The role of the nurse in the process
of breaking bad news in the inpatient
clinical setting
Clare Warnock, Practice Development Sister, Weston Park Hospital , Sheffield Teaching Hospitals NHS Trust (STHFT) Angela Tod, Research fellow, Sheffield Hallam University Julie Foster, Clinical governance co-ordinator, STHFT Cathy Soreny, Assessment staff nurse, Ophthalmology, STHFT Janet Turner, Clinical effectiveness project manager, STHFT
Why we did our study
We wanted to explore a subject that was important to the work of all AHP’s
Gaps in the research
little research on the process of breaking bad news or
the role of the nurse or AHPs in breaking bad news
We decided to explore the role of the nurse in the process of breaking bad news
Focusing on the inpatient clinical setting
Setting and sample
59 inpatient areas in STH took part in the study
Five questionnaires were sent to the ward manager
distributed to nurses with a range of grade and experience
30 questionnaires sent to members of the EBC
236 questionnaires were returned
71% response rate
132 from medical areas, 60 surgical areas, 44 others
e.g. ITU, neonatology, EBC
Response
Roles of participants
60% (N=142) were staff nurses
27% (N=64) were ward sisters/charge nurses
Others included nurse specialists, clinical educators and midwives
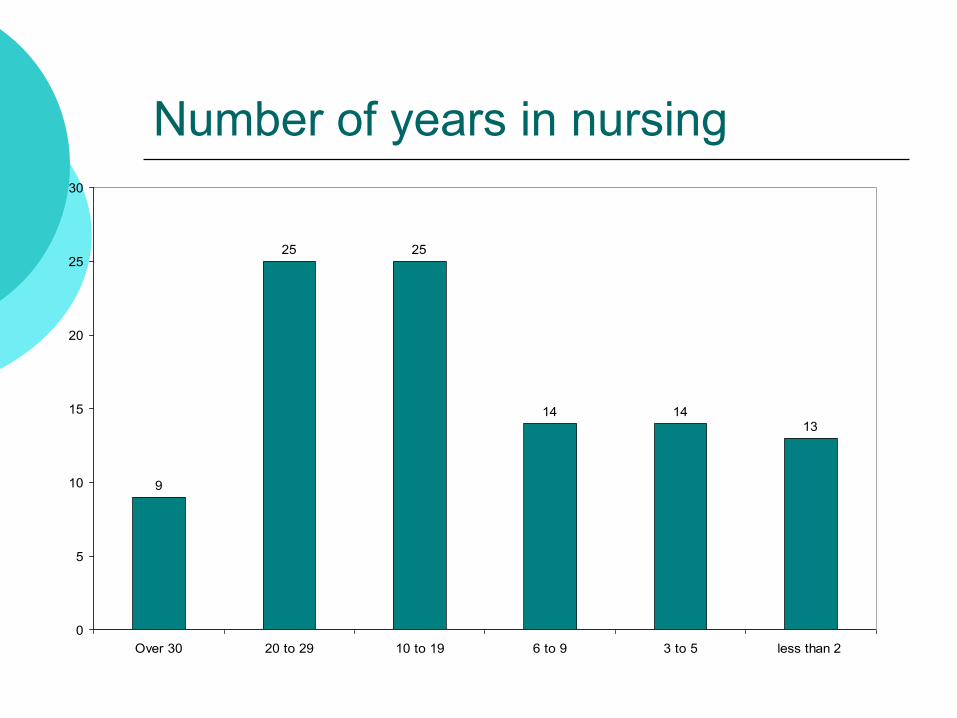
Number of years in nursing
9
25 25
14 1413
0
5
10
15
20
25
30
Over 30 20 to 29 10 to 19 6 to 9 3 to 5 less than 2
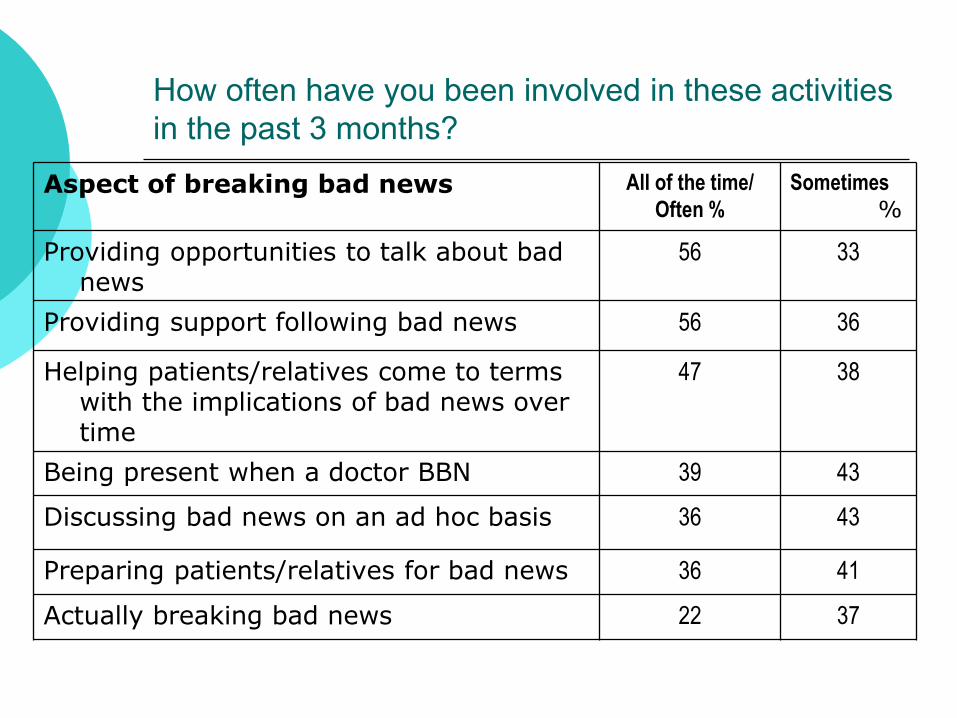
How often have you been involved in these activities
in the past 3 months?
Aspect of breaking bad news All of the time/ Often %
Sometimes
%
Providing opportunities to talk about bad news
56 33
Providing support following bad news 56 36
Helping patients/relatives come to terms with the implications of bad news over time
47 38
Being present when a doctor BBN 39 43
Discussing bad news on an ad hoc basis 36 43
Preparing patients/relatives for bad news 36 41
Actually breaking bad news 22 37
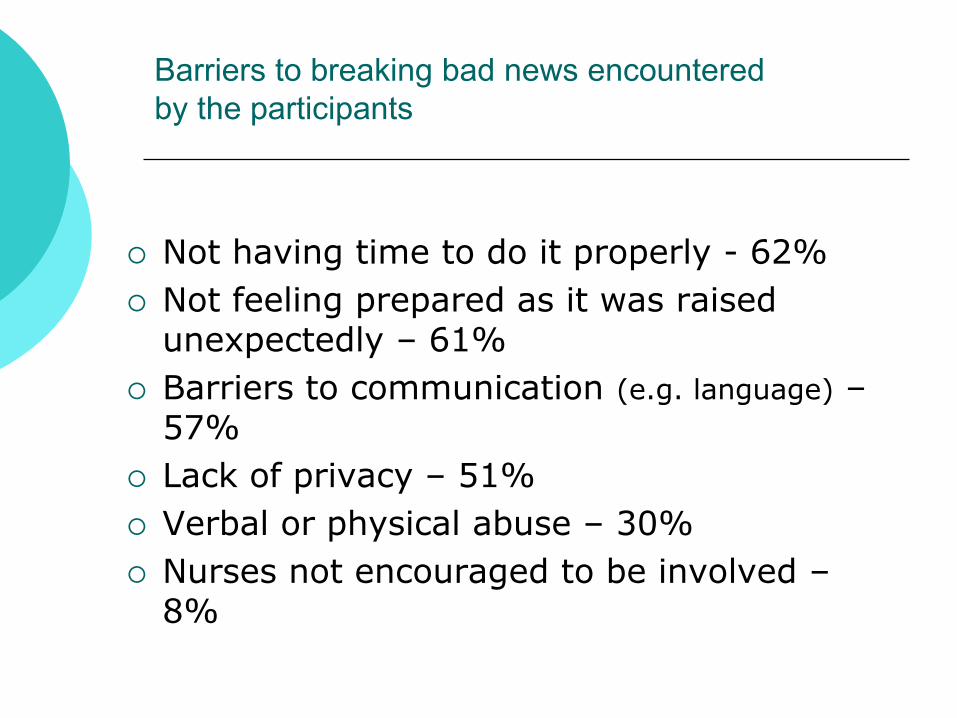
Barriers to breaking bad news encountered
by the participants
Not having time to do it properly - 62%
Not feeling prepared as it was raised unexpectedly – 61%
Barriers to communication (e.g. language) – 57%
Lack of privacy – 51%
Verbal or physical abuse – 30%
Nurses not encouraged to be involved – 8%

Feelings about being involved in BBN
Positive replies
I avoid being involved as I
find it difficult - 6%
I feel able to initiate
discussions around BBN-
70%
I have good strategies for
coping with my emotional
reactions - 61%
I have difficulty dealing
with patients/relatives
emotional reactions - 25%
Mixed replies
I feel confident in my skills in
the process of BBN- 55%
There is a good system of
support when I am involved
in BBN in my area - 50%
I feel able to support those
from different cultural
backgrounds - 41%
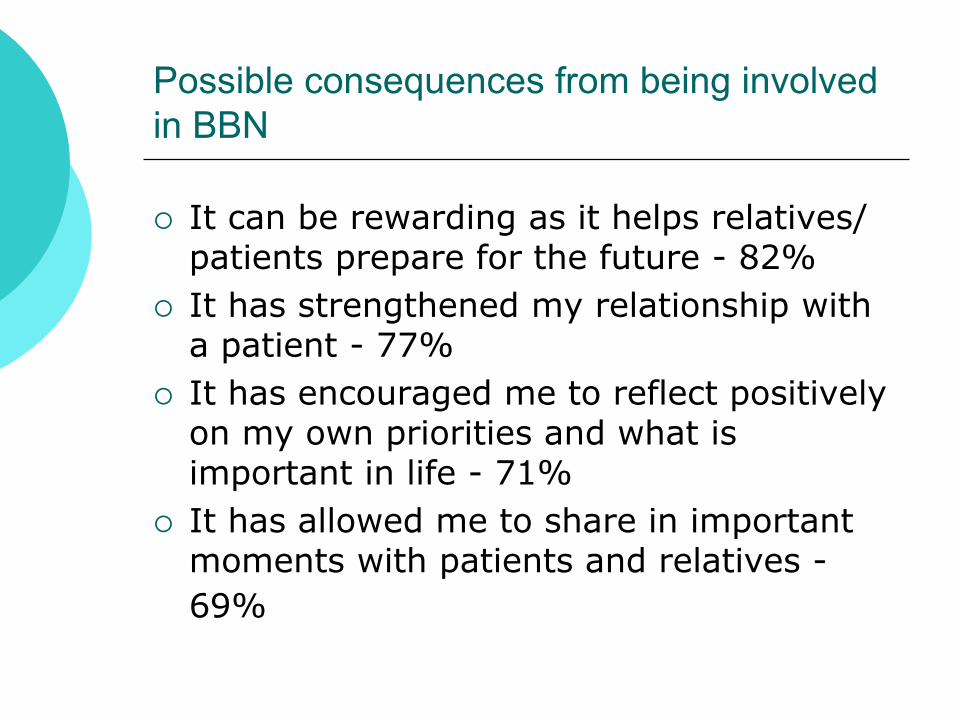
Possible consequences from being involved
in BBN
It can be rewarding as it helps relatives/ patients prepare for the future - 82%
It has strengthened my relationship with a patient - 77%
It has encouraged me to reflect positively on my own priorities and what is important in life - 71%
It has allowed me to share in important moments with patients and relatives -
69%

Difficult experiences of BBN
We asked participants to describe a difficult experience they had encountered when BBN
128 descriptions were provided
5 key themes were identified
How the bad news was broken
Information held by patients and relatives
Unexpected death
Reactions to bad news
Significant events

How bad news was broken
Two components Barriers to communication
Who is present
Barriers to communication
Practical/physical lack of privacy, lack of time to explain, giving bad
news over the phone, difficulty contacting family
Language e.g. tracheostomy, deafness, no shared language
Barriers to communication
Knowledge deficit
not knowing the relative/patient prior to breaking bad news
having limited knowledge of the events surrounding the need to break bad news
concerns about their own level of clinical knowledge in relation to a specific aspect of care
Examples of knowledge deficit
I had to talk to the relatives of a young man who had been on dialysis and had died earlier that day. I was on a late shift and this had occurred during the morning. I was not present at the time of death. I found it difficult to answer the family’s questions. It was distressing for all concerned.

A patient arrived onto the ward and died within 15 minutes. I did not know any of the patents relatives and I had to break the bad news to them on their arrival.
The decision to take a very ill patient off a ventilator: I found this difficult and hard to support the family as I had limited knowledge in this area

How bad news was broken
Who is (not) present
Relatives
Bad news broken and relatives not present
Doctor from patients specialty medical team
Patient an outlier, unable to contact own medical team
Nurse
Not present at the time so doesn’t know what has been said

Examples of “who is present”
A lady was told she was unable to have a CABG due to poor health. She was advised to have a relative present but insisted to be told before the relatives arrived. The relatives were annoyed and abusive to staff that she was told without their presence.
Examples of “who is present”
A patient was told bad news by the doctor with no nurse present. I eventually found the patient crying. I wasn’t very helpful as I did not have enough information to help.
It was difficult caring for a dying patient from a different specialty. Relatives needed information from medical staff who were busy elsewhere

Information held by relatives and patients
Issues around disclosure Relatives don’t want patient to be
informed
Relatives not being honest with the patient
Patient doesn’t want to be informed
Patients relatives not being aware of fundamental information not having been told the information
misunderstood or misinterpreted the information they had been given

Examples “disclosure”
We had a young girl whose treatment had stopped working and she was commenced on a palliative care regime. However, her parents wanted her to continue to think she was going to be cured. It was difficult to explain anything as you always had to watch everything you said to her
Examples “disclosure”
A female patient was keen to go home she was aware she was dying. Her partner was agreeing with her while in the room but as soon as he was away from her he was expressing concerns that he wouldn’t be able to manage and didn’t want the responsibility of looking after her
Unexpected death
The consequences of unexpected death
dying without a relative present
encountering practical barriers such as BBN over the phone
Relatives unprepared for the news
their reactions included shock, hysteria and disbelief
In three cases the nurses had given positive information about the patient’s condition shortly before an unexpected cardiac arrest

Reactions to bad news
Negative reactions included
verbal abuse
anger
physical aggression
intimidation
hysteria
complete denial
Significant events
Deaths that were particularly challenging or emotional for the relatives and/or the nurse a prolonged death a family finding it difficult to watch their loved
one die conflict between family members
Situations involving mothers and daughters E.g. helping a young mother come to terms
with her own incurable prognosis
Family disagreements about treatment decisions

Significant events
Events that were particularly burdensome for the patient
informing a patient they had been burgled while they were in hospital
discharge arrangement falling through for a third time
Exceptional demands being made of the nurse
a nurse who had cared for a patient from a large family had to accompany them to the mortuary on 5 separate occasions
Significant events
A patient who was dying, but whose death was prolonged. I had contacted the family and asked them to sit with the patient. I had thought that the patient would pass away imminently however, a week later I was still telling the relatives the same news, this was a distressing time for the family
Significant events
I looked after a patient who had died. The deceased came from a large family who all came at different times to say their goodbyes. I had to escort each relative separately to see the body (5 times)
On one shift I spent the whole day breaking bad news to relatives. I found this stressful and upsetting I cried later in the company of colleagues

Significant events
When a patient was dying the relatives wanted us to give more drugs to expedite the death. The relatives wanted the death to happen quickly because it was too painful for them to watch
A patient in a terminally ill condition had two daughters who did not communicate and hated each other caused a terrible atmosphere around the patients bed side

Formal training received
None – 53%
Half a day or less – 24%
Full day – 11%
2 to 5 days – 5%
6 to 10 days – 1%
More than 10 days – 5%
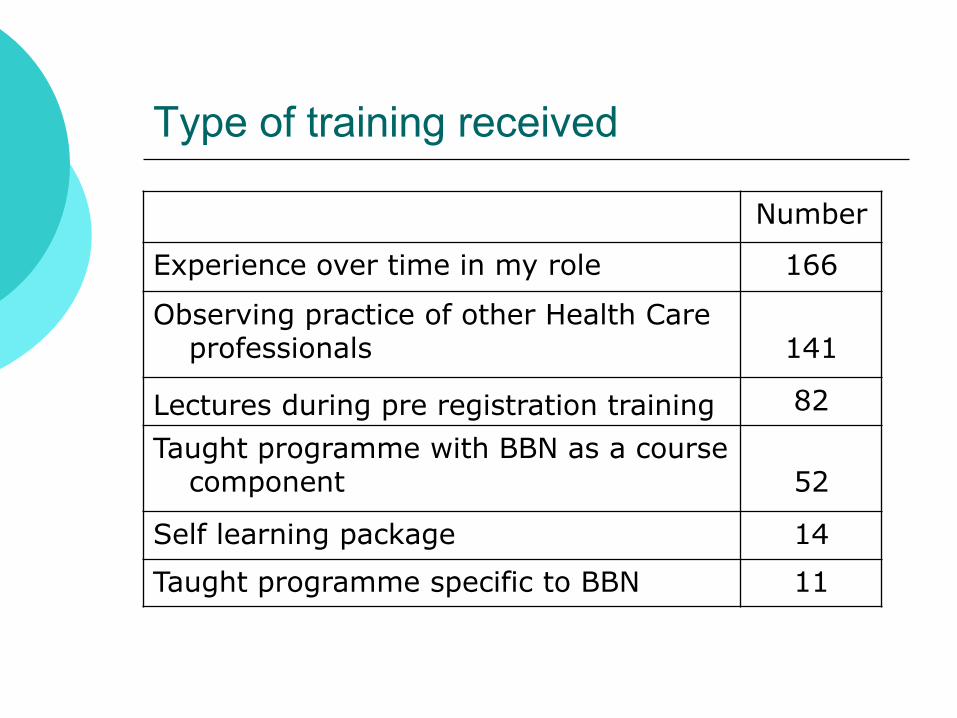
Type of training received
Number
Experience over time in my role 166
Observing practice of other Health Care professionals
141
Lectures during pre registration training 82
Taught programme with BBN as a course component
52
Self learning package 14
Taught programme specific to BBN 11
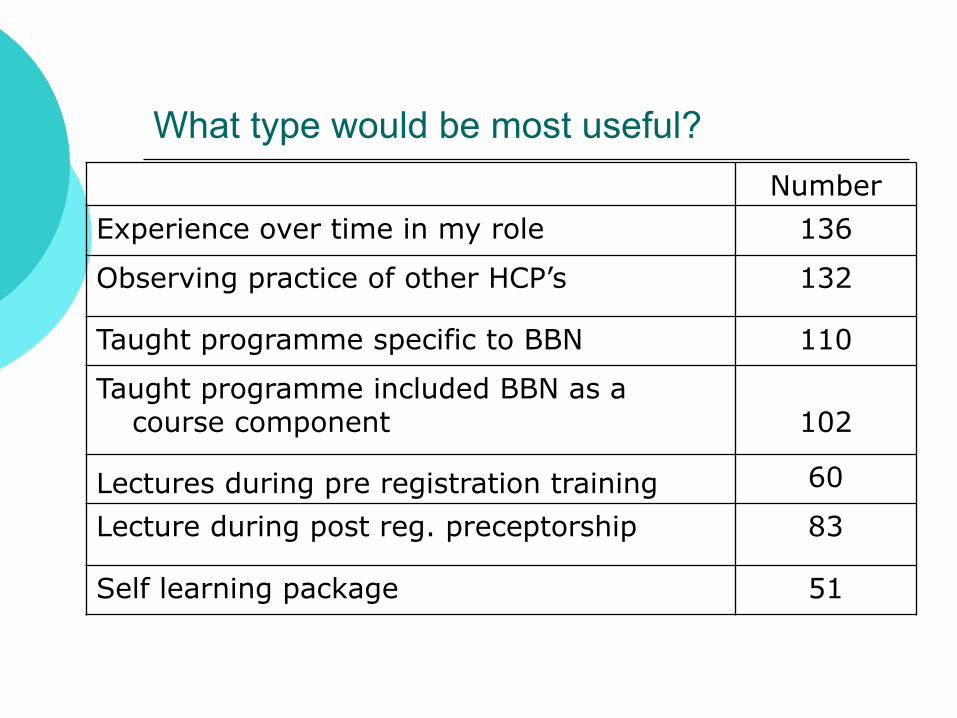
What type would be most useful?
Number
Experience over time in my role 136
Observing practice of other HCP’s 132
Taught programme specific to BBN 110
Taught programme included BBN as a course component
102
Lectures during pre registration training 60
Lecture during post reg. preceptorship 83
Self learning package 51
Conclusion
Our work identified that BBN was a complex activity often carried out in difficult circumstances
Being involved in the process of breaking bad news had positive consequences
It was also associated with difficulties and challenges
The majority of the nurses had no formal education in BBN
We need to
Acknowledge the role of all staff in the process of BBN
Provide opportunities for them to reflect on their role and their experience
Introduce ways in which they can look
after themselves when involved in BBN
Today’s programme is shaped around these themes







