
What is Good Quality Care?
SafeTimelyEffectiveEfficientEquitablePatient-Centred

Comparative Risks of Healthcare

Health Care Systems are Dangerous!
Examples BBC investigation through FOI Act, May
2013o Cases of foreign objects left inside
patients during operations– 322
o Cases of surgery on the wrong body part
– 214
BMJ July 2012; NPSA report methotrexateo Deaths - 26o Serious harm - 25


Reducing Risk Some industries have
dramatically reduced their risks. Which industries? How? By changing their ‘Safety
Culture’

Manchester Patient Safety FrameworkDescribes 5 safety cultures (in detail!)
GenerativeProactive
BureaucraticReactive
Pathological
The Francis Reporthttp://www.youtube.com/watch?v=CY-P9n_7atU

How Can We ChangeOur Safety Culture?
• Understand why accidents happen• Find out what mistakes are
happening• Change our systems to make it…
• …harder to do the wrong thing• …easier to do the right thing

Understandwhy accidents happen
1. System Failures a. Poor designb. Latent factors
2. Human Factors a. Focusb. Fitnessc. Filters

Focus
http://www.youtube.com/watch?v=ubNF9QNEQLA

Fitness

Filters
http://www.youtube.com/watch?v=oaGpaj2nHIo
Find outWhat mistakes are happening
From…1. Staff - event reporting, walk rounds, briefings
2. Patients - complaints, comments, surveys
3. External Staff - pharmacist, coroner, DNs
4. Metrics - trigger tools, audit

NHS Reporting & Learning System – incidents reported from England 03 to 09
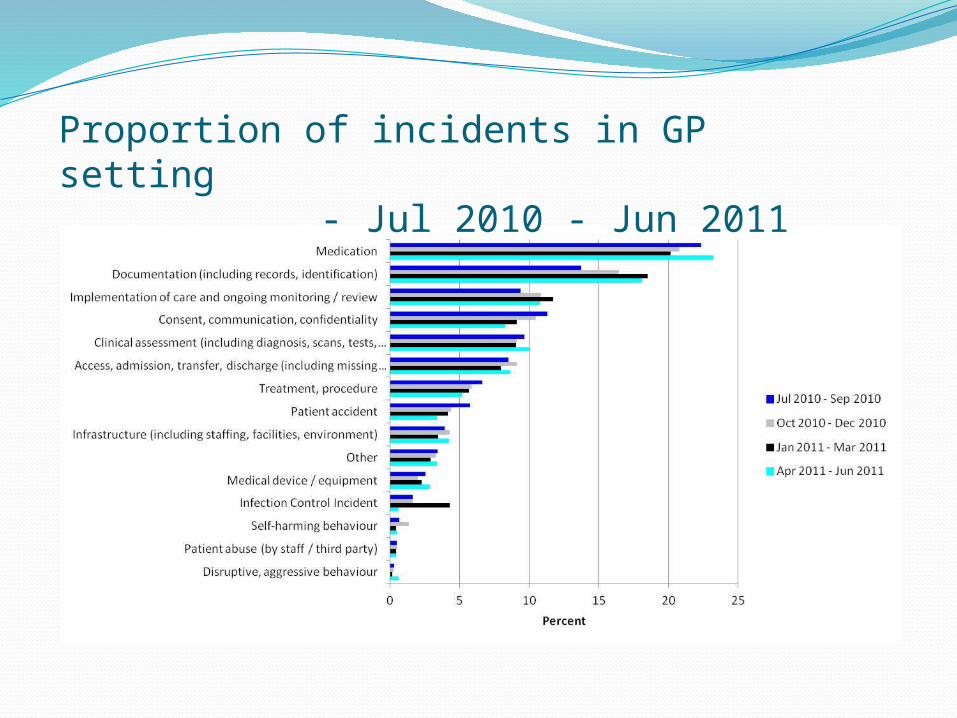
Proportion of incidents in GP setting - Jul 2010 - Jun
2011

Change our systemsbut how?
What are we trying to achieve?
How will we know if the change is an improvement?
What changes can we make that will result in an improvement?
Set clear and focused goals
Focus on problems that cause concern
Have clear, measurable targets

Application!Think of a significant event at workWhat happened?Who was involved?Why did things go wrong?
human factors? system weaknesses?How can the system be changed to make it
harder for this error to recur?easier to do the right thing?

ConclusionsAccept that making mistakes is normal
Talk about your mistakes and ask…How can we make it harder to do the wrong
thing?How can we make it easier to do the right
thing?Care for patients - look out for potential problems
Understand, Find Out, Change
The End







