Stretching Scarce Resources: State Strategies to Design Effective, Affordable Benefit Packages
Anne Markus, J.D., Ph.D.Senior Research Scientist
The George Washington University Medical Center

Definitions
• Premium: Set amount of dollars per defined payment period (usually monthly) paid to obtain health insurance coverage.
• Cost-sharing: Patient exposure to out-of-pocket costs associated with health service delivery. Includes:
• Deductible• Coinsurance• Copayment

Purposes of Cost-sharing
• General reasons:– Enticing families to be more cost conscious in seeking
care– Fostering a sense of ownership/personal responsibility– Directing consumers toward more cost-effective care– Deterring unnecessary utilization– Raising revenues to reduce sponsor costs of health care
coverage

Purposes of Cost-sharing (cont.)
• Additional reasons for states: – Making public health insurance programs
aimed at the poor look more like private insurance
– Limiting substitution and crowd-out of private insurance

Recent Trends
• Private sector
– No significant changes to contribution strategies, but changes to benefit structure
• Medicaid/SCHIP– HIFA initiative
• Medicare– Pharmacy Plus initiative

Cost-sharing Rules in Public Programs
• Medicaid– Premiums prohibited
with some exceptions
– “Nominal” cost-sharing allowed
with some exceptions
– No overall cap specified
• SCHIP– Premiums allowed
– Cost-sharing allowed
– Overall cap of 5% of family income
• State employee benefit plans– Premiums allowed
– Cost-sharing allowed
– May or may not impose overall cap
Medicaid and SCHIP Waivers
• Medicaid cost-sharing waivers: (1) inappropriate use of ER
(2) 2 year demonstration program
• Section 1115 waivers: (1) waiver of Medicaid and/or SCHIP cost-sharing
requirements as part of a 5-year demonstration program
(2) streamlined waiver process and increased flexibility to design cost-sharing rules under HIFA
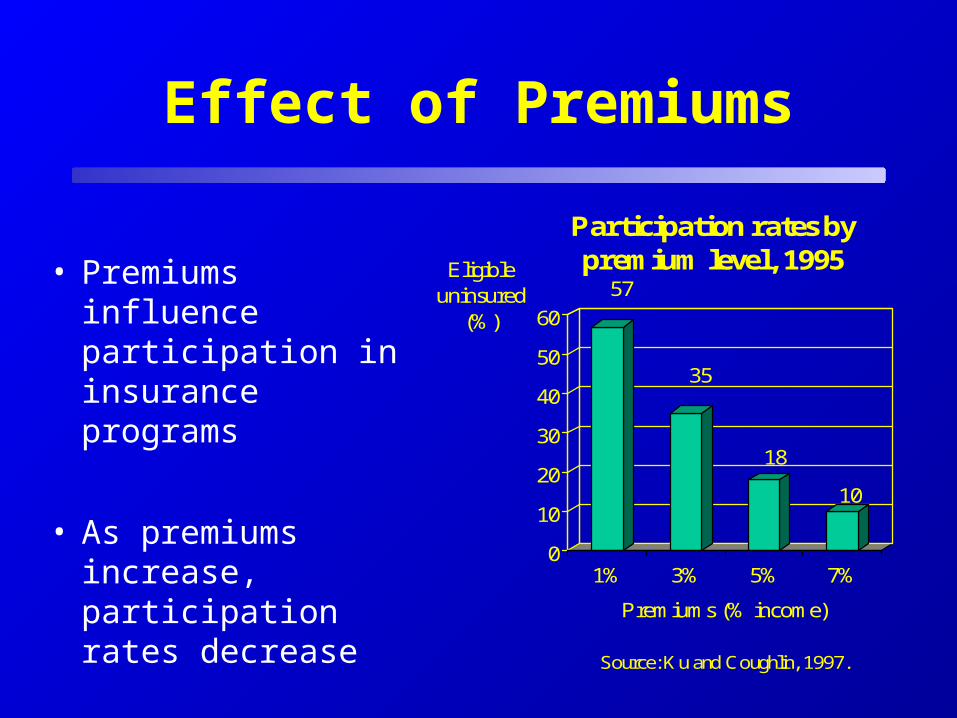
Effect of Premiums
• Premiums influence participation in insurance programs
• As premiums increase, participation rates decrease
57
35
18
10
0
10
20
30
40
50
60
Eligible uninsured
(%)
1% 3% 5% 7%
Premiums (% income)
Source: Ku and Coughlin, 1997.
Participation rates by premium level, 1995

Effects of Cost-sharing
• Use of services– Cost-sharing influences the
use of services
– As cost-sharing increases, use of services decreases
• outpatient care
• inpatient care
• prescriptions
• preventive services
• emergency room
• Health outcomes– Cost-sharing may have an
effect on health outcomes
– In general, cost-sharing has been found to have a minimal or no effect on health outcomes except for the poorest populations

Effect Across Population Groups
• Research shows that cost-sharing has a deterrent effect across the board:– children and adults– people who are healthy and people who have chronic conditions– rich and poor
• Existing body of knowledge also suggests that cost-sharing may have a more pronounced negative effect on low income people: – studies on premiums in state programs– non-Medicaid studies on cost-sharing– Medicaid studies on cost-sharing

SCHIP Experiences
• All States with separate SCHIP programs have some form of cost-sharing
• Research in this area thus far focuses on the effect of premiums on initial participation but also on continued participation in program
• Anecdotal evidence also suggests that collecting and processing premiums and other cost-sharing contributions is administratively burdensome and/or not worth the cost

Implications
• Income-related, sliding scale for premium and cost-sharing schedule
• Low premiums
• Limited cost-sharing
• Broaden the definition of preventive services exempt from cost-sharing
• Individuals with special needs

HIFA Cost-sharing Rules
• Mandatory eligibility groups (e.g., all children up to 100% FPL): same rules as Medicaid
• Optional eligibility groups (e.g., children beyond the mandatory eligibility levels): no cost-sharing rules specified other than an annual cap of 5% of family income for deductibles, copayments and coinsurance
• “Expansion” eligibles (e.g., nondisabled single working age adults, childless couples): no cost-sharing rules specified
Examples of State Flexibility Under HIFA
• Arizona (approved HIFA waiver): – Childless adults <100% FPL: same cost-sharing as Medicaid, i.e.,
$1-$5 except prenatal care, EPSDT services, family planning
– Parents of SCHIP and Medicaid children 100-200% FPL: same cost-sharing as SCHIP, i.e., family premiums up to $25 per month, $5 non-emergency use of emergency room, overall limit of 5% of annual family income
• California (approved HIFA waiver):– Parents of SCHIP and Medicaid children <200% FPL: similar to
cost-sharing under SCHIP, e.g., monthly premiums of $10 or $20, copays







