Download - Technetium-99m-FurifosminintheFollow-Upof
REFERENCES1. Vassilopoulou-SeIlin R, Klein Mi. Smith Ti-I, et al. Pulmonary metastases in children
and young adults with differentiated thyroid cancer. Cancer 1993;71 :1348 —1352.2. Vassilopoulou-Sellin R, Libshitz HI, Haynie TP. Papillary thyroid cancer with
pulmonary metastases beginning in childhood. Clinical course over three decades. MedPediatrOncol 1995;24:l19—122.
3. Hamess JK, Thompson NW, McLeod MK. Pasieka JL, Fukuuchi A. Differentiatedthyroid carcinoma in children and adolescents. World J Surg 1992;16:547—554.
4. WithersEH,RosenfeldL. O'NeilJ,LynchJB,HolcombH. Long-termexperiencewithchildhood thyroid carcinoma. i Pediatr Surg 1979,14:332—335.
5. BuckwalterJA, Gurll NJ, ThomasCG. Cancerof the thyroid in youth. WorldJ Surg198l;5:15—25.
6. Dc KeyserLFM, VanHerleAJ.Differentiatedthyroidcancerinchildren.HeadNeckl985;8:lOO—l14.
7. Tallroth E, Backdahl M, Einhorn J, Lundell G, Lowhagen T, Silfversward C. Thyroidcarcinoma in children and adolescents. Cancer l986;58:2329—2332.
8. La Quaglia MP, Corbally MT. Heller G, Exelby PR. Brennan MF. Recurrence andmorbidity in differentiated thyroid carcinoma in children. Surgen' 1988;104:1 149—I156.
9. Lamberg BA, Karkinen-Jaaskelainen M, Franssilla KO. Differentiated follicularderived thyroid carcinoma in children. Ada Paediatr 1989;78:4l9—425.
10. McConahey WM, Hay ID, Woolner LB. van Heerden JA, Taylor WF. Papillarythyroid cancer treated at the Mayo Clinic, 1946 through 1970: initial manifestations,pathologic findings, therapy and outcome. Mayo Clin Proc 1986;6l :978—996.
I I. Bonte FJ. Radioiodine and the child with thyroid cancer. AiR 1965;96: I—24.12. DeGrootLi, KaplanEL. McCormickM, StrausFH.Naturalhistory,treatmentand
course of papillary thyroid carcinoma. J Clin Endocrinol Mezab 1990;7l:414—424.I3. Clark OH, Duh QY. Thyroid cancer. Med C/in North Am I99 1;75:2 I 1—234.14. Katoch DS, Mehta Di, Somasundaram S. Role of shadow shield whole body counter
in clinical studies. In: Das KR, Gopalkrishnan AK, eds. Proceedings of NationalSeminar on Radiation Protection. Bombay: India: 1976:208 —213.
Is. KnudsonRi, SlakinRC, LebowitzMD, BurrowsB. The maximalexpiratoryflowvolume curve. Normal standards, variability and effects of age. Am Ret' Respir Dis1976;I13:587—600.
16. SamuelAM,UnnikrishnanTP, BaghelNS, RajashekharraoB. Effectof radioiodinetherapy on pulmonary alveolar-capillary membrane integrity. J Nuc/ Med 1995:36:783—787.
I7. lain SC, Mehta SC, Kumar B, Reddy AR, Nagaratnam A. Formulation ofthe referenceIndian adult:anatomic and physiologic data. Health Phvs 1995:68:509—522.
18. Loevinger R, Berman M. A schema for absorbed dose calculation for biologicallydistributed radionuclides. MIRD pamphlet no. I. J Nucl Med 1968;9(suppl l):7—l4.
19. CrileG. Carcinomaofthe thyroidin children.AnnSurg 1959;150:959—964.20. Winship T. Rosvoll RV. Thyroid carcinoma in childhood: final report on a 20 year
study. C/in Proc Child Hosp Wash DC 1970;26:327—347.2 1. Goepfert H, Dichtel Wi, Samaan NA. Thyroid cancer in children and teenagers. Arch
Otolarvngol Head Neck Surg 1984:1 10:72—75.22. Samaan NA, Maheshwari YK, Nader 5, Hill CS, Schultz PN, Haynie TP. Impact of
therapy of differentiated carcinoma of the thyroid: an analysis of 706 cases. J C/inEndocrinolMetab 1983:56:1131—1138.
23. Massin JP, Savoie IC, Gamier H, Guiraudon G, Leger FA, Bacourt F. Pulmonarymetastases in differentiated thyroid carcinoma: study of58 cases with implications forthe primary tumor treatment. Cancer 1984;53:983—992.
24. Samaan NA, Schultz PN, Haynie TP, Ordonez NG. Pulmonary metastases ofdifferentiated thyroid carcinoma: treatment results in 101 patients. J Clin EndocrinolMetab I985;60:376—380.
25. SchlumbergerM,TubianaM,DcVathaireF,et al. Longtermresultsof treatmentof283 patients with lung and bone metastases from differentiated thyroid carcinoma.J C/in Endocrinol Metab I986;63:960—967.
26. Mazzafem EL. Papillary thyroid carcinoma: factors affecting prognosis and currenttherapy.SeminOncol 1987:14:315—332.
27. SissonJC, GiordanoTi, iamadarDA,et al. Iodine-l3l treatmentof micronodularpulmonary metastases from papillary thyroid carcinoma. Cancer 1996;78:2 184 —2192.
patient-by-patient basis and of 91 % (78%—100%)on lesion-bylesion basis for 18F-FDG.The sensitivity of se@@@Tc@furffosminappearsto be poor,evenforcervicaland mediastinaltumormanifestationswhere the value of 20111-chlorideis established.
Key Words technetium-99m-furifosmin; differentiated thyroid carcinoma; fluorine-i 8-fluorodeoxyglucose; PET
J NucI Med 1998; 39:1536-1541
Tec@metium-99m-t'urifosminis a newtechnetium-labeledagent for myocardial perfusion imaging (1—5).It is composedofan equatorial Schiffbase ligand and two transaxial phosphineligands (l,2-bis(dihydro-2,2,5,5-tetramethyl-3(2H)-furanone-4-methyleneamino)ethane and tris(3-methoxy-propyl))phosphine.It is a lipophilic cationic agent (4 ). Rosetti et al. (2 ) describedgood heart uptake without significant washout up to 5 hr.
There is a variety of cardiac perfusion agents with a@glications in oncolo@ical imaging, such as, 201Tl-chloride, mTc..sestamibi and 9@'°'Tc-tetrofosmin(6). The myocardial kineticsof 201T1-chloride, 99mTc@sestamibi, 99mTc..tetrofosmin and99mTcffirifosmin are different (5). In the literature, 201T1-chloride imaging in metastases of differentiated thyroid carcinoma (DTC) is an established method (7—14). Because ofsuperior physical charcteristics of 99mTc and reduced radiationexposure there is a trend to prefer technetium-labeled agents(14—20). None of the approved radiopharmaceuticals has perfect diagnostic accuracy. Therefore, the investigation ofthe newagent 99mTc4.@rifosmin for thyroid cancer imaging seems to bejustified. The uptake-mechanism of99mTc@furifosmin in normal
Tumor scintigraphy with flow tracers, such as 20111-chloride,has anestablished role in the follow-up of differentiated thyroid cancer. Weinvestigated a new tracer, @‘Tc-furifosmin(Technescan Q12,Mallinckrodt Diagnostika, Hennef, Germany), in patients with elevated thyroglobulin levels or sonographic suspicion of lymph nodemetastases or recurrent disease. Methods: In a prospective study,we examined 20 patients with @Tc-furffosmin.Allpatients underwent a 18F-fluorodeoxyglucose (FDG) PET scan of the neck andchest Positive se@@Tc@furffosminfindings were validated by biopsy,1311 scan, CT or 18F-FDG PET examinations. Results: In threepatients with cervical lymph node metastases detected on a planar
@°Tc-furifosminscan, we found a rapid tracer accumulation in thetumor (maximum < 2 mm) and a significant washout in 2 of 3patients after 4 hr. The visual contrast and the tumor-to-nontumorratio was rather poor (average 1.2:1). In 3 additional patients, 3pulmonary and 2 mediastinal lymph node metastases were detected by the @“Tc-furifosminSPECT scan. Two patients weretrue-negative, and in 13 of 18 patients, the tumor could be localizedby ‘8F-FDGPET (10 cervical, 6 mediastinal, 4 pulmonary metastases, 1 bone metastasis); 5 patients were false-negative. In3 of thesefalse-negative cases we could not localize the tumor with otherdiagnostic methods. Two patients had a true-negative PET examination. Conclusion: The statistical analysis of our data onfurifosmin reveals that the sensitivity and 95% confidence interval of33% (11%—56%)on a patient-by-patient basis and of 34% (17%—57%) for the lesion-by-lesion analysis is significantly lower than thesensitivity and 95% confidence interval of 72% (50%—89%)on a
Received Jul. 21, 1997; revision accepted Dec. 19, 1997.Forcorrespondence or reprints contact: K Brandt-Mwnz, MD,Klinikund Poliklinikfür
Nuk1earmed@in,UniversitätsldinikumEssen, HUfelandtr.55, D-45122 Essen, Germany.
1536 THE JOURNALOFNUCLEARMEDICINE•Vol. 39 •No. 9 •September 1998
Technetium-99m-Furifosmin in the Follow-Up ofDifferentiated Thyroid CarcinomaK. Brandt-Mainz, S.P. MUller, W. Sonnenschein and A. BockischKlinik und Po!ik!inikflir Nuklearmedizin, Universitätsk!inikum Essen, Essen, Germany
.PatienthlgTumorno.HistokgyNM location 1311 Hlatokgy Sono CT Supp Stim
1 Pap T2NOMO Pos
TABLE IPatient Characterizationand ClinicalData
13 62Cet@tNegnaPosMedNegnaNegPulmNegnaNeg2EosinT3NOMOCervnaPosPosPosMednaPosPosPuImnanaPos3PapT4aN1aMOCerv
MedPuImna
nanana
nanaNegna
nana4EosinT3aNOM1Cent
MedPuImna
nanana
naPosNegP05
NegPos5
6Pap PapT4bN1bMOT4aN1aMOCerv
MedPuImCervMedPuImPos
NegNegPosNegNegna
nana
PosnanaPos
PosP05
NegNegNegNeg
Neg7PapT2aNOMOCerv
MedPuImNeg
NegNegPos
nanaPosPos
NegNeg8PapT4bN1bMOCon,
MedPulmNeg
PosNagna
nanaNegNag
PosPos9EosinT2aNOMOCan,
MedPulmNag
PosNagna
nanaNagNag
PosPosPapT3aNOMOCerv
MedPulmNag
NagNagPos
nanaPosPos
NagNagPapT2bNOMOCent
MedPuImNag
NagNagna
nanaPosNag
NagNagPap
FoIlT4bN1bM1 T4aNOMOCent
MedPulmCervMedPulmBoneNag
NagNagNagNagNagNagna
nanananananaNag
NagNag
NagP05NagNagNag
NagEosinT2aNOMOCan,
MedPuImNag
NagNagna
nanaNagNag
NagNagPapT1aN1aMOCerv
MedPuImNag
NagNagna
nanaPosNag
NagNagPap
Pap
Pap
PapT4bN1bM1
T4aNOMO
T2bN1aMO
T4aN1aMOCerv
MedPuImCervMedPuImCervMedPuImCentMedPulmNag
NagNagNagNagNagNagNagNagNagNagNagna
nana
PosnanananananananaNag
Pos
Nag
NagNag
NagNagPosNagNagnanana
NagPos
PosPapT4aN1aMOCerv
MedPuImNag
NagNagna
nanaPosNag
PosNag
<1.0 <1.0
8 117
211 na
42 344
<1.0 <1.0
6.3 24
89 365
na 11
22 na
<1.0 7.4
4 13
8.1 44
9.3
<1.0 4.8
4.5 81
27 655
9 28
na 780
<1.0 1.6
10
11
12
13
14
15
16
17
18
19
20
Pap = papillary;FoIl= follicularEosin = eosinophilic;Cerv = cervical;Med = mediastinal;Puim = pulmonary;Neg = negative;Pos = positive;na =not available.
TECHNETIUM-99M-FURIFOSMIN IN THYROID CANCER •Brandt-Mainz et al. 1537
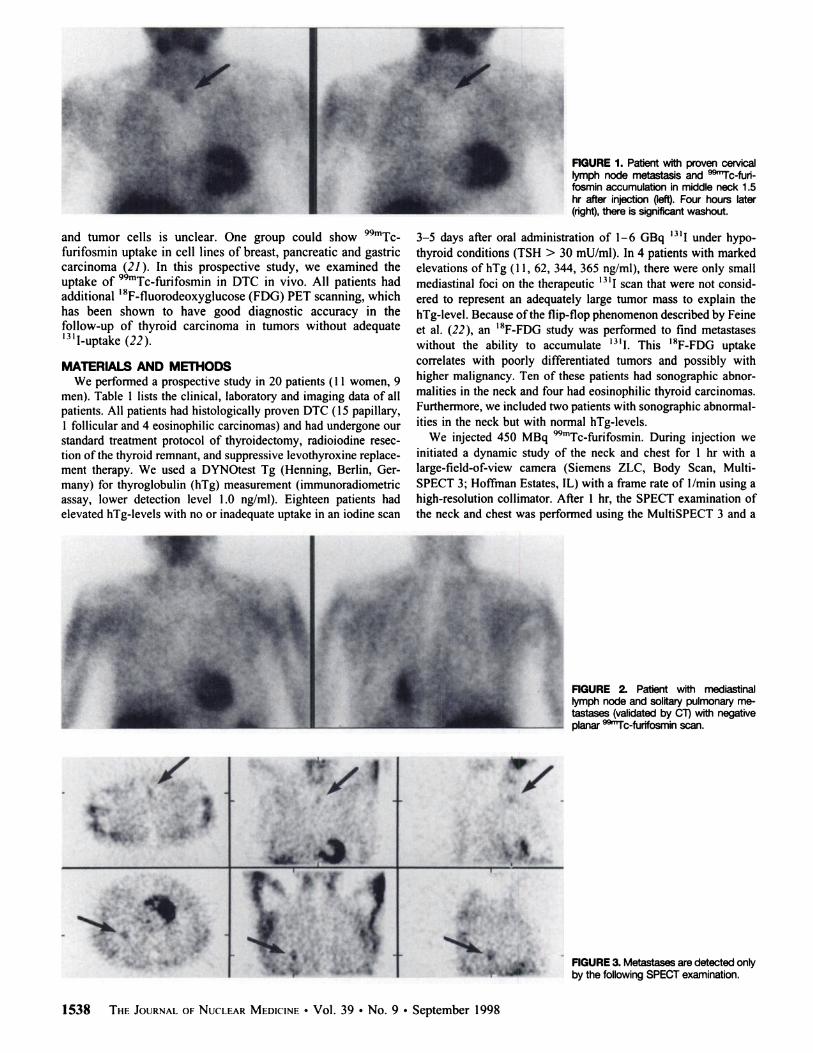
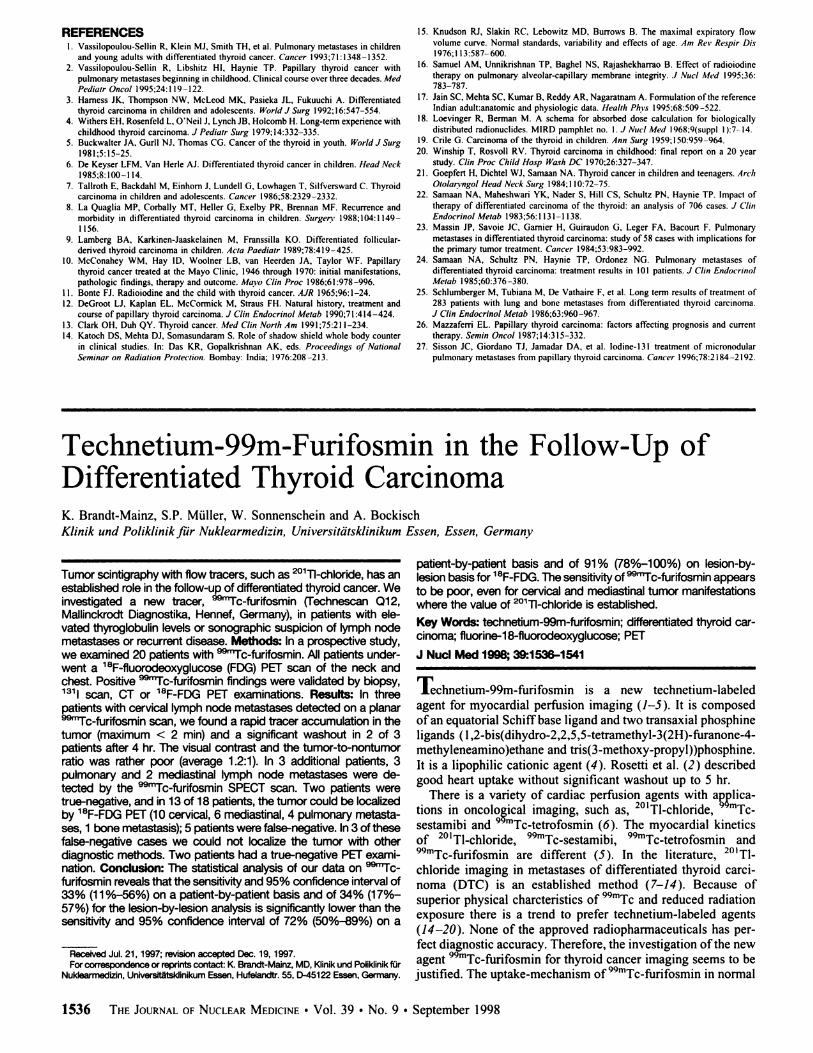
FiGURE1. Patient with proven cervk@allymph node metastasis and @Tc-funfosmin accumulation in middle neck 1.5hr after injection(left).Four hours later(right), there is significant washout.
3—5days after oral administrationof 1—6GBq ‘@‘Iunder hypothyroid conditions (TSH > 30 mU/ml). In 4 patients with markedelevations of hTg ( 11, 62, 344, 365 ng/ml), there were only smallmediastinal foci on the therapeutic 1311scan that were not considered to represent an adequately large tumor mass to explain thehTg-level. Because ofthe flip-flop phenomenon described by Feineet al. (22), an ‘8F-FDGstudy was performed to find metastaseswithout the ability to accumulate 1311. This ‘8F-FDGuptakecorrelates with poorly differentiated tumors and possibly withhigher malignancy. Ten of these patients had sonographic abnormalities in the neck and four had eosinophilic thyroid carcinomas.Furthermore, we included two patients with sonographic abnormalities in the neck but with normal hTg-levels.
We injected 450 MBq o9mTcffirifosmin During injection weinitiated a dynamic study of the neck and chest for 1 hr with alarge-field-of-view camera (Siemens ZLC, Body Scan, MultiSPECT 3; Hoffman Estates, IL) with a frame rate of 1/mm using ahigh-resolution collimator. After 1 hr, the SPECT examination ofthe neck and chest was performed using the Mu1tiSPECT 3 and a
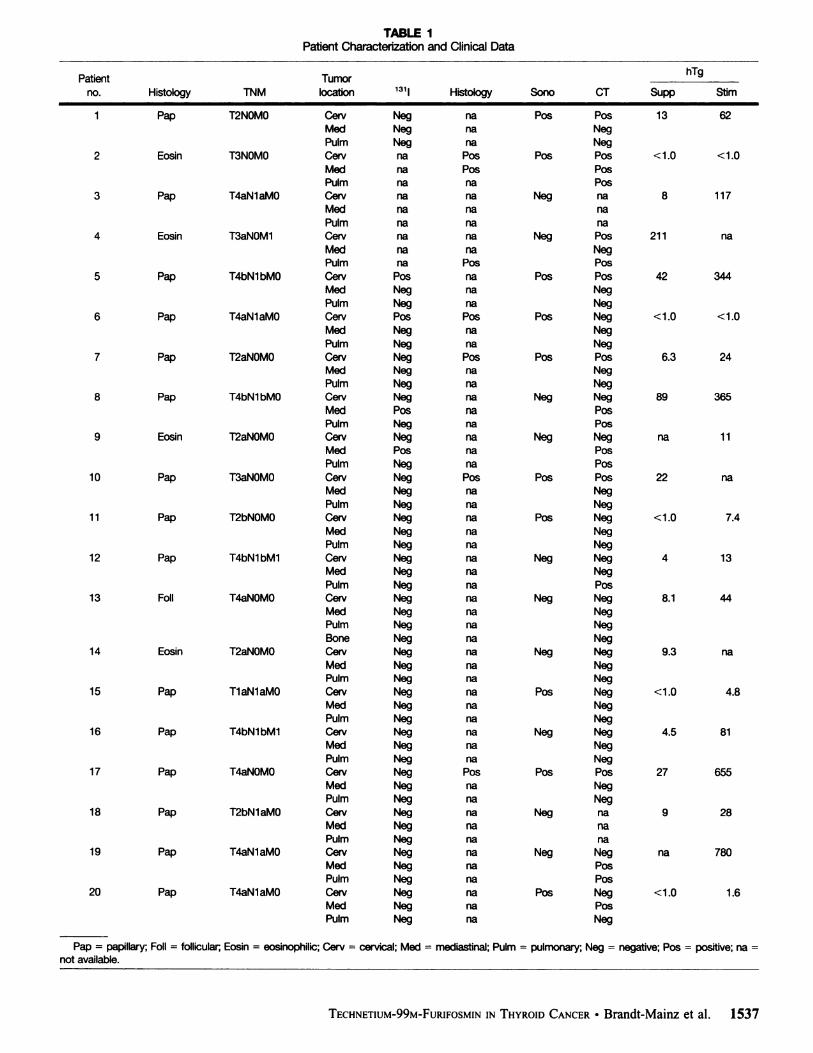
FiGURE 2. Patient with mediastinallymph node and solitary pulmonary metastases (validatedby CT)with negativeplanar @c-furifosminscan.
FIGURE3. Metastases are detected onlyby the followingSPECTexamination.
1538 THE JOURNALOF NUCLEARMEDICINE•Vol. 39 •No. 9 . September 1998
. ... @*‘
and tumor cells is unclear. One group could show 99mTc@furifosmin uptake in cell lines of breast, pancreatic and gastriccarcinoma (21 ). In this prospective study, we examined theuptake of 99mTcf.@rifoSmin in DTC in vivo. All patients hadadditional I8F-fluorodeoxyglucose (FDG) PET scanning, whichhas been shown to have good diagnostic accuracy in thefollow-up of thyroid carcinoma in tumors without adequate‘311-uptake(22).
MATERIALS AND METhODSWe performed a prospective study in 20 patients (1 1 women, 9
men). Table I lists the clinical, laboratory and imaging data of allpatients. All patients had histologically proven DTC ( 15 papillary,1 follicular and 4 eosinophilic carcinomas) and had undergone ourstandard treatment protocol of thyroidectomy, radioiodine resection of the thyroid remnant, and suppressive levothyroxine replacement therapy. We used a DYNOtest Tg (Henning, Berlin, Germany) for thyroglobulin (hTg) measurement (immunoradiometricassay, lower detection level 1.0 ng/ml). Eighteen patients hadelevated hTg-levels with no or inadequate uptake in an iodine scan
.4.- ,.
a'
@ :@ @i
k: V
4,4.,
Cer@i= cervical;Med= mediastinal;Plum = pulmonary;Nag = negative;Pos = positive;na = not available.
TABLE 2Comparison Between Technetium-99m-Furifosmin Planar andSPECT to fluorine-i 8-FDG Using a Lesion-by-Lesion Analysishigh-resolution
collimator. Data were acquired in I83 projectionsover 360°,30 sec/projection/image in a 128 X 128 matrix. Thetransverse images were reconstructed by filtered backprojectionwith a Shepp-Logan-Hanning filter with a cutoff of 0.5 pix I@After 1.5 and 4 hr postinjection all patients had a whole-body scan
.using a dual-head gamma camera (Siemens Body Scan) with ahigh-resolution collimator. The scan speed was 10 cm per mm.
All patients had a PET examination with ‘8F-FDGafter overnight fasting (Siemens/CTI ECAT 953/15); none of our patientswere diabetic. After a transmission scan (8—12mm/bed position),350 MBq ‘8F-FDGwere injected intravenously and 30 mmpostinjection scans of the neck and chest were acquired in 6 bedpositions because of the limited field of view of our PET scanner(5.4 cm). Images were reconstructed by filtered backprojectionwith a Hanning filter (cutoff 0.5 pix I)•In most cases,thePatient
Tumor Furifosmin Furifosminno. location planar SPECTFDG1
Cerv Nag Nag PosMed Nag Nag NagPulm Nag Nag Nag
2 Cerv Pos Pos PosMed Nag Nag PosPulm Nag Nag Nag
3 Cars, Nag Nag NagMed Nag Nag NagPuIm Nag Nag Nag
4 Can, Nag NagPosMedNag Nag Nag99mTc-furifosmin scan and the@ 8F-FDG PET study wereperformedPuImNag Pos Pos
5 Cerv Nag Nag PosMed Nag Nag NagPuIm Nag Nag Nag
6 Cervi Pos Pos PosCerv2 Nag NagMed Nag Nag NagPuIm Nag Nag Nag
7 Cerv Nag Nag Poswithin
1 wk. Four weeks was the longest interval between the twostudies and occurred in one patient.
All 99mTc@furifosminand@ 8F-FDG PET scans were read mdcpendently by two experienced observers blinded to the clinicaldata. All scans were interpreted visually for focal or diffuseanomalities. The positive findings were validated by surgery in 7 of13 cases (5 cervical lymph node mctastases, 1 mediastinal lymphnode metastasis and 1 pulmonary metastasis). In the other 6casesMed
Nag Nag Posthe presence of tumor was confirmed by CT examination withaPulmNag Nag Naghigh-resolution technique of the neck and thechest.8
Cerv Nag Nag NagMed Nag Pos PosPulml Nag Pos PosPulm2 Nag Pos Pos
9 Cerv Nag Nag NagMed Nag Pos NagPulm Nag Nag Nag
10 Cerv Pos Pos PosWe
calculated the sensitivity for 99mTc@furifosminin planar andSPECT technique and for the ‘8F-FDGPET examinations on apatient-by-patient basis and on a lesion-by-lesion basis. We calculated 95% confidence intervals for the sensitivities from thebinomial distribution and compared the sensitivity of 99mTc@furifosmin and 18F-FDG PET with each other and with valuesreported in theliterature.Med
Nag NagNagPulmNag NagNag1
1 Ceni Nag NagNagRESULTSMedNag Nag Nag
PuIm Nag Nag Nag12 Ceoi Nag Nag Nag
Med Nag Nag NagPuIm Nag Nag Nag
13 Cerv Nag Nag NagMed Nag Nag NagPuIm Nag Nag NagBone Nag Nag PosIn
the dynamic scans, we found a rapid tracer accumulation inthe tumor (peak < 2 mm); over 4 hr there was a noticeablewashout in 2 of 3 patients (Fig. I).
In three patients the planar 99mTc..furifosmin scan showedlymph node metastases, which were validated by surgery; 1patient had eosinophilic and 2 patients papillary carcinomas.From the positive patients, 2 had hTg-levels under the detectionlimit and 1 had an elevated hTg of 22 ng/ml under TSH
14 Cerv Nag Nag Nagsuppressive levothyroxine medication. In the SPECT examinaMed Nag Nag NagPulm Nag Nag Nag
15 Cent Nag Nag NagMed Nag Nag NagPulm Nag Nag Nag
16 Cer@, Nag Nag PosMed Nag Nag NagPuIm Nag Nag Nag
17 Cerv Nag Nag PosMed Nag Nag Postion
we found tumors (2 eosinophilic and I papillary carcinoma) in 3 additional patients, I with a mediastinal lymph nodeand nodular pulmonary metastases (Figs. 2 and 3), 1 withmediastinal lymph node and 1 patient also with a nodularpulmonary metastasis. One of these patients was validated bysurgery and the other two by CT. Two patients had a truenegative Tc-fL@rifosminscan.
In 13 patients the I8FFDG scan was positive with thefollowing tumor locations. We found 10 cervical lymphnodePuIm
Nag Nag Nagmetastases, 6 mediastinal metastases, 4 pulmonarymetastases18Can, Nag Nag NagMed Nag Nag NagPulm Nag Nag Nag
19 Cerv Nag Nag NagMed Nag Nag PosPulm Nag Nag Pos
20 Ceni Nag Nag NagMed Nag Nag PosPuIm Nag Nag Nagand
I bone metastasis. Six cervical lymph node metastases and1 pulmonary metastasis were validated by surgery, the otherpatients by CT with high-resolution technique. In 2 patients
@thonly stimulated elevated hTG-levels both the 18F-FDG PETand the @°@Tc-furifosminexamination were true negative.
In 5 of 18 patients the PET scans were false-negative. Allpatients had elevated hTg-levels (stimulated hTg 11—117 ng/ml). In 3 of these 5 false-negative patients no other diagnosticmodality was able to locate a tumor. In one false-negativepatient we found a mediastinal lymph node metastasis and in
TECHNETIUM-99M-FURIFOSMININ THYROIDCANCER •Brandt-Mainz et al. 1539
,r@4
@v,y@,
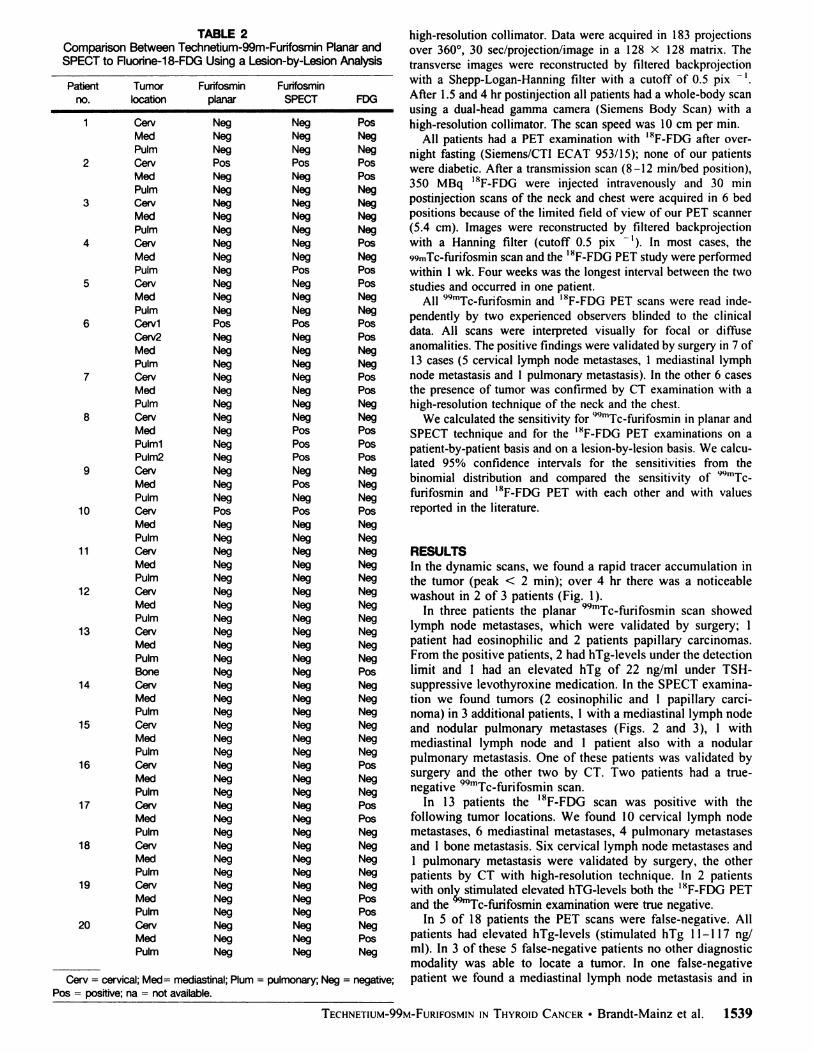
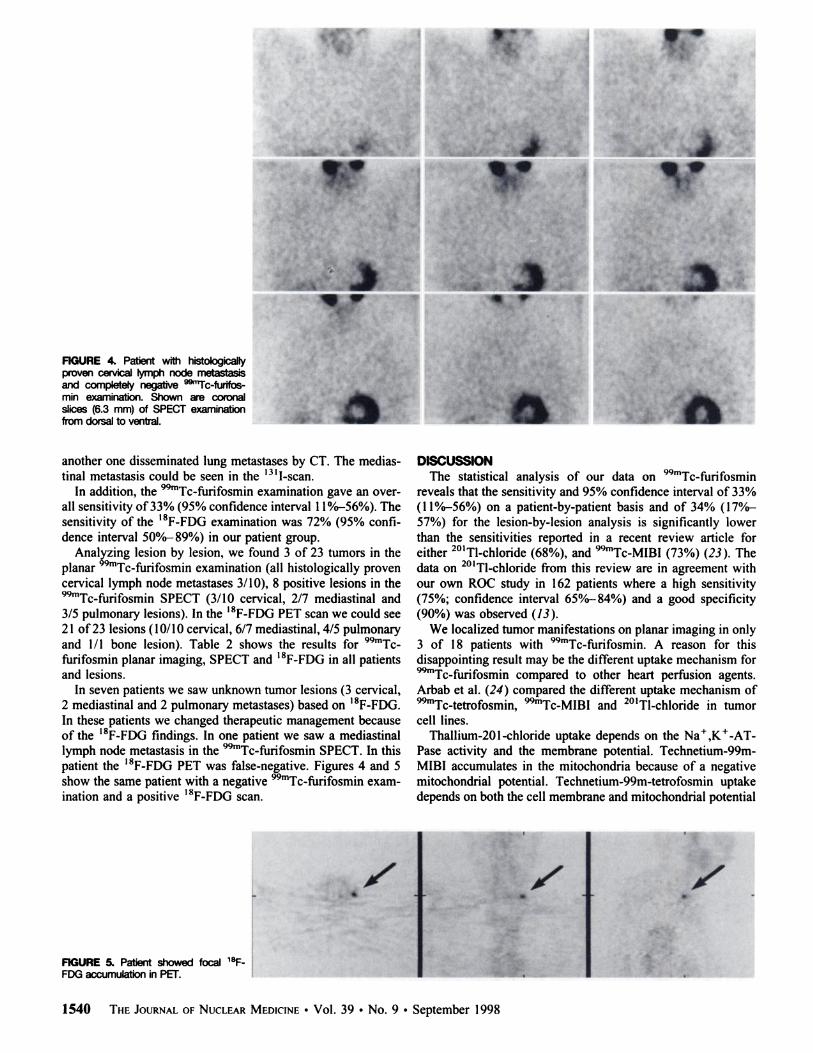
FIGURE 4. Patient wfth histokgIcallyproven cervical lymph node metastasisand completely negative @Tc-furifosmm examination. Shown are coronalslices (6.3 mm) of SPECT examinationfromdorsal to ventral.
another one disseminated lung metastases by CT. The mediastinal metastasis could be seen in the 13‘I-scan.
In addition, the 9@Tc-furifosmin examination gave an overall sensitivity of33% (95% confidence interval 1l%@56%).Thesensitivity of the ‘8F-FDGexamination was 72% (95% confidence interval 5O%—89%) in our patient group.
Analyzing lesion by lesion, we found 3 of 23 tumors in theplanar 99mTc$.@rifosmin examination (all histologically provencervical lymph node metastases 3/10), 8 positive lesions in the9@Tc-furifosmin SPECT (3/10 cervical, 2/7 mediastinal and3/5 pulmonary lesions). In the ‘8F-FDGPET scan we could see2 1 of23 lesions ( 10/10 cervical, 6/7 mediastinal, 4/5 pulmonaryand 1/1 bone lesion). Table 2 shows the results for 9@°'Tcfurifosmin planar imaging, SPECT and ‘8F-FDG in all patientsand lesions.
In seven patients we saw unknown tumor lesions (3 cervical,2 mediastinal and 2 pulmonary metastases) based on ‘8F-FDG.In these patients we changed therapeutic management becauseof the ‘8F-FDGfindings. In one patient we saw a mediastinallymph node metastasis in the 9@Tc-furifosmin SPECT. In thispatient the ‘8F-FDG PET was false-negative. Figures 4 and 5show the same patient with a negative @Tc-furifosminexamination and a positive ‘8F-FDGscan.
FIGURE 5@Patient showed focal @FFDG accumulation in PET.
DISCUSSIONThe statistical analysis of our data on 99mTc..f.@rifosmin
reveals that the sensitivity and 95% confidence interval of 33%(1 1%—56%)on a patient-by-patient basis and of 34% (l7%—57%) for the lesion-by-lesionanalysis is significantly lowerthan the sensitivities reported in a recent review article foreither 201Tl-chloride (68%), and 99mTc..MIBI (73%) (23). Thedata on 201Tl-chloride from this review are in agreement withour own ROC study in 162 patients where a high sensitivity(75%; confidence interval 65%—84%) and a good specificity(90%) was observed (13).
We localized tumor manifestations on planar imaging in only3 of 18 patients with 9@Tc-furifosmin. A reason for thisdisappointing result may be the different uptake mechanism for99mTcf..@fosmin compared to other heart perfusion agents.Arbab et al. (24) compared the different uptake mechanism of99mTc..tetrofosmin @°@Tc-MIBIand 201T1-chloride in tumorcell lines.
Thallium-20l-chloride uptake depends on the Na@,K@-ATPase activity and the membrane potential. Technetium-99m-MIBI accumulates in the mitochondria because of a negativemitochondrial potential. Technetium-99m-tetrofosmin uptakedepends on both the cell membrane and mitochondrial potential
. @‘.
.@ .
;a*;
1540 THE JOURNALOFNUCLEARMEDICINEâ€Vol. 39 •No. 9 . September 1998
‘,
I )@Ar.
.@@
I
@ -‘@@ , .— S
•r@
@‘
..

(24). Wolf et al. (21 ) observed uptake of 99mTc@MIBI, 99mTc..tetrofosmin and 99mTc@furifosmin in a tumor cell study. Theuptake of99mTc@MIBI was found to be the highest. Technetium99m-furifosmin uptake is also reported in a mouse model (25).
In the SPECT examination we could detect mediastinallymph node and pulmonary metastases in three additionalpatients. We found a higher sensitivity of SPECT compared toplanar images. This agrees with studies that show increasedsensitivities for SPECT examination. Charkes et al. (7) suggestan increase of sensitivity of 25% in thyroid cancer metastasesusing 201Tl-chloride SPECT. In their 201Tl-chloride SPECTexamination foci of I cm in the neck and of 1.5 cm in the lungswere seen. Disseminated lung metastases are better detectedwith CT (26). Muller et al. (18) compared planar to SPECTexaminations using 99mTcMIBI in patients with lung cancer byROC analysis and also found increased sensitivities usingSPECT.
Other studies deal with the multidrug resistance behavior ofthese agents. Both 99mTc@tetrofosmin and 99mTc..MIBI areuseful for imaging p-glycoprotein-status of tumor (27). Thallium-201-chloride is not a substrate for p-glycoprotein.
The sensitivity in our highly selected patient group ofI8F-FDG PET of 72% with a 95% confidence interval of
50%_ 89% on a patient-by-patient basis, and of 91% with 95%confidence interval of 78%—100%on a lesion-by-lesion basis isfar superior to 99mTc$.@rifoSmin and agrees with the reportedsensitivity of 83% in the literature (23 ). Despite having performed only PET studies of neck and thorax, our sensitivity agreeswith other studies performed on larger numbers of patients withwhole-body scans (22). Similar to other studies, ‘8F-FDGPETproved to be a valuable diagnostic method in the follow-up ofthyroid cancer, especially in tumors that do not accumulate 1311andpatients with elevated hTg-levels (22).
CONCLUSIONTechnetium-99m-funfosmin is not likely to be a competitive
radiopharmaceutical compared to established tracers for usewith SPECT and PET. Although 99mTc@furifosmin has betterphysical imaging characteristics, its diagnostic sensitivity issignificantly inferior to 201Tl-chloride. The study also confirmsthe value of the ‘8F-FDG PET. Although we did not performwhole-body scans, we achieved similar sensitivities in agreement with other studies using whole-body imaging.
We conclude that in our patients with DTC the scintigraphywith 99mTcffirifosmin is not useful, even for cervical andmediastinal lymph node metastases where the value of 201T1-chloride is established (12,13).
REFERENCES1. Gerson MC, Lukes I, Deutsch E, Biniakiewicz D, Washbum LC, Walsh RA.
Comparison of imaging properties of technetium-99m Q12 and technetium Q3 inhumans. J Nucl Cardiology 1995:2:224—320.
2. RosettiC, VanoliG, PaganelliG, et al. Humanbiodistribution,dosimetryandclinicaluse of technetium( IIl)-99m-Q 12. J Nod Med I994:35:1571—1580.
3. Okada RD. Nguyen KN, Lauinger M, et al. Effects of no flow and reperfusion ontechnetium-99m-Ql2 kinetics. J NucI Med 1995:36:2103—2109.
4. DeutschE, BushongW,GlavanKA,ci al. Heartimagingwithcationiccomplexesoftechnetium.Science198l;2l4:85—86.
5. NaruseH, DaherE, SinusasA, Ctal. Quantitativecomparisonof planarand SPECTnormal data files ofthallium-201 , technetium-99m-setamibi, technctium-99m-tetrofosmm and technetium.99m-furifosmin. J NucI Med 1996:37:1783—1788.
6. Sehweil AM. McKillop iH. Milroy R, Abdel-Dayem HM, Omar YT. Mechanism of
201Tluptakeintumors.EuriNuc/Med 1989:15:376—379.7. CharkesND, Vitti RA, BrooksK. Thallium-201SPECTincreasedetectabilityof
thyroid cancer metastases. J NucI Med 1990:3 1:147—153.8. lida Y, Hidaka A, Hatabu H, Kasagi K, Konishi I. Follow-up study of postoperative
patients with thyroid cancer by thallium-20l scintigraphy and serum thyroglobulinmeasurement. J Nucl Med 199l;32:2098—2100.
9. Ramanna L, Waxman A, Braunstein G. Thallium-201 scintigraphy in differentiated
thyroid cancer: comparison with radioiodine scintigraphy and serum thyroglobulindeterminations. J NucI Med l991;32:441—446.
10. Hoefnagel CA. Delprat CC, Marcuse HR. de Vijlder JiM. Role of thallium-201total.body scintigraphy in follow-up ofthyroid carcinoma. J Nod Med 1986;27: 1854—1857.
I I. Brendel Al, Guyot M, ieandot R, Lefort G, Manciet G. Thallium-201 imaging in thefollow-up of differentiated thyroid carcinoma. J NucI Med 1988:29:1515—1520.
12. MUller SP, Guth-Tougelidis B, Piotrowski B, Farahati I, Reiners C. Thallium-201scintigraphy in the follow-up ofeosinophilic thyroid carcinoma [Abstractl. J NucI Medl990;3I:767P.
13. Brandt-Mainz K, Muller SP, Sonnenschein W, Reiners Chr, Sciuk J, Bockisch A. Theinfluence of the location of thyroid cancer metastases on tumor detectability withthallium-20l [Abstract]. J Nucl Med l997;38:237P.
14. Reiners Chr, Muller SP, Farahati I, Eising EG. SPECT and planar scintigraphy indiagnostic and follow-up of thyroid cancer. &p C/in Endocrinol 1994:102:43—50.
I 5. Kosuda 5, Yokoyama H, Katayama M, Yokokawa T, Kusano, Yamamoto 0.
Technetium-99m tetrofosmin and technetium-99m sestamibi imaging of multiplemetastases from differentiated thyroid carcinoma. Eur J NucI Med 1995:22:1218—1220.
16. Klain M, Maurea 5, Lastoria S. Cuocolo A, Colao A. Salvatore M. Technetium-99m-tetrofosmin imaging of differentiated mixed thyroid cancer. J Nuc/ Med 1995:36:2248—2251.
17. Basoglu T, Sahin M, Coskun C, Koparan A, Bemay I. Erkan L. Technetium-99m-tetrofosmin uptake in malignant lung tumors. Eur J NucI Med 1995:22:687—689.
18. Muller SP, Paas M, Reiners Chr. ROC analysis of tumor detectability using 20111 (1)chloride and “Tc (I) hexakis (2-methoxy-2-isobutylisonitrile). Nuk/earmedi:in1994;33: 15—23.
19. MUllerSP, PiotrowskiB, Guth-TougelidisB, ReinersChr. Technetium-99mMIBIimaging in the follow-up of differentiated thyroid carcinoma [Abstract]. J Nod MedI989;30:904P.
20. Bride B, Hotze A, Kropp J, Bockisch A, et al. Comanson of 201T1and @“Tc-MlBlin the follow-up of differentiated thyroid carcinomas. Nuk/earmedi:in 1991 ;30: 115—124.
21. Wolf H, Fneling B, Tinnemeyer W, Brenner W, Henze E. Uptake von “Icmarkiertem sestamibi, tetrofosmin und furifosmin in mitoxantron-resisten versussensitiven Iumorzellen [Abstract]. Nuk/earmedizin 1997:36:97.
22. FeineU, LietzenmayerR, HankeiP, Held I, WöhrleH, MUller-SchauenburgW.Flourine-18-FDG and ‘@‘Iuptake in thyroid cancer. J Nucl Med 1996:37:1468—1472.
23. ReynoldsIC. RobbinsI. The changingrole of radiolodinein the managementofdifferentiated thyroid cancer. Semin NucI Med I997;27: I52—164.
24. Arbab AS. Koizumi K, loyama K, Araki I. Uptake of technetium-99m-tetrofosmin,technetium-99m-MIBI and thallium-201 in tumor cell lines. J Nucl Med 1996:37:1551—1556.
25. SchomãckerK, LöhrH, Gabruk-Szostak B, et al. Vergleich von ““Tc-MIBI,“'“Tc-tetrofosmin,““IcQl2 und 20111: Biokinetik in tumortragenden Mäusen[Abstract]. Nuk/earmedizin 1997;36:77.
26. Schober 0, Heintz P. Schwarzrock R, et a). Schilddrfisen-Carcinom: Rezidiv-undMetastasensuche: Sonographie, Röntgenund CT. Der Nuk/earmedi:iner 1986:9:139—I48.
27. BallingeriR, BannermannJ, BoxenI, FirbyP. HartmanNG,MooreMi.Technetium99m-tetrofosmin as a substrate for p-glycoprotein: in vitro studies in multidrugresistant breast tumor cells. J Nucl Med I996:37: I578 —I582.
TECHNETIUM-99M-FURIFOSMIN IN THYROID CANCER •Brandt-Mainz et al. 1541







