Download - Skeletal System: Bones and Bone Tissue. Four major components: BONES CARTILAGE TENDONS LIGAMENTS
Skeletal System:Bones and Bone Tissue

Four major components: BONES
CARTILAGE
TENDONS
LIGAMENTS

1. Support - provides hard framework for soft tissueStrong bones to bear weight
2. Protection of underlying organsSkull – BrainRib cage - heart & lungs
3. Movement - skeletal muscles use bones as leversTendons hold muscles to bones Joints – two bones come togetherLigaments –provide limited movement

4. StorageCalcium and PhosphorousFat stored in marrow cavities
5. Blood cell production (Hematopoiesis) Red bone marrow blood cells and
platelets
Hyaline cartilageMost bones develop from this type of
cartilage
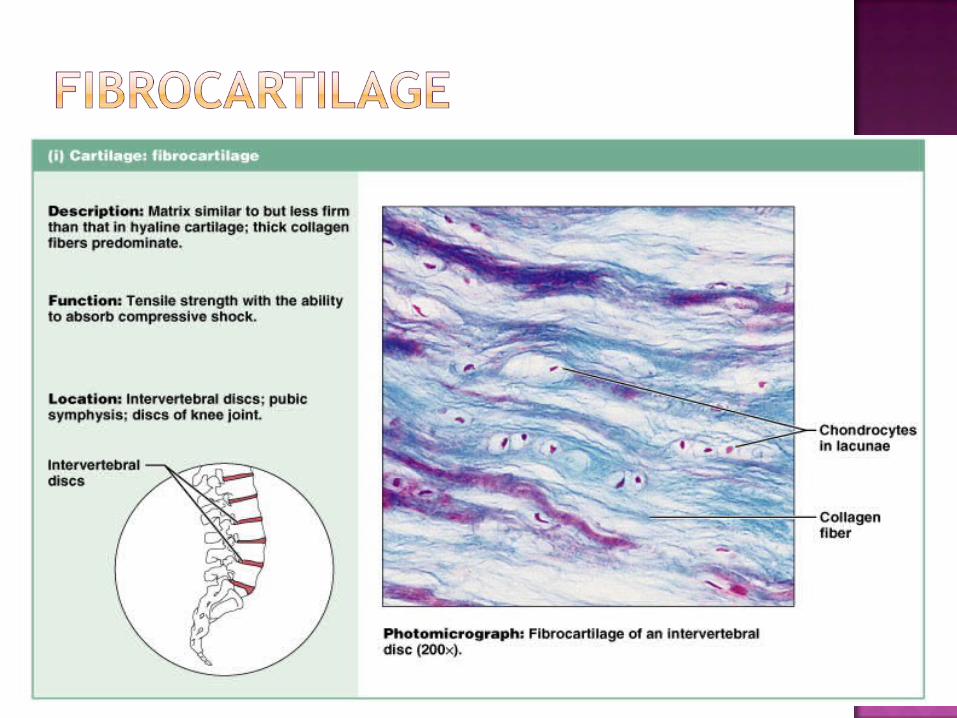
Fibrocartilage
Elastic cartilage
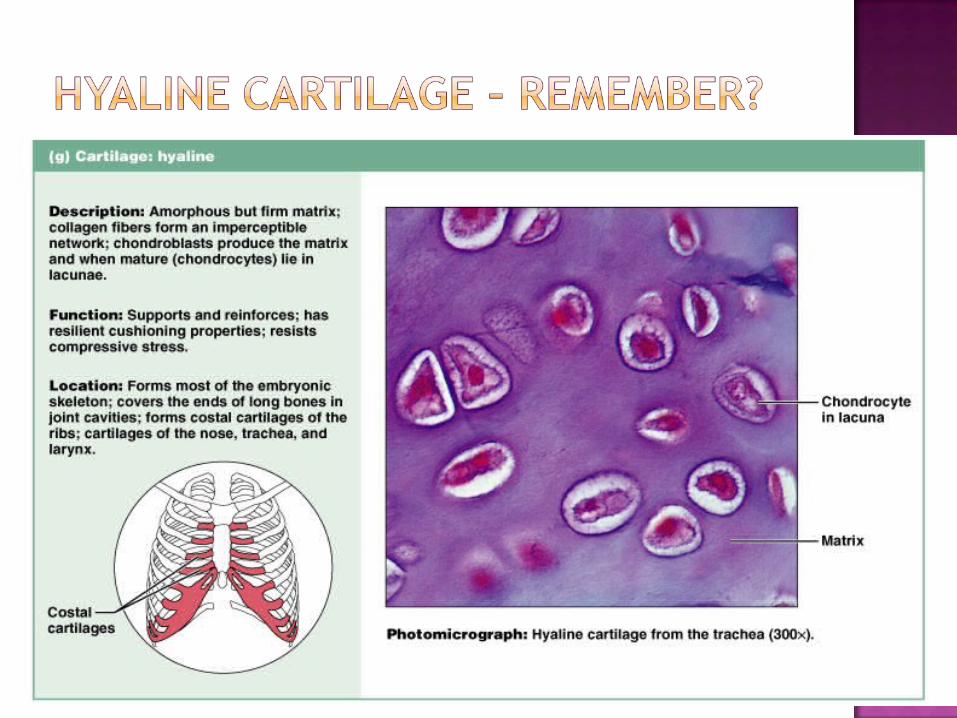
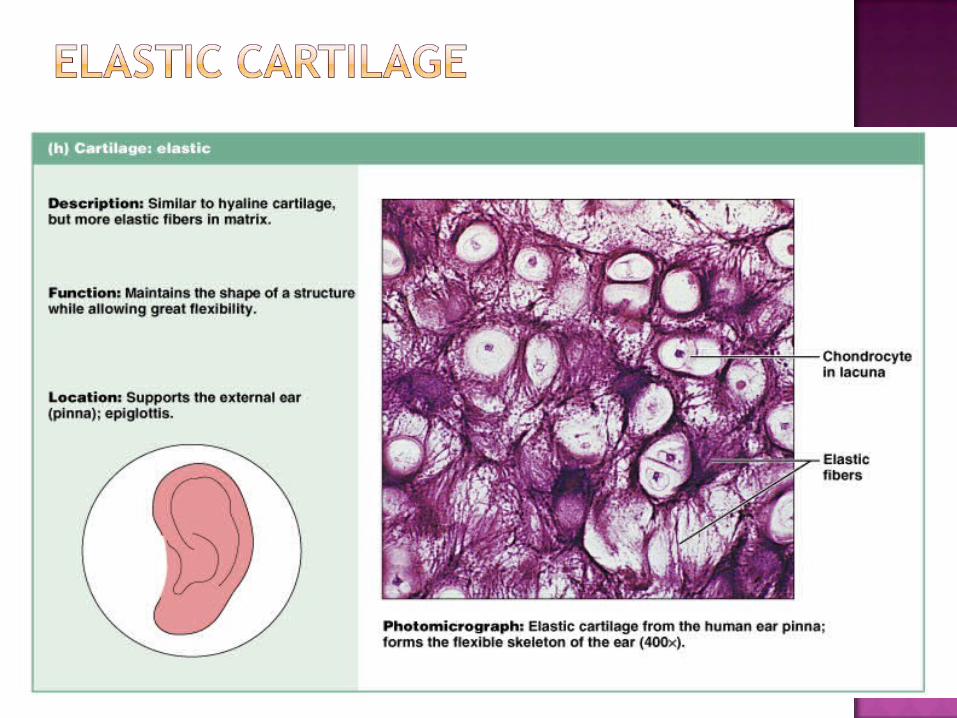

Hyaline – specialized cells that produce matrix surrounding cells
Chondroblasts – produce new cartilage matrix
Chondrocyte – cells that maintain the cartilage
Lacunae – space within the matrix
Matrix – contains collagen, provides strength
Perichondrium – double layered connective tissue sheathCovers most cartilage
Blood vessels and nerves penetrate outer layer of perichondrium
Does not enter cartilage matrix
Nutrients diffuse through cartilage matrix to reach chondrocytes
Articular cartilage Cartilage that covers end of bones where they form joints
Has no perichondrium, blood or nerves
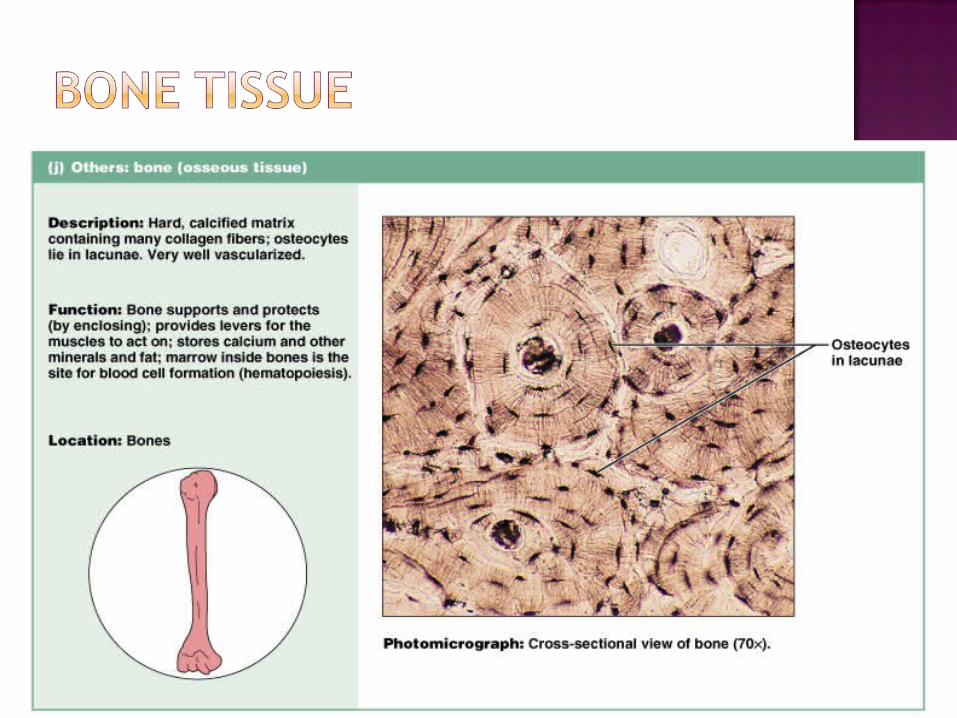
Bone connective tissue
Bone matrixSteel bars is collagen fibers, weight bearing
strength or cement is mineral components
Organic components (35%)Primarily collagen
Inorganic mineral salts (65%) Primarily calcium phosphate
Hydroxyapatite Gives bone its hardness; resists compression
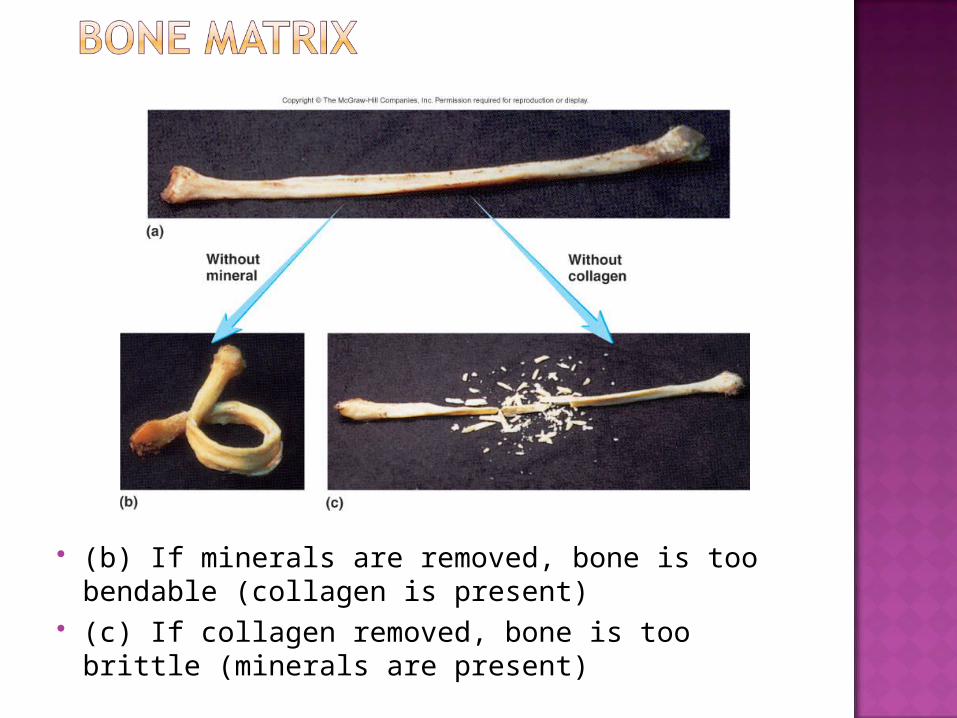
(b) If minerals are removed, bone is too bendable (collagen is present)
(c) If collagen removed, bone is too brittle (minerals are present)
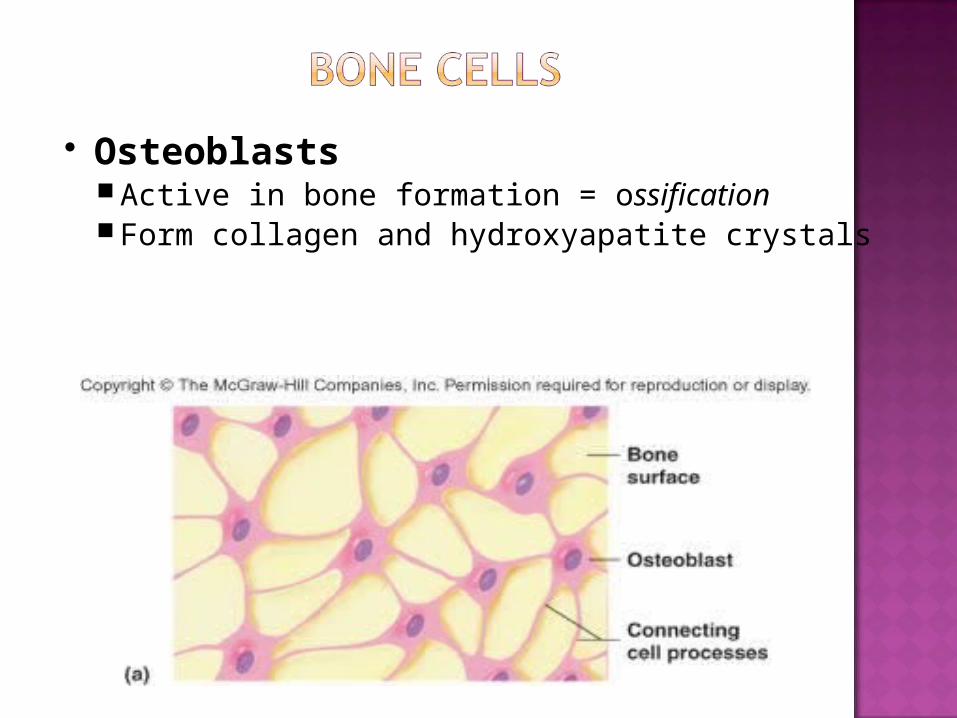
OsteoblastsActive in bone formation = ossificationForm collagen and hydroxyapatite crystals
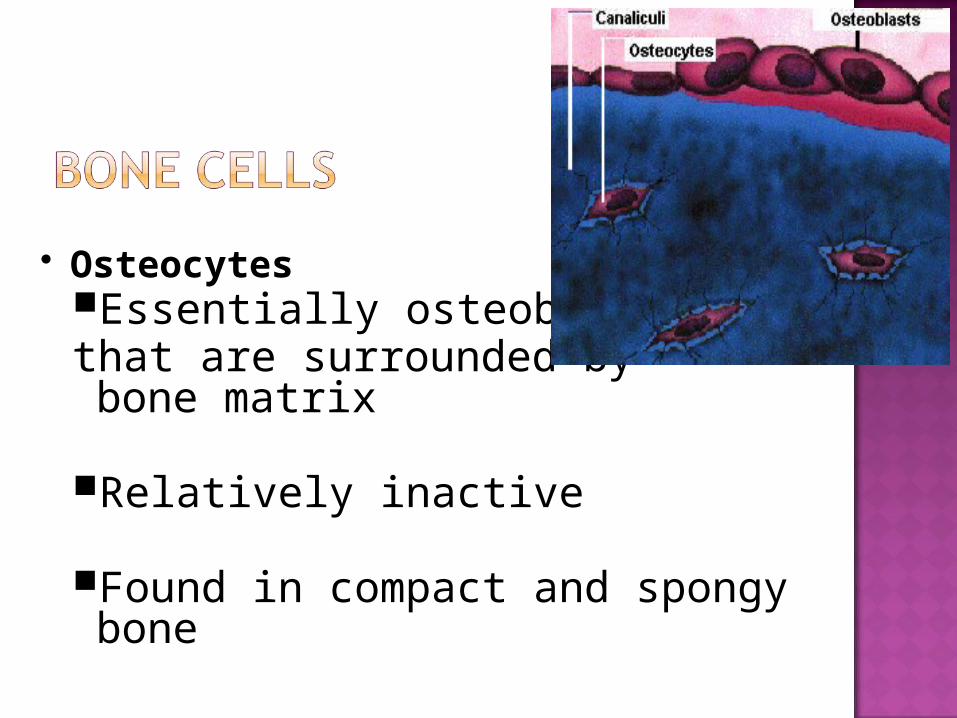
OsteocytesEssentially osteoblasts that are surrounded by bone matrix
Relatively inactive
Found in compact and spongy bone
OsteoclastsCells used to breakdown bone (bone resorption)
Stimulated by need for calcium & phosphate in the body
Breaks down mineral salts (demineralization or decalcification)
Resorption starts to exceed formation as people age
Bone classified based on collagen fibers within bone matrix:1. Woven bone – collagen randomly
oriented in many directions
Formed during fetal development or repair of fracture
Remodeling forms lamellar bone

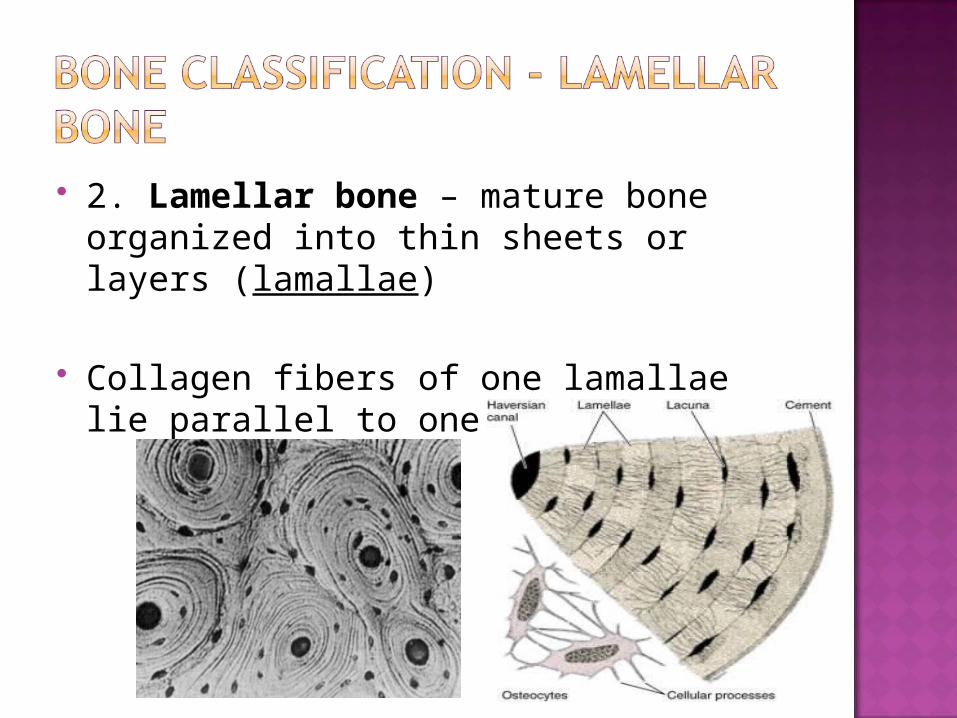
2. Lamellar bone – mature bone organized into thin sheets or layers (lamallae)
Collagen fibers of one lamallae lie parallel to one another

Bone classified by amount of matrix relative to amount of space in bone
Cancellous – less bone matrix, more space
Compact – more bone matrix less space; denser

Trabeculae: interconnecting rods or plates of boneBetween the trabeculae - filled with bone
marrow and blood vessels
Porous appearance
No blood vessels, osteocytes obtain nutrients through canaliculi
Covered with single layers of cells of osteoblasts and few osteoclasts

Denser
Has fewer spaces than cancellous bone
Blood vessels enter the substance of the bone itself
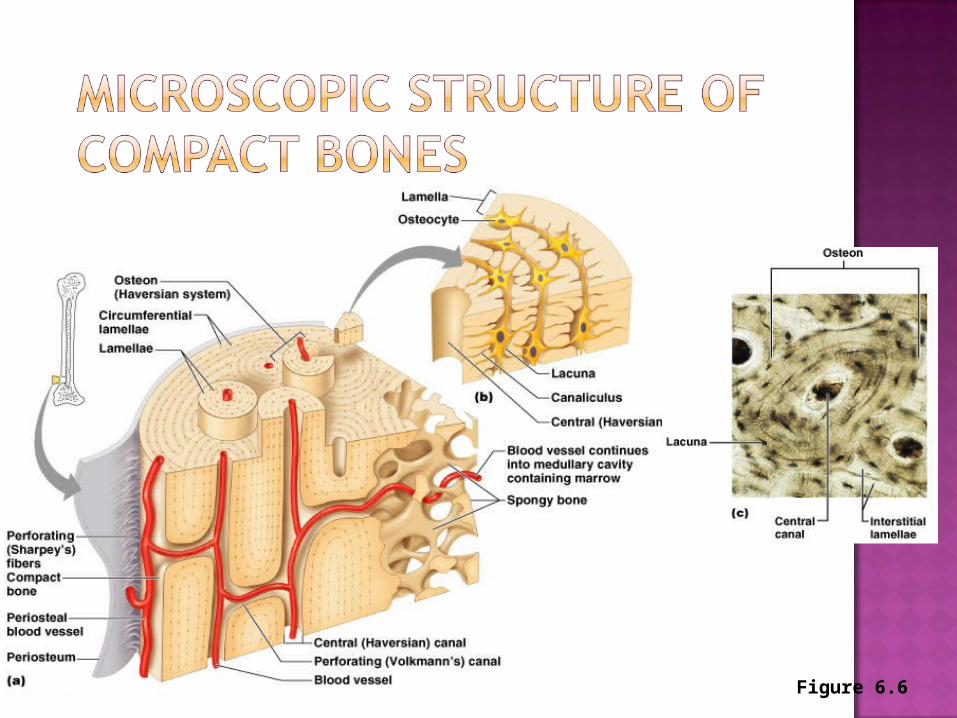
Figure 6.6
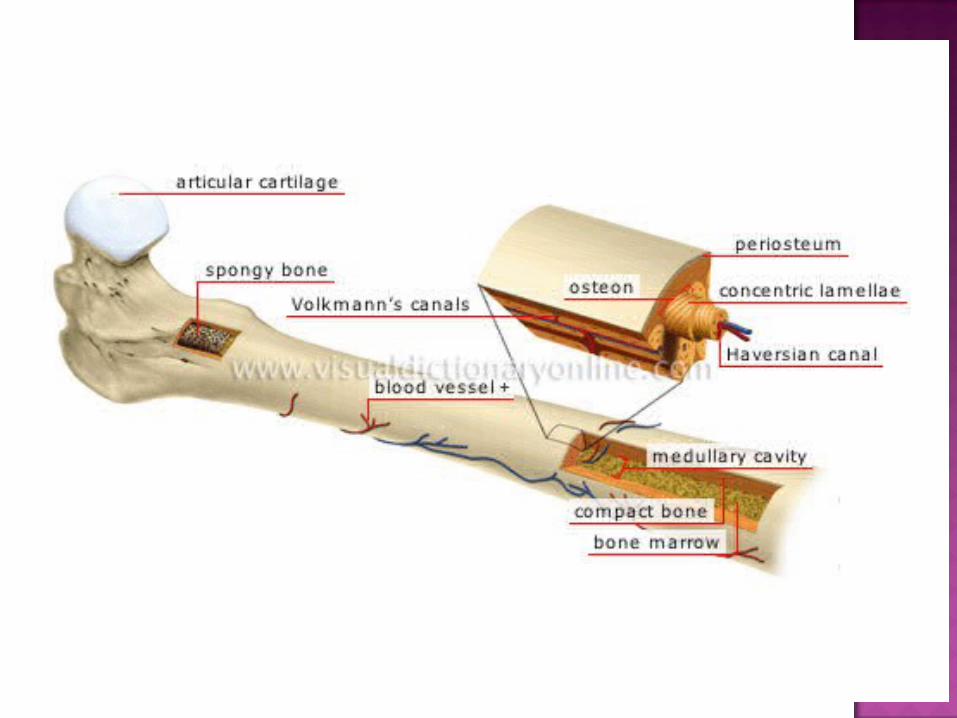
Osteon or Haversian SystemBasic unit of compact bone
Consists of a central canalrun parallel to surface of bone
Contains blood vesselsConcentric lamellae - cylinders of
bone
Circumferential lamellae – outer surfaces of compact bone
Interstitial lamellae – in between osteons Perforating or Volkmann’s canal –
Osteocytes receive nutrients and eliminate waste products through canal system
Contain blood vessels that then branch to enter central canal
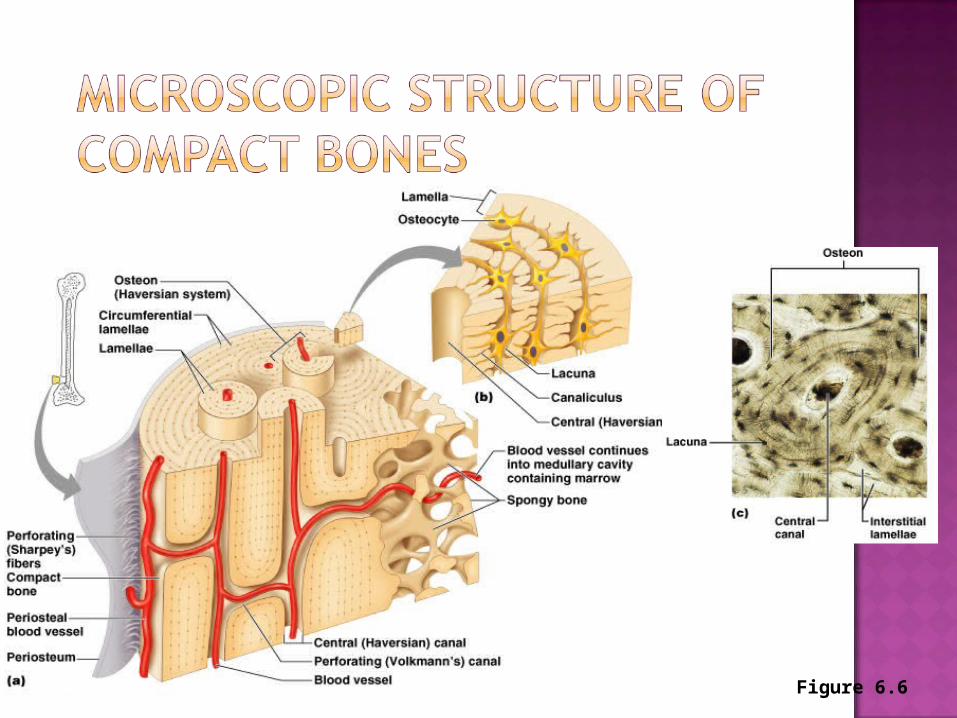
Figure 6.6
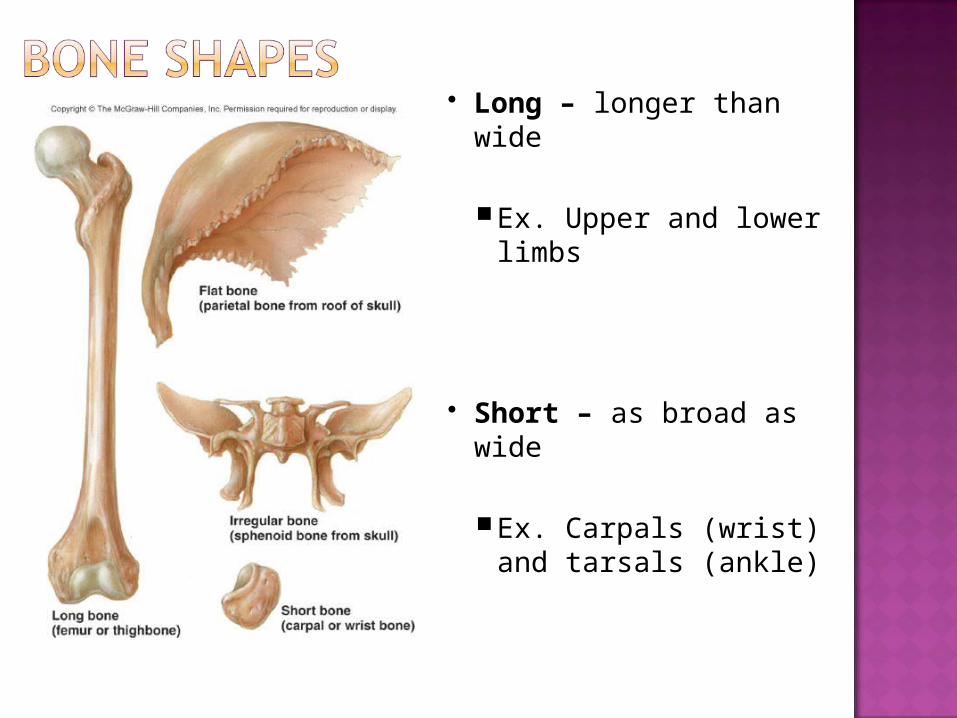
Long – longer than wide
Ex. Upper and lower limbs
Short – as broad as wide
Ex. Carpals (wrist) and tarsals (ankle)

Flat – thin, flattened shape, curved
Ex. Ribs, sternum, skull, scapulae
Irregular – doesn’t fit in other category
Ex. Vertebrae, facial
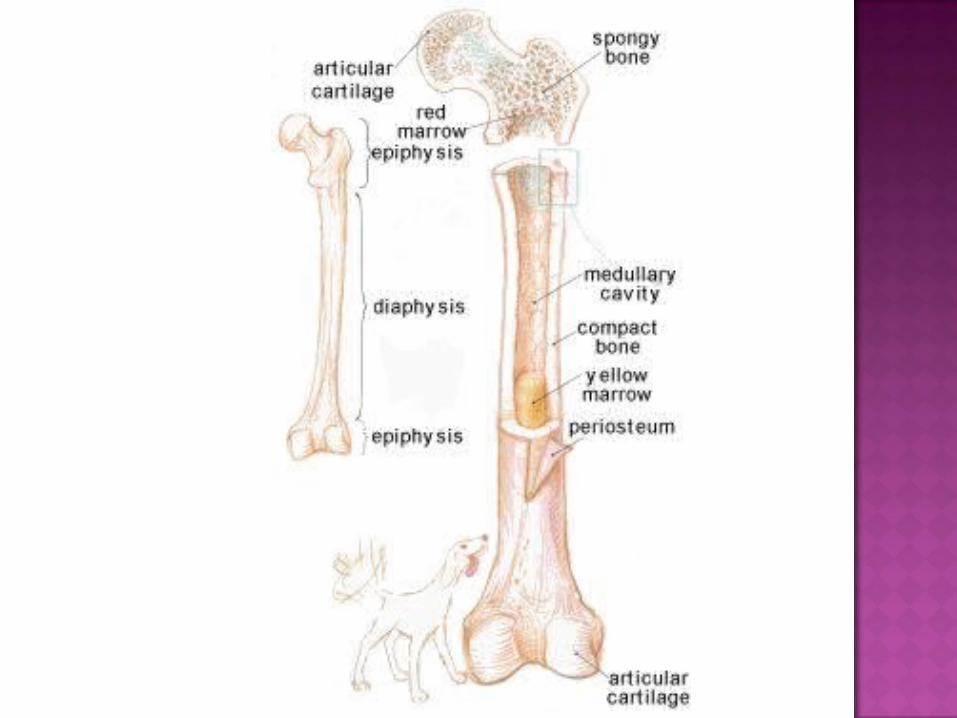
DiaphysisShaft of boneMostly compact bone, can contain cancellous
EpiphysisEnd of the bone - Cancellous boneCovered with articular cartilageDevelops from center of ossificationBones with one or more epiphyses:
Long bone of arm Forearm Thigh bone Lower leg
Epiphyseal plate - responsible for growth in length of bone
Composed of hyaline cartilage
Present until growth stops
Then becomes epiphyseal line
Medullary cavity - central, hollow cavityFilled with marrow
At birth, there’s more red marrow
Conversion from red to yellow as you age
Yellow marrow completely replaces red in long bones of limbs, except in proximal part of arm and thigh bones
Periosteum – connective tissue membrane covers outside of boneFibers of tendon that bind muscle to
bone become continuous with fibers of periosteum.
Sharpey’s fibers - fibers that penetrate into the bone matrixStrengthen attachment of tendon
to bone
EndosteumSimilar to inner layer of periosteum
Lines all internal spaces including spaces in cancellous bone
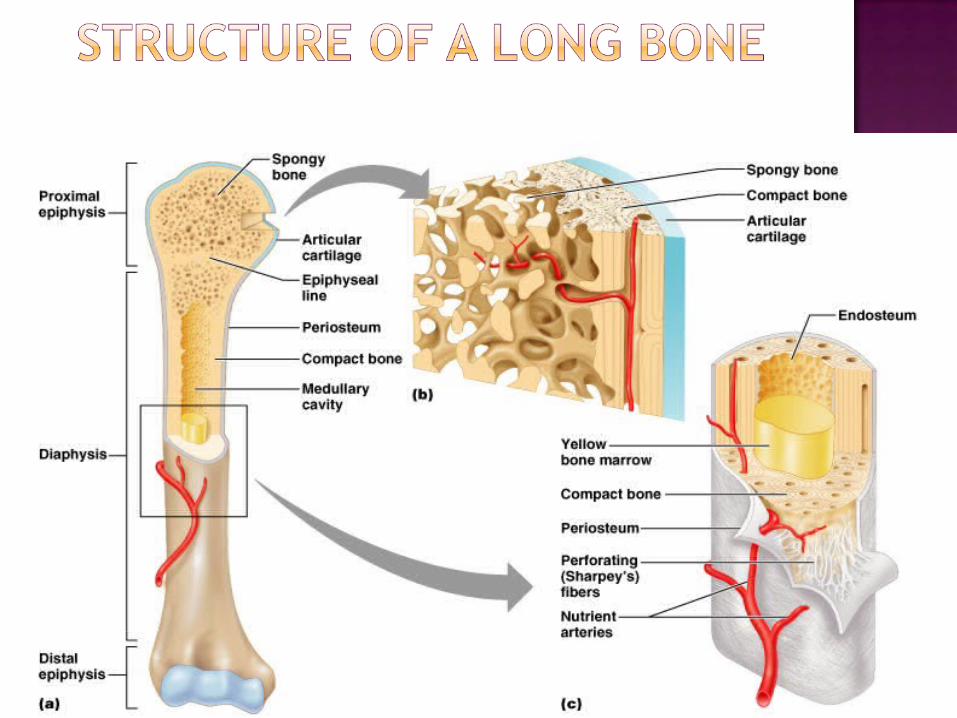
Figure 6.3a-c
1. What are the 4 different types of bones?
2. Identify the following:The end of a bone is called – The shaft of the bone is called –
3. What is found in the medullary cavity?
4. What is the difference between red and yellow marrow?

5. What is the name of cells that make new cartilage?
6. What is the name of cells that maintain cartilage?
7. What makes up the bone matrix?
8. What is the difference between cancellous and compact bone?

1. What are the 4 different types of bones?Long, short, flat and irregular
2. Identify the following:The end of a bone is called – EpiphysisThe shaft of the bone is called – Diaphysis
3. What is found in the medullary cavity? - Bone marrow
4. What is the difference between red and yellow marrow? Red – blood formation Yellow – adipose tissue
5. What is the name of cells that make new cartilage? Chondroblasts
6. What is the name of cells that maintain cartilage? Chondrocytes
7. What makes up the bone matrix? Collagen (35%)Calcium phosphate (65%) – aka hydroxy
apatite
8. What is the difference between cancellous and compact bone?Cancellous – less bone matrix, more space
betweenCompact – More bone matrix, less space,
denser
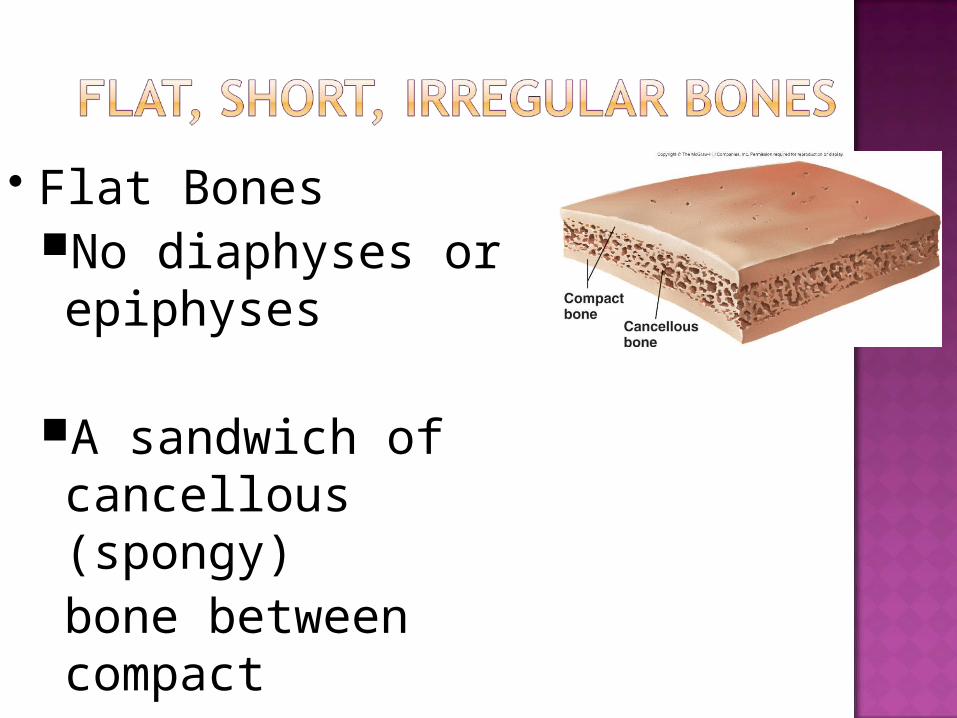
Flat BonesNo diaphyses or epiphyses
A sandwich of cancellous (spongy) bone between compact
Short and Irregular bonesSimilar composition to epiphyses of
long bones
Compact bone surfaces that surround cancellous bone center with small spaces filled with marrow

Short and Irregular bonesNot elongated and have no diaphyses
Certain regions of these bones have epiphyseal growth plates and small epiphyses

Bone formation occurs in 2 different ways Intramembranous ossification
Occurs in connective tissue membrane
Endochondral ossification Occurs in cartilage
Both produce woven bone that is then remodeled to lamellar
Internally, osteoblasts form cancellous bone
Externally, osteoblasts form compact bone
Forms many flat skull bones, part of mandible, diaphyses of clavicles
When remodeled, indistinguishable from endochondral bone
ALL bones except some bones of the skull and clavicles
Bones are modeled in hyaline cartilage
Begins forming late in 2nd month of human development

Continues forming until early adulthood
Blood vessel invade cartilage, matrix becomes calcified and chondrocytes die
Perichondrium becomes periosteum
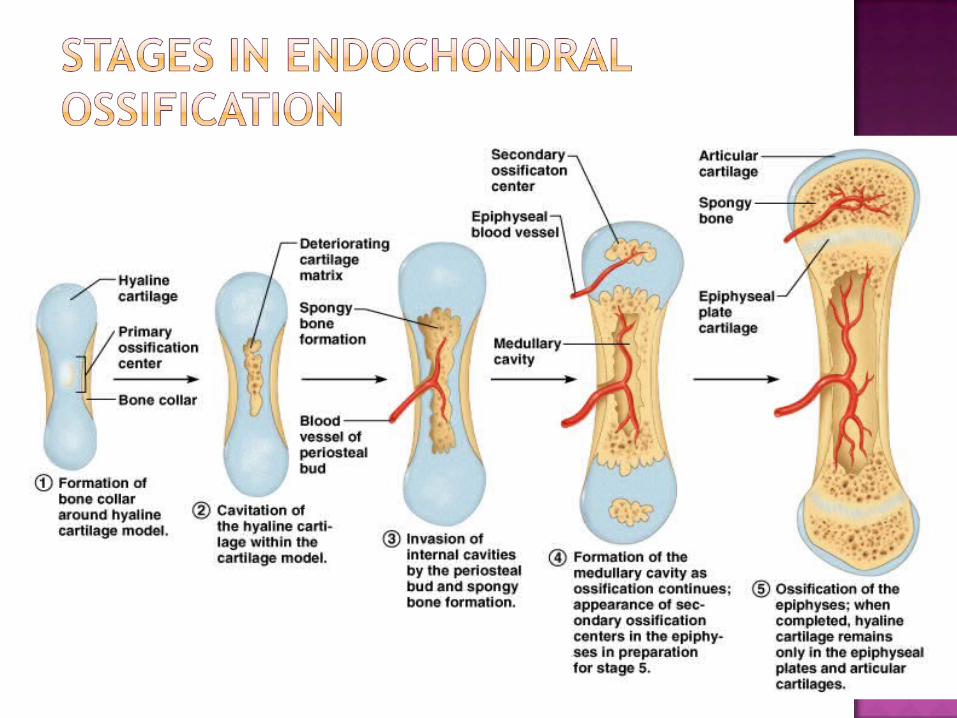
Figure 6.10

1. How are short, flat and irregular bones different from long bones?
2. What is “remodeling”?
3. How is intramembranous ossification different from endochondral ossification?
1. How are short, flat and irregular bones different from long bones?Short bones have no diaphysis or epiphysis;
cancellous bone sandwiched between compact
2. What is “remodeling”?Bone metabolismLife long process where mature bone tissue
is removed from the skeleton and new tissue is formed
3. How is intramembranous ossification different from endochondral ossification? Intramembranous
Forms the skull, shoulder blades, jaw Occurs in the connective tissue membrane Occurs in fetal development Cartilage is NOT present
Endochondral ALL other bones Cartilage (hyaline) is present Continues forming until early adulthood

Bone formation happens on surface of older bone or cartilage
Long bones increase in length because of growth at epiphyseal plate
Involves formation of new cartilage from inside of preexisting cartilage and bone growth of surface of cartilage

Interstitial growth – new cells formed from within tissue (cyte cells)
Appositional growth – new cells added to surface of tissue by blast cells

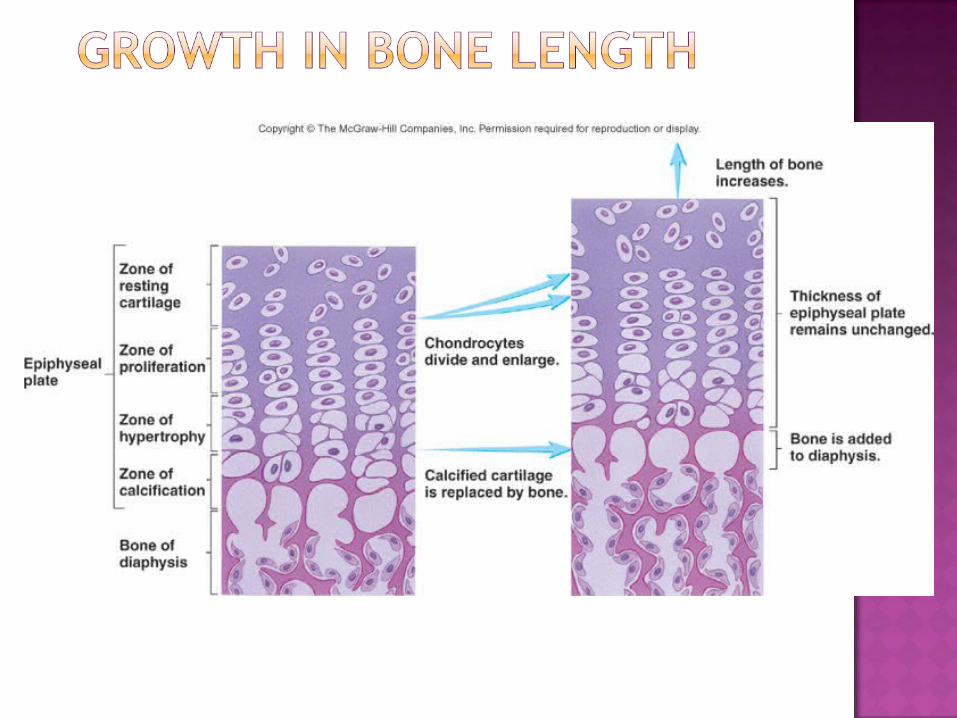
Composed of 4 zones:
1. Zone of resting cartilage – nearest epiphysis and contains random chondrocytes that don’t divide rapidly
2. Zone of proliferation – produce new cartilage through interstitial cartilage growth; chondrocytes form stacks
3. Zone of hypertrophy – chondrocytes produced mature and enlarge
cells nearer epiphysis: younger and actively proliferate
cells nearer diaphysis:older and maturing
4. Zone of calcification – thin and contains hypertrophied chondrocytes and calcified cartilage matrixHypertrophied chondrocytes die
Blood vessels from diaphysis grow into area
Connective tissue surround blood vessels contains osteoblasts
Osteoblasts make new bone matrix
In epiphyseal plates of growing bones...Length of diaphysis increases
Cells push the epiphysis away from the diaphysis
Once bones reach adult size, epiphyseal plate ossifies and becomes epiphyseal line
Occurs between 12-25 yrs of age (depends on bone and individual)

Long bones increase in width; other bones increase in size or thickness
Rapid growth – young bones or puberty
Size and shape of a bone determined genetically but can be modified
Influenced by Nutrition Hormones
NutritionLack of calcium, protein and other nutrients
during growth and development can cause bones to be small; illness and malnutrition
Nutrition con’tVitamin D
Necessary for absorption of calcium from intestines
Can be eaten or manufactured in the body
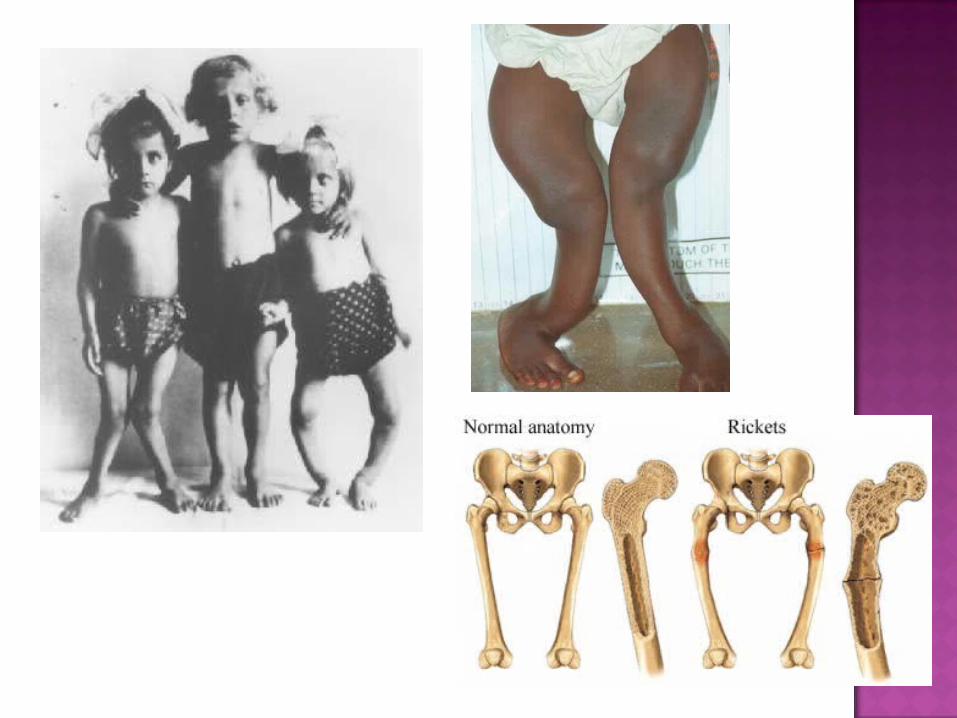
Rickets: lack of vitamin D during childhood
Osteomalacia: lack of vitamin D during adulthood leading to softening of bones

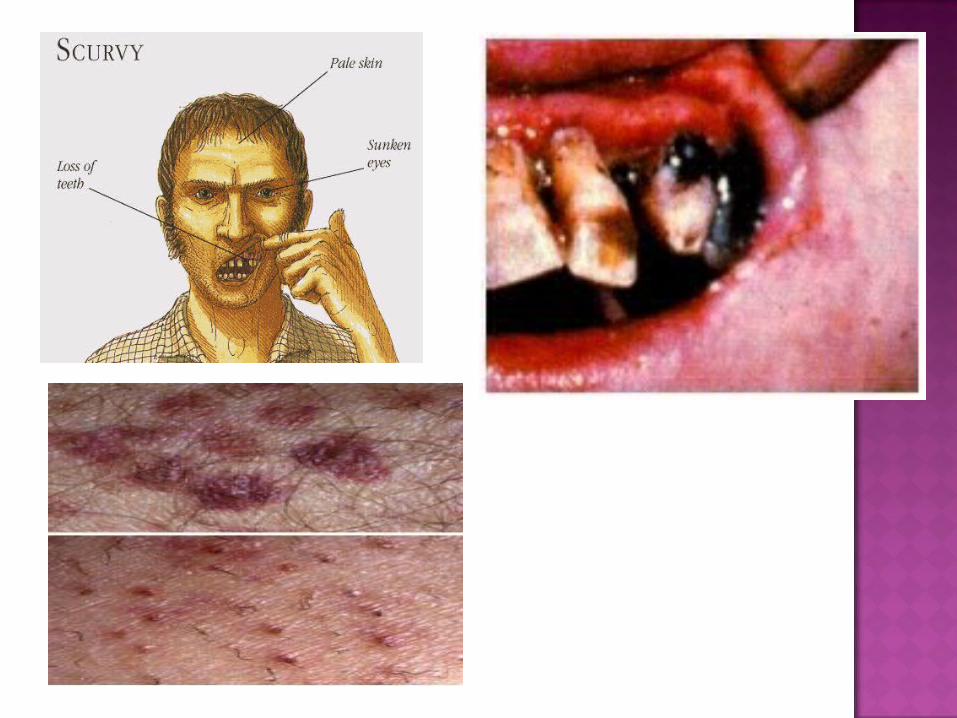
Nutrition con’tVitamin C
Necessary for collagen synthesisCan cause growth retardationScurvy: due to deficiency of vitamin C
Ulceration & hemorrhage in any area of body
Lack of vitamin C also causes wounds not to heal, teeth to fall out

HormonesGrowth hormone stimulates
interstitial cartilage growth appositional bone growth
Thyroid hormone required for growth of all tissues

HormonesSex hormones : estrogen and
testosterone
Cause growth at puberty, but also cause closure of the epiphyseal plates
Females stop growing earlier than males because estrogen causes quicker closure of epiphyseal plate
Bone deposit and removal Occurs at periosteal and endosteal surfaces
Bone deposition – accomplished by osteoblasts
Bone reabsorption – accomplished by osteoclasts
Converts woven bone into lamellar bone
Involves bone growth, change in bone shape, adjustment of bone stress, and bone repair

Completed through osteoclasts and osteoblasts
Travel through bone, removing old bone matrix and replacing it with new bone matrix
These specific cells renew the entire skeleton every 10 years

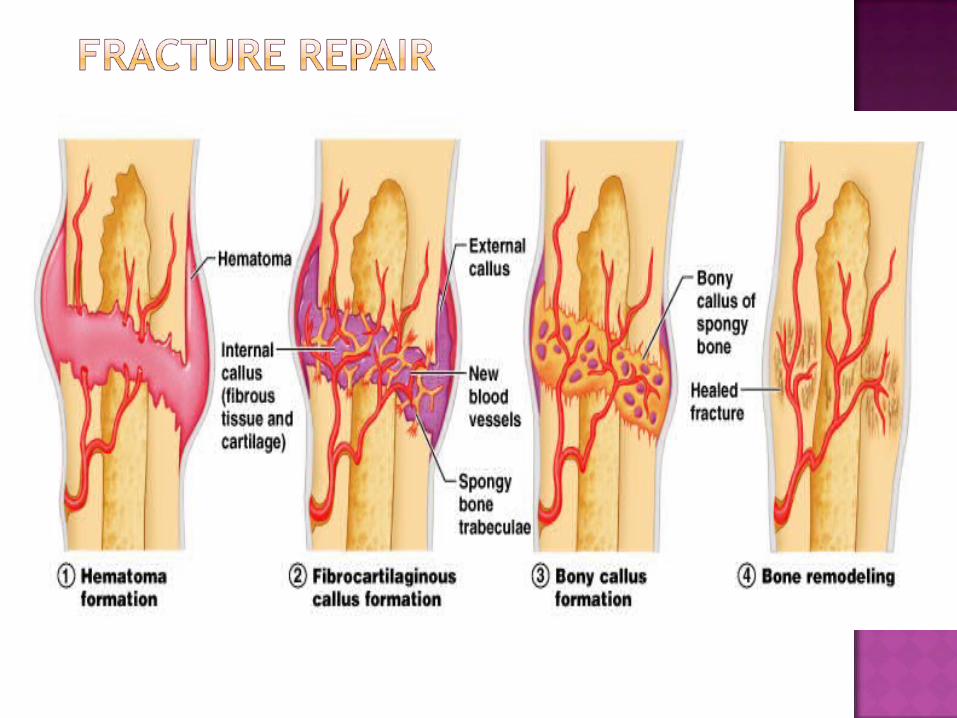
1. Hematoma formation - blood clot formation
Hematoma – localized mass of blood released from blood vessels but confined within a space
Injury followed by inflammation and swelling
2. Callus formation - mass of tissue that forms at a fracture site and connects the broken ends of the bone
Internal and external callus
Cartilage is formed
Osteoblasts invade = New bone is formed
Bone/cartilage (woven bone) stabilizes broken bone
3. Callus ossification Callus replaced by woven, cancellous bone
Stronger external callus
4. Bone remodeling Replacement of cancellous bone and damaged
material by compact bone
Remodeling takes sometimes more than a year; repaired zone thicker than adjacent bone

Open (compound) – bone break with open wound. Bone may be sticking out of wound.
Closed (simple) – Skin not perforated.
Complicated – soft tissue around closed fracture is damaged
Incomplete - doesn’t extend across the bone. (2+ fragments)
Complete – does extend across the bone
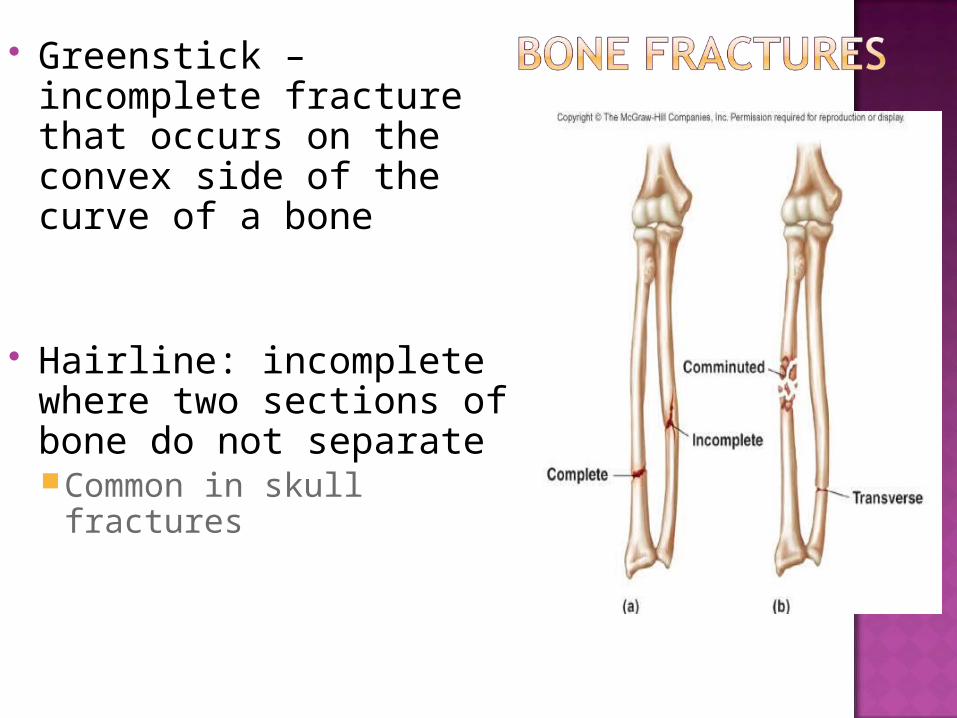
Greenstick – incomplete fracture that occurs on the convex side of the curve of a bone
Hairline: incomplete where two sections of bone do not separateCommon in skull fractures
RicketsSoft bonesVitamin D/Calcium/Phosphate deficiency in
CHILDREN If the blood levels of these mineral become
too low, hormones cause Ca and P to be released from bones
OsteomalaciaSoftening of bonesVitamin D deficiency in ADULTSLeads to improper calcium absorption
OsteomalaciaNormal bone density
Not enough Vitamin D in the diet Note enough exposure to sunlight Lactose intolerant
Bone fractures happen with very little injury
Widespread bone pain
Complete healing with treatment takes place in 6 months

Osteomyelitis Bacterial infections (or fungal) of bones
Infections spread via the blood from wounds, boils, TB
Infection can start after bone surgeryEspecially when rods or plates are used
Leads to destruction of bone
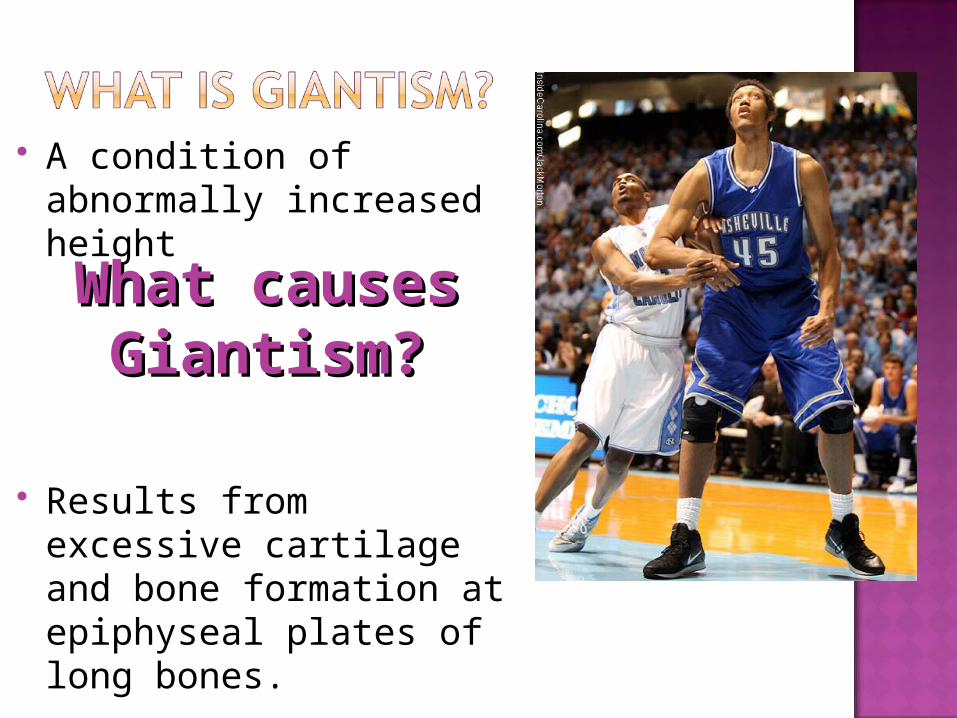
A condition of abnormally increased height
Results from excessive cartilage and bone formation at epiphyseal plates of long bones.
What causes What causes Giantism?Giantism?

Pituitary giantism – excess secretion of pituitary growth hormone.
Robert Wadlow's height of 8' 11.1" qualifies him as the tallest person in history.

Acromegaly – excess pituitary growth hormone secretion
Involves growth of connective tissue, including bones, after epiphyseal plates ossified
Mainly involves increased diameter of all bones
Growth hormone deficiency involves abnormally short stature with normal body proportions.
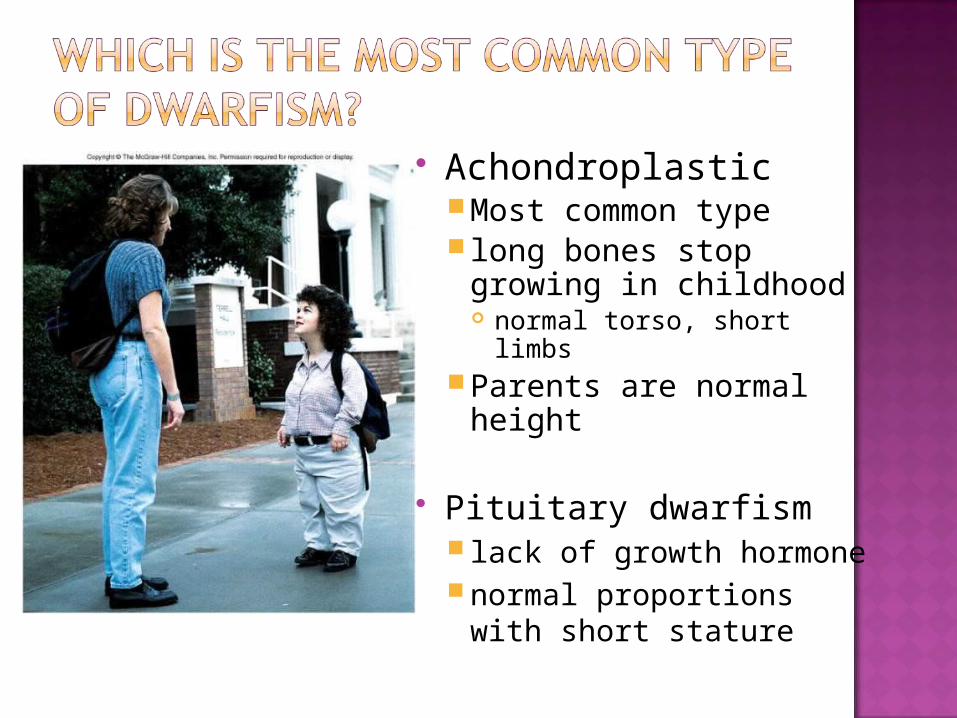
AchondroplasticMost common type long bones stop growing
in childhood normal torso, short limbs
Parents are normal height
Pituitary dwarfism lack of growth hormonenormal proportions with
short stature
Bone matrix decreases More brittle due to lack of collagenAlso less hydroxyapetite (calcium
phosphate)
Bone mass decreasesHighest around 30 yrs of ageMale bone mass denser due to
testosterone and greater weightRate of bone loss increases 10 fold after
menopause
Increased bone fractures
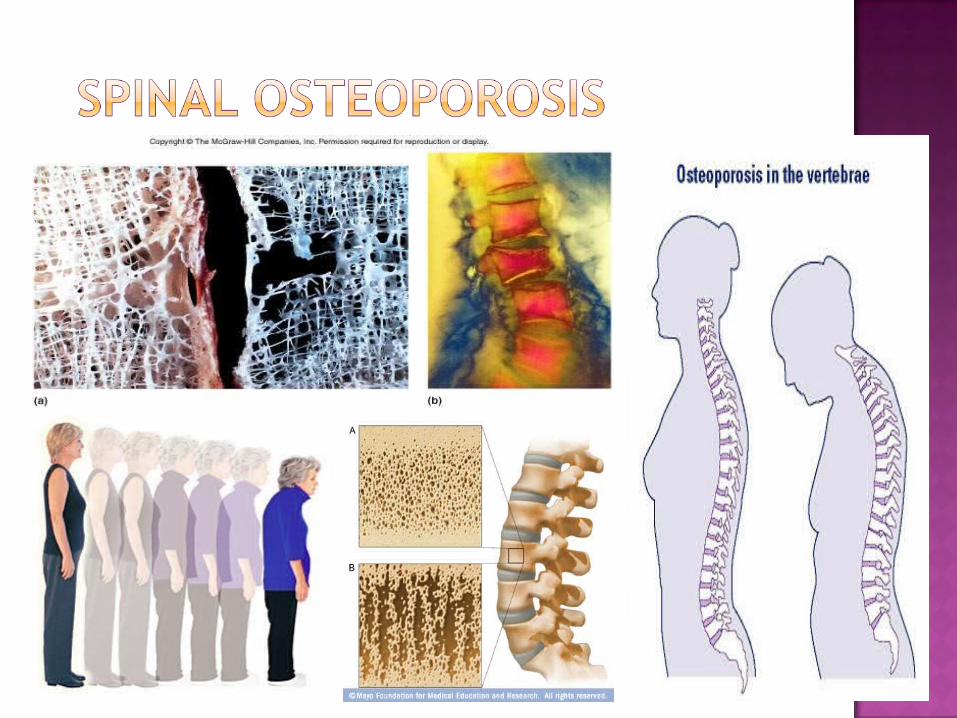
Bone loss causes deformity, loss of height, pain, stiffness Stooped posture Loss of teeth

Decrease in bone densityDepletion of calcium and phosorphous
Porous bone
Occurs when rate of bone resorption exceeds rate of bone formation
Bone is deformed and prone to fracture
Occurs mostly in older people

Occurrence increases in ageStrong genetic component 60% genetic; 40% environmental or lifestyle
(diet & exercise)
Loss of bone mass
Curvature of spine
Muscle weakness
Pain sensations
Impaired respiration

Postmenopausal women (> 50) at greatest riskDecrease of estrogen – maintains bone
mass Estrogen maintains density in both
sexes (inhibits resorption) Males, reduction of testosterone levels
Testosterone levels don’t decrease significantly until age 65
TreatmentsHRT – uses estrogen to decrease osteoclast
numbers Reduces bone loss
SERMS – class of drugs bind to estrogen receptors Inhibit osteoclasts, stimulate osteoblasts,
increase bone mass
Prevention -- exercise and calcium intake (1000 mg/day) between ages 25 and 40
What you need to know… The 5 functions of the skeletal system Components of the bone matrix Types of cartilage found in the body Chondroblasts vs chondrocytes vs condroclasts Osteoblasts vs osteocytes vs osteoclasts Compact vs cancellous bones Bone types & examples Compare & contrast the 4 bone types Types of marrow Factors affecting bone growth Labeling diagram of compact bone (ex – osteons)







