
03-24-2015
Paul D. Rennert
www.sugarconebiotech.com
Immune Checkpoint Inhibitors and the
Evolution of Combinatorial
Immuno-Oncology

sugarconebiotech.com
• The biology and utility of immune checkpoint modulation
drivers and critical issues in the evolution of cancer care
dissociating efficacy from toxicity
• Case study: immune checkpoint inhibitors in melanoma
• Combination immunotherapy
efficacy and toxicity profiles – can we improve both?
combinations with other therapeutic modalities
tumor cells, lymphocytes, the tumor microenvironment
• Future directions and new targets
What we'll cover
2

sugarconebiotech.com
Combinatorial – combination therapy is critical, and not just immune
checkpoint combinations
Pro: agnostic and opportunistic as to type of therapy used in combination
Con: there is currently little data to inform combo treatment choices
Immuno-oncology – the therapeutic approach targets the immune
system
Pro: novel immuno-modulatory targets will broaden the therapy toolkit
Con: we don't know how to sort patients yet, and the choices made may
have unique toxicities
diverse indications with a wide variety of SOC
complex indication subtypes with unique genetics, few other biomarkers
in all cases, unique patients
3
Immune checkpoint therapeutics are a component of
combinatorial immuno-oncology
What does that mean?

sugarconebiotech.com
primers
• cytotoxic
• cytokines
• vaccines
checkpoints
• CTLA4
• PD-1/PD-L1
• TIM3, many others
• other suppressors
expanders
• TNFRs
• cytokines
• CAR-T
• BiTEs
- Tumor cells
- Stromal cells/ECM
- Lymphocytes
- Therapeutics
Big Picture: Immune Checkpoint Modulation
4

sugarconebiotech.com
primers
• cytotoxics
• cytokines
• vaccines
checkpoints
• CTLA4
• PD-1
expanders
• TNFRs
• CAR T
• BiTEs
Idealized picture of combination immunotherapy
5
patient combo

sugarconebiotech.com
Idealized picture of combination immunotherapy
6
combo synergy
• this is what preclinical models show – we cannot
overinterpret those models and acknowledge that
these data only generate clinical hypotheses
• patient by patient analyses show dramatic variability in
genetics, mutation burden, immune profile
• nonetheless, some combinations have already
produced impressive results
sugarconebiotech.com
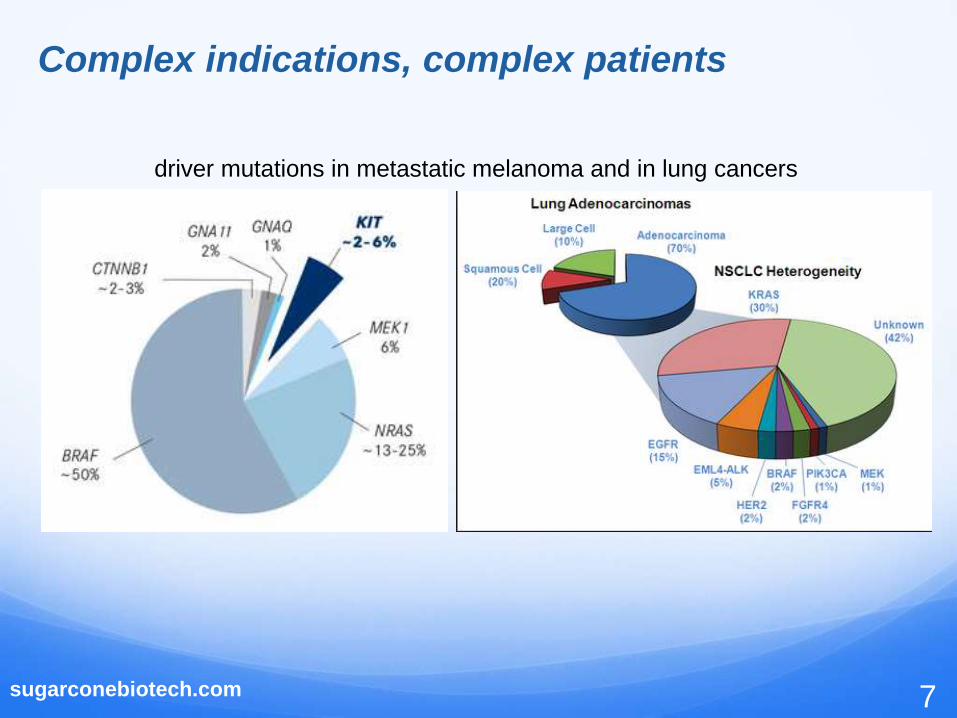
Complex indications, complex patients
7
driver mutations in metastatic melanoma and in lung cancers

sugarconebiotech.com
Complex indications, complex patients
8
expression of lymphocyte markers and PD-L1 in NSCLC
but this picture is highly variable degree of infiltration (starting at none)
geography of infiltration (marginal, interstitial, stromal, excluded)
functionality of infiltrates (PD-1, TIM-3, LAG3)
T cells NK cells
CD3+/CD8+ T cells
sugarconebiotech.com
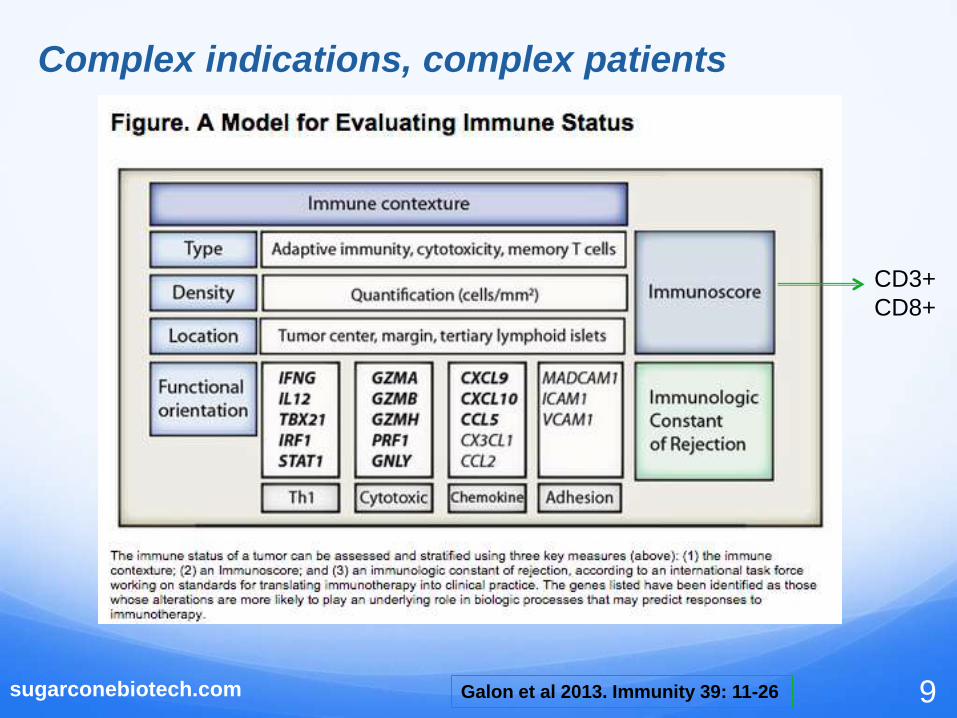
Complex indications, complex patients
9Galon et al 2013. Immunity 39: 11-26
CD3+
CD8+

sugarconebiotech.com
Such compexity offers significant challenge, but also
opportunity, for new drugs to have a positive impact
back to our combinatorial landscape....
10

sugarconebiotech.com
primers
• cytokines
• vaccines
• cytotoxics
expanders
• TNFRs
• CAR T
• BiTEs
Checkpoints Dominate....
11
checkpoints
• CTLA4
• PD-1
• Inhibition appears to be
dominant over activation
Preclinical models support
this view
Early clinical data support this
view, e.g. monotherapeutic
activity of TNFR agonists is
low
Even CAR T cells can be shut
down by immune checkpoint
expression
• We don't yet understand the
impact of removing constraints on
NK cell activity and on immuno-
suppression imposed by stromal
cells

sugarconebiotech.com
primers
• cytokines
• vaccines
• cytotoxics
checkpoints
• CTLA4
• PD-1
• TIM3 etc
expanders
• TNFRs
• CAR-T
• BiTEs
Chemotherapy
Radiation Therapy
Targeted Therapy
other (e.g SCT)
immune modulation does not exist in a vaccuum
12
sugarconebiotech.com
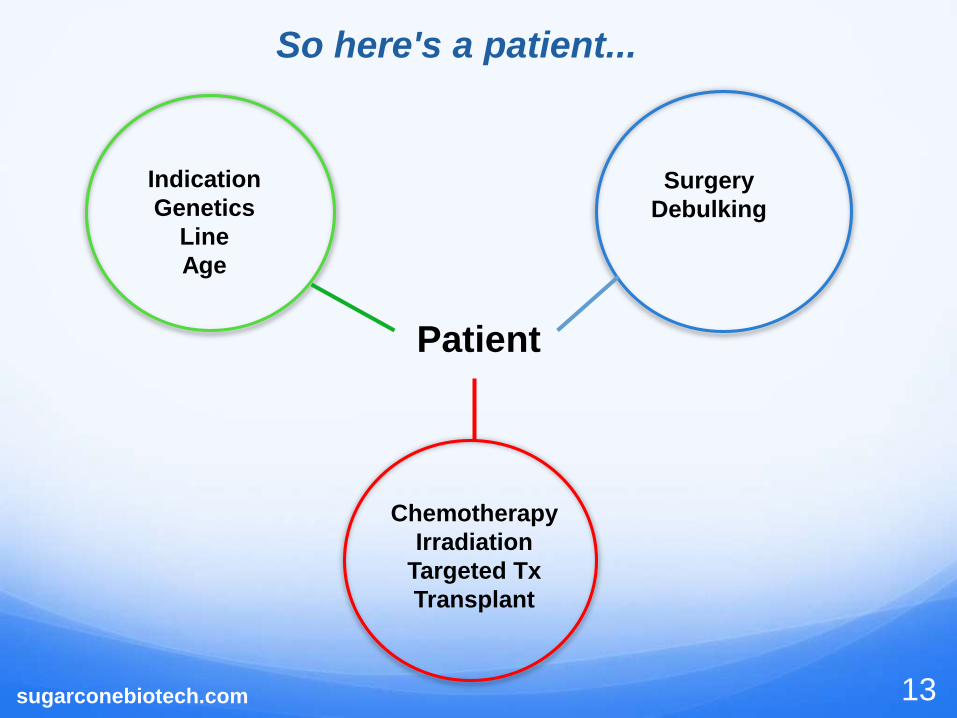
Surgery
Debulking
Chemotherapy
Irradiation
Targeted Tx
Transplant
Indication
Genetics
Line
Age
13
Patient
So here's a patient...

sugarconebiotech.com 14
high
low
low high
Efficacy/Tolerability
Newly diagnosed:
potential for
greatest benefit
Ideal Profile for New Therapeutics
indication
unmet need

sugarconebiotech.com
high
indication
unmet
need
low
low Efficacy/Tolerability high
15
newly
diagnosed
Clinically/Commerically unacceptable
sugarconebiotech.com 16
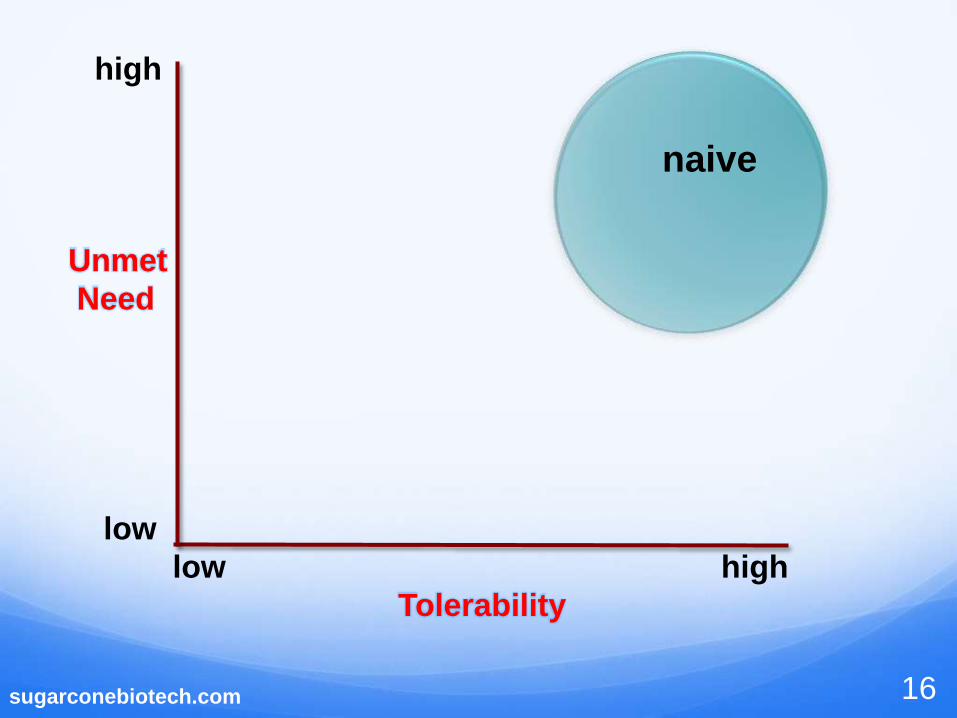
high
Unmet
Need
low
low high
Tolerability
naive

sugarconebiotech.com 17
high
Unmet
Need
low
low high
Tolerability
Ist line

sugarconebiotech.com 18
high
Unmet
Need
low
low high
Tolerability
2nd-3rd line
sugarconebiotech.com 19
high
Unmet
Need
low
low high
Tolerability
last - salvage

sugarconebiotech.com 20
high
Unmet
Need
low
low high
Tolerability
This is a typical early stage
clinical trial population
sugarconebiotech.com 21
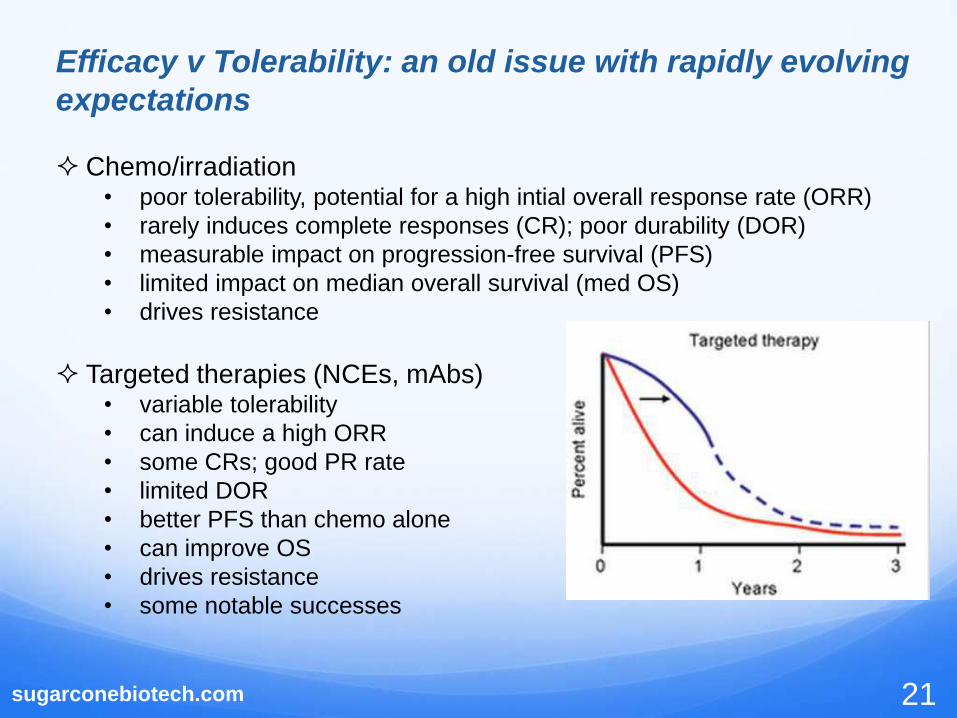
Efficacy v Tolerability: an old issue with rapidly evolving
expectations
Chemo/irradiation • poor tolerability, potential for a high intial overall response rate (ORR)
• rarely induces complete responses (CR); poor durability (DOR)
• measurable impact on progression-free survival (PFS)
• limited impact on median overall survival (med OS)
• drives resistance
Targeted therapies (NCEs, mAbs)• variable tolerability
• can induce a high ORR
• some CRs; good PR rate
• limited DOR
• better PFS than chemo alone
• can improve OS
• drives resistance
• some notable successes

sugarconebiotech.com 22
Efficacy v Tolerability: an old issue with rapidly evolving
expectations
Immunotherapy –
• low ORR, but...
• CRs, PRs and SD with good DOR
• Clear PFS and OS benefit, but let's look more closely...
with immune checkpoint
monotherapy this
number can be low
the long tail
drags OS with it

sugarconebiotech.com 23
Efficacy/Tolerability: where we are headed depends on
the indication
Hematologists have been excited about the "post-chemo" era.
Why? Ibrutinib, rituxumab, idelalisib, revlimid etc ...
Solid tumor oncologists already know from targeted therapies that
some of their patients can be cured (e.g. targeted therapies &
antibodies in breast cancer) – anticipating better cure rates with IO
Oncologists in general are seeing success where for decades there has
been only abject failure (NSCLC, H&N, bladder, etc)
All oncologists recognize the importance of being able to treat their
elderly (or just beaten down) patients
In this landscape, the efficacy/tolerability profile can be
differentiating

sugarconebiotech.com
Next Gen Immuno-Oncology: Central Themes
• what we want in specific indications:
better response rates
more durable responses
better tolerability
• because we are addressing new benchmarks clinical
practice is evolving quickly
• for preclinical and early clinical programs a critical
exercise is to look ahead in an effort to anticipate unmet
need in a rapidly changing environment
24
sugarconebiotech.com
The Big Three
25

www.sugarconebiotech.com
Immunotherapeutics: CTLA-4 and PD-1
Lymph Node "inflammatory site (tumor)
www.sugarconebiotech.com
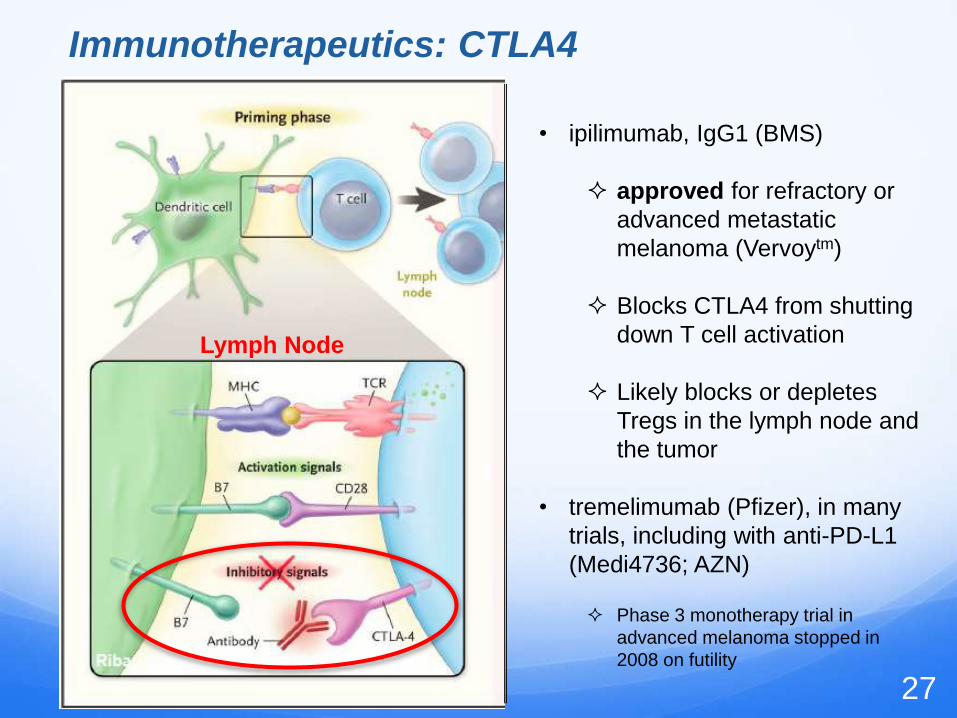
Immunotherapeutics: CTLA4
Lymph Node
• ipilimumab, IgG1 (BMS)
approved for refractory or
advanced metastatic
melanoma (Vervoytm)
Blocks CTLA4 from shutting
down T cell activation
Likely blocks or depletes
Tregs in the lymph node and
the tumor
• tremelimumab (Pfizer), in many
trials, including with anti-PD-L1
(Medi4736; AZN)
Phase 3 monotherapy trial in
advanced melanoma stopped in
2008 on futility
27

www.sugarconebiotech.com
Immunotherapeutics: PD-1
"inflammatory site (tumor)
• anti-PD-1 mAbs
nivolumab, IgG4 (Opdivotm,
BMS)
pembrolizumab, IgG4
(Keytrudatm,Merck)
• anti-PD-L1
MDPL3280A, IgG1 (Roche)
MEDI-4736, IgG1 (AZN)
• These agents block the interaction
of PD-L1 (expressed on tumor
cells and Tregs) with PD-1
expressed on T effector cells
28

anti-PD-1 approvals
Pembrolizumab (Keytruda)
1) Unresectable or metastatic melanoma who no longer respond to other
treatments (September 2014)
Pembrolizumab was granted accelerated approval
Nivolumab (Opdivo)
1) Unresectable or metastatic melanoma who no longer respond to other
treatments (December 2014).
- breakthrough designation, priority review and orphan product designation
- where treatments include Vervoy (ipilimumab) or, if BRAF V600 mutation
positive, a BRAF inhibitor.
2) Advanced/metastatic squamous non-small cell lung cancer (NSCLC) with
progression on or after platinum-based chemotherapy (March 2015)
29sugarconebiotech.com

Melanoma case study
30sugarconebiotech.com

sugarconebiotech.com
Immunotherapy case study: melanoma
31
Historical treatment of stage III/IV non-resectable and/or metastatic
disease (not segmented by mutation status)
ORR med OS 1 yr survival
dacarbazine, other chemo 10-15% 7-9 mo 26-36%
high-dose IL-2 16%* 12 mo n/r
• *A small number patients experience long-term survival. High-dose IL-2
regimen is not more widely used due to toxicity profile.
These IL-2 data supported the hypothesis that melanoma is an immune
responsive cancer.

sugarconebiotech.com 32
Ipilimumab in resistant/advanced melanoma patients
Phase 3, n= 676*
ORR %med OS
(months)
1 yr %
survival
%
progressed
ipilimumab 38** 10 45.6 59
ipi+gp100 20 10.1 43.6 51
gp100 15 6.4 25.3 65
* Hodi et al. 2010. NEJM 363: 711-723; **atypically high

sugarconebiotech.com
Ipilimumab in treatment-naive melanoma
33
ORR %med OS
(months)
1 yr %
survival
comparator data
(prior slide)
20 10 45
ipilimumab 38 13.5 54
* Dummer et al. 2014. J. Transl. Med. 12(Suppl 1):P8.
post-hoc analysis of 4 trials*
• moving to first line modestly improves outcome
• stresses need for combination therapy
• toxicity is a complicating issue, approved dose is 3mpg

sugarconebiotech.com
Ipilimumab plus SOC
34
• ipilimumab plus dacarbazine in adv melanoma*
not better than ipilimumab alone at 1 year
higher dropout rate than monotherapy due to adverse events
med OS 1 yr OS Gr 3/4 AEs
combo 11.2 mo 47.3% 56.3%
dacarbazine 9.1 mo 36.3% 27.5%
* Robert et al. 2011 NEJM 364: 2517-2526

sugarconebiotech.com
Ipilimumab and dacarbazine
35
prior
treatmenttreatment
3 yr %
survival
4 yr %
survival
5 yr %
survival*
Phase 3 (trial '024)
none ipi 10mpg plus
dacarbazine
21.2 19 18.2
" none dacarbazine 12.1 9.6 8.8
Phase 2 ('007, '008, '022)
none ipi 0.3, 3, 10
mpk
- 38 - 49 38 - 49
" yes " - 14 - 28 12 - 28
longer term followup
*JCO published online on February 23, 2015 (Wolchok)ESMO abstracts 2012

sugarconebiotech.com
Toxicity is a complicating issue – why?
36
• biggest issue assocated with these toxicities is treatment discontinuation
(drop-out), leaving patients with an unclear path forward. This has the
effect of lowering therapy penetrance into the patient population.
• anti-PD-1 pathway therapeutics already show better tolerability

sugarconebiotech.com
Check-in: central themes
• better response rates response rate improved
we don't know which patients will respond, and this
remains an issue for the front line setting
• more durable responses some durable responses are obtained
some responders can do remarkably well
• better tolerability better than chemo but toxicity may lead to discontinuation
tolerability is an evolving issue – still trumped by efficacy
37

sugarconebiotech.com
Melanoma and PD-1 pathway inhibitors: nivolumab
38
ORR % med OS1 yr
survival %
pts
progressing
%
nivolumab in pre-
treated patients,
ipi-naive*
41 20.3 63 >55%
nivolumab in
untreated, BRAF
wt patients**
40
not reached
(follow-up up to
16.7 mo)
73 47
dacabazine
control** 14 10.8 42 85
* Hodi, ASCO 2014; ** Robert et al NEJM Nov 2014

sugarconebiotech.com
PD-1 pathway inhibitors: pembrolizumab
39Mahoney and Atkins, 2014 Oncology 28 Suppl 3:39-48
adv/met melanoma
adv/met melanoma
adv/met melanoma

sugarconebiotech.com
PD-1 pathway inhibition
resistant, ipi-refractory metastatic melanoma
40Mahoney and Atkins, 2014 Oncology 28 Suppl 3:39-48
ORR (2 diff
doses)PFS
1 yr
survival
pembro 26-34% 34-38 58-72%
chemo 4 16 26-35%

sugarconebiotech.com
Nivolumab + ipilimumab combination
41Mahoney and Atkins, 2014 Oncology 28 Suppl 3:39-48
• 80% 1 year survival

sugarconebiotech.com
Melanoma summary
42
ORR % med OS 1 yr survival %
where we
started12 8 months 30
ipi/nivo combo 42 40 months 85
best
comparator* 64
not
reached**72
* dabrafenib (BRAFi) + trametinib (MEKi) in BRAF V600E/K
mutated melanoma; Robert et al. NEJM Nov 2014.
** median followup ~10 months

Comparative tox profiles - monotherapy
43Kim and Eder 2014 Oncology

sugarconebiotech.com 44
Tox profiles – combotherapy ipi/nivo
• 21% of patients terminated
treatment due to toxicity
• toxicity is associated with
positive clinical response
• oncologists: the GI tox is very
difficult and limits use
Kim and Eder 2014 Oncology

45
Tox profiles –
BRAF/MEK combo
• grade 3/4 AEs in 48% of pts
• 3 pts died: 2 w/ cerebral
hemorrhage and 1 w/
brainstem hemorrhage
• new tumors (non-
melanoma) developed
in 3 pts
• cardiac abnormalities in 8%
• we'll have to wait for
resistance data

sugarconebiotech.com
Immunotherapy for melanoma: food for thought
46
• Resistance to ipilimumab therapy following radiotherapy includes
upregulation of PD-L1 (Victor et al 2015. Nature, doi:10.1038/nature14292; also
AACR15 abstract #2858)
• Preclinically, anti-CTLA4 and anti-PD-1 therapeutics have been
shown to augment neoantigen responses within TIL populations;
this has important implications for adjacent fields (e.g vaccines)
• BRAF inhibitors transiently release neoantigens that can expand T
cell responses in the presence of immune checkpoint inhibition;
conversely MEK inhibition may blunt T cell activation by direct
effects on T cells (AACR15 Abstract #SY26-03)
• The sequence in which combination therapies are applied has yet to
be optimized – update here?

sugarconebiotech.com
Immunotherapy in other indications
47

BMS declared IO pipeline (March 2015)
48sugarconebiotech.com

sugarconebiotech.com
Ipililumab Phase 3 examples
49
indication combination comparator trial
newly diagnosed
adv melanoma
nivolumab placebo CheckMate 067NCT01844505
adv melanoma nivolumab; dabrafenib*
(BRAFV600); trametinib(MEK)
none, cross-over
design by
sequence
NCT02224781
adv prostate - placebo NCT01057810
sq NSCLC + chemo chemo NCT02279732
adv/met RCC nivolumab sunitinib CheckMate 213NCT02231749
ED-SCLC + chemo chemo NCT01450761
* Rx of melanoma w/1 mo run-in w/vemurafenib (BRAF V600E i) followed by ipilimumab caused grade 3
elevations in aminotransferase levels and concomitant grade 2/3 change in the total bilirubin level: liver
toxicity sufficiently severe to cause study termination (Ribas et al. 2013. NEJM 368: 1365-1366)
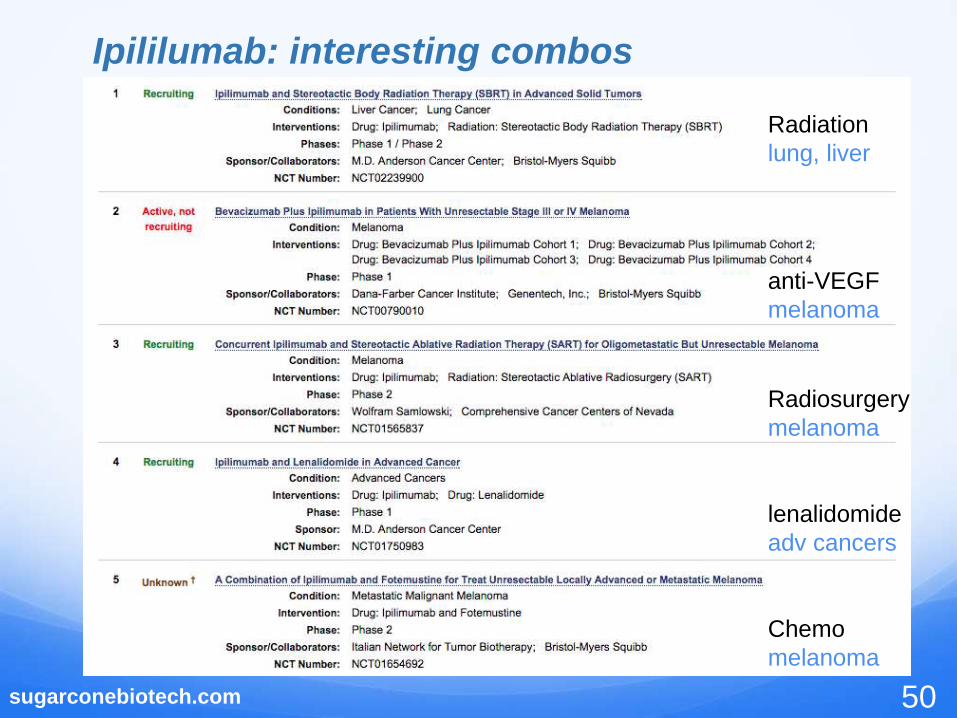
sugarconebiotech.com
Ipililumab: interesting combos
50
Radiation
lung, liver
anti-VEGF
melanoma
Radiosurgery
melanoma
lenalidomide
adv cancers
Chemo
melanoma

sugarconebiotech.com
Ipililumab combos continued
51
imatinib (TKI)
adv cancers
IL-21
melanoma
an RTKi*
renal
radiation
melanoma
* Sunitinib blocks VEGF signaling and it's use is linked to elevated immune responses to solid tumors,
notably RCC. But we have to be careful....a clinical trial of ipilimumab and sunitinib was halted abrupty
due to acute renal failure
sugarconebiotech.com
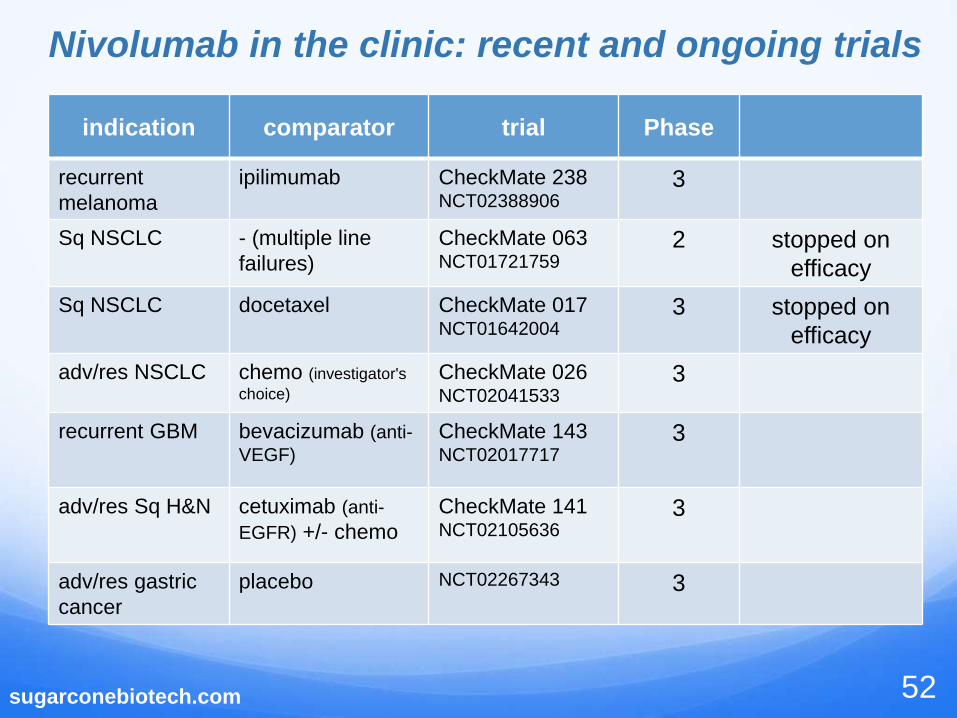
Nivolumab in the clinic: recent and ongoing trials
52
indication comparator trial Phase
recurrent
melanoma
ipilimumab CheckMate 238NCT02388906
3
Sq NSCLC - (multiple line
failures)
CheckMate 063NCT01721759
2 stopped on
efficacy
Sq NSCLC docetaxel CheckMate 017NCT01642004
3 stopped on
efficacy
adv/res NSCLC chemo (investigator's
choice)
CheckMate 026NCT02041533
3
recurrent GBM bevacizumab (anti-
VEGF)
CheckMate 143NCT02017717
3
adv/res Sq H&N cetuximab (anti-
EGFR) +/- chemo
CheckMate 141NCT02105636
3
adv/res gastric
cancer
placebo NCT02267343 3

Nivolumab in the clinic: interesting combos
53
RTK* or ipilimumab
met RCC
Abraxane/Chemo
adv solid tumors
CELG
anti-KIR
heme malignancies
kitchen sink
NSCLC
anti-VEGF
mRCC
sugarconebiotech.com
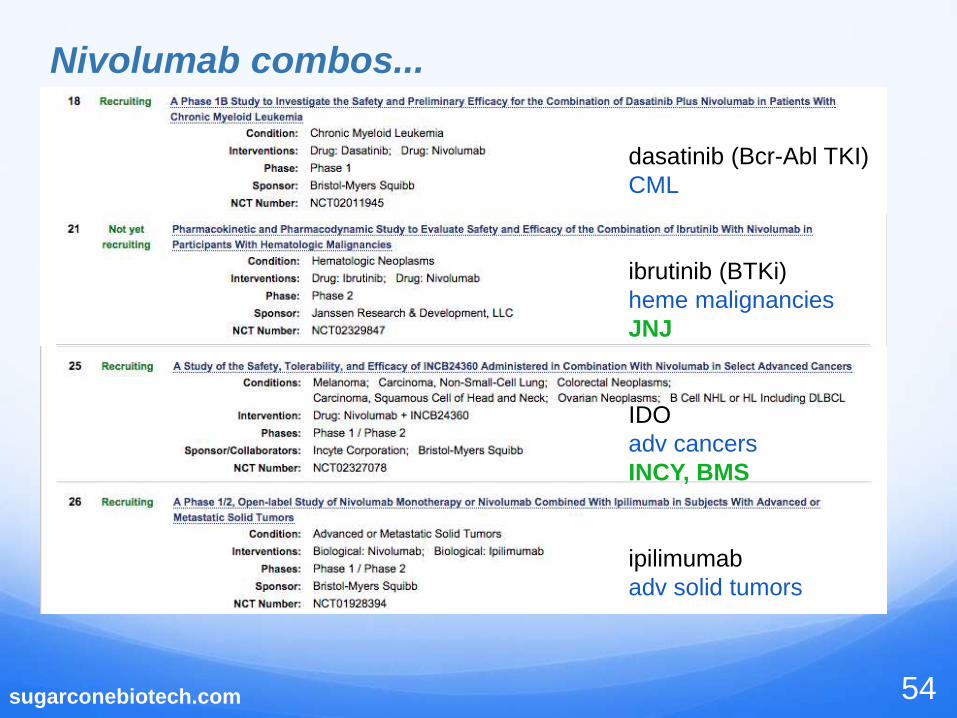
Nivolumab combos...
54
dasatinib (Bcr-Abl TKI)
CML
ibrutinib (BTKi)
heme malignancies
JNJ
IDO
adv cancers
INCY, BMS
ipilimumab
adv solid tumors

sugarconebiotech.com
Nivolumab combos...last page
55
anti-CD27
select adv cancers
Celldex, BMS
ipilimumab
CNS melanoma
dabrafenib +/- trametinib
melanoma

sugarconebiotech.com
Pembrolizumab in the clinic:
Phase 3 and other select examples
56
indicationcombination
or othercomparator trial note
met Sq H&N (1st
line)
chemo cetuximab
(anti-EGFR) +
chemo
Keynote-048NCT0235803 P3
PD-L1+ adv
NSCLC
- chemo Keynote-042NCT02220894 P3
adv melanoma - ipilimumab Keynote-006NCT01866319
P3
adv urothelial
cancer
- chemo Keynote-045NCT02256436 P3
adv/res gastric
adenoCa
- paclitaxel Keynote-061NCT02370498 P3
adv cancers response relative
to tumor PD-L1+- Keynote-001
NCT01295827
P1, NSCLC data at
AACR15 #CT104
mesothelioma - - Keynote-028NCT02054806
P1, data at
AACR15 #CT103

sugarconebiotech.com
Pembrolizumab: example combos
57
VEGFR1/2-Fc
adv solid cancers
post-chemoradiation
NSCLC
Abraxane
NSCLC
Merck, CELG
chemoradiation
pancreatic cancer
RTKi (EGFR/Her2)
NSCLC

sugarconebiotech.com
Pembrolizumab – other indications
58
chemo
CRC
Merkel Cell
HL and DLBCL
bevacizumab(anti-VEGF)
GBM
sugarconebiotech.com
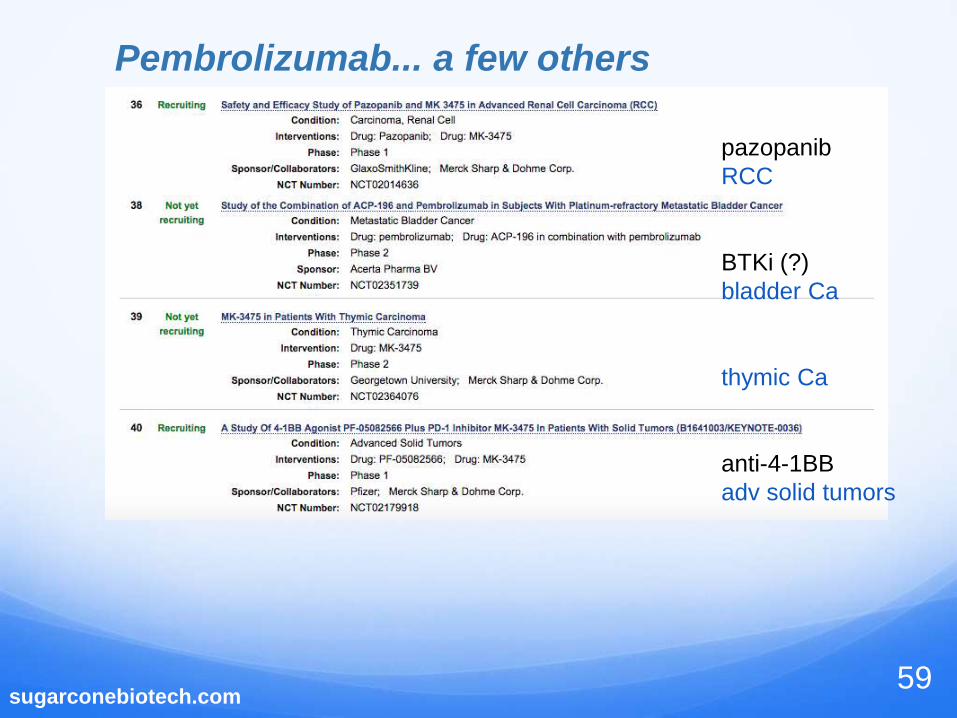
Pembrolizumab... a few others
59
pazopanib
RCC
BTKi (?)
bladder Ca
thymic Ca
anti-4-1BB
adv solid tumors

sugarconebiotech.com
What does this landscape tell us?
• the volume of clinical data will be enormous, difficult to absorb
• immune checkpoint inhibitors to CTLA4, PD-1 and PD-L1 (see
backup slides) are likely to become dominant background
therapeutics in many indications
• the penetrance of these therapeutics into diverse indications will
depend on at least three distinct factors:
immune response profile of the specific indication and further, of
that indication (tumor) in each specific patient (e.g, immunoscore)
mutational profile (oncogenic, antigenic) of the tumor(s) in each
specific patient
efficacy/safety profile of the therapeutic in combination with SOC
or novel therapeutics
the evolving competitive landscape
- as an example, hematologic malignancies may be better served
by other therapeutic modalities
Novel therapeutics will need to fit into this landscape
60

sugarconebiotech.com
A note on PD-L1 inhibition
61
• Anti-PD-L1 inhibitors have the gentlest tox profile of the class, albeit
with less efficacy data behind them, so we'll see...
• updates here?
MEDI4736 (PD-L1)
dabrafenib (BRAFi)
trametinib (MEKi)

www.sugarconebiotech.com
WHAT NEXT?
62

sugarconebiotech.com
Novel Immunotherapies: Organizing Principals
63
Tumor cells Lymphocyte subsets
Microenvironment

www.sugarconebiotech.com 64
which is what is wrong with this
picture:
• Diverse targets
• Inhibitory and activating pathways
• Known and unknown biologies
• Static
• Rationale required for targeting as
mono- or combo-therapy absent
How do you approach this
complexity?
Mahoney et al, NRDD in press
This target list just
keeps growing

sugarconebiotech.com 65
Organizing Principals – Deconstructing the landscape

sugarconebiotech.com 66Mahoney et al. NRDD, in press
Activating pathways of the TNFRSF
• Multiple antibodies in clinical development, none very far advanced
• All appear relatively tolerable, once dose is established
• Although diverse MOA are postulated within this group of receptors, it is
unclear how much the biology will overlap or be affected by FcR-engagement

sugarconebiotech.com 67
4-1BB/CD137
• Co-stimulatory molecule on T cells and NK cells: ligation induces cell activation
and enhances effector function
• Abundant preclinical data support of combination studies with many other
agents
• Clearly capable of driving T cell expansion and memory as demonstrated
(artificially) by the UPenn CAR T program
• Early clinical PD data show expansion of T cell and NK cell subsets and clinical
activity in melanoma, RCC, ovarian Ca (PR and sustained SD)
• 4-1BB expression appears to accurately identify tumor reactive TIL in some
tumor types, such as ovarian cancer*
• On NK cells, FcR-engagement by therapeutic antibodies (rituximab, cetuximab,
etc) strongly upregulates 4-1BB expression, opening the door for rational
combinations**
* Ye et al. 2014. Clin. Can. Res. 20: 44-55
** Khort et al. 2014. JCI 124: 2668-2682

www.sugarconebiotech.com 68
Therapeutics targeting 4-1BB
• Broad campaign by BMS to profile anti-4-1BB agonist activity of urelumab, an
IgG4 agonist
monotherapy: solid tumors and Non-Hodgkin lymphoma (NHL)
rituximab combination for NHL
combination with elotuzumab (anti-CS-1 mAb) or lirilumab (anti-KIR mAb) for
multiple myeloma
nivolumab combination in solid tumors and NHL
cetuximab (anti-EGFR mAb) in colorectal, Head and Neck carcinomas
• Pfizer campaign with PF-05082566, an IgG2 agonist
monotherapy cohorts in melanoma and Merkel cell carcinoma and combination
trials with rituximab in NHL
combination with pembrolizumab in solid tumors
The PFE/MRK deal will bring additional combos

sugarconebiotech.com 69
OX-40/CD134
• OX40L/OX40 pathway sustains the immune response during inflammation,
i.e. during T cell activation, allowing T cell memory to develop
• OX40 engagement can activate memory T cells as well and has diverse
(mainly negative) effects on Tregs
• Early clinical data showed a PD response that included increased numbers of
circulating CD4+ T cells, CD8+ T cells and NK cells
• OX40 plus 4-1BB agonist combination may drive an anti-tumor immune
response by generating CD8+ T cell activity characterized by very high levels
of IFN-g and granzyme B – the super CD8s
We'll come back to look at CD27 in a bit...

sugarconebiotech.com 70Mahoney et al, NRDD, in press
TCR, B7/CD28 and PD-L1/PD-1 clusters
Novel targets:
HHLA2 – TMIGD2
ICOS – agonist
LAG3 – antagonist
VISTA - ?

sugarconebiotech.com 71
HHLA2
• HHLA2 (aka B7H7/B7-H5/B7y): most closely related to butyrophilins
• Putative ligand identified and an inhibitory role postulated
• HHLA2 protein is widely expressed in human cancer*
breast, lung, thyroid, melanoma, pancreas, ovary, liver, bladder, colon,
prostate, kidney, esophagus
In 50 patients with stage I-III TNBC, 56% of patients had high HHLA2 expression
that was significantly associated with regional lymph node metastasis
low level normal expression on epithelial cells (gut, kidney, breast)
• TCGA analysis showed that HHLA2 copy number gains were present in 29%
of basal breast cancers
• No clinical assets developed
* Janakiram et al. Clin Can Res Dec 2014
sugarconebiotech.com 72
LAG3• A CD4 homologue, LAG3 was shown to confer Treg function on transfected
naive CD4+ T cells
• LAG3 binds to the MHCII protein and is required (with CD4) for optimal T cell
activation
• LAG3 overexpression (e.g on anergic T cells and tumor cells) functions as a
negative regulator of T cell response to MHCII-restricted antigen
• Antagonism of both LAG3 and PD-1 can synergistically reactivated
exhausted CD8+ T cells in mouse models
• LAG3/PD-1 gene-deficient mice are highly competent to reject even poorly
immunogenic tumors.
• Several clinical agents in development, no data yet.

sugarconebiotech.com
VISTA
• Normally expressed on hematopoietic cells including myeloid
cells and T cells
• In multiple cancer models VISTA is found at particularly high
levels on tumor-infiltrating myeloid cells
• Appears to be a negative regulator of T cell responses, may
suppress myeloid cell responses in the tumor microenvironment
• Anti-VISTA antibody treatment blunts tumor development even in
the presence of high PD-1 expression
• Antibodies to VISTA are being developed by a private company,
ImmuNext, in collaboration with Johnson&Johnson (JNJ)
73

sugarconebiotech.com
Complicated targets
74

sugarconebiotech.com
Complicated targets
75
Ceacam-1*
Huang et al. 2015. Nature 517: 386-390
Ceacam-1*
• Excellent preclinical data support targeting TIM-3, Ceacam1 and select
components of the LIGHT/HVEM system
• It seems likely that the clinic will teach us more about the activity of the HVEM
and TIM-3 systems than we can learn from mouse modeling – the actual
kinetics and function of pathway components in situ is likely to be critical to
successful targeting

www.sugarconebiotech.com 76
• lets break away, and look
more closely at specific
cell types within the tumor
microenvironment

www.sugarconebiotech.com 77
B7-H3/B7-H4: Poorly understood
biology, B7-H3 is an ADC target
Butyrophilins are widely expressed,
ligands usually unknown, likely that
new targets will be found here
Aberrant and highly variable
expression of TNFRs – ADC targets,
CD30 also a CAR T target
Mahoney et al, NRDD, in press
Immune-modulatory proteins on tumor cells

78Mahoney et al, NRDD, in press
Immune-modulatory proteins on Tregs
• Primary targets: inhibition overrules
activation
• Additional TNFRSF proteins: all of
these are under preclinical and clinical
investigation
• VEGF receptors critical for cross-talk
with stromal cells

sugarconebiotech.com 79
CD27, our third costimulatory TNFR
• CD27 is constitutively expressed on most T effectors and a subset of NK cells
• As postulated for 4-1BB and OX-40, CD27 is important for sustained T cell
activity and the generation of T cell memory; indeed, CD27 is a marker of
memory T cells; CD27 also drives the cytolytic activity of some NK cells
• Celldex has developed varililumab, an anti-CD27 agonist antibody and arly
clinical data from a Phase 1 dose trial in NHL and solid tumors demonstrated
tolerability and some measureable clinical responses
• Listed clinical trials include a combination with nivolumab in solid tumors
Other critical pathways under active investigation:
CD40
GITR
TNFRSF25
DR5/TrailR2

sugarconebiotech.com 80Mahoney et al, NRDD, in press
NK cells: the next wave of immune-modulators

sugarconebiotech.com 81
NK cells: the next wave of immune-modulators
Watch list:
KIRs (Innate Pharma)
LIRs (ILTs)
Siglecs
The PVR/nectin family (TIGIT; Genentech)
C-Type lectins (Innate Pharma)

sugarconebiotech.com 82
KIR-modulators
• Killer inhibitory receptors fall into two subclasses,
the killer cell immunoglobulin-like receptors (KIRs)
C-type lectin transmembrane receptors (eg. NKG families)
• KIR function is regulated through interaction with cell surface HLA
proteins that transduce an inhibitory signal to NK cells.
• lirilumab is an antagonist antibody that binds to the KIR2DL1,2,3
receptors to prevent their inhibitory signaling and increasing NK cell–
mediated killing of HLA-C–expressing tumor cells.
• In a Phase I monotherapy trial in acute myeloid leukemia (AML)
IPH2101/lirilumab had only modest toxicity (grades 1-2) and showed
signs of clinical activity
• A Phase II study of lirilumab in AML is in progress

sugarconebiotech.com 83
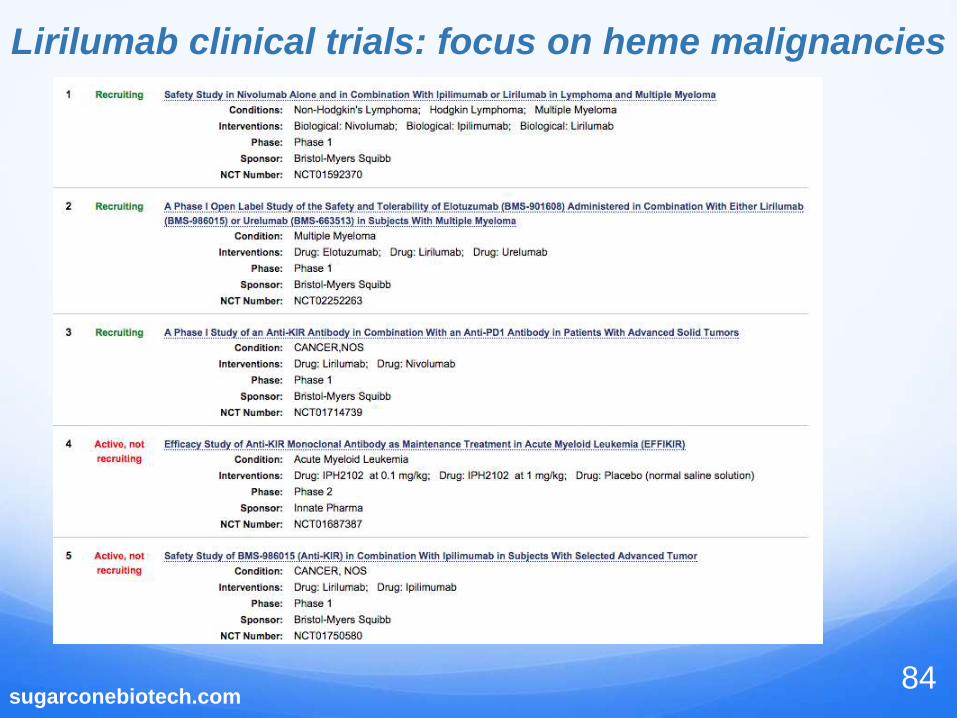
BMS doubles-down with Innate's mAb
• Innate Pharma and BMS are collaborating to develop lirilumab.
• Combination Phase 1 trials of lirilumab in combination with nivolumab and
ipilimumab for solid tumors have begun and a combination trial with
elotuzumab (depleting anti-CS1 antibody from BMS and AbbVie) is underway
for multiple myeloma.
• A recent update to clinical trial filings indicates that BMS is adding lirilumab
combinations with nivolumab to clinical trials of ipilimumab/nivolumab combos
for hematological malignancies (next slide)
• These updates are suggestive of broad utility of engaging NK cell activity
• Innate is also developing an anti-MICA antibody to block inhibition mediated
by MICA/NKG2D interaction, and they have an NKG2A program. Both are
quite early.
sugarconebiotech.com84
Lirilumab clinical trials: focus on heme malignancies

sugarconebiotech.com 85
TIGIT• TIGIT is a relatively new IgSF protein, with clear cell inhibitory function.
• Defined binding to PVR and Nectin-2, potentially leading the way to
influencing both T cells and NK cells through inhibition of this pathway
• However, proteins in the nectin family may have diverse binding partners,
complicating development, e.g. the TIGIT ligands may also bind DNAM and
other PVRs
• Genentech has developed TIGIT-specific therapeutics and recently showed
that co-blockade of TIGIT and PD-L1 resulted in tumor rejection by restoring
the function of exhausted tumor-infiltrating CD8+ T cells; however high
concentration of ADCC-competent antibody was used, complicating
interpretation*
• Regardless, targeting TIGIT may be especially beneficial in tumor settings
where both T cells and NK cells have therapeutic potential
johnston et al. 2014. Cancer Cell
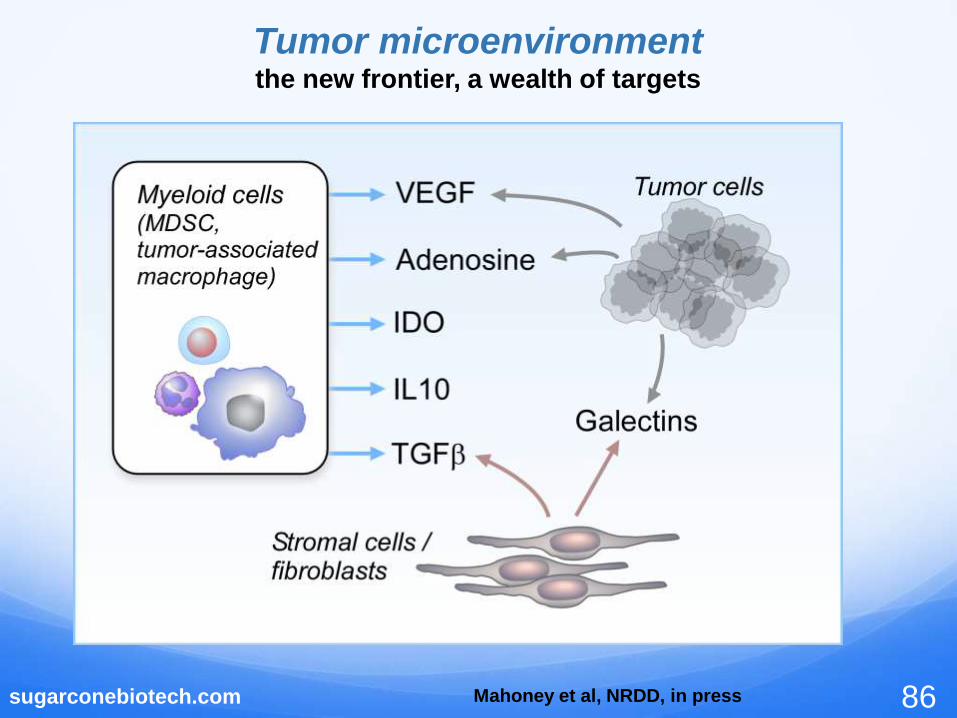
sugarconebiotech.com 86Mahoney et al, NRDD, in press
Tumor microenvironmentthe new frontier, a wealth of targets
sugarconebiotech.com 87
IDO1
Indoleamine 2,3-dioxygenase (IDO1) is the rate-limiting enzyme for the catabolism
cellular tryptophan. High levels of IDO1 reduce tryptophan levels and create
bioactive tryptophan metabolites, a highly immunosuppressive combination
In the tumor microenvironment IDO is produced by tumor cells and by tumor
associated MDSC and tumor-associated macrophages (TAM) in response to
inflammatory signals (IL-10, IFNy)
Incyte's IDO1 inhibitor INCB024360 is in Phase 1 & 2 clinical trials for metastatic
melanoma in combination with ipilimumab and as monotherapy for ovarian cancer.
In the ipilimumab combination study, many patients demonstrated an objective
response and maintained stable disease
Other studies include a Phase 1/2 study in advanced/metastatic cancers including
melanoma and NSCLC in combination with pembrolizumab, nivolumab, MPDL3280A
and MEDI4736 – the benefit of multiple collaborations
Newlink and Flexus deals highlight the intense interest in this target

sugarconebiotech.com88
TGFb• Diverse methods have been employed in attempts to safely block TGFb activity,
one of the most potent immunosuppressive growth factors
• Among many other activities, TGFb stimulates expression and phosphorylation
of IDO. This triggers additional signaling to allow paracrine (and chronic)
expression of both TGFβ and IDO1
• Current therapeutics target activating integrins, e.g. avb6 or the GPCRs that are
responsible for activating the integrins (e.g. LPA, other GPCRs)
• LY2157299/galunisertib is a small-molecule kinase inhibitor from Eli Lilly
designed to selectively block TGFb receptor signaling
• Galunisertib has a well-defined therapeutic window based on reducing receptor
signaling and has shown clinical activity in a variety of solid tumor models
• Successful (safe) targeting of TGFb will be a stunning advance

www.sugarconebiotech.com 89
Adenosine
A2aR is expressed on CD8+ TIL, NK cells and MDSC and is an important
component of immune regulation, helping to stop immune responses in the
context of inflammation
Adenosine is produced by the nucleotidases CD39, an ATP/ADPase, and CD73,
an AMPase. Both nucleotidases can be upregulated on tumor cells and also on
tumor-associated Treg
A proof of concept study using a substrate analog inhibitor of CD73 demonstrated
additive anti-tumor activity with anti-CTLA4 antibody treatment in a melanoma
model
An anti-CD73 antibody had additive activity when combined with anti-CTLA4 or
anti-PD-1 antibodies in multiple tumor models

sugarconebiotech.com 90
adenosine ...
This study demonstrated particularly strong additive activity in the setting of
anti-PD-1 therapy, possibly because adenosine upregulated PD-1 expression
on the target tumor cells.
These two studies focused on the effect of adenosine production and
signaling through A2aR on CD8+ T cells.
Emerging data suggest that A2aR signaling also triggers MDSC to promote
immunosuppression, and that NK cells are negatively regulated via this
pathway

sugarconebiotech.com
• Checkpoints
CTLA4 and PD-1/L-1: crowded, little room for differentiation
although top tier assets are still being sought – not every antibody
is a success (see pidilizumab)
TIM-3, LAG-3: multiple programs underway at large pharma
(NVS) and many small biotechs
Enough deals have been done that some sub-par assets are
sitting on the shelf
• Novel Pathways
What are these? everyone wants one...
Drives steep valuations (e.g. NLNK, Flexus)
How can drug discovery navigate this landscape
91

sugarconebiotech.com
• Vaccines
High value accrues to some programs, but the rules for
success are unknown
Biggest issue: high risk – vaccines fails in Phase 3!
• Immuno-stimulatory Pathways
4-1BB, GITR, OX40 illustrate the tortuous development
pathways these assets can take
Some legacy anti-TNFRs signal non-physiologically
There is room for novel constructs like bispecifics
There are many novel pathways that are under-
represented
How can drug discovery navigate this landscape
92

sugarconebiotech.com
• The optimal efficacy/tolerability paradigm will impact more
and more indications as therapeutics are successful
• Niche indications with high unmet need allow access to
this remarkably competitive landscape
• Novel interrogation points to drive diffferentiation:
T cells: effectors and Tregs
NK cells
The tumor microenvironment
The tumor itself
Moving ahead
93

sugarconebiotech.com
Novel Therapeutics: Organizing Principals
94
Tumor cells Lymphocyte subsets
Microenvironment
• TNFRSF proteins
• KIRs
• C-type lectins
• TGFb
• IDO-1
• Chemokine receptors
• LAG3
• HHLA2
• TIM-3

sugarconebiotech.com96
BACKUPs on PD-L1 antagonists

sugarconebiotech.com
Medi4736 in the clinic
97

sugarconebiotech.com
Medi4736 in the clinic
98

sugarconebiotech.com
Medi4736 in the clinic
99

sugarconebiotech.com
Medi4736 in the clinic
100

sugarconebiotech.com
Medi4736 in the clinic
101

www.sugarconebiotech.com
Medi4736 in the clinic
102

www.sugarconebiotech.com
MPDL3280a in the clinic
103

www.sugarconebiotech.com
MPDL3280a in the clinic
104

MPDL3280a in the clinic
105

sugarconebiotech.com
MPDL3280a in the clinic
106

sugarconebiotech.com
MPDL3280a in the clinic
107







