
Professional Information and Order Forms
SOLARISF R E E D O M T O L I V E
TributeNightTM
M A N U F A C T U R E D B Y S O L A R I S

2 Visit us online at solarismed.com
How do I provide Solaris products to my patients?There are three ways you can provide Solaris products: 1. Solaris will provide therapists with the names of retailers in your area. 2. Open an account with net 30 terms with the approval of a credit application. 3. Open an account with credit card terms. We will keep your card number on file and take payment prior to processing the order.
How long does it take to manufacture and ship TributeNight™ therapeutic nightwear garments?We recommend that you tell your client it will take 5 - 7 days for manufacturing and an additional 3 - 5 days for shipping.
Does insurance cover TributeNight garments? What is the insurance billing code?Private health insurance policies that include durable medical equipment are currently paying for TributeNight garments. We always recommend checking with the insurance provider prior to ordering. Medicare does not have a payable code for our product line. However, we always encourage patients to submit the bill to Medicare with a copy of the Solaris packing slip and bill. Medicaid in many states will pay for the garments if you are a provider and complete the DME Prior Authorization Form.
Current insurance billing codes can be found on the Insurance Benefits Inquiry Template in this catalog.
How long does a TributeNight garment last?Solaris provides a one-year warranty on TributeNight garments. We recommend that most patients reorder every 12-18 months.
How long does an Outer Jacket or VCJ last?An Outer Jacket or VCJ should be replaced every 6 months. We suggest ordering a duplicate OJ or VCJ with your original order so they will last the life of the TributeNight garment.
What is the difference between Vertical and Chevron Channels?Select Vertical Channels for those patients who have intact lymph nodes and in which the therapist is directing the flow to the primary lymphatic system. This includes patients with venous considerations.
Select Chevron Channels for those patients who have impaired lymph nodes and/or if the therapist is directing the flow to the collateral lymph pathways.
Please explain the Garment Codes.UE is the designation used for all Upper Extremity garments; the first letter following the dash designates the distal start point of the garment as indicated on the measuring chart. For instance. “A” is the distal end of the third digit (middle finger), “C” is the wrist crease. The last letter corresponds with the proximal ending point of the garment. For instance, “E” is the elbow, “G” represents the axilla. Generally speaking you will only need to record the information for the garment style you have chosen for your client. When ordering a UE-CG garment we will need the length and girth measurements from the wrist (C) to the axilla (G).
LE is the designation for all Lower Extremity garments; the first letter following the dash designates the distal starting point of the garment. For instance, “A” is the distal end of the great toe and “B” is the ankle. The last letter corresponds with the proximal ending point of the garment. For instance, “D” on the measurement form is just below the patella and “G” is the groin. Generally speaking, you will only need to record the information for the garment style you have chosen for your client. When ordering a LE-AD garment we will need the length and girth measurements from the great toe (A) to the distal knee (D).
Remember all TributeNight garments are custom made for your individual client needs.
Frequently Asked Questions

3Questions? Call us at (855) 892-4140
2
3
4
5
6
7
8
10
12
14
16
18
FAQs
Contact Us
Policies and Warranty Information
Product Selection and Fitting & Tiny Tributes
Letter of Medical Necessity Template
Insurance Benefit Inquiry Template
TributeNight Upper Extremity Measuring & Order Form
TributeNight Torso Measuring & Order Form
TributeNight Lower Extremity Measuring & Order Form
TributeNight Head / Neck Measuring & Order Form
TributeNight Hand Order Forms
Alteration Form and Instructions
Customer Service
Table of Contents
Customer Service Representatives are available to assist you from 7 AM to 7 PM Central, Monday through Friday.
(855) 892-4140 (414) 892-4150 [email protected]
Solaris3880 W Wheelhouse RoadMilwaukee, WI 53208 USA
Tel:Fax:
Email:

4 Visit us online at solarismed.com
Wholesale Pricing Confidentiality PolicyWholesale invoices are confidential. Wholesale invoices may not be forwarded to any consumers, including insurance companies and support groups, who do not have state issued reseller’s licenses. Retail invoices will be provided to you for insurance documentation. Prices will reflect suggested retail pricing. Solaris reserves the right to refuse sales to any wholesale customer who violates pricing confidentiality.
Retailers/Distributor PolicySolaris does not offer exclusive territorial contracts. Consumers contacting Solaris will be offered retail provider names based on regional information. The website allows consumers to search by zip code. Retail information will be provided by proximity. Solaris maintains quality assurance files on all retailers, including: consumer compliments and concerns, sales volume statistics, and payment history.
Retail Pricing PolicySolaris does quote suggested retail pricing to insurance companies, consumers and regulatory agencies.
SureFitSM Guarantee for TributeNight GarmentsWithin two weeks of the ship date, Solaris will alter or remake any TributeNight garment that does not provide the patient with a therapeutic fit. Modifications requested after the original order will be billed the standard cost of the modification(s) plus shipping. To request a Return Authorization (RA) Number, please call Solaris at (855) 892-4140 or visit pro.solarismed.com.
One Free Alteration within the Warranty Period for Registered TributeNight GarmentsWithin one year of the ship date, Solaris will provide one free girth reduction alteration on registered TributeNight garments. To redeem a girth reduction alteration, contact Solaris for a Return Authorization (RA) Number and complete the TributeNight Alteration Form. Alteration Forms can be found in TributeNight professional catalogs, at pro.solarismed.com or by contacting Solaris directly at (855) 892-4140 [email protected].
One Year Workmanship and Materials Warranty for Registered TributeNight GarmentsWithin one year of the ship date, Solaris warrants all registered TributeNight garments against manufacturer defect. Solaris will repair or replace any garment found to be defective.
Using bleach, fabric softener, dryer sheets, or other additives will void the warranty. Heat over 130° F will damage the garment and void the warranty. Damage due to fingernail tears, animals, bodily fluids, or excessive pulling are not under warranty. Solaris does not warrant Outer Jackets (OJ) or Variable Compression Jackets (VCJ).
If you believe that a warranted garment is defective, contact Solaris for a Return Authorization (RA) Number. Solaris will examine the garment to determine if it is defective. Defective garments under warranty will be repaired or replaced.
Post-Warranty Alterations and RepairsSolaris will not perform any alteration or repairs on TributeNight garments that are not under warranty. We recommend that your clients purchase a new garment annually to ensure the greatest therapeutic results.
Returns and CancellationsSince TributeNight products are custom made, they cannot be returned nor refunded.
Policies and Warranty Information
5Questions? Call us at (855) 892-4140
Determining when to measure your clientExperienced therapists report that they use one or more of the following criteria to determine when to measure for a garment.
• When client reaches a plateau in girth reduction.• When developing the client’s home program.• When the client is unwilling or incapable of bandaging or following the bandaging protocol.• Clients with dominant fibrosis may be fitted in the early stages of treatment. Garments will need to be altered as girth decreases.
Choosing the right garment styleThe general rule of garment style selection is simple: Provide coverage if the area currently has swelling or has had a substantial history of swelling.
Evaluate your clients ROM, strength, cognition and stress levels. Select modifications that will adapt standard products to provide a garment that will become a natural part of the client’s daily routine. Call our customer service staff to discuss individual cases. We are here to assist you.
Ensuring a proper fit and client toleranceRefer to the User Guide included for donning and care instructions. Remember TributeNight garments are worn while sleeping – have the client don the garment then lie in supine position to check fit.
• The dispensing therapist or fitter should then check the garment to determine that the sizing is correct. The client should report that the garment feels “snug,” not tight, and compression decreases proximally. (Note: A sizing allowance at the elbow or the knee is standard, so that the client may sleep in a normal, relaxed position.)• The dispensing therapist or fitter should initially monitor the treated tissue to ensure skin integrity and to check for any unusual reactions, by having the client wear their new garment for one hour, then inspecting the limb. If client has a history of skin sensitivity, they should wash the garment twice, and then follow the above protocol.
Product Selection and Fitting
1.2.
1.2.
1.2.
Infant / Toddler(0 - 4 Years)
Child(5 - 8 Years)
Pre-Teen(9 - 13 Years)
Solaris believes it is important for the child and parent that we do not disassociate the affected limb. As such, we will produce either upper body pajama tops or lower body pajama bottoms for toddlers up to 4 years old. To assist us in this, please complete all measurement forms necessary to make this garment.
One garment per year free of chargeSecond garment at 25% of wholesale price
One garment per year at 25% of wholesale priceSecond garment at 50% of wholesale price
One garment per year at 50% of wholesale priceSecond garment at 75% of wholesale price
Solaris does not design Head & Neck garments for the Tiny Tribute program.
Solaris is proud to offer garments to our valued customers at no cost or at a reduced price for individuals 13 years of age or younger. A therapist or DME must provide us the measurements and include a copy of the physician’s prescription. Shipping and Handling charges do apply to these orders. If more than two garments are needed during one year from date of purchase, no discount will be given for the third garment.
Tiny Tribute™ Policies and Eligibility

6 Visit us online at solarismed.com
Date: Re: (Patient’s Name) DOB:
Subject: LMN - TributeNight™ Therapeutic Nightwear Garment(s)
To Whom It May Concern:
This letter is to indicate the medical necessity for TributeNight directional flow, custom-made, therapeutic, nightwear, garment(s) for the treatment of lymphedema and chronic swelling with indurate tissue for my patient, _______________. Impairment of the lymphatic system has significantly reduced the normal capacity of the lymphatic system to provide tissue drainage necessary to ensure tissue health, to support normal immune response, and maintain fluid balance of the circulatory system in the affected quadrant. _______________ has received restorative occupational therapy or physical therapy for this condition. However, it is now necessary to provide a garment that will maintain gains made in therapy and continue to provide therapeutic intervention in the home setting.
It is my opinion that the garment recommended is medically necessary for _____________. TributeNight garments are custom-made therapeutic garments, which are listed with the FDA. Patients with chronic swelling wear the garments nightly to address tissue fibrosis and facilitate interstitial fluid movement. All garments meet the Medicare guideline for durable medical equipment—they are dispensed only for medical conditions, warranted for one year, include one alteration as girth decreases, are machine washable/dryable and increase patient compliance to the necessary home program, however, there is not an assigned HCPCS code.
I anticipate that with successful use of this device we will be able to reduce the utilization of other health care services, including physical/occupational therapies, and the possible need for hospitalization for such complications as cellulitus.
Sincerely,
(Physician Signature)
(Physician’s Letterhead)
Letter of Medical Necessity (Template)

7Questions? Call us at (855) 892-4140
Insurance Co. Name ________________________________________________ Date_____________ Time_______________
Insurance Co. Representative’s Name ______________________________________________________________________
I am calling to check the durable medical equipment benefits for your insured ___________________________
Policy # ______________________________________________________ Group #_____________________________________
His/Her diagnosis CPT code is: 457.0 Post mastectomies Lymphedema Syndrome 757.0 Hereditary edema of legs 457.1 Lymphedema – Primary or Secondary, (not post mastectomy Lymphedema Syndrome) 608.86 Edema of Male Genital Organs
Does the policy include coverage for Medical Equipment? Yes No (if No, end call)If Yes, the product(s) needed is _________________________________________________________ A TributeNight™ garment is a custom-made therapeutic garment that is listed with the FDA. Patients with chronic swelling wear the garments nightly to address tissue fibrosis and facilitate interstitial fluid movement. All garments meet the Medicare guideline for durable medical equipment-dispensed for medical conditions only, the garment has a one year warranty, one alteration is provided during the warranty period as girth decreases, all garments are machine washable and dryable, and increase patient compliance to their home program, however, there is no assigned code.
Is my company Out-of-Network? Yes No In-Network? Yes NoWhat is the annual deductible? ________________ How much of the deductible that has been met? _______How much is the co-pay? ______________________Is pre-authorization recommended/required? Yes No Is a prescription recommended/required? Yes No Do you require a letter of medical necessity? Yes No Do you require therapy notes? Yes No
Is this Which of the following HCPCS Codes do you prefer? Code Capped? Anticipated Benefits
A6542 Gradient Compression Stocking, Custom Made Yes No
A6543 Gradient Compression Stocking, Lymphedema Yes No
S8422 Gradient Compression Stocking, not otherwise specified Yes No
E1399 Lower Extremity Orthosis, not otherwise specified Yes No
A4465 Upper Limb Orthosis, not otherwise specified Yes No
Where do we mail the claim to:Company Name ____________________________________________________________________________ Address __________________________________________________________________________________ City/State/Zip ______________________________________________________________________________ Direct phone number and/or extension __________________________________________________________
Could you provide your name and an employee ID # if you use them:
Name _____________________________________________________ ID # _______________________
Insurance Benefits Inquiry (Template)

8
Positioning Your Client When Measuringfor Arm Garments
Measuring Guidelines for TributeNight Arm Garments
TributeNight garments are most commonly worn while the client is sleeping, therefore, take the measurements with the client in supine position, if possible. Indicate on the order form which measuring position you chose.
Measuring Lengths:
With the client in supine position, the arm lying next to the trunk, measure the length of the limb. Use a water based marker to indicate the length reference point on the skin according to the following suggested procedure:
A to B length: Measure with palm up, from the digit crease (MCP) to the fingertip of the third digit (middle finger).
B to C length: With the palm up, position the tape measure with zero at the wrist crease; measure the length to the base of the third digit (MCP of middle finger).
C to D length: With the tape measure placed with zero (0) at the wrist crease, measure the length to the D point (typically the largest girth point of the forearm). Using a water based marker dot this point of the arm.
C to E length: Continue to measure from the wrist C to the medial elbow crease E with the elbow in slight flexion (10° to 20°). Using a water based marker dot this point of the arm.
C to F length: Measure from the wrist to the F point (typically the largest girth point of the upper arm). Dot this point with a water based marker.
C to G length: Measure from the wrist to the axilla. (Place a pencil or dowel in the armpit as a visual guide.) Abducting the arm during this length measure ment will result in a garment that is too long. Measuring with shoulder flexion will result in a garment that is too short.
G to H length: The standard lateral shoulder cap is 10cm longer than the medial length. To customize this length and for I length garments, measure from lateral G to AC joint.
H to I length: Measure from AC joint to high point shoulder (HPS) or base of neck for I length garments.
Measuring Circumference: Note: Record all circumference measure ments on the left side of the measuring chart on the Arm Order Form.
B: Measure the circumference of the palm across the MCP’s with the hand in NEUTRAL posture, simulating the posture of the hand when a person is sleeping.
C: Measure the circumference of the wrist over the styloids.
D: Measure the circumference of the forearm where you have dotted the skin.
E: Measure the girth with the elbow in slight flexion (10° to 20°). Use the medial elbow crease and mid-olecranon process as your reference points.
F: Measure the circumference of the upper arm at the marker dot. If the arm tends to be fleshy, you have the option of recording the girth as a range. Record the girth measurement with the tape pulled taut and the girth measurement with the tape measure laid on the tissue (i.e. 36 cm to 39 cm).
G: Measure the girth at the level of the axilla, STRAIGHT ACROSS. Be careful not to angle the tape measure proximally on the lateral side of the arm.
H: Measure diagonal girth from anterior AC around the torso to posterior AC.
Customized Modifications forTributeNight Arm Garments
MO-ZP: Zipper is placed from the thenar eminence to mid-bicep The garment is closed at the proximal and distal end to make it easier for the client to zip the garment closed.MO-DS: Digit Spacers similar to the ones used in TributeNight glove units will be added to the UE-AG garments. Complete both the Hand Order Form and the Arm Order Form when ordering this modification.MO-PL: Pull-up Loops may be added to the volar surface of the arm unit. MO-AP / MO-VC: Use the Comments Section to indicate the starting and ending points of the Velcro modifications.UE-OJ: An Outer Jacket will be custom made to cover the garment, applying additional compression. An option of snap or Velcro fastener is available.UE-VCJ: Variable Compression Jackets allows therapist to adjust compression laterally. Zipper opening on medial aspect allows ease of use.

9
SHIP TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:E-Mail for Shipping Notification:
BILL TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
Account #______________________________
PO #____________________________________
CC #___________________________________ Exp____ /_____
If we have a question, whom should we contact?
Contact Phone #:
Therapist Name:
Client Name or Order Reference #:
DX 457.1 457.0 Other ________________________
Age_______ Height_________ Weight ________________
For Internal Usage:
Comments: _____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
TributeNight Arm Order FormFax completed order form to (414) 892-4150.Solaris will fax a quote confirming your order and cost. Questions? Call Customer Service at (855) 892-4140.
Please Measure in Centimeters C = Circumference
HC - Diagonal Strap Length
GC
FC
EC
DC
CC
BC
BL
CL
DL
EL
FL
GL
HL
ILHC
G
F
E
D
C
B
AL
MCP To DistalEnd of Garment
Wrist To MCP
L = Length
Zero
Garment Code: UE-
Outer Jacket
Variable Compression Jacket
Zipper (on TributeNight only)
Velcro
Digit Spacers (include hand order form)
Pull Up Loops (on TributeNight only)
Easy Slide Application Aid
Priority Production Fee ($40)
QTY UNIT PRICE
TOTAL:
Shipping Bus. GRD Res. GRD 2nd Day Overnight
MO-AP MO-VC
Fabric ColorTributeNight: Black Blue Maroon Pink Purple Teal
Outer Jacket: Black Blue Maroon Pink Purple Teal
SnapFastener: Velcro

10
Positioning Your Client When Measuringfor Torso Garments
TributeNight garments are most commonly worn while the client is sleeping, therefore we usually recommend that the measurements be taken with the client in a supine position; however, we understand that it is much more difficult to measure the trunk in supine. Please indicate on the order form the position that measurements were taken (standing or supine) so that we may adjust accordingly.
Measuring Guide forTributeNight Lower Torso Garments
Measuring Lengths:
For Solaris, the natural waist line is designated as zero on the measuring diagram. Length measurements are taken along the side. Use a water based marker to indicate the length reference point on the skin according to the following suggested procedure:
I to J length: We recommend that TributeNight Lower Torso garments extend above the Transverse Plane or watershed. Position the tape measure with zero (0) at the waist (I), along the Coronal Plane. Measure up the torso 5cm. Dot this location with the water based marker.
I to H length: On the lateral aspect, position the tape measure with zero (0) at the waist, measure to approximately the level of the iliac crests or to the largest girth point of the hips. Dot this location with the water based marker.
I to G length: Continue to measure from the waist to the groin level as indicated on the diagram.
I to F length: Continue to measure from the waist to the level on the mid-thigh.
Straddle Length:
B: Mid-crotch reference point for straddle measurements.
Anterior Straddle Length (AS): Measure from the mid-crotch (B) to the anterior natural waist.
Posterior Straddle Length (PS): Measure from the mid-crotch (B) to the posterior natural waist.
Measuring Circumferences:
Measure and record girth circumferences for points J, I, and H on the left side of the Torso Order form. For clients with soft tissue, circumferences may be recorded as a range (i.e. waist may be recorded as 98-101 cm).
RGC/LGC: Measure girth of right leg and left leg at groin level. Record the girth.
RFC/LFC: Measure girth of right leg and left leg at mid-thigh. Record the girth.
Measuring Guidelines for TributeNight Torso Garments
Measuring Guide forTributeNight Upper Torso Garments
Measuring Lengths:
For TributeNight garments, the natural waistline is designated as zero (0) on the diagram. Length measurements are taken on the Midsagittal or Median Plane. Use a water based marker to indicate the length reference point on the skin according to the following suggested procedure:
I to H length: We recommend that Upper Torso garments extend below the Transverse Plane or watershed at the waist approximately five (5) centimeters. For most clients this point will be just above the Iliac Crest. Dot with water based marker.
I to J length: Position the tape measure with zero (0) at the waist, at the midline or Midsagittal Plane measure the length to just below the breast. Dot this location with the water based marker. Record on order form. (Disregard line location on order form.)
I to K length: Continue to measure the length to the mid-breast at the level of the nipples. Dot with water based marker.
I to L length: Measure the length to the L point (at the level of the axilla).
M length: Measure AC joint to high point shoulder (HPS) or base of neck for garments with shoulders.
N Shoulder Straddle length: With the client holding the tape measure at zero (0) measure from the midline anterior waist over the shoulder to the midline posterior waist. Record the length.
O length: Measure AC joint under axilla to AC joint for arm opening length.
Measuring Circumferences:
H: Measure the circumference of the hips. If the hips tend to be fleshy, record the girth as a range of measurements. Document the girth with the measuring tape laid on the tissue and the girth with the measuring tape taunt (ex. 98-101 cm).
I: Measure the circumference at the natural waist. If needed use girth range.
J: Measure the circumference just underneath the breast. Lift breast if necessary. (JC line appears lower on the diagram.)
K: Measure at the level indicated on the diagram. For unilateral mastectomy, measure each side independently from anterior midline to spine. Use comment section to record unilateral measurements.
L: Record circumference above breasts at the level of the axilla. Indicate breast tissue turgor on order form.

11
Breast Tissue Turgor: Firm Moderate Drape Lax(For Upper Torso Garments)
HC
IC
JC
KC
LC
OL
NL
PSASRGCLGC
LFC RFCB
Arm Hole
Shoulder Straddle
ML
KL
JL
LL
HL
GL
FL
=
=
=
=
=
I (0)
Garment Code: TT-
Zipper
Snap Tape Closure
Priority Production Fee ($40)
QTY UNIT PRICE
TOTAL:
TributeNight Torso Order Form
SHIP TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:E-Mail for Shipping Notification:
BILL TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
Account #______________________________
PO #____________________________________
CC #___________________________________ Exp____ /_____
If we have a question, whom should we contact?
Contact Phone #:
Therapist Name:
Client Name or Order Reference #:
DX 457.1 457.0 Other ________________________
Age_______ Height_________ Weight ________________
For Internal Usage:
Comments: _____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
Fax completed order form to (414) 892-4150.Solaris will fax a quote confirming your order and cost. Questions? Call Customer Service at (855) 892-4140.
Please Measure in Centimeters C = Circumference L = Length
Shipping Bus. GRD Res. GRD 2nd Day Overnight
Fabric ColorTributeNight: Black Blue Maroon Pink Purple Teal

12
Positioning Your Client When Measuringfor Leg Garments
TributeNight garments are most commonly worn while the client is sleeping, therefore, take the measurements with the client in supine position or standing.
Measuring Lengths:
Please record all length measurements on the right side of the leg diagram on the Leg Order Form.
With the client in supine position, the legs adducted in a natural relaxed posture, measure the length segments of the limb. Use a water based marker to indicate the length reference point on the lateral leg following this suggested procedure:
A length: With the foot in neutral, position the tape measure with zero (0) at the heel. Measure the length to the tip of the great toe. (If you want the garment to end at the metatarsals measure to that point.) Record the length of the foot on the lower left side of the leg diagram.
B length: With the tape measure placed with zero (0) at the heel, measure the length to the B point on the lateral side of the leg (the largest girth point of the ankle).
C length: Measure the length to the C point (typically the largest girth point of the calf).
D length: Measure from the heel to the D point, just below the patella.
E length: Measure from the heel to mid-patella.
F length: Continue to measure from the heel to F (the largest girth point of the thigh). Dot this point with a water based marker.
LG length/lateral leg length: Measure from the heel to the G point. Place a pencil or dowel in the groin as a visual guide if needed. Abducting the legs will result in a garment that is too short.
MG length: Measure the medial inseam length from the medial heel to the medial G length (groin). Note this length on the order form.
H length: Measure from the heel to the Iliac Crest. Record this length measurement on the right side of the leg diagram.
I length: For garments ending at points I or J continue to measure length from the heel to the natural waistline. Record this length.
J Length: To cross the transverse plane or watershed add an additional five (5) cm to the overall length or customize length to meet your client’s need.
Anterior Straddle Length (AS): Measure from the anterior natural waist to the mid-crotch (B).
Posterior Straddle Length (PS): Measure from the posterior natural waist to the mid-crotch (B).
Measuring Guidelines for TributeNight Leg Units
Measuring Circumference:Please record all circumference measurements on the left side of the leg diagram.
A: Measure the circumference of the foot across the MTPs with the foot in NEUTRAL posture, simulating the posture when a person is sleeping.
B: Measure the circumference of the ankle where you dotted the skin. When skin folds are present measure the largest girth NOT the circumference under the skin fold.
Y: Position the tape measure to provide the angular ankle to heel circumference.
C: Measure the circumference of the calf where you have dotted the skin
D: Measure the girth just below the patella.
E: Measure the girth at the mid-patella.
F: Measure the circumference of the upper leg at the marker dot. If the leg tends to be fleshy a slight snugging of measuring tape is recommended to decrease the girth circumference. If you are concerned about this measurement, record the girth as a range – with the tape pulled taut and laid on the tissue (i.e. 76cm to 84cm).
G: Measure the girth at the level of the groin, STRAIGHT ACROSS. Be careful not to angle the tape measure proximally on the lateral side of the thigh.
H: Measure the circumference across the hips (usually across the Iliac Crest, but you can use the largest point also).
I: Circumferentially measure the natural waistline. If you are concerned about this measurement, record the girth as a range as discussed at F.
J: Measure the circumference five (5) cm above the natural waistline or where you’ve determined to end the garment.
Customized Modifications forTributeNight Leg Garments
MO-ZP: Zipper may be custom placed. Please indicate the starting and ending points in the Comments Section.MO-PL: Pull-up Loops may be added to all leg units.MO-SO: Non-skid pads may be added to the sole of a TributeNight garment, or on an Outer Jacket or VCJ when ordering a garment with a jacket.MO-AP / MO-VC: Use the Comments Section to indicate the starting and ending points of the Velcro modifications.LE-OJ: An Outer Jacket will be custom made to cover the garment. An option of snap or Velcro fastener is available.LE-VCJ: Variable Compression Jackets allows therapist to adjust compression laterally. Zipper opening on medial aspect allows ease of use.

13
Garment Code: LE-
Outer Jacket
Variable Compression Jacket
Zipper (on TributeNight only)
Velcro
Non-skid Pads
Pull Up Loops (on TributeNight only)
Easy Slide Application Aid
Priority Production Fee ($40)
Vertical Chevron
QTY UNIT PRICE
TOTAL:
AC
BC
CC
DC
EC
FC
GC
HC
ASL
IC
IL
AL
JC
PSL
MGL LGL
FL
EL
DL
CL
BL
Y
HL
JL
TributeNight Leg Order Form
SHIP TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:E-Mail for Shipping Notification:
BILL TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
Account #______________________________
PO #____________________________________
CC #___________________________________ Exp____ /_____
If we have a question, whom should we contact?
Contact Phone #:
Therapist Name:
Client Name or Order Reference #:
DX 457.1 457.0 Other ________________________
Age_______ Height_________ Weight ________________
For Internal Usage:
Comments: _____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
Fax completed order form to (414) 892-4150.Solaris will fax a quote confirming your order and cost. Questions? Call Customer Service at (855) 892-4140.
Please Measure in Centimeters C = Circumference L = Length
Shipping Bus. GRD Res. GRD 2nd Day Overnight
MO-AP MO-VC
SnapFastener: Velcro
TributeNight OJ
Fabric ColorTributeNight: Black Blue Maroon Pink Purple Teal
Outer Jacket: Black Blue Maroon Pink Purple Teal

14
Measuring Guidelinesfor TributeNight Facial Units
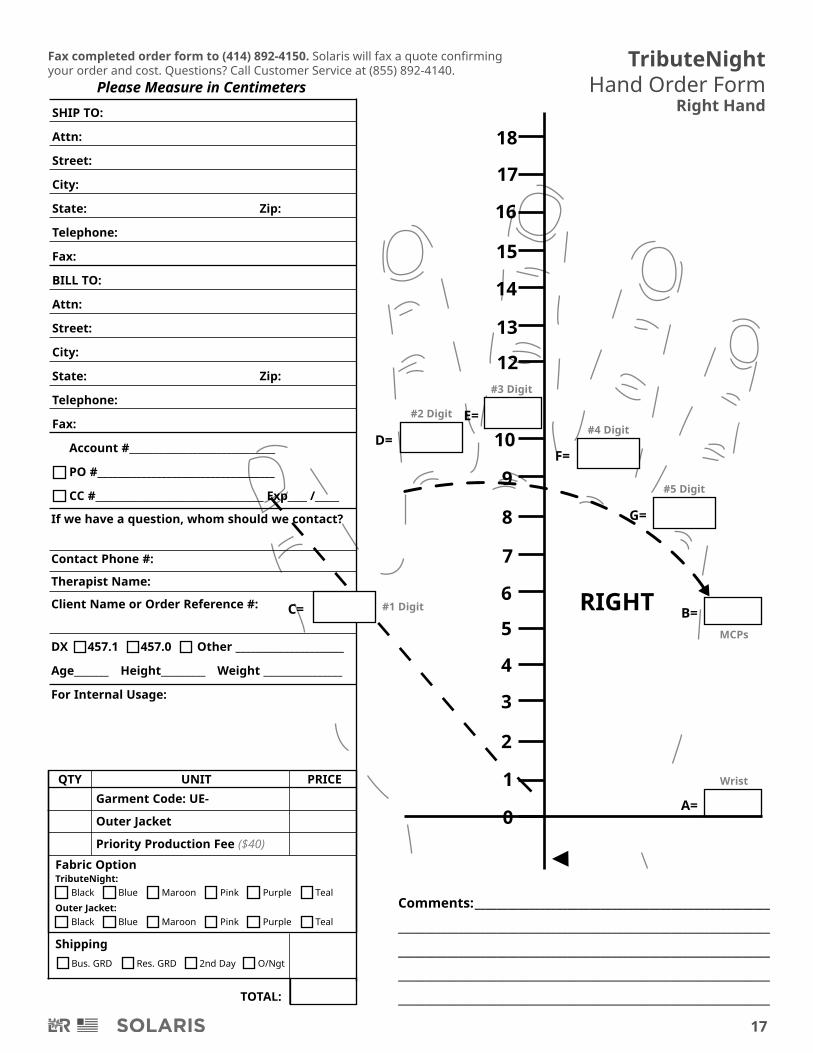
Measuring Guidelinesfor TributeNight Hand Units
Positioning Your Client When Measuringfor Facial Garments
TributeNight garments are most commonly worn while the client is sleeping, however, clients with facial swelling may be measured in a seated posture.
Measuring:
Please record the needed measurements in the designated areas on the Facial Order Form.
A: Measure the length from one ear tip to the other.
B: Measure the head circumference at the temple line or
C: Measure the distance from the outside crease of the
D: Measure the length of the nose.
E: Measure the length at the midline from the nose to the
F: Measure the length at the midline from the lower lip to
G: Measure the length from the sterno-clavicalur notch to
H: Measure from the right ear lobe to the right nostril.
I: Measure from the left ear lobe to the left nostril.
J: Measure the distance from the right TMJ to the chin.
K: Measure the distance from the left TMJ to the chin.
L: Measure the length from the right ear lobe to the HPS
M: Measure the length from the left ear lobe to the HPS.
N: Measure the neck circumference.
Positioning Your Client When Measuringfor Hand Garments
The Hand Order Forms are Right / Left specific.
Position your client’s hand on a copy of the order form. Align the wrist crease to approximate the Center Wrist Line on the copy of the order form. Trace around the client’s hand with a pen or pencil, keeping the tip of the pen/pencil close to the digits and hand. Have the client remove their hand from the copy of the Hand Order Form.
Measuring Circumferences:
Please record the needed measurements in the designated areas on the specific Hand Order Form.
A: Measure the wrist circumference over the styloid.
B: Measure the palm circumference across the metacarpal
C: Measure the proximal circumference of the thumb.
D: Measure the proximal circumference of the index
E: Measure the proximal circumference of the middle
F: Measure the proximal circumference of the ring finger.
G: Measure the proximal circumference of the small finger.
right eye to the outside crease of the left eye.
upper lip.
the chin.
the chin. Follow the contour with chin in relaxed posture.
(High Point of Shoulder).
heads.
finger.
finger.
largest part.

15
If we have a question, whom should we contact?
Contact Phone #:
Therapist Name:
Client Name or Order Reference #:
DX 457.1 457.0 Other ________________________
Age_______ Height_________ Weight ________________
For Internal Usage:
A
B
C
H I
D
F
E
GN
Denote with Hash Marks / / / / Areas of Scarring or Fibrosis on Diagram.
A=
B=
C=
D=
E=
F=
G=
H=
I=
J=
K=
L=
M=
N=
Garment Code: FN-
Garment Code: FN-
Lip Bridge
Trach Modification (no additional charge)
Priority Production Fee ($40)
QTY UNIT PRICE
N/A
N/A
MLJ K
TOTAL:
TributeNight Facial Order Form
SHIP TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:E-Mail for Shipping Notification:
BILL TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
Account #______________________________
PO #____________________________________
CC #___________________________________ Exp____ /_____
Comments: _____________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
___________________________________________________________________________________________________________________________________
Fax completed order form to (414) 892-4150.Solaris will fax a quote confirming your order and cost. Questions? Call Customer Service at (855) 892-4140.
Please Measure in Centimeters
Shipping Bus. GRD Res. GRD 2nd Day Overnight

16
Fax completed order form to (414) 892-4150. Solaris will fax a quote confirming your order and cost. Questions? Call Customer Service at (855) 892-4140.
SHIP TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
BILL TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
Account #______________________________
PO #____________________________________
CC #___________________________________ Exp____ /_____
LEFT
18
17
16
15
14
13
12
10
9
8
7
6
5
4
3
2
1
0
TributeNight Hand Order FormLeft Hand
If we have a question, whom should we contact?
Contact Phone #:
Therapist Name: Client Name or Order Reference #:
DX 457.1 457.0 Other ________ _________________
Age_______ Height_________ Weight ___________________
For Internal Usage:
A=
D=
E=
F=
G=
C=B=
Please Measure in Centimeters
TOTAL:
Garment Code: UE-
Outer Jacket
Priority Production Fee ($40)
QTY UNIT PRICEWrist
MCPs
#5 Digit
#4 Digit
#3 Digit
#2 Digit
#1 Digit
Comments: ______________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Fabric Option
Shipping Bus. GRD Res. GRD 2nd Day O/Ngt
TributeNight: Black Blue Maroon Pink Purple Teal
Outer Jacket: Black Blue Maroon Pink Purple Teal
17
TOTAL:
Garment Code: UE-
Outer Jacket
Priority Production Fee ($40)
QTY UNIT PRICE
Fabric Option
Shipping
18
RIGHT
17
16
15
14
13
12
10
9
8
7
6
5
4
3
2
Fax completed order form to (414) 892-4150. Solaris will fax a quote confirming your order and cost. Questions? Call Customer Service at (855) 892-4140.
TributeNight Hand Order Form
Right Hand
1
0A=
D=
E=
F=
G=
C= B=
Comments: ______________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Wrist
MCPs
#5 Digit
#4 Digit
#3 Digit
#2 Digit
#1 Digit
If we have a question, whom should we contact?
Contact Phone #:
Therapist Name:
Client Name or Order Reference #:
DX 457.1 457.0 Other ______________________
Age_______ Height_________ Weight ________________
For Internal Usage:
SHIP TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
BILL TO:
Attn:
Street:
City:
State: Zip:
Telephone:
Fax:
Account #______________________________
PO #____________________________________
CC #___________________________________ Exp____ /_____
Please Measure in Centimeters
Bus. GRD Res. GRD 2nd Day O/Ngt
TributeNight: Black Blue Maroon Pink Purple Teal
Outer Jacket: Black Blue Maroon Pink Purple Teal

Alteration Requirements & Important Considerations:1. Call Solaris at (855) 892-4140 prior to shipping to obtain an RA# (Return Authorization Number).2. Ensure that the garment has been freshly laundered. We will return garments for washing if they arrive soiled,
or contract out a laundering service and assess a $50.00 service fee, which is to be paid prior to alterations.3. Complete the alteration form and attach any photos or additional paperwork with the returned garment.4. TributeNight garments are altered only during the one year warranty period.5. Use of bleach or fabric softener will void the warranty as stated in professional literature and in the
TributeNight Usage Guidelines for the customer.6. Tears or holes are not included in the warranty.7. Always include a new measurement form.
TributeNight Alterations InstructionsMail alterations to: Solaris, 3880 W Wheelhouse Road, Milwaukee, WI 53208
Completing the Alteration Form:1. An alteration form must be included with the returning garment.2. Call Solaris at (855) 892-4140 to obtain a Return Authorization Code. Write this number on the form.3. Product ID number is found on the TributeNight label in the seam of the garment.4. Complete the requested information.5. Please keep in mind that our alterations staff are not medical personnel, please use lay terms if possible.
Marking the Garment (You will need a China Marker or Wax Pencil and Large Binder Clips):
• Have your client don their TributeNight garment, then lie down in a supine position.
• To shorten the length: • With the china marker, mark the length all the way around the garment where you would like the
• To reduce the girth: • Starting at the distal end of the garment, gently pinch along the lateral side of the garment, apply the
• Continue to work proximally until you have clipped the full length of the garment.
• If you are unable to get a snug fit with the lateral marking, mark the medial side of the garment
garment to be cut off.
binder clip to the excess material.
in the same manner. Ask the patient to move in the clipped garment to ensure a snug, not tight, fit.
marker, mark the edge of the binder clip on the top and bottom of the garment. (You may mail the garment with the binder clips attached, or remove the binder clips making sure your marks are visible on both sides of the garment)
• Leave the binder clips in place, using a china
Adding Modifications:If a TributeNight has been ordered without a modification and you want to add one, complete a new order form indicating the modification and mail the form back with the garment. You will be charged for the modification and shipping. If your company uses purchase orders, you will need a new number for the modification.

First time alterations are returned to the therapist/fitter by ground at no charge: Please provide ship to information:
Date Received:_________ By: _________
Date Repaired:_________ By: _________
Date Inspected:________ By: _________
Date Shipped:_________ By: _________
Garment(s) being returned:
Reason for the return:
Please provide, in detail, the problems you have with the garment(s) and changes you would like us to perform
(Please do not use short-hand or medical symbols): _______________________________________________________________________________
_______________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________________
Return Authorization Number: _______________________
Product ID Number: ____________________________________
Clinic Name: _____________________________________________
Therapist/Fitter Name: _________________________________
Client Name: ____________________________________________
Whom should we contact if we have questions?
__________________________________________________________
Phone # of Contact: ___________________________________
TributeNight Alterations FormMail alterations to: Solaris, 3880 W Wheelhouse Road, Milwaukee, WI 53208
Check List: Do you have a Return Authorization number? Is the garment clean and recently laundered? Have you included an order form with the new measurements?
Important Considerations:
1. TributeNight garments are altered only during the one year warranty period.2. Use of bleach or fabric softener will void the warranty as stated in professional literature and in the
TributeNight Usage Guidelines for the customer. Tears or holes are not included in the warranty.3. Please do not ship back the mesh bag.
For Internal Use
Clinic Name:____________________________________________________
Attention: ____________________________________________________
Street: _________________________________________________________
City:___________________________________________________________
State:________________________ Zip: ______________________________
Is the garment under warranty? Have you registered the warranty card?
TributeNight Outer Jacket VCJ Other
Shorten Girth Reduction Garment Style Modifications Wear/Tear Other
Garment(s) Received:Notes: _________________________________________
_______________________________________________
_______________________________________________
_______________________________________________
_______________________________________________
_______________________________________________
_______________________________________________
_______________________________________________
Mesh Bag TributeNight Outer Jacket VCJ

REV 02/16
Solaris3880 W Wheelhouse RoadMilwaukee, WI 53208 USA
(855) 892-4140 (414) 892-4150 [email protected] solarismed.com
/solarisinc
@solarisinc
/solarisinc
Tel:Fax:
Email:Web:







