
Risk-adjusted and Case-matched Comparative Study Comparing Antegrade and Retrograde Cerebral Perfusion in Aortic Arch Surgery Based on the Japan Adult Cardiovascular Surgery Database
The Japan Cardiovascular Surgery Database Organization
Usui A, Miyata H, Ueda Y
Motomura N, Takamoto S
Objective
Antegrade cerebral perfusion (ACP) and retrograde cerebral perfusion (RCP) are two techniques for brain protection in aortic arch surgery.
We conducted a large-scaled, comparative clinical study between ACP and RCP to evaluate up-to-date clinical outcomes based upon Japan Adult Cardiovascular Surgery Database (JACVSD).

Patients selection
Ascending or arch AOElective surgeryNo-dissection10 pt./year < (65 institutes)Risk adjusted analysis
Matched pair analysis
1185 ACP 392 RCP
463 ACP 304 RCP
3359 ACP1232 RCP
8470 aortic surgery
Use of ACP or RCP
2005-2007116 institutes
Statistical analysis

End points Mortality
30 days mortality Operative mortality
In-hospital complications: CNS dysfunction (Stroke, TIA, Coma) Paraparesis / paraplegia Reoperation for any reason Prolonged ventilation 24< hours Renal failure required dialysis Deep sternal wound infection
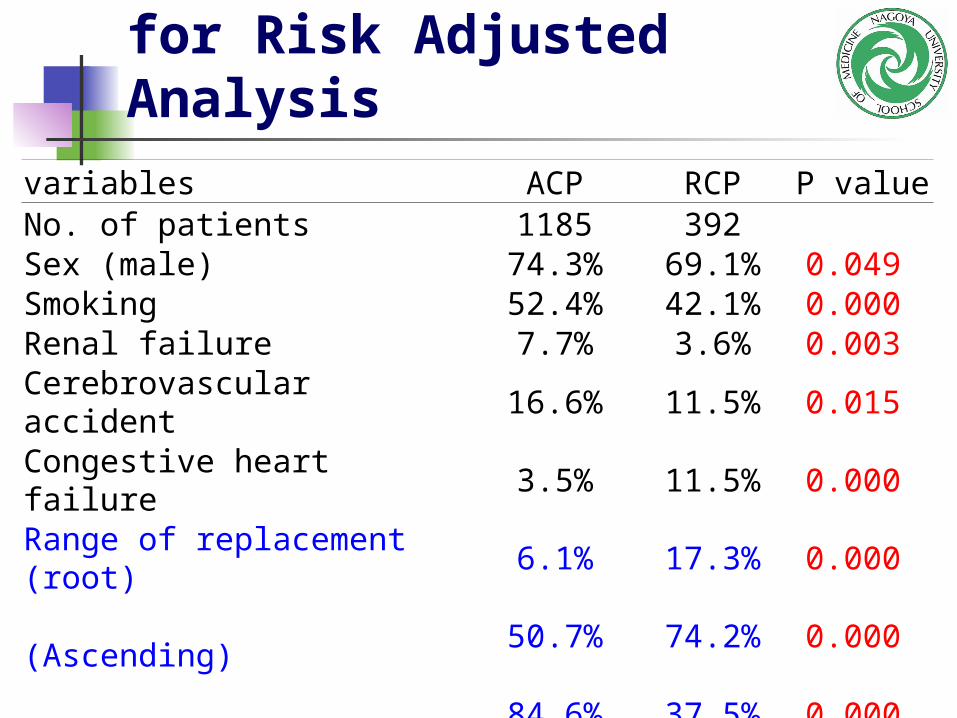
Patients Characteristics for Risk Adjusted Analysis
variables ACP RCP P valueNo. of patients 1185 392 Sex (male) 74.3% 69.1% 0.049 Smoking 52.4% 42.1% 0.000 Renal failure 7.7% 3.6% 0.003 Cerebrovascular accident 16.6% 11.5% 0.015 Congestive heart failure 3.5% 11.5% 0.000 Range of replacement (root) 6.1% 17.3% 0.000 (Ascending)
50.7% 74.2% 0.000
(Arch) 84.6% 37.5% 0.000 Age 71 +/- 9 67 +/- 12 0.000 Annual volume 34 +/-19 39 +/- 23 0.000
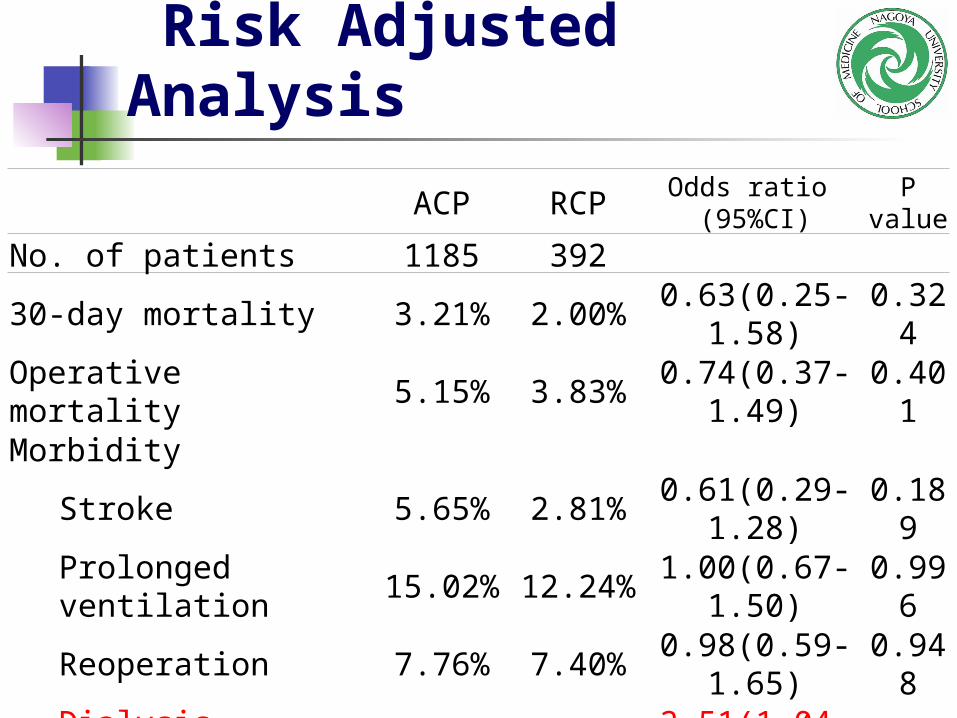
Risk Adjusted Analysis
ACP RCPOdds ratio
(95%CI)P
value
No. of patients 1185 392 30-day mortality 3.21% 2.00% 0.63(0.25-1.58)0.324Operative mortality 5.15% 3.83% 0.74(0.37-1.49)0.401Morbidity
Stroke 5.65% 2.81% 0.61(0.29-1.28)0.189Prolonged ventilation 15.02% 12.24% 1.00(0.67-1.50)0.996Reoperation 7.76% 7.40% 0.98(0.59-1.65)0.948Dialysis required 2.53% 3.06% 2.51(1.04-6.03) 0.04Deep sternal infection 1.69% 1.79% 1.12(0.39-3.24)0.837
Paraparesis 3.29% 2.04% 0.96(0.41-2.28)0.934
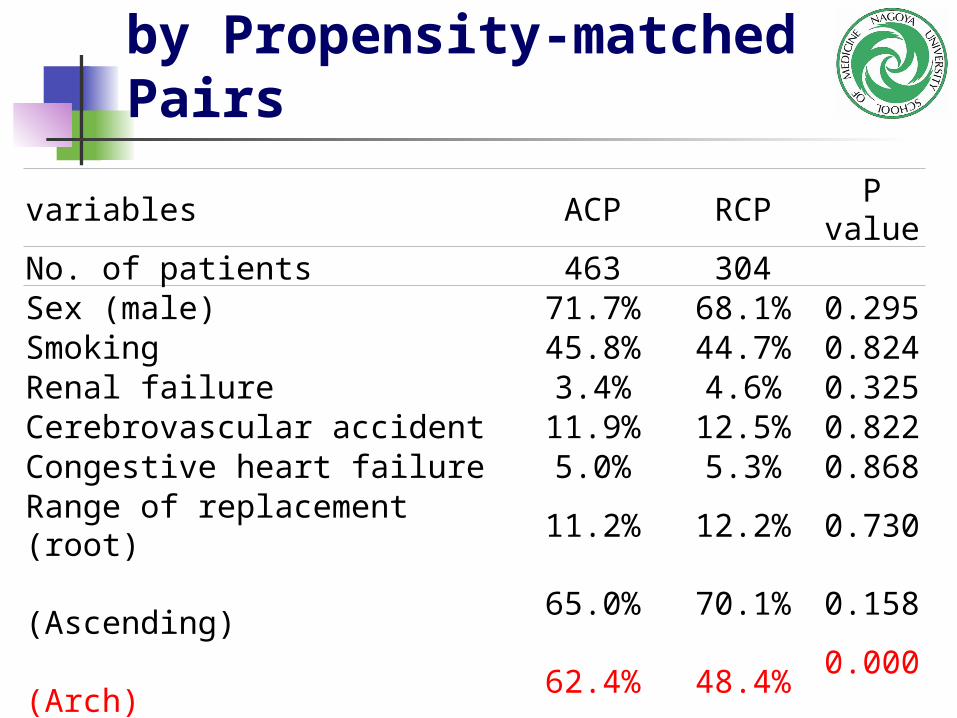
Patient Characteristics by Propensity-matched Pairs
variables ACP RCPP
valueNo. of patients 463 304 Sex (male) 71.7% 68.1% 0.295 Smoking 45.8% 44.7% 0.824 Renal failure 3.4% 4.6% 0.325 Cerebrovascular accident 11.9% 12.5% 0.822 Congestive heart failure 5.0% 5.3% 0.868 Range of replacement (root) 11.2% 12.2% 0.730 (Ascending)
65.0% 70.1% 0.158
(Arch)
62.4% 48.4%0.000
Age 69 +/-10 68 +/- 11 0.253 Annual volume 36 +/- 19 34 +/- 21 0.229

Propensity-matched Analysis ACP RCP Odds ratio (95%CI) P value
No. of patients 463 304 30-day mortality 2.81% 2.30% 0.721(0.28-1.85) 0.497
Operative mortality 3.67% 3.95% 0.991(0.46-2.12) 0.981
Morbidity
Stroke 4.54% 2.96% 0.610(0.27-1.36) 0.228
Transient 3.90% 5.90% 1.536(0.785-3.006) 0.21
Continuous Coma 1.30% 1.00% 0.683(0.168-2.774) 0.594
Prolonged ventilation 13.6% 13.5% 0.939(0.61-1.14) 0.774
Reoperation 7.56% 8.88% 1.129(0.66-1.92) 0.654
Dialysis required 1.30% 3.29% 2.556(0.92-7.13) 0.073
Deep sternal infection 1.10% 1.64% 1.480(0.42-5.17) 0.539
Paraparesis 3.02% 2.30% 0.752(0.30-1.89) 0.543
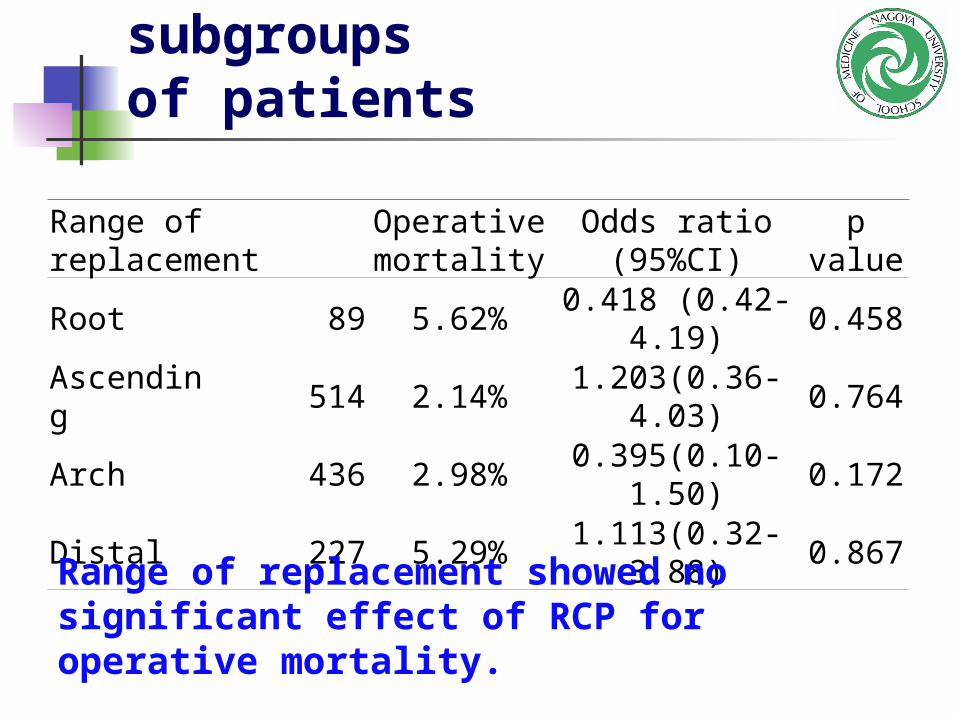
Effect of RCP in subgroups of patients
Range of replacementOperative mortality
Odds ratio (95%CI)
p value
Root 89 5.62% 0.418 (0.42-4.19) 0.458
Ascending 514 2.14% 1.203(0.36-4.03) 0.764
Arch 436 2.98% 0.395(0.10-1.50) 0.172
Distal 227 5.29% 1.113(0.32-3.88) 0.867
Range of replacement showed no significant effect of RCP for operative mortality.

Effect of RCP in subgroups of patients
Cross clamp time (min) < 120 403 3.47% 1.036(0.348-3.083) 0.949>-120 355 4.23% 1.071(0.363-3.158 0.9
Perfusion time (min) <200 421 5.46% 0.891(0.369-2.1519 0.798>-200 337 1.78% 1.457(0.288-7.359) 0.649
Lowest core tempreture ℃ <22 392 3.83% 1.165(0.235-5.772) 0.851>-22 368 3.80% 1.486(0.448-4.937) 0.518
Operation time (min) <400 381 6.30% 0.918(0.376-2.224) 0.851>-400 385 1.30% 1.716(0.282-10.427) 0.558

Effect of RCP for Mortality and Neurologic dysfunction
30 day mortality
Operative mortality
StrokeTransient neurologic dysfunction
Coma
Paraparesis
Risk adjusted analysisPropensity-matched analysis
RCP showed no significant effect for operative mortality and neurologic dysfunction.

Conclusion This is the first clinical study based on a
large scaled database. Both RCP and ACP provide excellent and
comparable clinical outcomes including mortality, stroke and other morbidity.
Brain protection has been applied for aortic arch surgery in reasonable selection criteria in Japan.







