
MOVING TOWARDS TB ELIMINATION: EXPERIENCE AND LESSON LEARNED
THROUGH ERS ENGAGEMENT IN EUROPE
G. B. MiglioriWHO Collaborating Centre for TB and Lung Disease,
Fondazione S. Maugeri, Care and Research Institute
Tradate, Italy

Faculty disclosure
NO COI !!!

Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.
Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.

Sotgiu et al, NEJM 2013
6
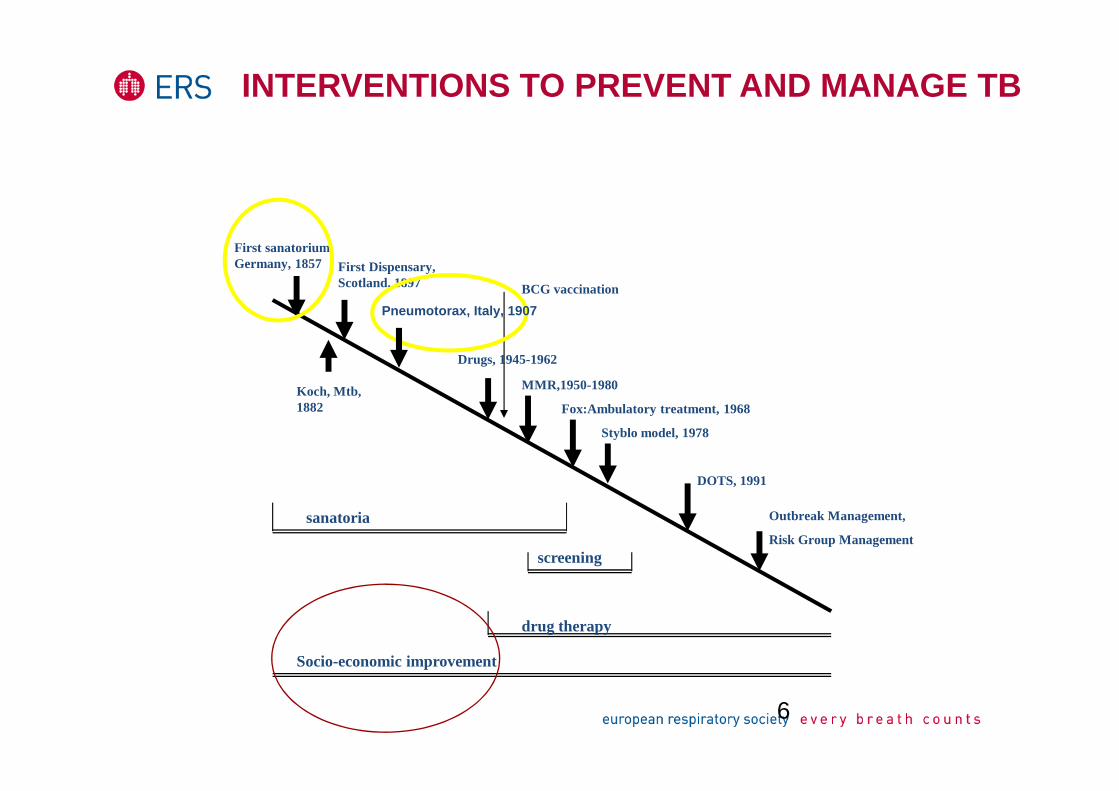
INTERVENTIONS TO PREVENT AND MANAGE TB
First sanatorium Germany, 1857 First Dispensary,
Scotland, 1897
Koch, Mtb,1882
Drugs, 1945-1962
MMR,1950-1980
Fox:Ambulatory treatment, 1968
Styblo model, 1978
DOTS, 1991
sanatoria Outbreak Management,
Risk Group Managementscreening
BCG vaccination
drug therapy
Socio-economic improvement
Pneumotorax, Italy, 1907

7
DOTS
• Government commitment
• Case detection by SS microscopy among self-reporting symptomatic patients
• Standardised short-course chemotherapy for at least all confirmed smear positive cases, DOT during the intensive phase for all new SS+ cases, continuation phase of RMP-containing regimens and the whole re-treatment regimen.
• A regular, uninterrupted supply of all essential anti-TB drugs
• A standardised R&R system allowing assessment of case-finding and treatment results and of NTP performances
Int J Tuberc Lung Dis 2001; 5(3):213-215

STOP TB STRATEGY (WHO)
1. Pursue high-quality DOTS expansion and enhancement
• Political commitment with increased and sustained financing• Case detection through quality-assured bacteriology• Standardised treatment, with supervision and patient support• An effective drug supply and management system• Monitoring & evaluation system, and impact measurement
2 Address TB/HIV, MDR-TB and other challenges
3. Contribute to health system strengthening
4. Engage all care providers
5. Empower people with TB and communities
6. Enable and promote research
Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.


Core additional interventions to pursueelimination
• 1) Ensuring early detection of TB patients and their treatment until cure and preventing avoidable death from TB
• 2) Reducing the incidence of infection by risk group management and prevention of transmission of infection in institutional settings
• 3) Reducing the prevalence of tuberculosis infection through outbreak management and provision of preventive therapy for specified groups and individuals

Core additional interventions to pursueelimination
• 1) Ensuring early detection of TB patients and their treatment until cure and preventing avoidable death from TB (C);
• 2) Reducing the incidence of infection by risk group management and prevention of transmission of infection in institutional settings (C,E)
• 3) Reducing the prevalence of tuberculosis infection through outbreak management and provision of preventive therapy for specified groups and individuals (E)

Elimination programmaticpre-requirements (1)
• Government and private-sector commitment towards elimination
• National schemes for TB control and elimination • National TB policy • National TB network • Legal framework • Human resources development and health
education • Research • International and European collaboration
Elimination programmaticpre-requirements (2)
• Case detection through case-finding among symptomatic individuals presenting to health services and
• Active case-finding in special groups • Standard approach to treatment of disease and
TB infection• Accessibility to TB diagnostic and treatment
services• Surveillance and treatment outcome monitoring
for TB diseases and TB infection

Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.

WORLD HEALTH ASSEMBLY APPROVES POST-2015 GLOBAL TB STRATEGY AND TARGETS –
WHA TB RESOLUTION

ZERO
TB DEATHS
A WORLD FREE OF TB
Vision
ZERO
TB CASES
ZERO
TB SUFFERING
GLOBAL TB
PROGRAMME

Goal and Targets
Target 1
95% reduction in TB deaths (compared
with 2015)
Target 2
<10/100 000 TB incidence rate
2035
GOAL: End the Global TB Epidemic
GLOBAL TB
PROGRAMME

TARGETS
• 35% reduction in TB deaths
• <85/100 000 TB incidence rate
• No affected families with catastrophic costs due to TB
TARGETS
• 75% reduction in TB deaths
• <55/100 000 TB incidence rate
• No affected families with catastrophic costs due to TB
TARGETS
• 90% reduction in TB deaths
• <20/100 000 TB incidence rate
• No affected families with catastrophic costs due to TB
GOAL
• 95% reduction
in TB deaths
• <10/100 000 TB
incidence rate
• No affected
families with
catastrophic
costs due to TB
20352020 20302025
Getting there: Milestones
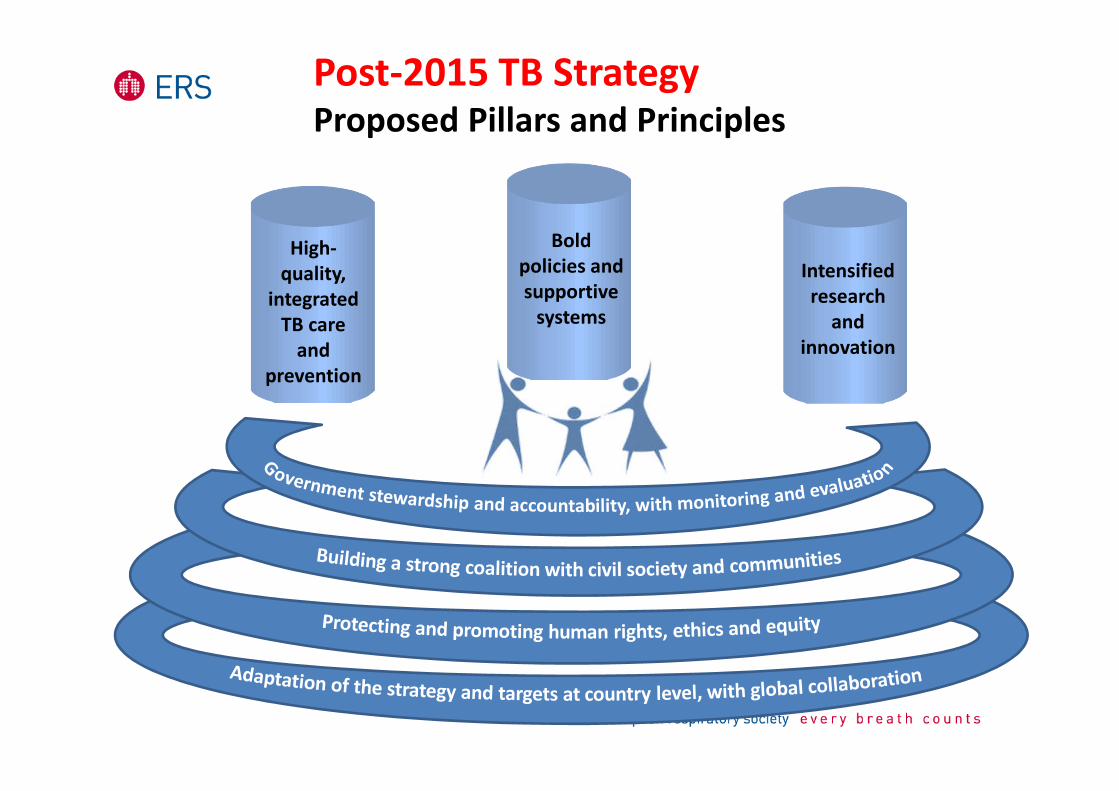
High-
quality,
integrated
TB care
and
prevention
Bold
policies and
supportive
systems
Intensified
research
and
innovation
Post-2015 TB StrategyProposed Pillars and Principles

POST-2015 TB STRATEGY: PILLAR 1
Treatment of all people with TB including drug-resistant TB, with patient-centered support
3
Preventive treatment of people at high-risk and
vaccination for TB4
Early diagnosis of TB including universal drug susceptibility testing; systematic
screening of contacts and high-risk groups
1 2
Collaborative TB/HIV activities and management of co-morbidities
High-
quality,
integrated
TB care
and
prevention
GLOBAL TB
PROGRAMME

Integrated, patient-centered TB Care and
Prevention
Early diagnosis of TB including universal drug-susceptibility testing ; systematic screening of contacts and high-risk groups
Treatment of all people with TB including drug -resistant TB; and patient support
Collaborative TB/HIV activities and management of co-morbidities
Preventive treatment for persons at high-risk; and vaccination against tuberculosis
Bold policies and supportive systems
Political commitment with adequate resources for TB care and prevention
Engagement of communities , civil society organizations, and all public and private care providers
Universal health coverage policy; and regulatory framework for case notification, vital registration, quality and rational use of medicines, and infection control
Social protection, poverty alleviation, and actions on other determinants of TB
Intensified Research and Innovation
Discovery, development and rapid uptake of new tools, interventions and strategies
Research to optimize implementation and impact, and promote innovations
Targets: 95% reduction in deaths and 90% reduction in
incidence (< 10 cases / 100,000 population) by 2035
Post-2015 Global TB Strategy: Pillars
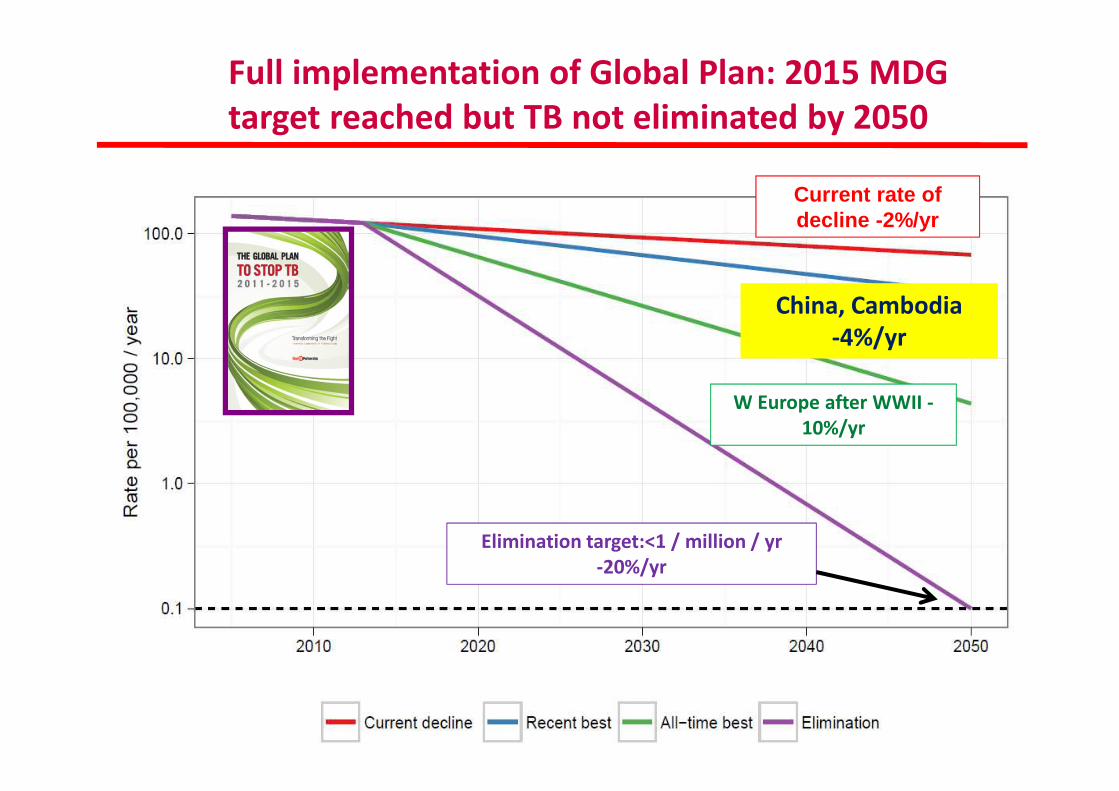
Full implementation of Global Plan: 2015 MDG
target reached but TB not eliminated by 2050
Current rate of decline -2%/yr
W Europe after WWII -
10%/yr
China, Cambodia
-4%/yr
Elimination target:<1 / million / yr
-20%/yr
China, Cambodia
-4%/yr
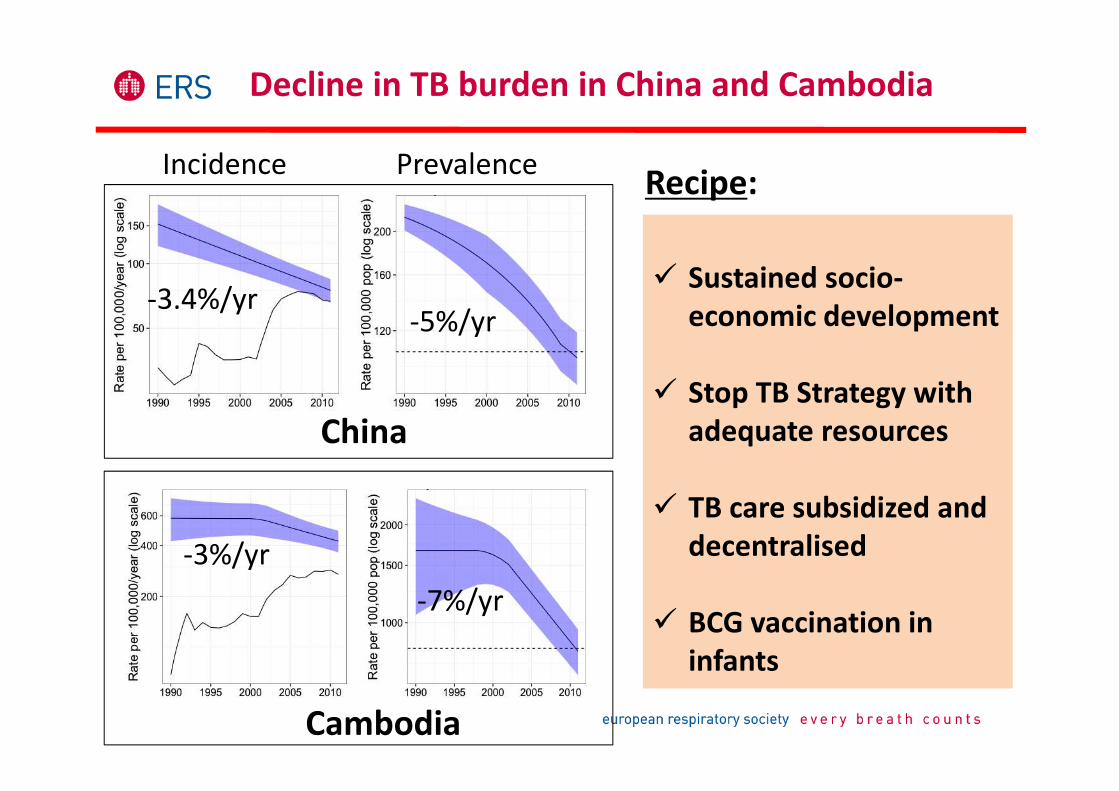
-3.4%/yr-5%/yr
Incidence Prevalence
-3%/yr
-7%/yr
China
Cambodia
� Sustained socio-
economic development
� Stop TB Strategy with
adequate resources
� TB care subsidized and
decentralised
� BCG vaccination in
infants
Decline in TB burden in China and Cambodia
Recipe:

Full implementation of Global Plan: 2015 MDG
target reached but TB not eliminated by 2050
Current rate of decline -2%/yr
W Europe after WWII
-10%/yr
China, Cambodia
-4%/yr
Elimination target:<1 / million / yr
-20%/yr
W Europe after WWII
-10%/yr

Nat Rev Microbiol 2012; 10: 407–16.
-10%/year � Sustained socio-economic
development
� Universal health coverage &
social protection
� TB care widely accessible
� BCG vaccination in children
� Screening of high-risk groups (but
limited impact)
� Infection control practices (?)
TB incidence declined 10%/year
after WWII in Europe (the Netherlands)
Recipe:

Full implementation of Global Plan: 2015 MDG
target reached but TB not eliminated by 2050
Current rate of decline -2%/yr
W Europe after WWII -
10%/yr
China, Cambodia
-4%/yr
Elimination target:<1 / million / yr
-20%/yr
Eskimos> 10 ; < 20
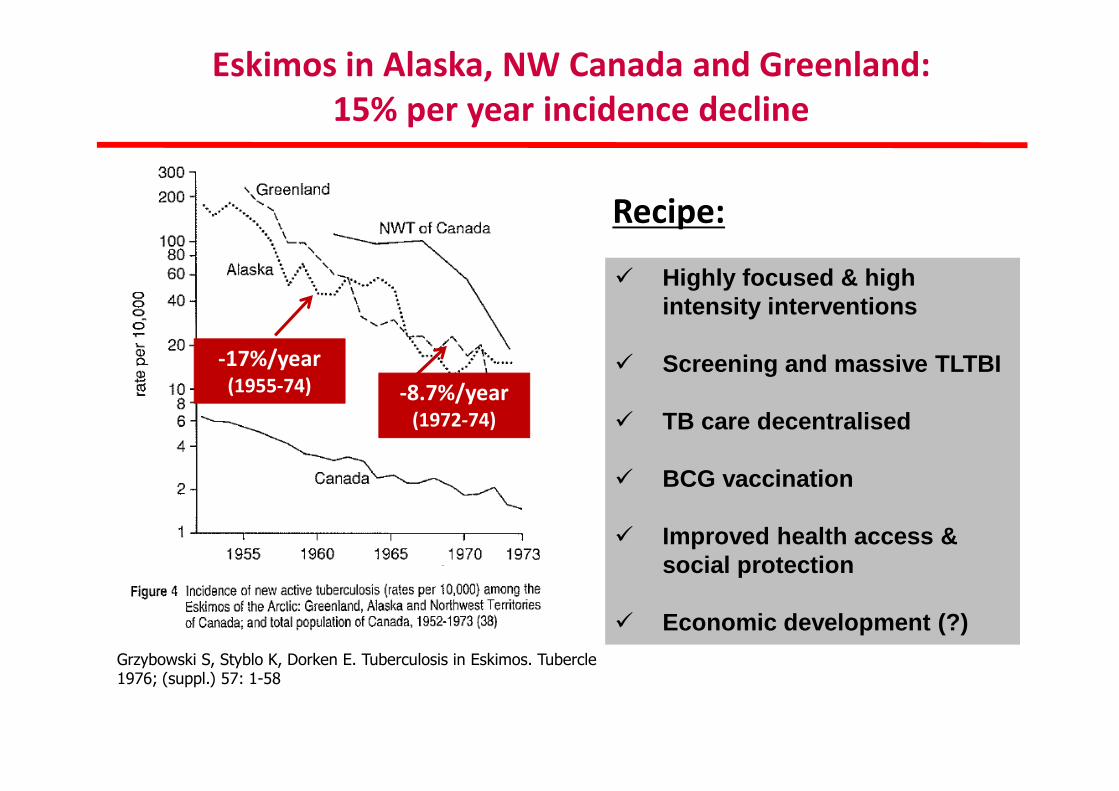
Eskimos in Alaska, NW Canada and Greenland:
15% per year incidence decline
� Highly focused & high intensity interventions
� Screening and massive TLTBI
� TB care decentralised
� BCG vaccination
� Improved health access & social protection
� Economic development (?)
Recipe:
-17%/year(1955-74) -8.7%/year
(1972-74)
Grzybowski S, Styblo K, Dorken E. Tuberculosis in Eskimos. Tubercle 1976; (suppl.) 57: 1-58
Can TB control among Eskimos be generalised to
the world?

Full implementation of Global Plan: 2015 MDG
target reached but TB not eliminated by 2050
Current rate of decline -2%/yr
W Europe after WWII -
10%/yr
China, Cambodia
-4%/yr
Elimination target:<1 / million / yr
-20%/yr
Elimination target:<1 /million/yr-20%/yr

DEFINITIONS
• Low-incidence countries: TB notification rate of <10 cases (all forms) per 100,000 population and year. Previous al ternative thresholds: <20/100,000, or <16/100,000.
• Pre-elimination: <10 notified TB cases (all forms) per million population per year. This is the same as proposed b y Clancy et al in 1991.
• TB elimination: <1 notified TB case (all forms) per million population and year.
• Alternative definitions: European region, <1 sputum -smear positive case per million; ECDC has proposed all fo rms of TB. US CDC defines elimination in the USA as < 1 case of T B, all forms, per million population.

TARGETS
<100 cases per millionCurrent TB burden-2012
in low-incidence countries
<10 cases per millionPre-elimination: 2035
in low-incidence countries
<1 case per millionElimination: 2050

� Economic development: better nutrition & housing
� Universal health coverage & social protection
� TB care widely accessible to all and of high-standards
� Focused, high-intensity interventions, including BCG in children
� Screening of high-risk groups and mass TLTBI
� Infection control practices
However… while incidence decline can accelerate, “elimination” is
another story, as it requires major reduction of:
In turn, this requires…new tools and increased financing
(i) transmission rate, and (ii) reactivation of latent infection among the already infected
What is needed to accelerate incidence decline and target "elimination"?
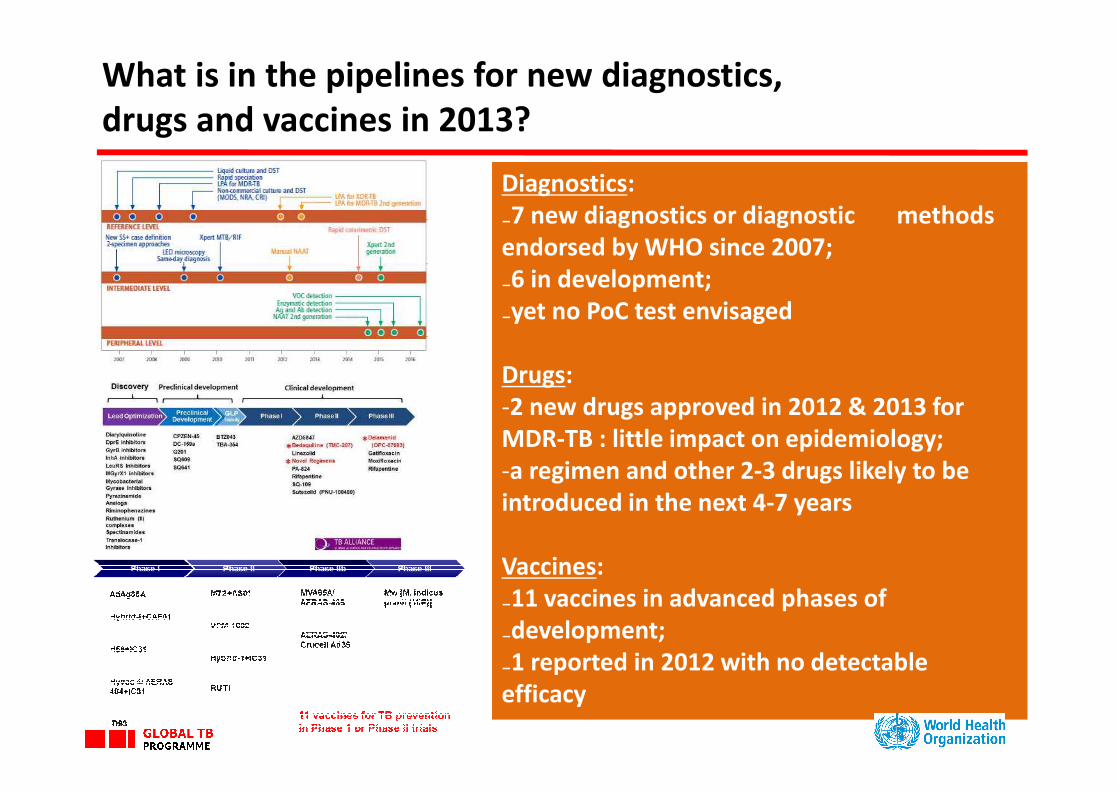
What is in the pipelines for new diagnostics,
drugs and vaccines in 2013?
Diagnostics:
₋7 new diagnostics or diagnostic methods
endorsed by WHO since 2007;
₋6 in development;
₋yet no PoC test envisaged
Drugs:
-2 new drugs approved in 2012 & 2013 for
MDR-TB : little impact on epidemiology;
-a regimen and other 2-3 drugs likely to be
introduced in the next 4-7 years
Vaccines:
₋11 vaccines in advanced phases of
₋development;
₋1 reported in 2012 with no detectable
efficacy

Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.

7 Core areas:
1. TB control commitment, TB awareness, and capacity of health systems
2. Surveillance3. Laboratory services4. Prompt, quality TB care for all5. M/XDR-TB and TB/HIV co-
infection6. New tools7. Partnership and collaboration

ACKNOWLEDGMENTSCOUNTRY RESPONDENTS
ALBANIA Hasan Hafizi
BELGIUM Maryse Wanlin, Wouter Arrazola de Onate, Guido Groenen
CROATIA Vera Katalinić Janković, Alexander Simunovic
CZECH REPUBLIC Jiri Wallenfels
DENMARK Peter Henrik Andersen
ESTONIA Piret Viiklepp, Manfred Danilovits, Tiina Kummik FINLAND Petri Ruutu
FRANCE Thierry. M. Comolet
GERMANY Walter Haas
GREECE Mina Gaga
HUNGARY Zsofia Pusztai
IRELAND Joan O Donnell
ISRAEL Daniel Chemtob
ITALY Enrico Girardi
KOSOVO-UNIMIK Rukije MehmetiLATVIA Vija Riekstina
MALTA Analita Pace Asciak
NORWAY Trude M Arnesen
POLAND Ewa Augustynowicz-Kopeć
PORTUGAL Raquel Duarte, Ana Maria Correia
R. OF MACEDONIA Stefan Talevski
ROMANIA Gilda Popescu, Domnica Chiotan
SERBIA Gordana Radosavljevic Asic
SLOVAKIA Ivan Solovic
SLOVENIA Marijan Ivanuša
SPAIN Elena Rodríguez Valín
SWEDEN Jerker Jonsson
SWITZERLAND Peter Helbling, Jean Pierre Zellweger
THE NETHERLANDS Gerard de Vries, Connie Erkens
UK Laura Anderson,Ian Laurenson

EUROPE HOW FAR TO REACH ELIMINATION?
EU LOW / MIDDLE TB INCIDENCE COUNTRIES ITALY
10 (33%) No TB Elimination plan NO
7 (23%) No TB elimination guideline NO
15 (50%) No HRD plan NO
10 (33%) No TB Reference centres YES
16 (53%) No TB budget NO
11 (37%) No supervision NO
25 (87%) No modelling NO
5 (17%) No NRL performing all F/SLD DST YES
4 (13%) No free access for all TB cases YES
20 (67%) No all F/SLD NO
10 (33%) Drugs stock-outs NO
10 (33%) No TB/HIV collab. activities NO
13 (43%) Hospital-based MDR-TB care YES
21 (70%) No strategy to introduce new tools NO
21 (70%) No international collaboration for TB
control/elimination
NO
10 (33%) No TB Consilium NO

INCIDENCE DECLINE: TECHNOLOGICAL BREAKTHROUGH BY 2025
ADDRESSING THE POOL OF LATENT INFECTION
Business as usual
Optimize current tools, ensure UHC and SP
New tools: vaccine, prophylaxis
Average -10%/year
-5%/year
-2%/year
Average -17%/year
GLOBAL TB
PROGRAMME

Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.

TB Elimination: from Wolfheze to Rome
THANK Rome 4-5 July 2014
Wolfheze, May 1990

WHO/ERS SUMMIT ON TBRome July 4 th-5th 2014
Elimination of TB in low incidence countries
• New WHO/ERS Framework launched on Sunday (Room AZ-4 h. 12.45)• Summary report published in the ERJ
• Unprecedent media coverage :187 cuttings, in 11 countries, > 500,000 page views every months

� Generalised (with social gradient)� Important community transmission� Many incident cases from recent transmission� Relatively high burden among young people� Dominant public health problem� Poorly resourced health systems
Low incidence
High incidence
Epidemiological characteristics
� Highly concentrated to risk groups� Close to elimination in large parts of the population� Low transmission� Outbreaks in special groups� LTBI relatively more important� Migration impact� Stronger health system but less TB visibility

ACTION FRAMEWORK8 PRIORITY ACTIONS FOR ELIMINATION IN LOW-INCIDENCE COUNTRIES
Invest in
research
and new tools
Optimize the
prevention and care
of drug-resistant TB
Address special needs of migrants and cross-border
issues
Address the most vulnerable and hard-
to-reach groups
Support global
TB prevention, care
and control
Ensure continuedsurveillance, programme
monitoring & evaluation , and case-based data
management
Undertake
screening for active
TB and latent TB infection
in TB contacts and
selected high-risk groups,
and provide appropriate
treatment
Ensure political
commitment, funding
and stewardship for
planning and
essential services
of high quality
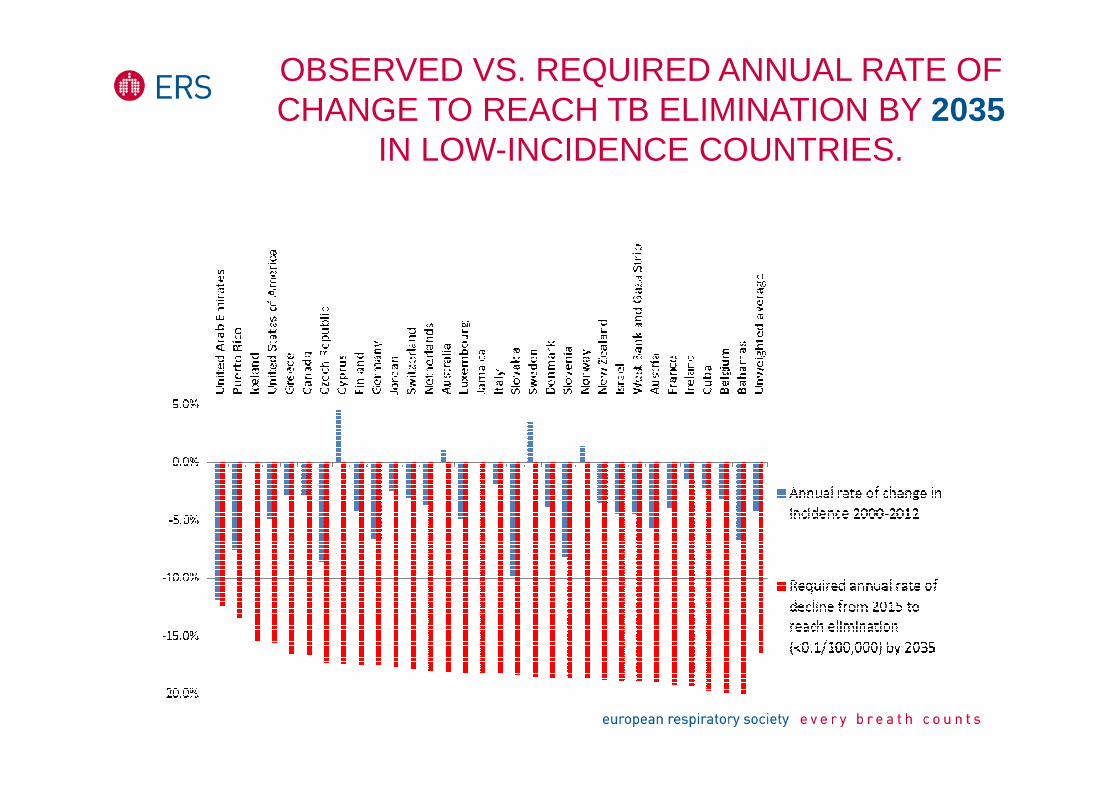
OBSERVED VS. REQUIRED ANNUAL RATE OF CHANGE TO REACH TB ELIMINATION BY 2035
IN LOW-INCIDENCE COUNTRIES.

OBSERVED VS. REQUIRED ANNUAL RATE OF CHANGE TO REACH TB ELIMINATION BY 2050
IN LOW-INCIDENCE COUNTRIES.
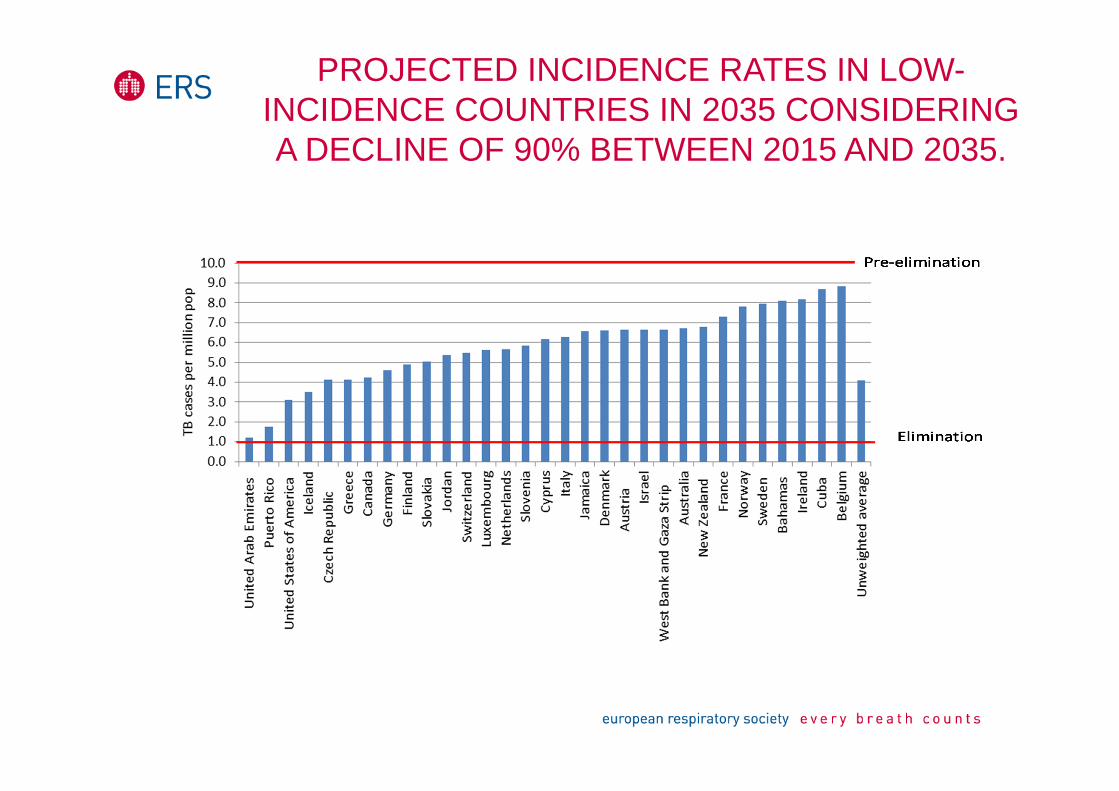
PROJECTED INCIDENCE RATES IN LOW-INCIDENCE COUNTRIES IN 2035 CONSIDERING A DECLINE OF 90% BETWEEN 2015 AND 2035.

-5
5
15
25
35
45
55
65
75
85
95
105
115
125
135
145
155
1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
All SS+ cases
SS+ Cypriots
SS+ ForeignBorn
All TB per1,000,000 pop
1 Caseper million
TB Elimination is possible: the case of Cyprus (ERJ 2014)

Introduction
AIMS: to describe
• The evolution of the strategies to prevent and manage TB• The evolution of the concept of TB elimination• The new WHO Post-2015 Strategy and the concept of pre-elimination • The outcomes of a European ERS, WHO and ECDC survey evaluating
European preparedness to reach elimination• The strategies to prevent and manage TB within the new TB Elimination
framework for low TB incidence countries • An example of epidemic of XDR-TB in a major city, which summarizes the
different issues discussed above.

L’UNDICENNE È IN ISOLAMENTO ALLA CLINICA DE MARCHI
Casi di Tbc a Milano, iniziata la terapiasul ragazzino con forma multiresistenteEsposito (Sitip): casi pediatrici del genere mai riscontrati negli ultimi 30 anni.
Terapia sperimentale con 5 farmaciPreoccupano i casi di tubercolosi a Milano. Sette quelli resi noti negli ultimi giorni: tre bambini di una scuola media, due di una scuola elementare della zona nord-est (asintomatici) e due studenti stranieri della facoltà di Scienze politiche dell’Università Statale. A far scattare l’allarme è stato un bambino italiano di 11 anni che frequenta la scuola media. «È arrivato da noi per un problema apparentemente di otorinolaringoiatra, ma le sue
condizioni generali e il quadro respiratorio ci hanno insospettito. Subito abbiamo pensato alla tubercolosi e la diagnosi è stata confermata» spiega Susanna Esposito, direttore della Clinica Pediatrica I dell’Ospedale Maggiore Policlinico di Milano e presidente della Società Italiana di Infettivologia Pediatrica (SITIP). Il bambino, ricoverato nella clinica De Marchi, «è affetto da un ceppo multiresistente, chiamato XDR, caratterizzato da una resistenza
allargata a un vasto numero di farmaci - chiarisce Esposito -. Si tratta di un ceppo molto raro e difficile da trattare che abitualmente non colpisce soggetti in età pediatrica, né quelli perfettamente immunocompetenti o senza
patologie di base
Corriere della Sera 31/10/2011

Index caseFAMILY
Male, 12 yearsLaryngeal + PTBLong diagnostic delayDirect Sputun examination +++Resistant to SHREZ+FQ+Inj+EtoHaarlem strain Mother, TST+, QF+
PTB, immigrant, histopathology+, CXR improved Cat 1
21 classmates tested:1 monolateral pleurisy (immigrant)10 TST+, QF+ (7 native, 3 immigrant)
2 dental hygienists tested: 2TST+, QF+
56 playmates tested:3 TST+, QF-(BCG vaccinated)
24 students tested in parallel class performing common activities:1 TST+, QF+1TST+, QF-
57 students tested in other classes:1TST+, QF+13 TST+, QF-
TB disease TST+, QF+ TST+, QF -
18 school staff tested:4TST+, QF+5TST+, QF-
Sister 6 yrs, PTB
Brother 10 yrs, PTB
Father, TST-, QF-
19 school canteen staff tested:3 TST+, QF -
37 educators tested:1 TST+, QF-
Summer camp circle
27 tested: All TST-, QF-
Sport related circle
Catechism related circle
50 tested: 1 TST+, QF+4 TST+, QF-
Other contacts

TREATING M/XDR-TB IS DIFFICULT
www.tbconsilium.org

ERS/WHO Consilium for M/XDR-TB
� Objectives:
� To allow a European clinician, free cost, to load patient’s data and receive in 1 working day suggestions by 2 experts on how to manage a difficult-to treat TB case
� To support follow-up of TB patients travelling within Europe
� Web-based regional platform
� Specialized team able to cover several perspectives:(clinical for both adults and children, surgical, radiological, public health, psychological, nursing, etc.
� Managed by ERS, in collaboration with WHO Europe (formal agreement) and ECDC
The web platform www.tbconsilium.org
• Now in ENG. RUS, SPA, PORT (FREN)
• Hosted in Switzerland (-> Swiss regulation)
• 4 processes supported + 2 in preparation:
o “Consilium” (get experts advice on cases in24-36 hrs)o Trans border cases (send a case to a National TB Project
Representative)o M&E of guidelines implementationo Expert opinion for compassionate useo Patient’s tracko LTBI management
• Next steps: « Drug-O-Gram » plug in

www.tbconsilium.org


Conclusions
• 1. While TB Elimination was considered an advocacy tool for >20 years, there is epidimiological plausibility
• 2. The majority of low TB incidence counries is on track to reach pre-elimination by 2035 (2050) and scale-up e limination thereafter
• 3. Among the conditions to reach TB elimination: - new vaccine, new point-of-care/rapid test, new effe ctive short
regimens to treat TB and LTBI- Sound health policies beyond NTP

ERS Conference, Munich, September 2014: the launch

THANKYOU !







