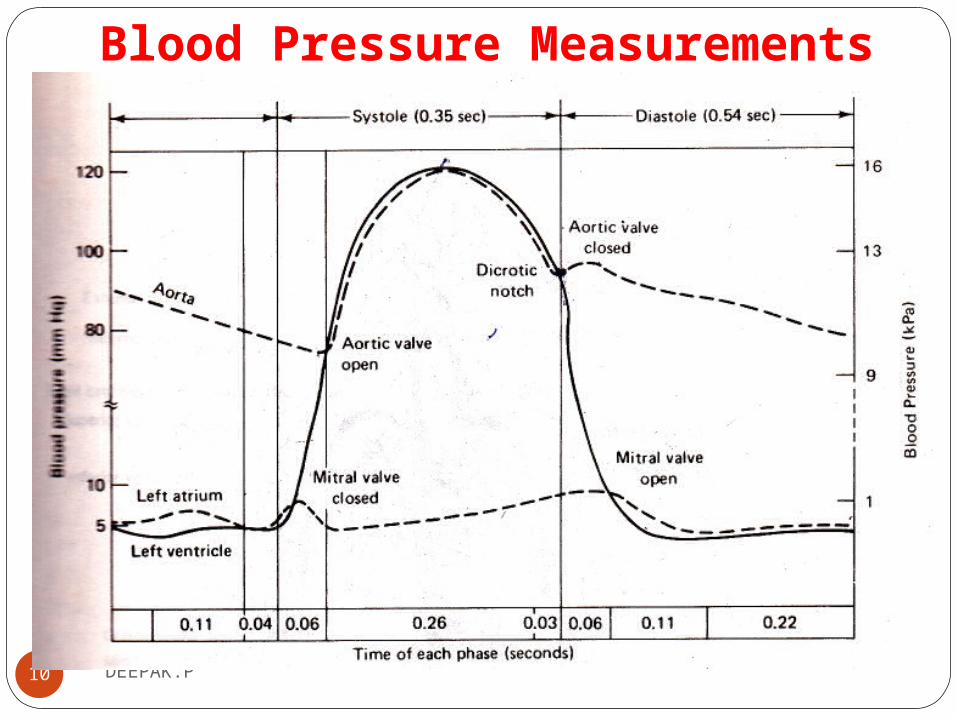
The maximum pressure reached during cardiac ejection is called Systole.
Minimum pressure occurring at the end of ventricular relaxation is called diastole.
7 DEEPAK.P

Blood Pressure MeasurementsIn routine clinical tests, blood pressure is usually measured by
means of an indirect method using a sphygmomanometer (from the Greek word, sphygmos, meaning pulse).
This method is easy to use and can be automated.
The automated indirect method of B.P measurement is called Electro sphygmomanometer
8 DEEPAK.P

Blood Pressure MeasurementsIt has, however, certain disadvantages in that it does not
provide a continuous recording of pressure variations and its practical repetition rate is limited.
Blood pressure is measured in millimeters of mercury (mm Hg) and recorded with the systolic number first, followed by the diastolic number.
A normal blood pressure would be recorded as 120/80 mm Hg.
9 DEEPAK.P
Blood Pressure Measurements
10 DEEPAK.P
Blood Pressure Measurements The systolic pressure is the maximum pressure in an artery at
the moment when the heart is beating and pumping blood through the body.
The diastolic pressure is the lowest pressure in an artery in the moments between beats when the heart is resting.
Both the systolic and diastolic pressure measurements are important
If either one is raised, it means you have high blood pressure (hypertension).
11 DEEPAK.P

Blood Pressure MeasurementsThe nominal values in the basic circulatory systemArterial system-------30-300mmHgVenous system--------5-15mmHgPulmonary system----6-25mmHg
Blood pressure measurement can be classified in to1. Indirect2. Direct
12 DEEPAK.P

Blood Pressure MeasurementsIndirectSimple equipment ,Very little discomfort, Less informative
and IntermittentThe indirect method is also somewhat subjective, and often fails
when the blood pressure is very low (as would be the case when
a patient is in shock).
13 DEEPAK.P
DEEPAK.P14
Indirect Blood Pressure Measurement

Blood pressure measurements1. Auscultatory Auscultatory method uses aneroid sphygmomanometer with
a stethoscope. The auscultatory method comes from the Latin word
"listening.
2. Oscillometric The oscillometric method was first demonstrated in 1876 and
involves the observation of oscillations in the
sphygmomanometer cuff pressure which are caused by the
oscillations of blood flow, i.e., the pulse.15 DEEPAK.P

Blood pressure measurements
3. Palpatory Physician identifies the flow o blood in the arteries by
feeling the pulse
16 DEEPAK.P
1. B.P measurements using sphygmomanometer
17 DEEPAK.P
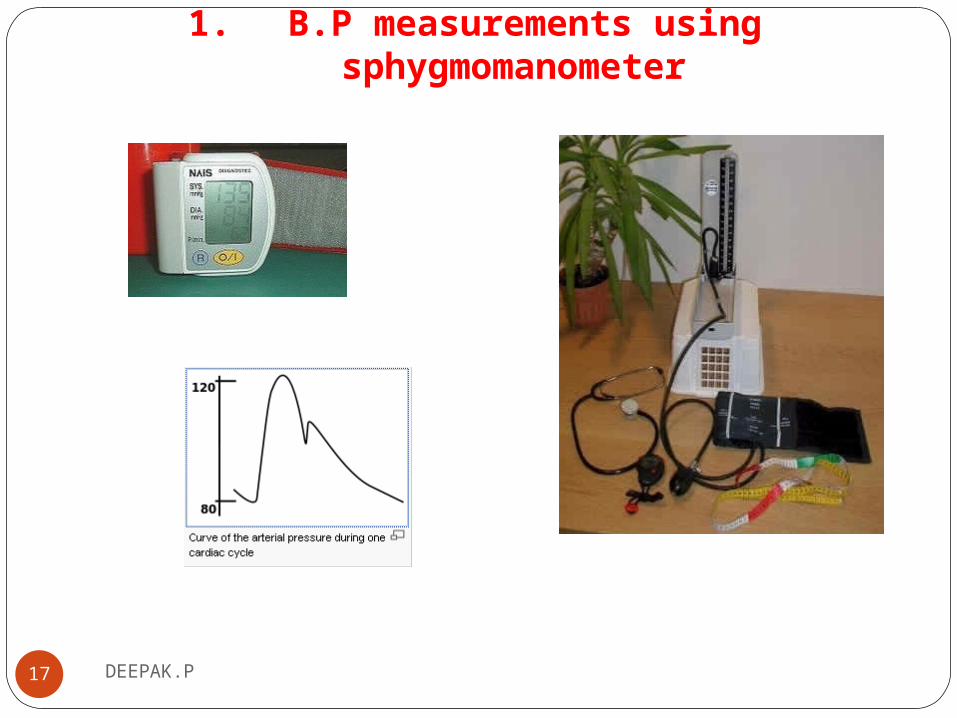
Blood pressure measurements using sphygmomanometerFirst, a cuff is placed around your arm and inflated with a
pump until the circulation is cut off.
A small valve slowly deflates the cuff, and the doctor measuring blood pressure uses a stethoscope, placed over your arm, to listen for the sound of blood pulsing through the arteries.
That first sound of rushing blood refers to the systolic blood pressure; once the sound fades, the second number indicates the diastolic pressure.
18 DEEPAK.P

Blood pressure measurements using sphygmomanometer
19 DEEPAK.P

Blood pressure measurements using sphygmomanometer
20 DEEPAK.P
DEEPAK.P21
Direct Blood Pressure Measurement

2. Direct Blood Pressure Measurements
Provide continuous measurementReliable informationTransducers are directly inserted in to the blood streamMethods for direct blood pressure measurement, on the other
hand, do provide a continuous readout or recording of the blood
pressure waveform and are considerably more accurate than the
indirect method
22 DEEPAK.P
Direct B.P MeasurementMethods of direct blood pressure were classified in to two
1. The clinical method by which the measuring device was coupled to the patient
2.Second, by the electrical principle involved.
First category is expanded, with the electrical principles involved being used as four subcategories.
23 DEEPAK.P
B.P measurements using direct method ln l972, Hales inserted a glass tube into the artery of a horse and vulgarly measured arterial pressure.
Regardless of the electrical or physical principles involved, direct
measurement of blood pressure is usually obtained by one of three methods
1.Catheterization (vessel cut down).
2.Percutaneous insertion.
3.Implantation of a transducer in a vessel or in the heart.
24 DEEPAK.P

Direct B.P Measurement
1. A catheterization method involving the sensing of blood pressure through a liquid column.
In this method the transducer is external to the body, and the blood pressure is transmitted through a saline solution column in a catheter to this transducer
25 DEEPAK.P

Direct B.P Measurement
2. The catheterization method involving the placement of the transducer through a catheter at the actual site of measurement in the blood stream or by mounting the transducer on the tip of the catheter.
3. Percutaneous methods in which the blood pressure is sensed in the vessel just under the skin by the use of a needle or catheter.
4. Implantation techniques in which the transducer is more Permanently placed in the blood vessel or the heart by surgical methods.
26 DEEPAK.P
1. Percutaneous insertion ( direct method)Typically, for Percutaneous insertion , a local anesthetic is injected near the site of invasion.
The vessel is occluded and a hollow needle is inserted at a slight angle towards the vessel.
When the needle is in place, a catheter is fed through the hollow needle , usually with some sort of a guide.
When the catheter is securely place in the vessel, the needle and guide are withdrawn.
27 DEEPAK.P

Percutaneous insertion ( direct method)For some measurements, a type of needle attached to an airtight tube is used, so that the needle can be left in the vessel and the blood pressure sensed directly by attaching a transducer to the tube.
Other types have the transducer built in-the tip of the catheter.
This latter type is used in both percutaneous and catheterization models.
28 DEEPAK.P
2. Catheterization( direct method)It was first developed in the late 1940s and has become a major technique for analyzing the heart and other components.
Catheter is a long tube that is inserted in to the heart or major vessels.
Sterilized catheters are used Apart from obtaining blood pressures in the heart chamber and great vessels, this technique is also used to obtain blood samples from the heart for oxygen-content analysis and to detect the location of abnormal blood flow pathways.
29 DEEPAK.P

Catheterization( direct method)
Measurement of blood pressure with a catheter can be achieved in two ways. In the first method is to introduce a sterile saline solution into the catheter so that the fluid pressure is transmitted to a transducer out side the body.
In the second method, pressure measurements are obtained at the source.Here,the transducer is introduced into the catheter and pushed to the point at which the pressure is to be measured. or the transducer is mounted at the tip of the catheter.
30 DEEPAK.P

Catheterization( direct method)
31 DEEPAK.P

Catheterization( direct method)
This device is called a catheter-tip blood pressure transducer.For mounting at the end of a catheter, one manufacturer uses an un bonded resistance strain gage in the transducer, whereas another uses a variable inductance transducer .Implantation techniques involve major surgery.
Transducers can be categorized by the type of circuit element used to sense the pressure variations, such as capacitive, inductive, and resistive.Since the resistive types are most frequently used.
32 DEEPAK.P

B.P measurements using direct method ln l972, Hales inserted a glass tube into the artery of a horse and crudely measured arterial pressure.Regardless of the electrical or physical principles involved, directmeasurement of blood pressure is usually obtained by one of three methodsPercutaneous insertion.Catheterization (vessel cut down).lmplantation of a transducer in a vessel or in the heart.
33 DEEPAK.P
DEEPAK.P34
Heart

HeartThe cardiovascular system is made of the heart, blood and
blood vessels
35 DEEPAK.P

Anatomy of the Heart The human heart is a four-chambered muscular organ
The heart is enclosed in a pericardial bag.
The purpose of it is to protect and lubricate the heart.
The peircardium is the outermost covering of your heart.
It protects against friction rubs and protects against shocks(traumatic) as it contains 40-50 ml of pericardial fluid.
It acts as a shock absorber
.36 DEEPAK.P
Anatomy of the Heart Heart normally pumps 5 liters of blood per minute
Two side of the wall is separated by the septum or dividing wall of tissue.
This septum include AV node
Right auricle is lies between inferior(lower) and superior(upper) vena cava
At the junction of Superior vena cava and right atrium SA node is situated.
.37 DEEPAK.P
Anatomy of the Heart The communication between atria and ventricle is
accomplished only through AV node and delay line.The activated AV node, after a delay, initiates an impulse in to
the ventricle, through the bundle of his, and bundle branches
that connect to the purkinje fibers.
1. Ventricle wall is thicker than auricular wall2. Left atrium is smaller than Right atrium3. Left ventricle is considered as most important.4. It wall thickness is 3 times than right ventricle.
38 DEEPAK.P

Heart anatomyLeft heart is considered as pressure pump
Right heart is similar to a volume pump
Muscle contraction of left heart is larger and stronger than that of right heart.
39 DEEPAK.P

Heart circulationThe work of the heart is to pump blood to the lungs through
pulmonary circulation and to the rest of the body through systemic circulation.
In pulmonary circulation, the pressure difference between arteries and veins is small.
In systemic circulation, the pressure difference between arteries and veins is very high.
40 DEEPAK.P

Heart ValvesThe pumping action is accomplished by systematic contraction
and relaxation of the cardiac muscle in the myocardium.Cardiac muscles gets the blood supply from coronary
circulation.Heart contains 4 valves Tricuspid---Between RA and RV----- Three cupsPulmonary/Semi lunar-- Between RV and Right lungsMitral/Bicuspid--- Between LA and LV---- Two cupsAortic--- Between LV and aortaThe sounds associated with the heartbeat are due to vibrations
in the tissues and blood caused by closure of the valves.
41 DEEPAK.P

Heart valves
42 DEEPAK.P

Heart SoundListening of sound produced by heart is called auscultationHeart sound is heard by the physician through his stethoscope.This sound is called Korotkoff soundThe sounds associated with the heartbeat are due to
vibrations in the tissues and blood caused by closure of the valves.
Normal heart produces two sounds called lub-dubLub is called the first heart soundIt occurs at the time of QRS complex of the ECGLub is related to the closure of atrioventricular valveWhich permits blood flow from auricle to ventricles.It prevents blood flow in reverse direction
43 DEEPAK.P

Heart SoundDub is called the second heart soundDub is related to the closure of semilunar valveThis valve releases blood into the pulmonary and systemic
circulation system.It occurs at the end of the T wave of of the ECGAbnormal heart sounds is called murmurs.It is due to the improper opening of the valve.Graphic recording of heart sound is also possibleIt is called phonocardiogramRecording of the vibrations of the heart against thoracic
cavity is called vibrocariogram
44 DEEPAK.P

DEEPAK.P45
Cardiac Output and Rate
Cardiac OutputCardiac output is the volume of blood pumped by the heart
per minute (mL blood/min).Cardiac output is a function of heart rate and stroke volume.Cardiac Output in mL/min = heart rate (beats/min) X stroke
volume (mL/beat)Cardiac Output = 70 (beats/min) X 70 (mL/beat) = 4900
mL/minute.The total volume of blood in the circulatory system of an
average person is about 5 liters (5000 mL).
46DEEPAK.P
Cardiac OutputThe heart rate is simply the number of heart beats per
minute. This can be easily measured through the use of heart rate
monitors or taking ones pulse (counting the ‘pulses’ at the radial artery for example over a one minute period).
Children (ages 6 - 15) 70 – 100 beats per minute Adults (age 18 and over) 60 – 100 beats per minute
47DEEPAK.P

Cardiac OutputThe stroke volume is the volume of blood, in milliliters (mL),
pumped out of the heart with each beat.Stroke volume (SV) refers to the quantity of blood pumped
out of the left ventricle with every heart beat.If the volume of blood increased (waste products not being
removed to the kidneys due to kidney failure for example)
then there would be a greater quantity of blood within the
system increasing the pressure within.
48DEEPAK.P

Cardiac OutputIncreasing either heart rate or stroke volume increases cardiac
output.
49DEEPAK.P

Cardiac OutputThe SA node of the heart is enervated by both sympathetic and
parasympathetic nerve fibers. Under conditions of rest the parasympathetic fibers release
acetylcholine, which acts to slow the pacemaker potential of the
SA node and thus reduce heart rate.Under conditions of physical or emotional activity sympathetic
nerve fibers release norepinephrine, which acts to speed up the
pacemaker potential of the SA node thus increasing heart rate.
50DEEPAK.P

Cardiac OutputStroke volume is increased by 2 mechanisms:1. Increase in end-diastolic volume2. Increase in sympathetic system activity
51DEEPAK.P

Cardiac Output
52DEEPAK.P

Cardiac OutputAn increase in venous return of blood to the heart will result in
greater filling of the ventricles during diastole. Consequently the volume of blood in the ventricles at the end of
diastole, called end-diastolic volume, will be increased. A larger end-diastolic volume will stretch the heart. Stretching the muscles of the heart optimizes the length-
strength relationship of the cardiac muscle fibers, resulting in
stronger contractility and greater stroke volume.
53DEEPAK.P

DEEPAK.P54
ECG

Electro Cardio Gram(ECG)Bio electric potentials generated by heart muscles are called
Electro Cardio Gram.
It is sometimes called EKG(Electro Kardio Gram)
Electrocardiography (ECG) is an interpretation of the electrical activity of the heart over a period of time.
The recording produced by this noninvasive procedure is termed as electrocardiogram (also ECG or EKG).
55 DEEPAK.P
Early ECG measurement system
56 DEEPAK.P

Electro Cardio Gram(ECG)Heart is divided in to 4 chamberUpper chamber------ Atria( left and right)Lower chamber------Ventricles(left and right)Right auricles receives blood from the veins and pump in to
right ventricles.The right ventricle pump the blood to lungs, where it is
oxygenatedThe oxygenated blood enters in to left auricle.Left auricle pumps blood in to left ventricle.
To work the cardiovascular system properly , the atria and ventricles must operate in a proper time relationship.
57 DEEPAK.P

Electro Cardio Gram(ECG)Action potential in the heart originates near the top of the
right atrium at a point called pacemaker or sinoatrial node (S.A node).
This action potential is then propagated in all directions along the surface of both atria.
The waves terminate at a point near the centre of the heart is called A.V node(Atrioventricular node)
At this point some special fiber act as a delay line to provide proper timing between the action of auricles and ventricles.
Once electrical pulses has passed through the delay line , it is spread to all parts of both ventricles by the bundle of His
It is called purkinje fibers.
58 DEEPAK.P

Electro Cardio Gram(ECG)This bundle is divided in to two branches to initiate action
potential simultaneously in the two ventricles.
59 DEEPAK.P
ECG waveform/ PQRST wave form

Electro Cardio Gram(ECG)The “P” wave is called base line or isopotential line.
P wave ----- De polarization of Auricles.
Combined QRS wave---- Re-polarization of atria and depolarization of ventricles
T wave ----- Ventricular re polarizationU wave --- after potentials in the ventricles
P-Q interval – Time during which excitation wave is delayed in the fiber near AV node.
60 DEEPAK.P

Electro Cardio Gram(ECG)
61 DEEPAK.P

ECG
62 DEEPAK.P

ECG
63 DEEPAK.P

ECG
64 DEEPAK.P

ECG
65 DEEPAK.P

DEEPAK.P66
ECG Recorder

Simple ECG measurement system
67 DEEPAK.P
ECG measurement systemThe ECG system comprises four stages, each stage is as follows:(1)The first stage is a transducer—AgCl electrode, which convert ECG into electrical voltage. The voltage is in the range of 1 mV ~ 5 mV.(2) The second stage is an instrumentation amplifier (Analog Device, AD624), which has a very high CMRR (90dB) and high gain (1000), with power supply +9V and -9V.(3) We use an opto-coupler (NEC PS2506) to isolate the In-Amp and output. (4) After the opto-coupler is a bandpass filter of 0.04 Hz to 150 Hz filter. It’s implemented by cascading a low-pass filter and a high pass filter.
68 DEEPAK.P

Simple Block diagram of ECG
69 DEEPAK.P

ECG Machine
70 DEEPAK.P

DEEPAK.P71
ECG Leads
EKG Leads
Leads are electrodes which measure the difference in electrical potential between either:
1. Two different points on the body (bipolar leads)
2. One point on the body and a virtual reference point with zero electrical potential, located in the center of the heart (unipolar leads)

EKG Leads
The standard EKG has 12 leads:
3 Standard Limb Leads
3 Augmented Limb Leads
6 Precordial Leads
The axis of a particular lead represents the viewpoint from which it looks at the heart.

Placement of ECG electrode
74 DEEPAK.P
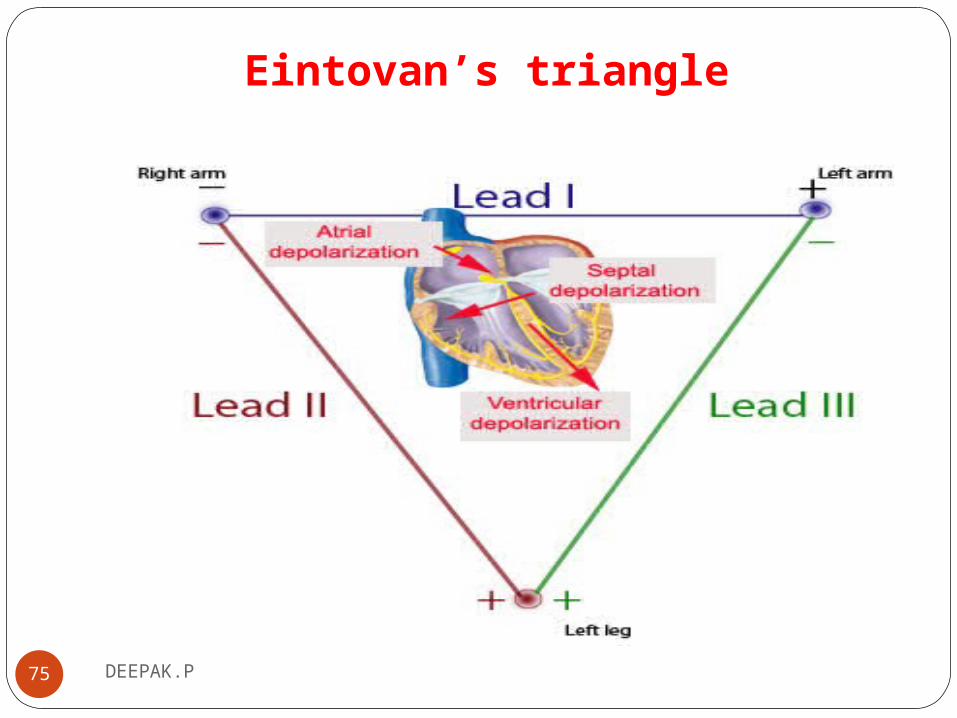
Eintovan’s triangle
75 DEEPAK.P
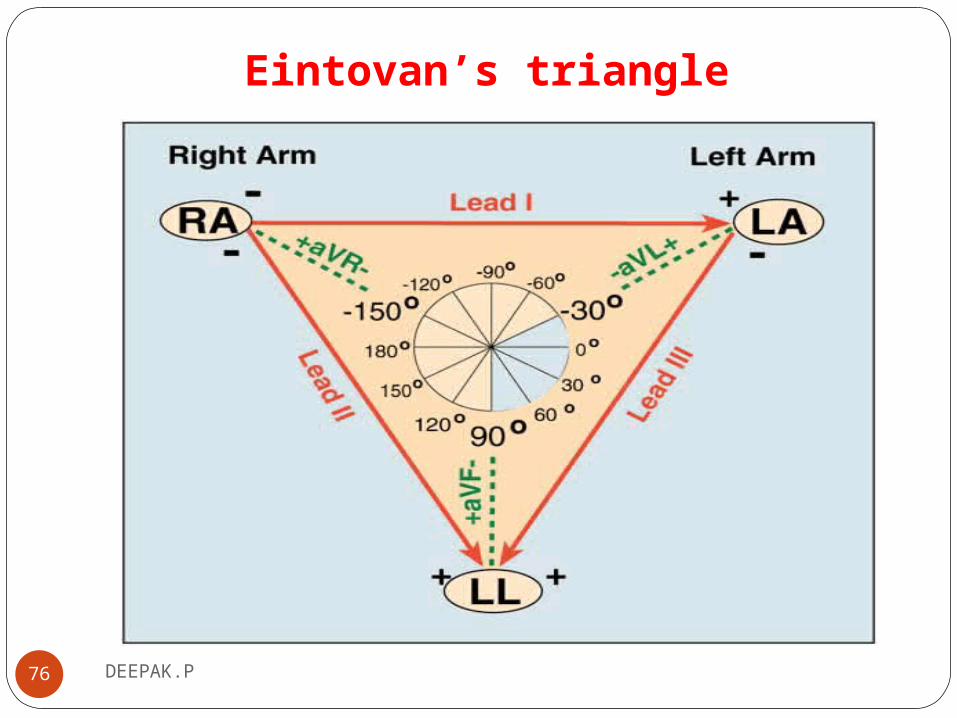
Eintovan’s triangle
76 DEEPAK.P
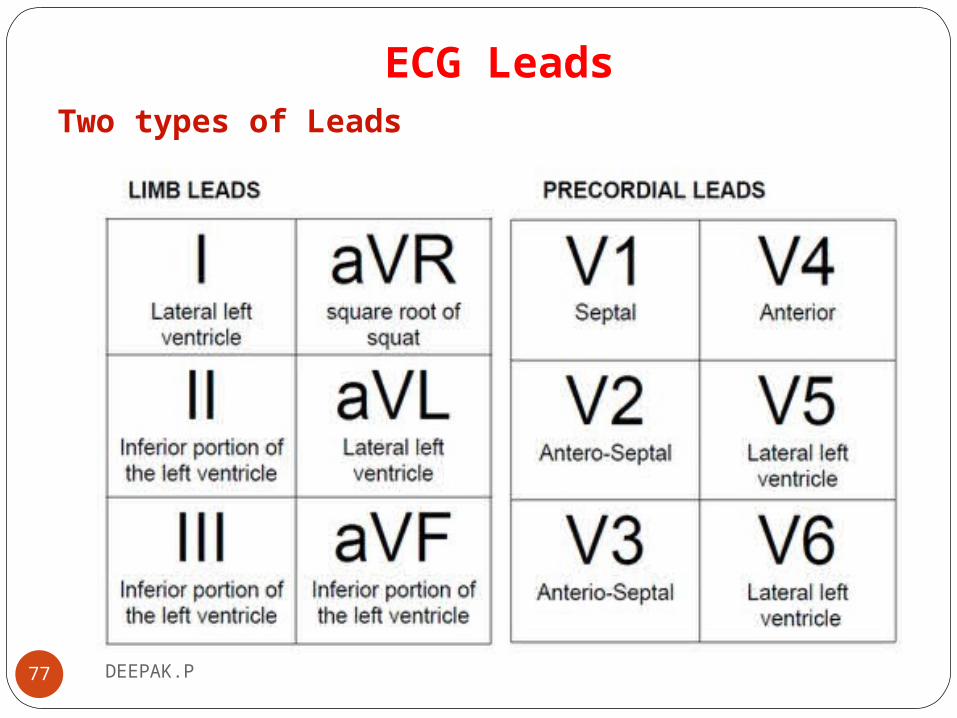
ECG LeadsTwo types of Leads
77 DEEPAK.P

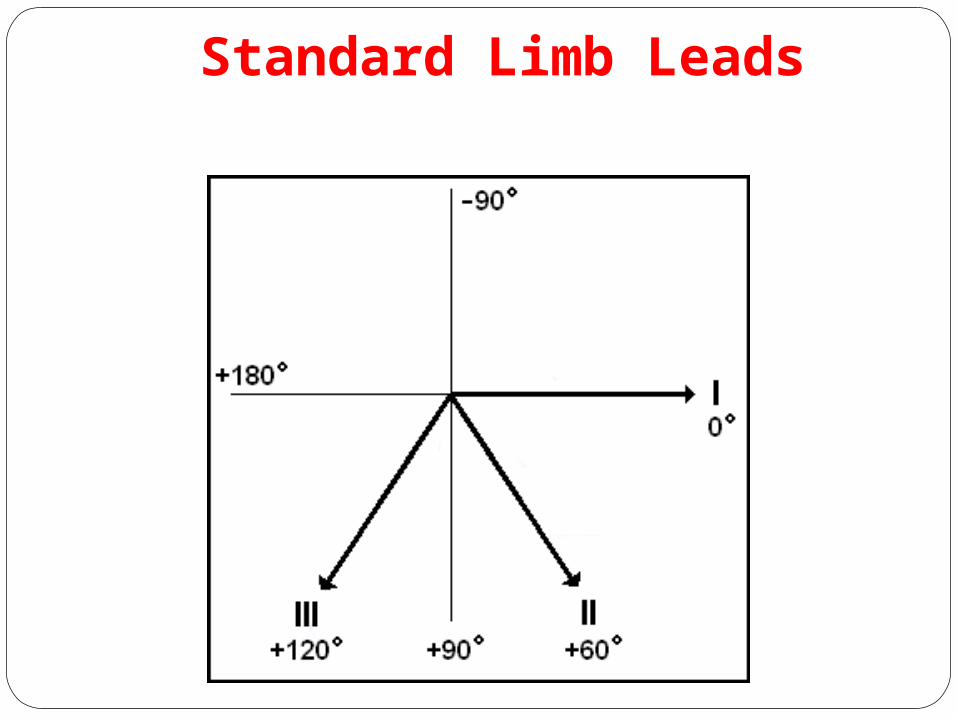
Standard Limb Leads
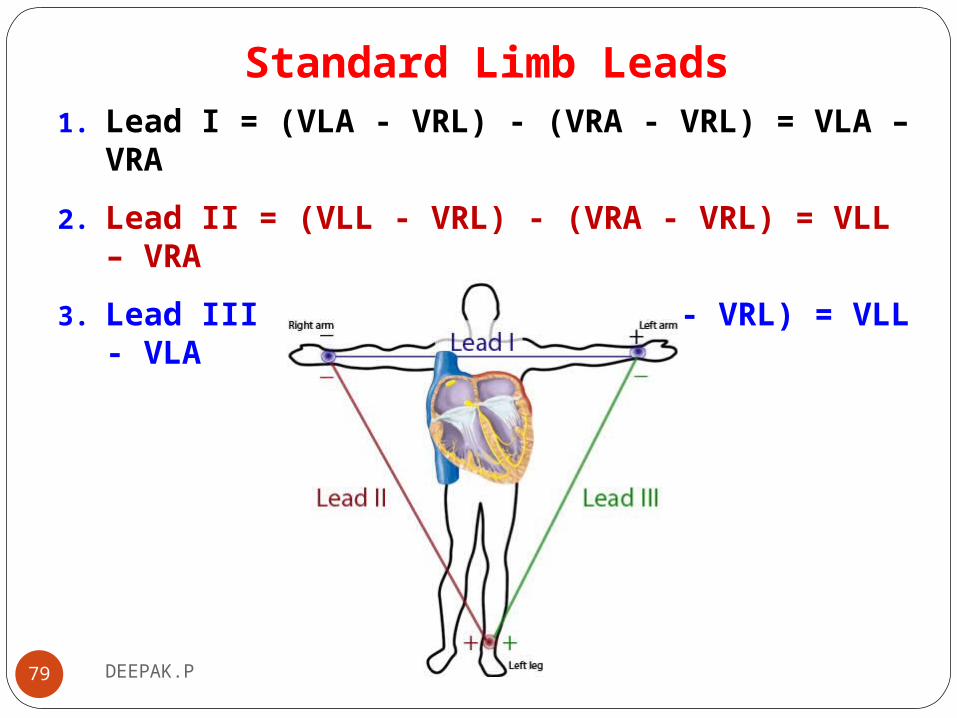
Standard Limb Leads1. Lead I = (VLA - VRL) - (VRA - VRL) = VLA – VRA
2. Lead II = (VLL - VRL) - (VRA - VRL) = VLL – VRA
3. Lead III = (VLL - VRL) - (VLA - VRL) = VLL - VLA
79 DEEPAK.P
Standard Limb Leads

Augmented Limb Leads
81 DEEPAK.P

Augmented Limb Leads

Chest Leads
Chest LeadsUnipolar (+) chest leads (horizontal plane): Leads V1, V2, V3: (Posterior Anterior)
Leads V4, V5, V6:(Right Left, or lateral)
The 6 leads are labelled as "V" leads and numbered V1 to V6. They are positioned in specific positions on the rib cage.
84 DEEPAK.P

All Limb Leads
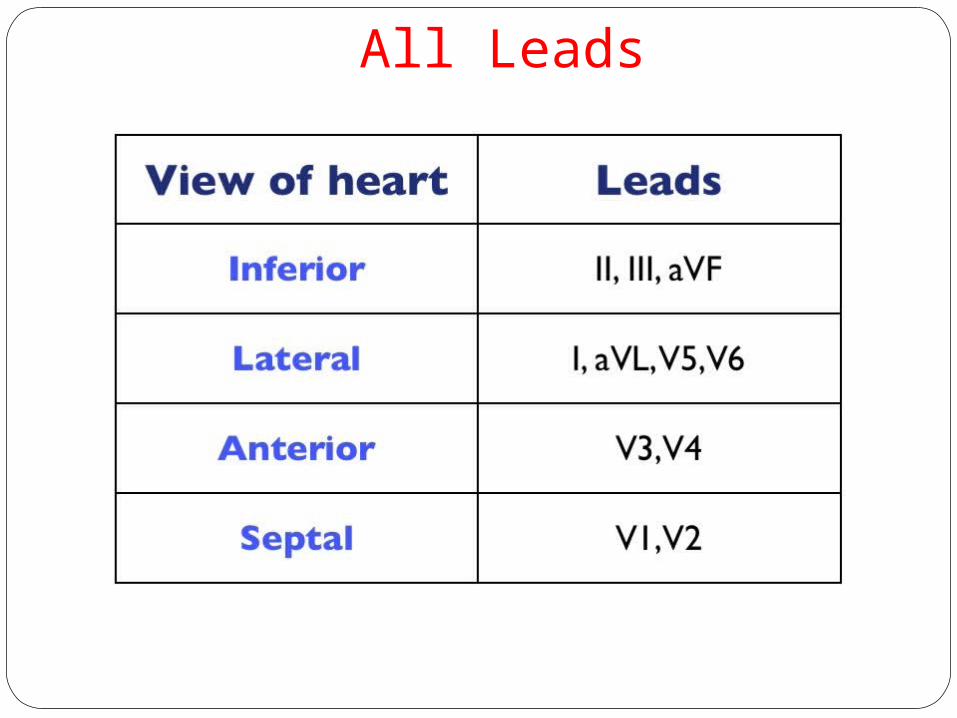
All Leads
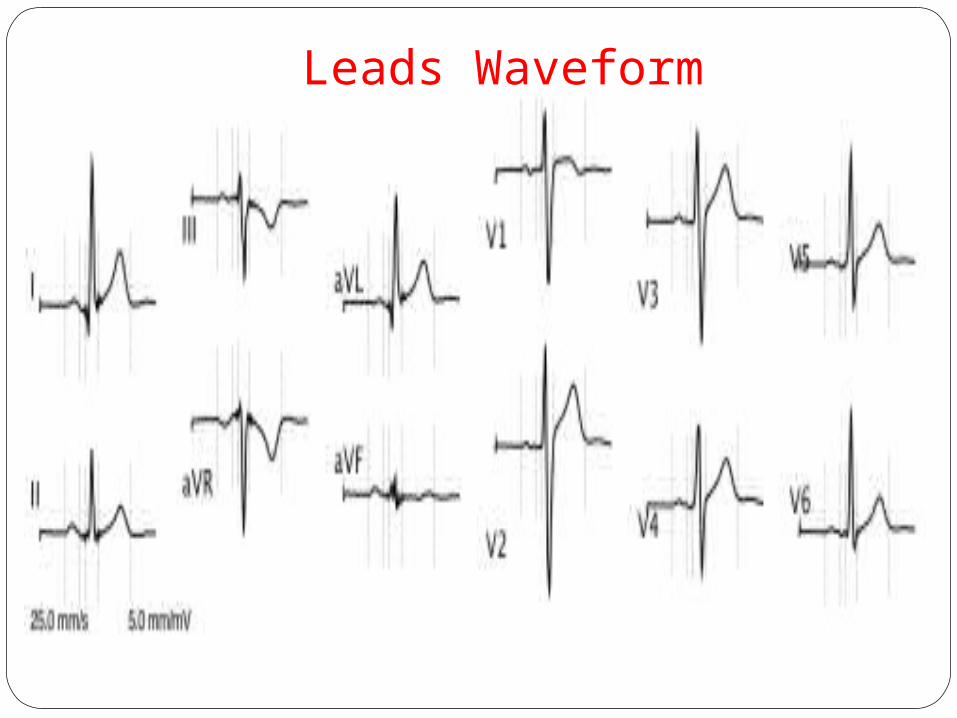
Leads Waveform
DEEPAK.P88
ECG Amplifier

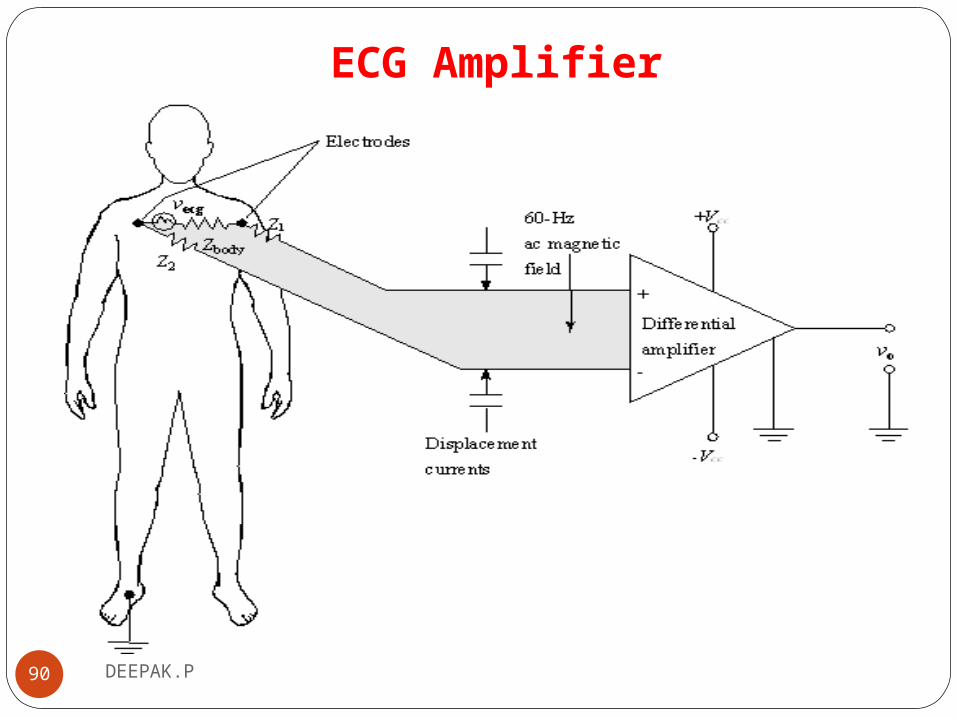
ECG AmplifierWe measure the ECG by connecting two electrodes on the
right and left chest respectively, as shown.
The body should be connected to ground of the circuits, so that we connect the leg to the ground.
To boost the raw ECG signal level without boosting the noise amplifiers are used.
An electronic circuit should amplify the potential difference across a lead
89 DEEPAK.P
ECG Amplifier
90 DEEPAK.P

ECG Amplifier
91 DEEPAK.P

Instrumentation Amplifier
92 DEEPAK.P

Instrumentation Amplifier
93 DEEPAK.P

Practical Instrumentation Amplifier
94 DEEPAK.P

Instrumentation AmplifierLow signal noiseVery high open-loop gainVery high common-mode rejection ratioVery high input impedanceInstrumentation amplifier can reduce common-mode noise, but
not completely
95 DEEPAK.P
DEEPAK.P96
Phonocardiogram

Heart SoundListening to sound produced by human organ is called
auscultation.
Heat sound is related with the closing of valves.
Hippocrates (460-377 BC) provided the foundation for
auscultation when he put his ear against the chest of a patient
and described the sounds he could hear from the heart.
97 DEEPAK.P

Heart Sound
The biggest breakthrough in auscultation came in 1816 when René Laennec (1781-1826) invented the stethoscope
98 DEEPAK.P

Heart SoundThere are two types of sounds 1. High frequency sounds associated with closing and opening of
the valves and 2. Low frequency sounds related to early and late ventricular
filling events.
99 DEEPAK.P

Heart Sound1. Mitral area:2. Tricuspid area:3. Aortic area:4. Pulmonic area:
Microphones and accelerometers are the natural choice of sensor when recording sound.
100 DEEPAK.P
Heart Sound1. The first heart sound (S1) – systolic sound:
Appears at 0.02 – 0.04s after the QRS complex the “lub” frequency of 30-40Hz
2. The second heart sound (S2) – diastolic soundAppears in the terminal period of the T wave the “dub”frequency of 50-70 Hz
3. The third heart sound (S3) - protodiastolic soundLow frequency
101 DEEPAK.P

Heart Sound4. The fourth heart sound (S4) – presistolic sound
Appears at 0.04s after the P wave (late diastolic-just before S1)
Low frequency S1 – onset of the ventricular contraction S2 – closure of the semilunar valves S3 – ventricular run S4 – atrial gallop
102 DEEPAK.P
Heart Sound
103 DEEPAK.P

Heart Sound
104 DEEPAK.P

PhonocardiographyGraphic recording of heart sound is called phonocardiogram
( PCG)
Phonocardiography, diagnostic technique that creates a graphic record, or phonocardiogram, of the sounds and murmurs produced by the contracting heart,
The phonocardiogram is obtained either with a chest microphone or with a miniature sensor in the tip of a small tubular instrument that is introduced via the blood vessels into one of the heart chambers.
105 DEEPAK.P

Phonocardiography
106 DEEPAK.P

Phonocardiography
107 DEEPAK.P

DEEPAK.P108
Ballistocardiograph

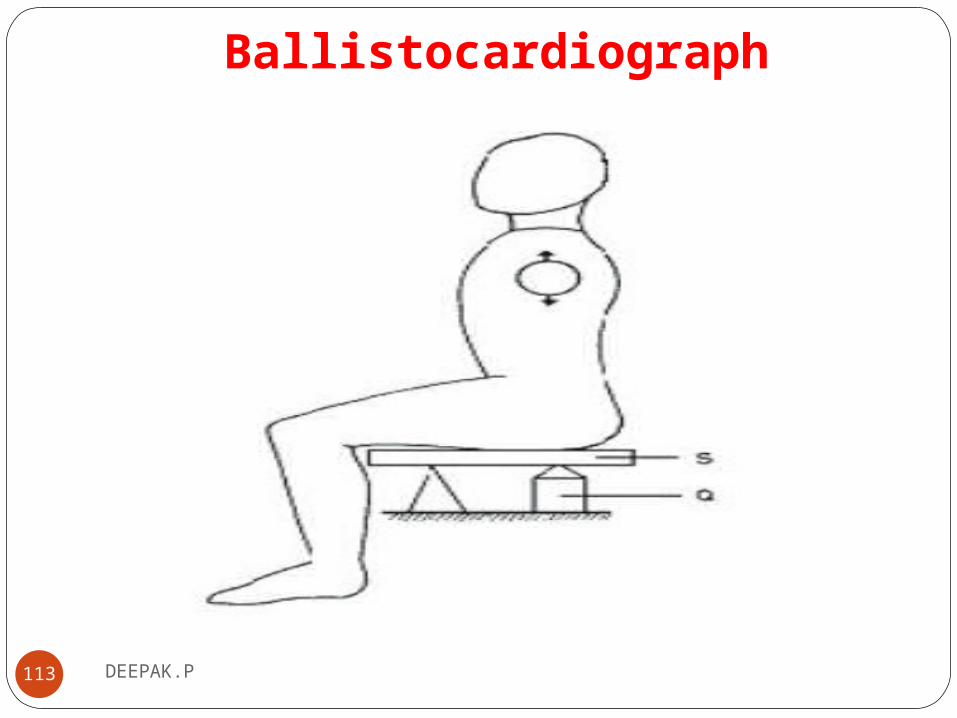
Ballistocardiograph(BCG)Ballistocardiography (BCG) is based upon Newton's Third
Law, which states that for every action there is an equal and opposite reaction.
Ballistocardiography, graphic recording of the stroke volume of the heart for the purpose of calculating cardiac output.
BCG measures cardiac output by means of recoil forces. With each systole, blood is ejected through the aorta.
There are two basic types of ballistocardiographic methods. In the older method, high-frequency BCG, the subject is
restrained and force is measured by displacement of a supporting spring.
109 DEEPAK.P

BallistocardiographIn ultra-low-frequency BCG, the subject is free to move and
force is calculated from his/her mass and the measured acceleration.
Typically, in obtaining a BCG the subject lies on a light, frictionless table which is either suspended from the ceiling or supported from below on an air cushion.
The movements of this ballistotable, resulting from body movements produced by cardiac activity, are transduced into electrical energy by means of either mechanoelectronic tubes (Geddes & Baker, 1968) or a compound transducer in which movement of the table is converted into a varying light intensity
110 DEEPAK.P

Ballistocardiograph Methods
111 DEEPAK.P

BallistocardiographDock and Taubman (1949) recorded body movements without
the use of a ballistotable by devising a photoelectric transducer which was attached to the shins of the subject.
Cardiac-induced body movements alter the transmission of light to these photoelectric detectors, thus producing a variable electrical output proportional to movement.
112 DEEPAK.P
Ballistocardiograph
113 DEEPAK.P
DEEPAK.P114
Defibrillator

Defibrillator
115 DEEPAK.P

DefibrillatorDefibrillation is a process in which an electronic device gives
an electric shock to the heart.
This depolarizes a critical mass of the heart muscle, terminates the arrhythmia and allows normal sinus rhythm to be reestablished.
This helps reestablish normal contraction rhythms in a heart having dangerous arrhythmia or in cardiac arrest.
Defibrillation is a common treatment for life-threatening ventricular fibrillation and pulse less ventricular tachycardia.
116 DEEPAK.P

Defibrillator
117 DEEPAK.P
DefibrillatorDefibrillators were first demonstrated in 1899 by Jean-
Louis Prévost and Frédéric Batelli, two physiologists from University of Geneva, Switzerland.
These early defibrillators used the alternating current from a power socket, transformed from the 110–240 volts available in the line, up to between 300 and 1000 volts, to the exposed heart by way of "paddle" type electrodes.
118 DEEPAK.P

DefibrillatorEarly successful experiments of successful defibrillation by the
discharge of a capacitor performed on animals were reported by N. L. Gurvich and G. S. Yunyev in 1939.
119 DEEPAK.P

DefibrillatorIn recent years small portable defibrillators have become
available. These are called automated external defibrillators or AEDs.Nowadays implantable defibrillator are available in the
market
120 DEEPAK.P

Defibrillator Principles
121 DEEPAK.P
Defibrillator PrinciplesThere are many types of defibrillators 1. Monophasic, 2. Biphasic and 3. Internal.The first two types are known as external defibrillators, and
these are used on the exterior of the patient’s chest.
Pads are placed on the chest and a button is pushed to send an electrical current to the heart.
The type of external defibrillator determines the type of current sent to the heart.
122 DEEPAK.P

Defibrillator Principles
123 DEEPAK.P

Defibrillator PrinciplesA monophasic defibrillator sends out a single electrical pulse.
This shot of electricity goes from one pad to the other with the heart in between.
A monophasic defibrillator needs high electricity levels to function correctly.
The charge is typically started at 200 joules and increased to 300 joules; if necessary, the highest level is 360 joules.
124 DEEPAK.P

Defibrillator Principles
125 DEEPAK.P
Defibrillator PrinciplesThe second type of external device is biphasic, and it sends out
two electrical currents.
A current first travels from one pad to the other.
The electricity then reverses direction and returns a current to the first pad.
This enables the biphasic device to use less electricity than the monophasic variety.
126 DEEPAK.P

Defibrillator PrinciplesThe biphasic defibrillator also is able to adjust to the patient's
body type.
127 DEEPAK.P

Defibrillator PrinciplesThe third type of defibrillator is the internal or implantable
variety, which is surgically placed in the chest of a patient.
The electrode wires are inserted through the veins into the right chamber of the heart.
An internal defibrillator monitors the heartbeat for any irregularities.
Internal defibrillators run on battery power instead of electricity.
128 DEEPAK.P

Block Diagram of Defibrillator
129 DEEPAK.P
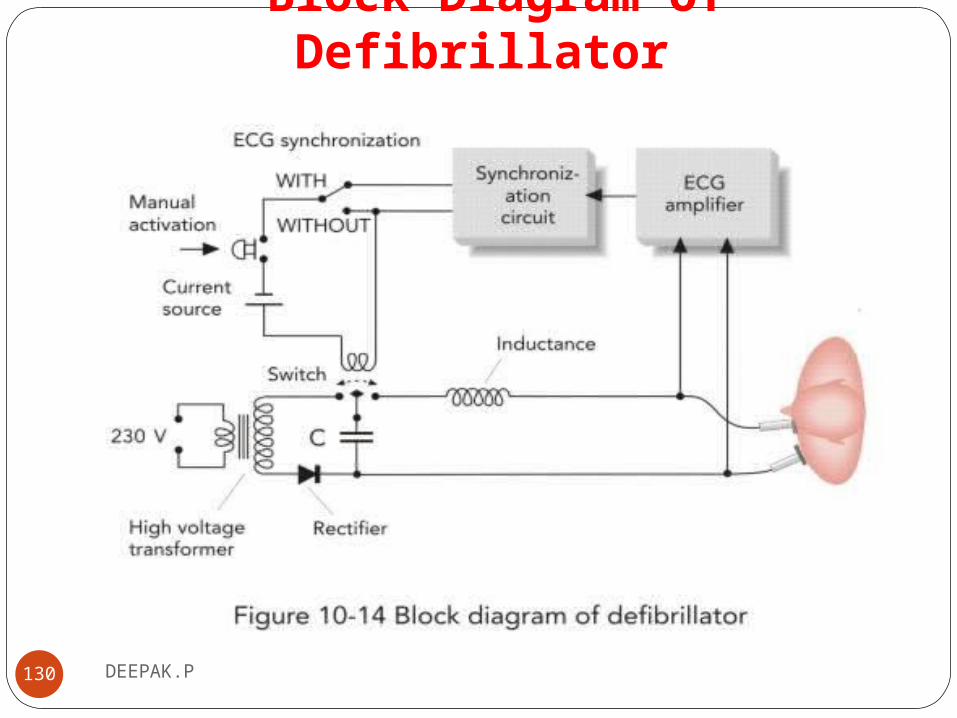
Block Diagram of Defibrillator
130 DEEPAK.P

Block Diagram of Defibrillator
131 DEEPAK.P
Defibrillator Electrodes
132 DEEPAK.P

Defibrillator Electrodes
133 DEEPAK.P
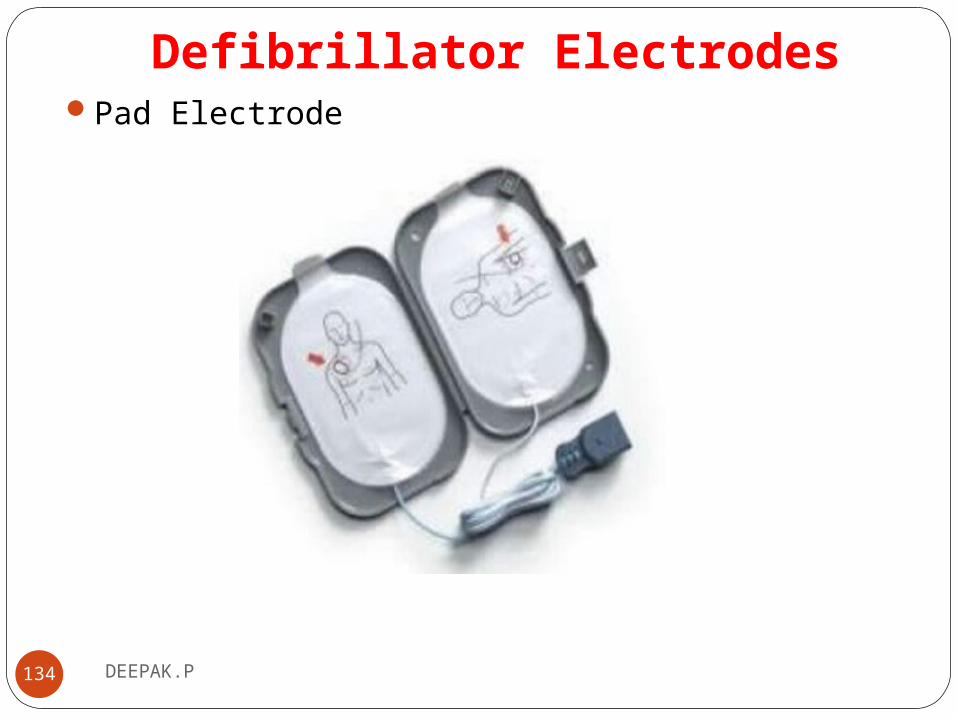
Defibrillator ElectrodesPad Electrode
134 DEEPAK.P

DEEPAK.P135
Pacemaker

PacemakerA pacemaker (or artificial pacemaker, so as not to be
confused with the heart's natural pacemaker) is a medical device that uses electrical impulses, delivered by electrodes contracting the heart muscles.
The primary purpose of a pacemaker is to maintain an adequate heart rate,
Modern pacemakers are externally programmable and allow the cardiologist to select the optimum pacing modes for individual patients.
136 DEEPAK.P
Pacemaker
137 DEEPAK.P
PacemakerDoctors recommend pacemakers for many reasons.
The most common reasons are bradycardia and heart block.
Bradycardia is a heartbeat that is slower than normal.
Heart block is a disorder that occurs if an electrical signal is slowed or disrupted as it moves through the heart.
Heart block can happen as a result of aging, damage to the heart from a heart attack, or other conditions that disrupt the heart's electrical activity.
138 DEEPAK.P

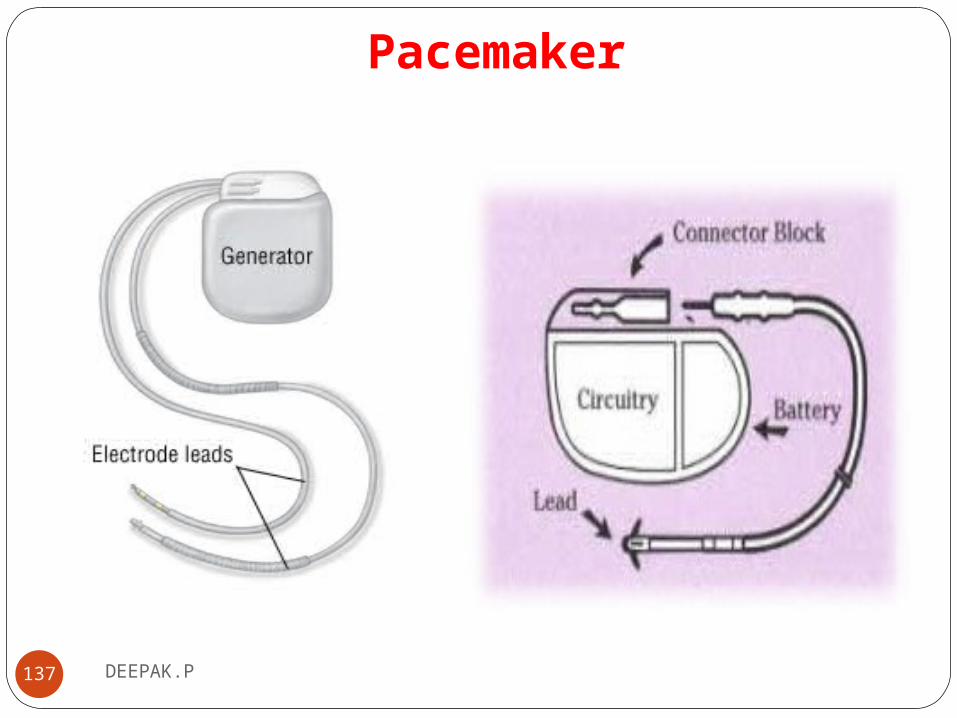
PacemakerA pacemaker consists of a battery, a computerized generator,
and wires with sensors at their tips. (The sensors are called electrodes.)
The battery powers the generator, and both are surrounded by a thin metal box.
The wires connect the generator to the heart.
A pacemaker helps monitor and control your heartbeat.
139 DEEPAK.P

PacemakerThe electrodes detect your heart's electrical activity and send
data through the wires to the computer in the generator.
The two main types of programming for pacemakers are demand pacing and rate-responsive pacing.
A demand pacemaker monitors your heart rhythm.
It only sends electrical pulses to your heart if your heart is beating too slow or if it misses a beat.
140 DEEPAK.P

PacemakerA rate-responsive pacemaker will speed up or slow down
your heart rate depending on how active you are.
To do this, the device monitors your sinus node rate, breathing, blood temperature, and other factors to determine your activity level.
People may need a pacemaker for a variety of reasons — mostly due to one of a group of conditions called arrhythmias, in which the heart's rhythm is abnormal.
141 DEEPAK.P

PacemakerDuring an arrhythmia, the heart may not be able to pump
enough blood to the body.
This can cause symptoms such as fatigue (tiredness), shortness of breath, or weakness.
Severe arrhythmias can damage the body's vital organs and may even cause loss of consciousness or death.
A pacemaker can often be implanted in your chest with a minor surgery.
142 DEEPAK.P

Pacemaker TypesThere are three types of artificial pacemakersSingle chamber pacemakers set the pace of only one of your
Heart s chamber s , usually the left ventricle , and need just one lead
143 DEEPAK.P

Pacemaker TypesDual chamber pacemakers set the pace of two of your hearts
chambers and need two leadsDual chamber pacemakers are ideal if you have heart block
144 DEEPAK.P

Pacemaker TypesBiventricular pacemakers use three leads, one in the right
atrium (one of the top pumping chambers in your heart) and one in each of the ventricles (left and right)
145 DEEPAK.P

Pacemaker Types1. Pacing function2. Sensing function3. Capture functionAtrial pacing: stimulation of RT atrium produce spic on ECG
preceding P waveVentricle pacing :stimulation of RT or LT ventricle produce a
spic on ECG preceding QRS complexAVpacing:direct stimulation of RT atrium and either
ventricles
146 DEEPAK.P

Pacemaker TypesSensing :Ability of the cardiac pace maker to see intrinsic cardiac
activity when it occursDemand: pacing stimulation delivered only if the heart rate falls
below the preset limit.Fixed: no ability to sense. constantly delivers the preset stimulus at
preset rate.Triggered: delivers stimuli in response to (sensing )cardiac event.
147 DEEPAK.P
Pacemaker TypesCapture: Ability of the pacemaker to generate a
response from the heart (contraction) after electrical stimulation
According to pacing1.Permanent2.Temporary3.biventricular
148 DEEPAK.P







