
INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY
Int. J. Geriatr. Psychiatry 2008; 23: 109–110.
Published online 31 May 2007 in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/gps.1826
RESEARCH LETTER
The fast track day hospital maintaining clinical improvementin community setting
Emma Law*, Neil Prentice and Peter Connelly
Old Age Psychiatry, Murray Royal Hospital, Perth, UK
INTRODUCTION
In a previous article (Prentice et al., 2005) wedescribed the benefits of a fast track day hospital forpeople with dementia, which provides rapid assess-ment and intensive management of behaviour pro-blems. In this follow-up paper we describe a largerdata set and examine the stability of improvementafter discharge.
PATIENTS, METHODS AND PROCESSOF CARE
General practitioners, community psychiatric nurses,and social workers refer patients with dementia andassociated behavioural disorders. Problem behavioursare identified before admission and efforts made eitherat home or in the care home setting to address these.The Day Hospital operates with no waiting list, andaims for patient attendance 2 days per week over 6weeks, with follow up thereafter by Day Hospital staffin the residential setting for a further 6-week period.This means that problem behaviours recurring in thecare setting during the post-discharge period can beidentified and targeted by Day Hospital outreach staffwho have been involved in the comprehensive
*Correspondence to: E. Law, Practice Development Manager of OldAge Psychiatry, Murray Royal Hospital, Muirhall Road, Perth PH27BH, UK. E-mail: [email protected]
Copyright # 2007 John Wiley & Sons, Ltd.
assessment and treatment of the patient during theirattendance period. Flexible attendance arrangementsinclude an effort to involve a carer from the residentialsetting to explain basic principles of psychologicaland behavioural management. Carer involvement isexpected at a planning meeting during week 6 ofattendance. Psychometric assessment has been stan-dardised with development of the model and currentlycomprises the Mini-Mental State Examination(MMSE) (Folstein et al., 1975), and the Neuropsy-chiatric Inventory with Carer Distress Scale (NPI-d)(Kaufer et al., 1998) to include a global cognitivemeasure, a behavioural component, and a measure ofcaregiver distress.Changes in cognition, behaviour, and carer distress
were subjected to statistical analysis using pairedt-tests; all statistical analysis was performed usingSPSS for Windows Version 11.5.
RESULTS
We report here on the care of 169 care episodes. Asthese data were collected as part of routine clinicalpractice we have incomplete data for 56 patients,primarily because of omission of testing, lack ofcompliance or non-attendance. Our group thuscomprises 78 patients undergoing full psychometricassessment at admission, discharge and follow up, anda further 35 for whom we have an incomplete data set.The total group consisted of 59 men (34.9%) and
Received 20 January 2007Accepted 26 March 2007
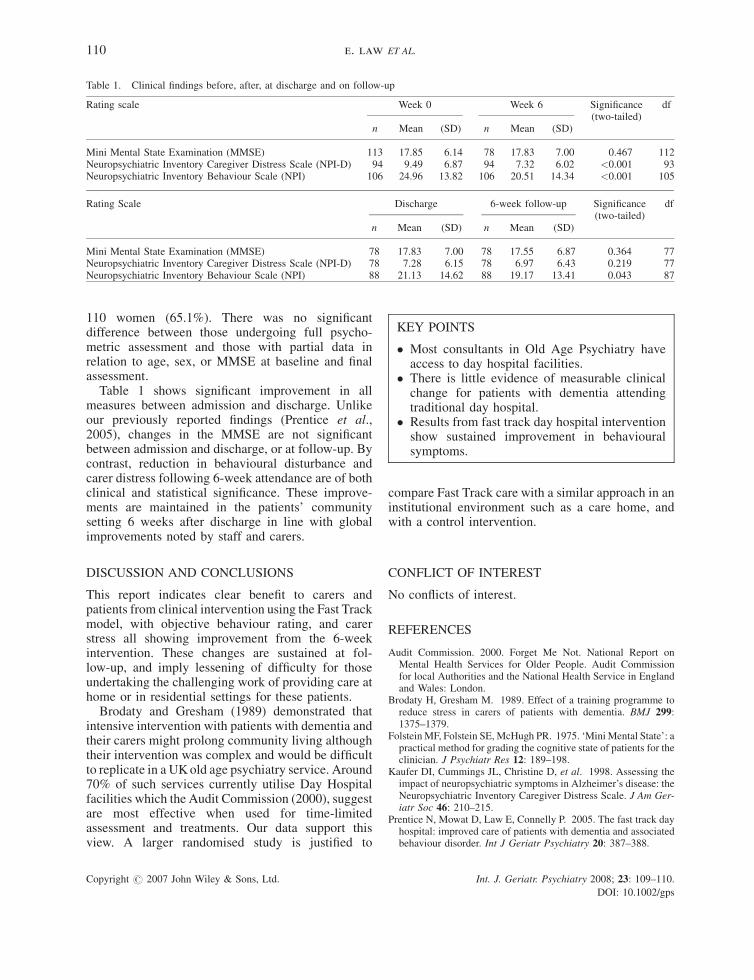
Table 1. Clinical findings before, after, at discharge and on follow-up
Rating scale Week 0 Week 6 Significance(two-tailed)
df
n Mean (SD) n Mean (SD)
Mini Mental State Examination (MMSE) 113 17.85 6.14 78 17.83 7.00 0.467 112Neuropsychiatric Inventory Caregiver Distress Scale (NPI-D) 94 9.49 6.87 94 7.32 6.02 <0.001 93Neuropsychiatric Inventory Behaviour Scale (NPI) 106 24.96 13.82 106 20.51 14.34 <0.001 105
Rating Scale Discharge 6-week follow-up Significance(two-tailed)
df
n Mean (SD) n Mean (SD)
Mini Mental State Examination (MMSE) 78 17.83 7.00 78 17.55 6.87 0.364 77Neuropsychiatric Inventory Caregiver Distress Scale (NPI-D) 78 7.28 6.15 78 6.97 6.43 0.219 77Neuropsychiatric Inventory Behaviour Scale (NPI) 88 21.13 14.62 88 19.17 13.41 0.043 87
KEY POINTS
� Most consultants in Old Age Psychiatry haveaccess to day hospital facilities.
� There is little evidence of measurable clinicalchange for patients with dementia attendingtraditional day hospital.
� Results from fast track day hospital interventionshow sustained improvement in behaviouralsymptoms.
110 e. law ET AL.
110 women (65.1%). There was no significantdifference between those undergoing full psycho-metric assessment and those with partial data inrelation to age, sex, or MMSE at baseline and finalassessment.Table 1 shows significant improvement in all
measures between admission and discharge. Unlikeour previously reported findings (Prentice et al.,2005), changes in the MMSE are not significantbetween admission and discharge, or at follow-up. Bycontrast, reduction in behavioural disturbance andcarer distress following 6-week attendance are of bothclinical and statistical significance. These improve-ments are maintained in the patients’ communitysetting 6 weeks after discharge in line with globalimprovements noted by staff and carers.
DISCUSSION AND CONCLUSIONS
This report indicates clear benefit to carers andpatients from clinical intervention using the Fast Trackmodel, with objective behaviour rating, and carerstress all showing improvement from the 6-weekintervention. These changes are sustained at fol-low-up, and imply lessening of difficulty for thoseundertaking the challenging work of providing care athome or in residential settings for these patients.Brodaty and Gresham (1989) demonstrated that
intensive intervention with patients with dementia andtheir carers might prolong community living althoughtheir intervention was complex and would be difficultto replicate in a UKold age psychiatry service. Around70% of such services currently utilise Day Hospitalfacilities which the Audit Commission (2000), suggestare most effective when used for time-limitedassessment and treatments. Our data support thisview. A larger randomised study is justified to
Copyright # 2007 John Wiley & Sons, Ltd. Int. J. Geriatr. Psychiatry 2008; 23: 109–110
DOI: 10.1002/gp
compare Fast Track care with a similar approach in aninstitutional environment such as a care home, andwith a control intervention.
CONFLICT OF INTEREST
No conflicts of interest.
REFERENCES
Audit Commission. 2000. Forget Me Not. National Report onMental Health Services for Older People. Audit Commissionfor local Authorities and the National Health Service in Englandand Wales: London.
Brodaty H, Gresham M. 1989. Effect of a training programme toreduce stress in carers of patients with dementia. BMJ 299:1375–1379.
FolsteinMF, Folstein SE,McHugh PR. 1975. ‘MiniMental State’: apractical method for grading the cognitive state of patients for theclinician. J Psychiatr Res 12: 189–198.
Kaufer DI, Cummings JL, Christine D, et al. 1998. Assessing theimpact of neuropsychiatric symptoms in Alzheimer’s disease: theNeuropsychiatric Inventory Caregiver Distress Scale. J Am Ger-iatr Soc 46: 210–215.
Prentice N, Mowat D, Law E, Connelly P. 2005. The fast track dayhospital: improved care of patients with dementia and associatedbehaviour disorder. Int J Geriatr Psychiatry 20: 387–388.
.
s







