Navin K. Kapur, MD, FACC, FSCAI, FAHAAssociate Professor, Department of Medicine
Interventional Cardiology & Advanced Heart Failure ProgramsExecutive Director, The Cardiovascular Center for Research & Innovation
The Pathophysiology of Cardiogenic ShockKnowledge Gaps & Opportunities

Relevant Disclosures
Research Funding & Speaker/Consulting Honoraria: Abiomed, Abbott, Boston Scientific, Maquet, Medtronic, MD Start, Cardiac Assist
Herbert J. Levine Foundation
Tufts Medical Center
RO1HL139785, RO1H133215Charlton Award
Tufts Medical Center

10/2007
Anterior MI
LAD PCI and IABPLVEF 20%
11/2007
ReadmittedHeart FailureLVEF 25%
11/2007
Readmitted - HFICD ImplantedLVEF 25%
3/2008
ReadmittedRecurrent HFLVEF 25%
4/2009
Readmitted – HF/ACS
Impella SupportedLAD and LCx PCI
LVEF 25%
7/2012
ReadmittedRecurrent HFLVEF 20%
3/2015
ReadmittedRecurrent HFLVEF 20%
12/2017
Cardiogenic Shock
Impella + VA-ECMOLVEF 10%
12/2017
Cardiogenic Shock
BiventricularCentrimags
LVEF 10%
4/2018
OrthotopicHeart Transplant
LVEF 65%
Which Cardiogenic Shock Are We Talking About?AMI-Shock HR-PCI
Advanced HF-ShockAmbulatory Shock
Acute HF Syndromes

Modified from Goodlin. JACC 2009;54:386
Acute MICardiogenic Shock
Advanced HFCardiogenic Shock
Which Cardiogenic Shock Are We Talking About?

Our Current Understanding of CGS PhysiologyFounded in AMI-Shock
AHA Shock Consensus Statement Circ 2017
Coronary Problem
Ventricular Failure
Vascular Response

Primary Target of Heart Failure Therapy: Reduce LV Wall Stress
Normal AcuteLoad(AMI)
CompensatoryHypertrophy
Systolic Failure
DilatedCardiomyopathy
Plumbing Principles: Pressure and Volume
Pressure x Radius ESP x EDV2 x Wall Thickness LV MassLaplace’s Law: Wall stress = =
Wall Stress

Pres
sure
Volume
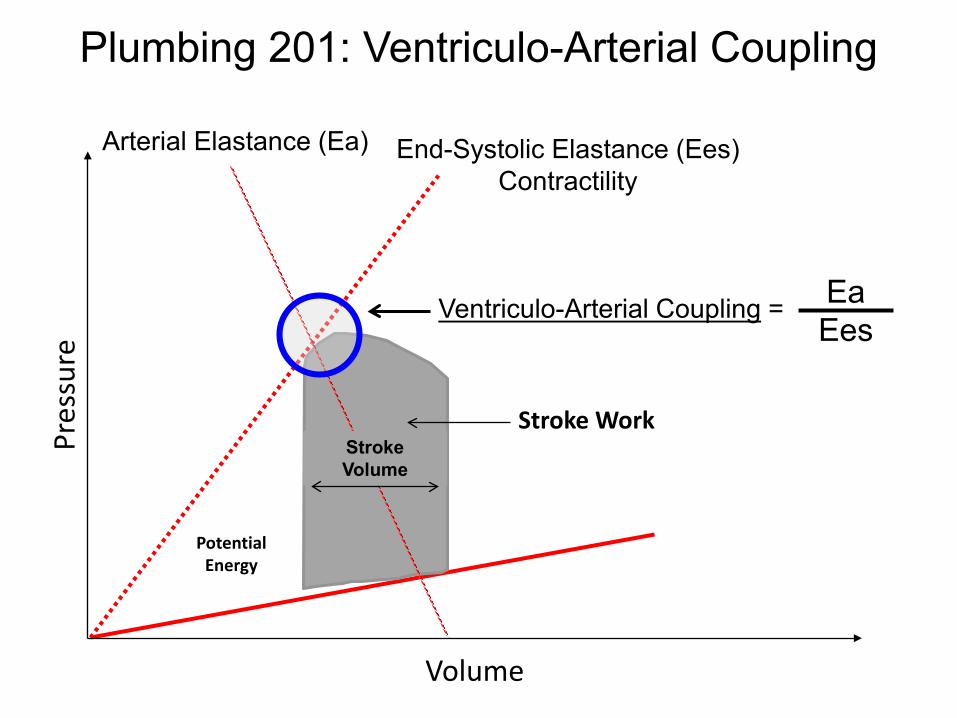
Arterial Elastance (Ea)
Stroke Volume
Stroke Work
PotentialEnergy
End-Systolic Elastance (Ees)ContractilityEa =ESP
SVAfterload = Wall Stress = ESP x EDV
Plumbing 101: Ventricular ‘Loading’ Conditions
Pres
sure
Volume
Arterial Elastance (Ea)
Stroke Volume
Stroke Work
PotentialEnergy
End-Systolic Elastance (Ees)Contractility
Ventriculo-Arterial Coupling = EaEes
Plumbing 201: Ventriculo-Arterial Coupling
Stro
ke V
olum
e
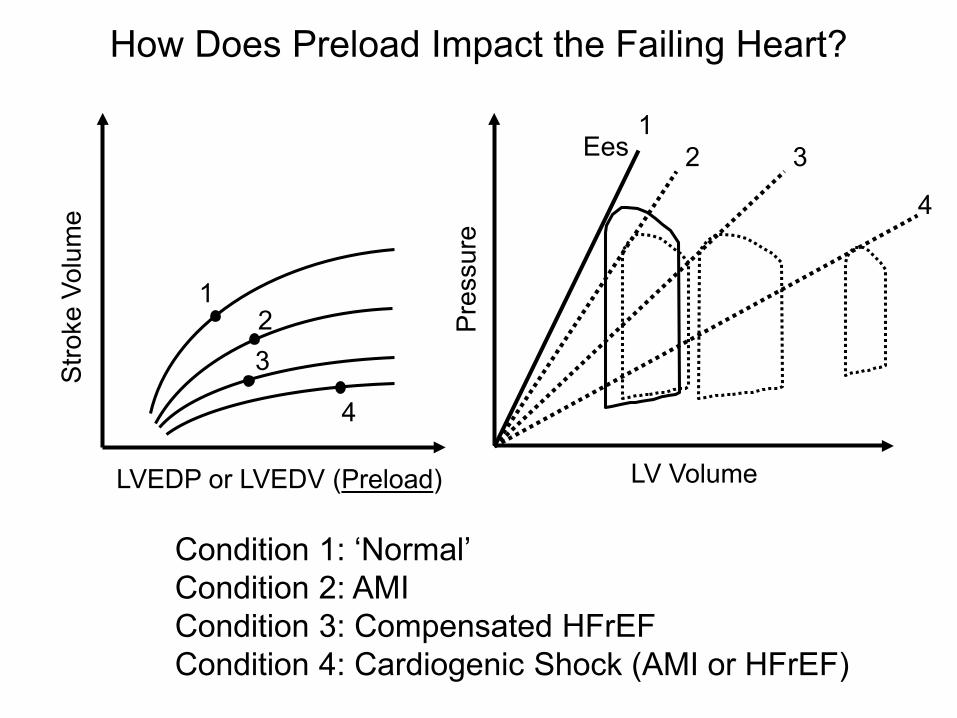
LVEDP or LVEDV (Preload)
1
3
4
2
LV Volume
Ees
Pres
sure
12 3
4
Condition 1: ‘Normal’Condition 2: AMICondition 3: Compensated HFrEFCondition 4: Cardiogenic Shock (AMI or HFrEF)
How Does Preload Impact the Failing Heart?

Volume
Pres
sure
Inefficient VA-Coupling & Increased Wall Stress in Shock
EaEes
= 1
EaEes
>> 1

Courtesy of HC Champion
Afterload:1. Resistance 2. Impedance3. PA compliance4. PA elastance
Pulm. ArterialHypertension
Plumbing 301: RV-PA Coupling

Effect of elevated pulmonary capillary wedge pressure (PCWP) onpulmonary vascular resistance-compliance relationship (RPA-CPA).
Tedford R J et al. Circulation 2012;125:289-297
PA Compliance
PA ResistancePCWP =
Pulm. VenousCongestion
Plumbing 401: RV-PA-LV Coupling
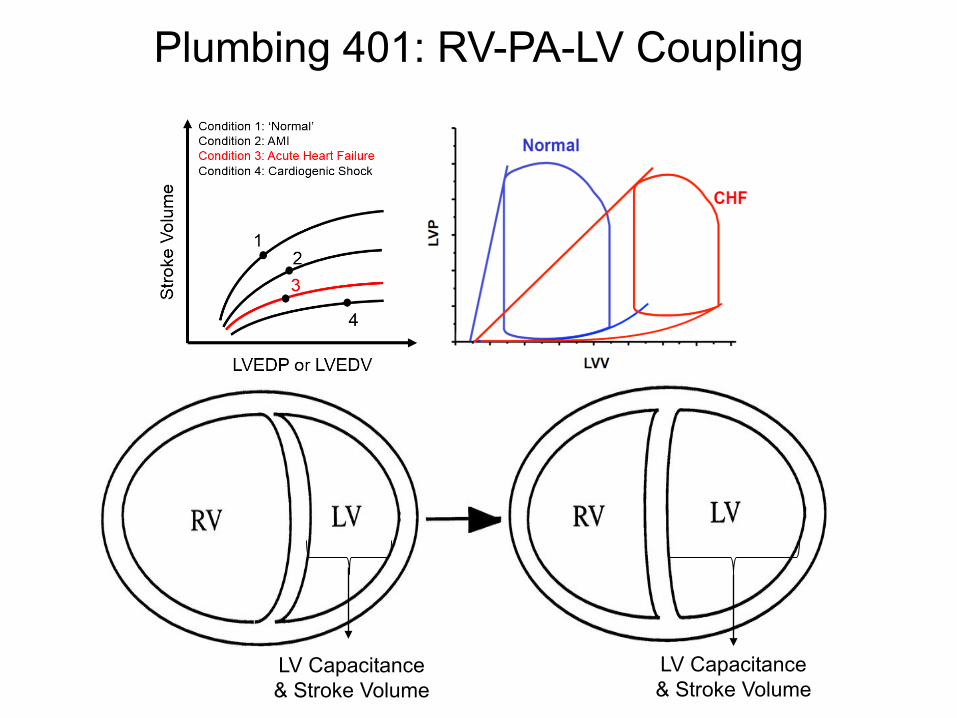
LV Capacitance& Stroke Volume
LV Capacitance& Stroke Volume
Plumbing 401: RV-PA-LV Coupling
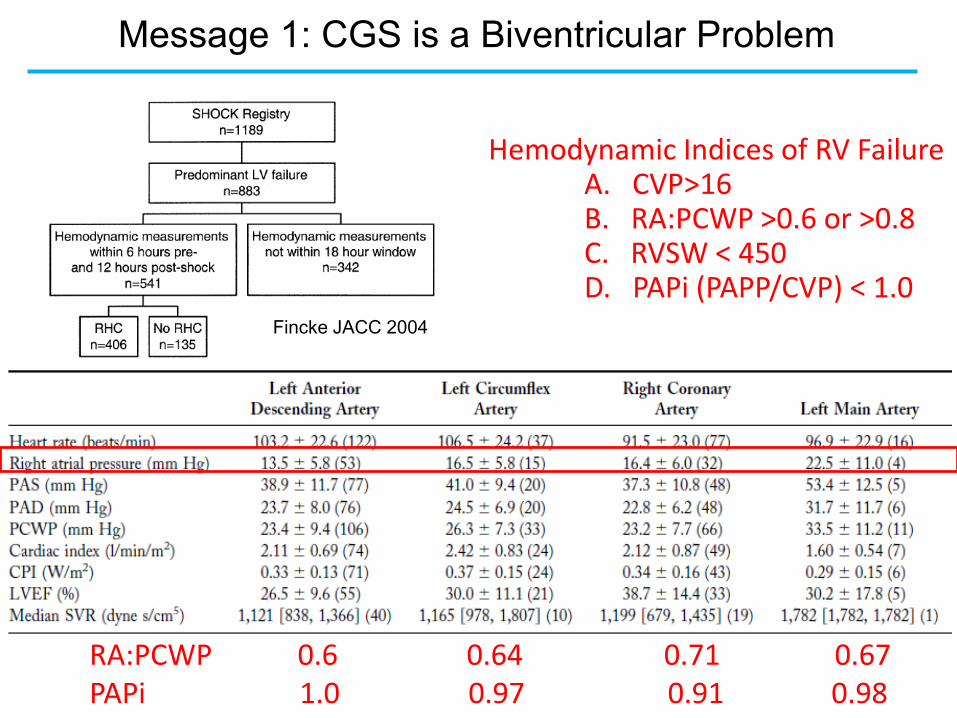
Hemodynamic Indices of RV FailureA. CVP>16B. RA:PCWP >0.6 or >0.8 C. RVSW < 450D. PAPi (PAPP/CVP) < 1.0
RA:PCWP 0.6 0.64 0.71 0.67PAPi 1.0 0.97 0.91 0.98
Fincke JACC 2004
Message 1: CGS is a Biventricular Problem

Lala and Kapur et al. J Card Failure 2017
Message 1: CGS is a Biventricular Problem

Largest US registry of Acute MCS device use in Cardiogenic ShockOver 500 patients with PA Catheter Indices
Total: 1010 Cases
The Cardiogenic Shock Working Group

Tufts Cardiogenic Shock AlgorithmHemodynamically driven decision making
Biventricular Congestion in Cardiogenic Shock is Commonand Associated with High In-Hospital Mortality
Cardiogenic Shock Working Group
Message 1: CGS is a Biventricular ProblemMessage 1: CGS is a Biventricular Problem
J Card Fail 2016
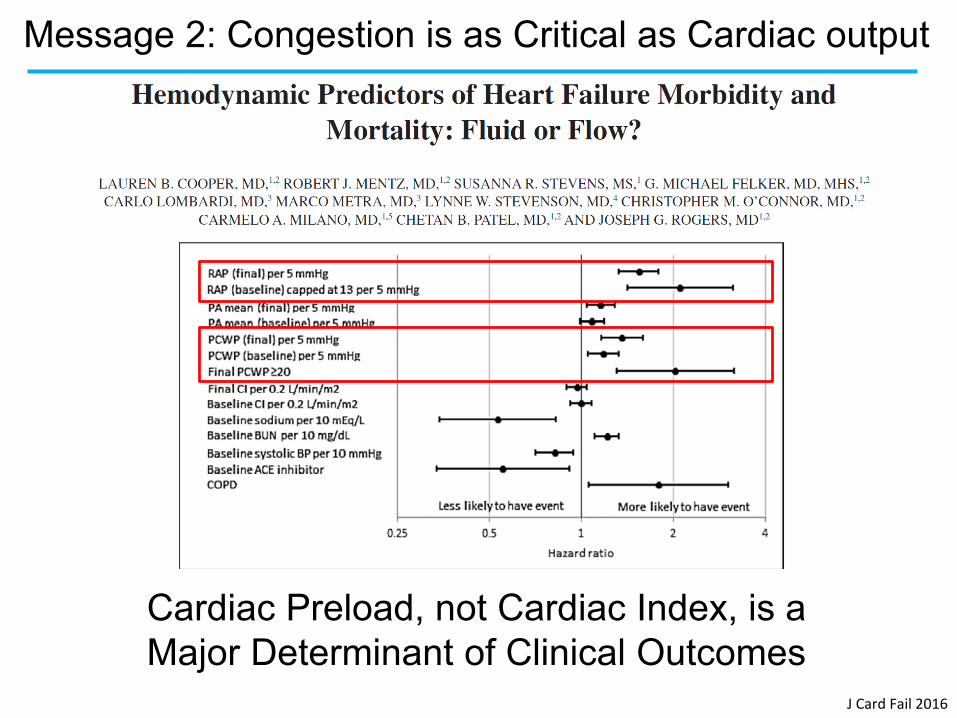
Cardiac Preload, not Cardiac Index, is a Major Determinant of Clinical Outcomes
Message 2: Congestion is as Critical as Cardiac output

Mullens and Tang JACC 2009
Central Venous Congestion Worsens Renal Function in HF
Message 2: Congestion is as Critical as Cardiac output
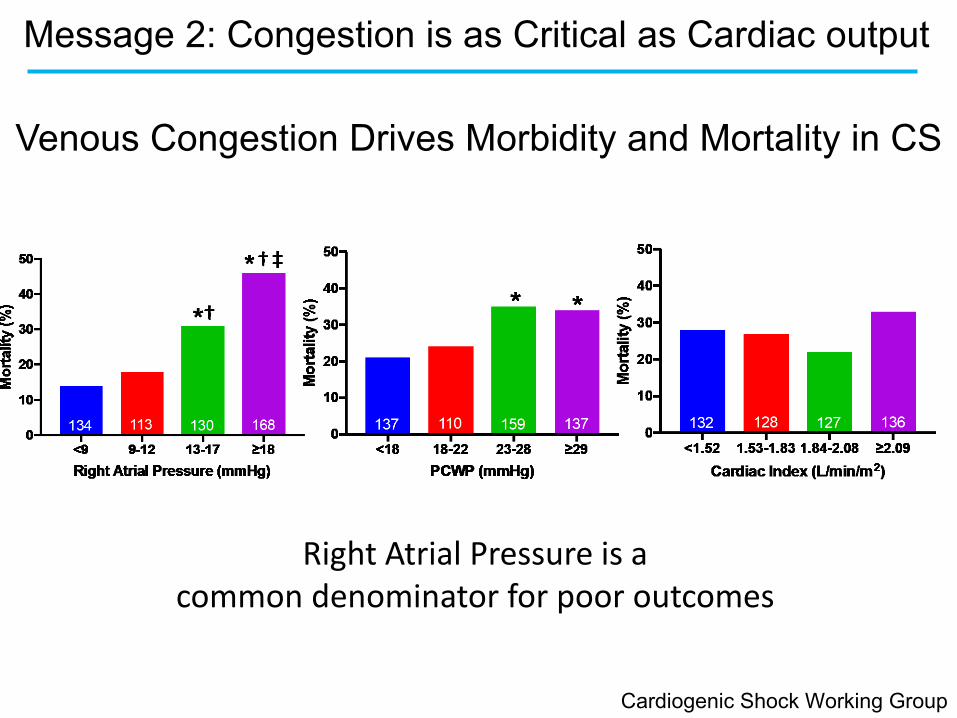
Right Atrial Pressure is a common denominator for poor outcomes
Venous Congestion Drives Morbidity and Mortality in CS
Cardiogenic Shock Working Group
Message 2: Congestion is as Critical as Cardiac output
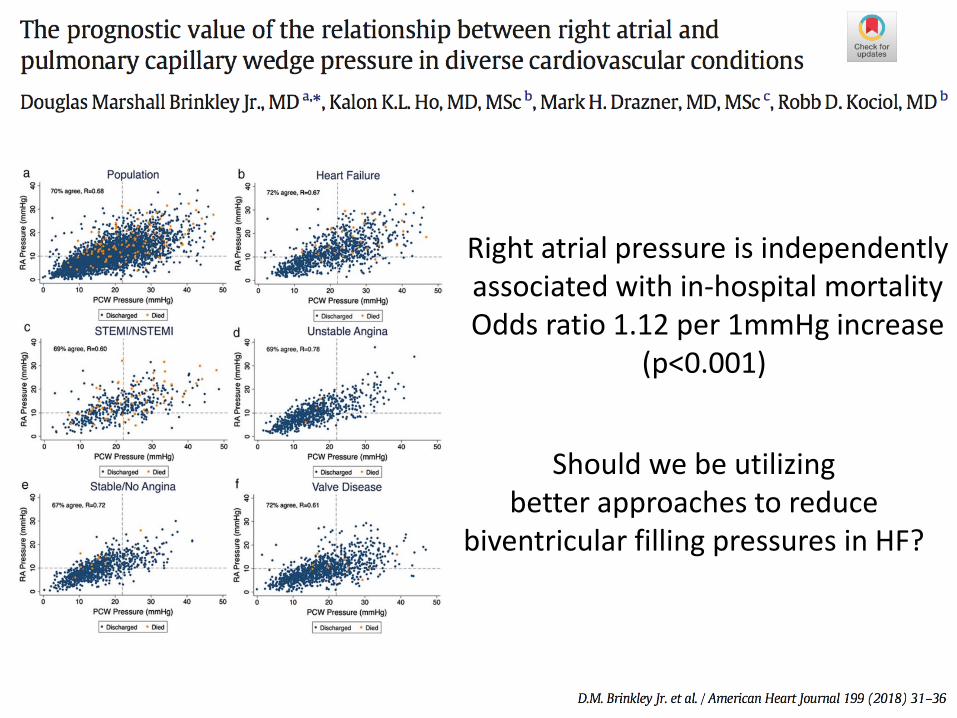
Right atrial pressure is independentlyassociated with in-hospital mortalityOdds ratio 1.12 per 1mmHg increase
(p<0.001)
Should we be utilizing better approaches to reduce
biventricular filling pressures in HF?
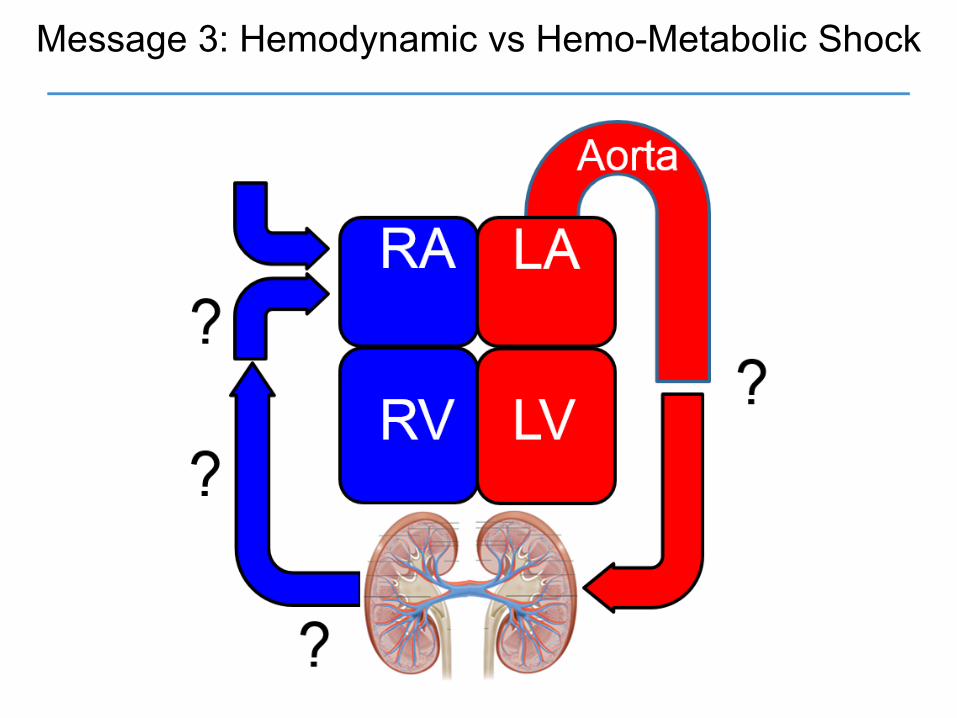
Message 3: Hemodynamic vs Hemo-Metabolic Shock

Morine & Kapur et al. Shock Working Group
Late ShockDeep ShockSevere Shock
Hemo-MetabolicShock
Pre-ShockEarly ShockMild Shock
HemodynamicShock
Message 3: Hemodynamic vs Hemo-Metabolic Shock
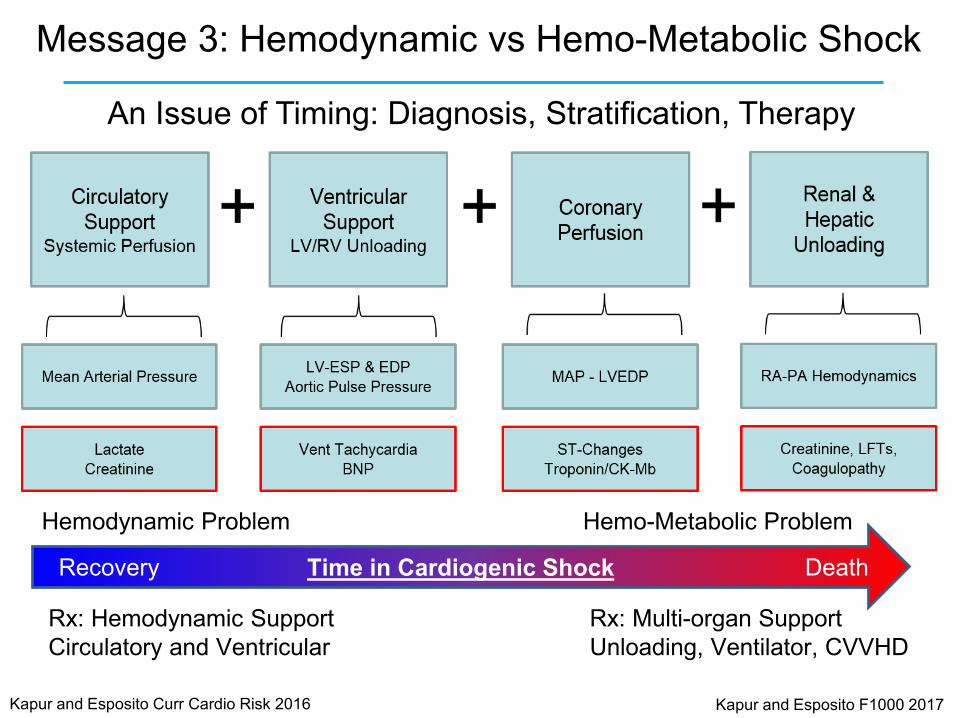
Time in Cardiogenic Shock
Rx: Multi-organ SupportUnloading, Ventilator, CVVHD
Hemo-Metabolic Problem
Rx: Hemodynamic SupportCirculatory and Ventricular
Hemodynamic Problem
Recovery Death
Kapur and Esposito Curr Cardio Risk 2016 Kapur and Esposito F1000 2017
An Issue of Timing: Diagnosis, Stratification, Therapy
Message 3: Hemodynamic vs Hemo-Metabolic Shock

Tufts Cardiogenic Shock AlgorithmHemodynamically driven decision making
Morine & Kapur et al. Shock Working Group
Escalating Inotrope/Vasopressor UseMessage 4: Escalating Pharmacologic Therapy is Futile

Kapur & Esposito. Curr Cardiol. 2016
Message 5: Hemodynamically Driven Decision Making
CGS Management begins with a PA Catheter

Future Directions for the Science of Cardiogenic Shock
Ventricular Load Impacts Myocardial Recovery
C
Esposito, Zhang, Qiao & Kapur et al JACC 2018
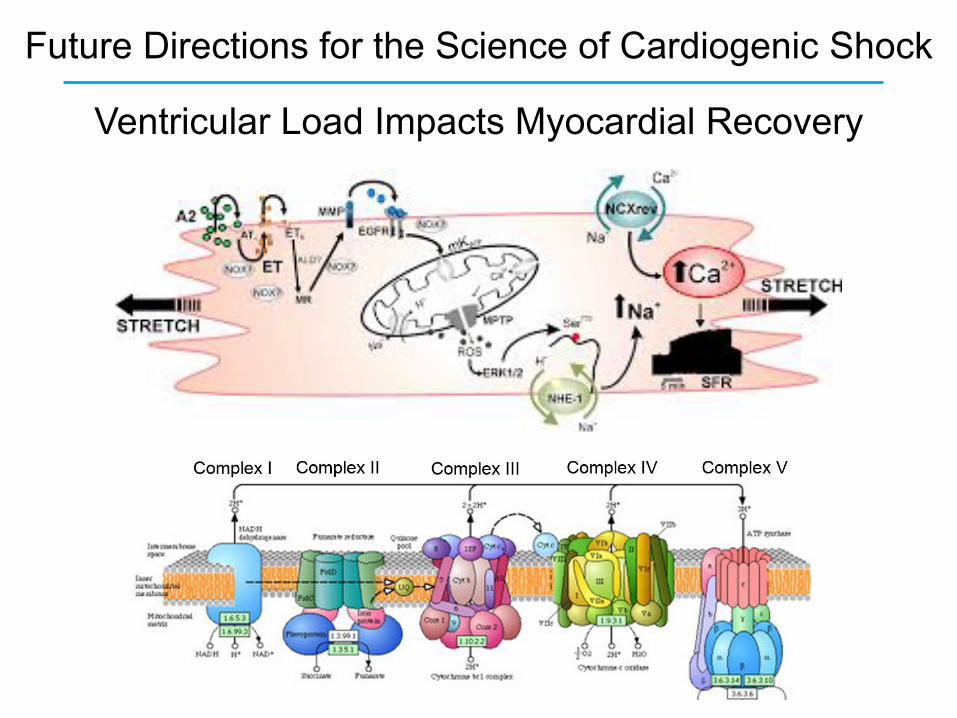
Future Directions for the Science of Cardiogenic Shock
Ventricular Load Impacts Myocardial Recovery








