Download - ROSC Lecture 2 Part 1

Cardiac Arrest, Hypothermia and Resuscitation Science
Lecture 2: CPR – the foundation of resuscitation care
Benjamin S. Abella, MD MPhil
Clinical Research Director
Center for Resuscitation Science
Department of Emergency Medicine
University of Pennsylvania
Coursera
July 2012
An introductory course for the educated lay public and health care providers

Dr. Abella: conflicts of interest disclosures
Employment: University of Pennsylvania
Research funding: National Institutes of Health
Philips Healthcare
Medtronic Foundation
Consulting: Velomedix, Inc.
HeartSine Technologies
Volunteer: American Heart Association Sudden Cardiac Arrest Association
No equity or intellectual property related to resuscitation science

Refresher from Lecture 1: What is cardiac arrest?
Without any blood flow to the lungs or brain,
the victim of cardiac arrest is technically
“dead” and appears lifeless
(For brief minutes, may have “gasping” or
“seizure” activity)
The immediate actions required to restore blood flow:
1. Cardiopulmonary resuscitation (CPR)
2. Electrical defibrillation
Both of these can be done by the lay public

Refresher from Lecture 1: Survival from cardiac arrest is highly variable
Survival from cardiac arrest depends on where you live
From a large research study in 2008, showing survival to hospital discharge for victims of cardiac arrest:
Su
rviv
al to
dis
ch
arg
e
Dallas Pittsburgh Portland Seattle
4.5% 7.0%
10.6%
16.3%
Nichol et al, JAMA 2008

Why is survival so variable?
CPR is key to variable survival
In a given community:
Lay public factors:
How many people know CPR?
How many people deliver CPR?
What is the quality of the CPR?
Professional factors:
What is the time to professional CPR delivery?
What is the quality of professional CPR?

What do we know about CPR training among the lay public?
Many organizations offer CPR training:
American Heart Association American Red Cross
local training organizations
Millions trained each year, but most are health professionals
Performing re-certification
Imagine a map showing areas with High or low CPR training rates –
No such map exists!
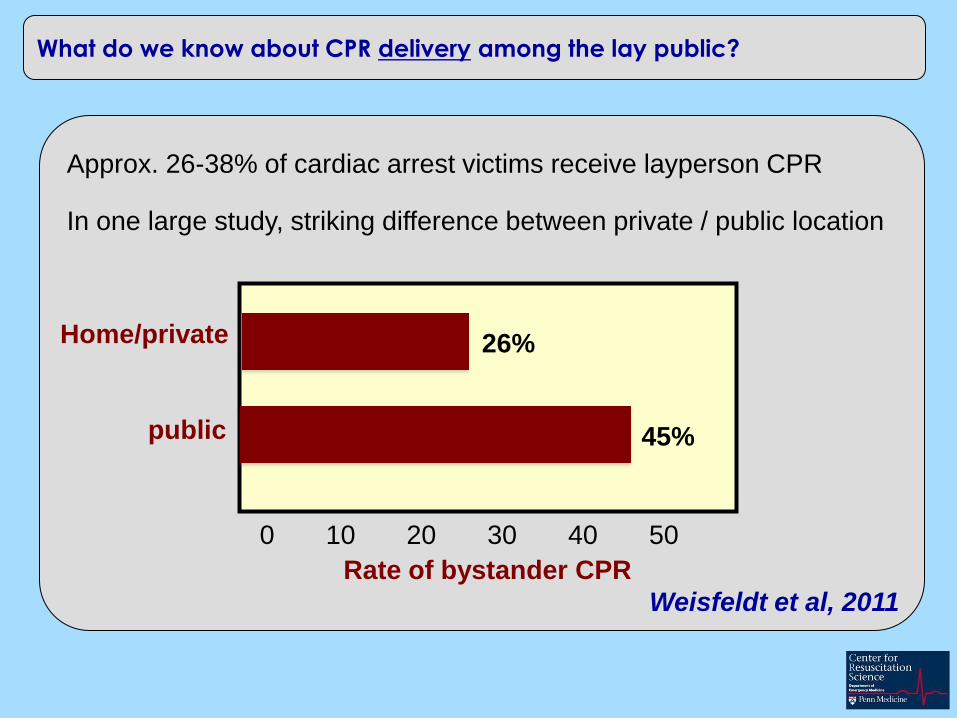
What do we know about CPR delivery among the lay public?
Approx. 26-38% of cardiac arrest victims receive layperson CPR
In one large study, striking difference between private / public location
Home/private
public
Rate of bystander CPR
0 10 20 30 40 50
26%
45%
Weisfeldt et al, 2011
The quality of CPR makes a big difference in survival
Study of CPR in New York City
Lay public CPR was observed by
arriving EMS professionals
CPR quality was judged as “high”
or “low” quality
Victims receiving high quality CPR were FOUR TIMES more likely
To be resuscitated
Gallagher et al, 1995

Detailed study by Ken Nagao et al (Japan)
In Japan, some regions had emergency dispatch
protocols that INCLUDED breaths, and some that OMITTED breaths
Should we provide breaths during CPR?
Important to note: study of bystander
CPR provided by the public, and the
CPR wasn’t measured….
Investigators asked: did it matter?

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
80
60
40
20
0
30
da
y s
urv
iva
l, %
Minutes from bystander CPR to defibrillator
Chest compressions only
standard CPR with breaths
SOS-KANTO et al, 2007
Breaths during public CPR don’t help, and they may hurt
Better survival with only
chest compressions, no
matter how long it took to
respond!

Bystander
contacted
9-1-1
survival to hospital discharge
11.5% 14.4%
standard CPR (n=960) chest compression alone (n=981)
The DETAILS of CPR delivery makes a big difference
CPR with chest compression alone or with rescue breathing
T Rea et al, 2010

Berg et al, 2001
Blo
od
pre
ssu
re
Time
= chest compression
Why pauses in chest compressions may be a bad thing

Berg et al, 2001
Blo
od
pre
ssu
re
Time
= chest compression
Few compression pauses lead to better blood flow







