
2/17/2015
1
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org
Root Cause Analysis
Joyce Black, PhD, RN, CWCN, FAAN
Background
• Process to determine why a problem
happened in the first place, so it wont
happen again
• Correcting the symptom alone is a waste
of resources
• Be aware of bias
– Intentional and unintentional
• Finding the root of the problem is not
easy work
– But if the latent source of the problem can be
found you can get rid of the problem©2015 National Pressure Ulcer Advisory Panel | www.npuap.org2

2/17/2015
2
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org3

2/17/2015
3
• Is this wound a pressure ulcer?
– Was it due to pressure?
– Was it due to shear?
• Is this wound on a previously healed PrU?
• When was this wound discovered?
– What size, stage, location?
– Due to a medical device? On mucous
membrane?
• What was risk score
– Was it accurate?
– Did a prevention plan stem from the score?
Starting with the pressure ulcer
• Stage at time of initial discovery
– Stage I --- likely began in last 12-24 hours
– DTI --- purple tissue without epidermal loss
likely began 48 hours ago
• Important because
– you might not have had this patient 48 hours ago
– Turning may have been impossible
» OR cases
– Stage II --- likely began in last 24 hours
– Stage III-IV --- began at least 72 hours ago
Determining the timing of the ulcer development

2/17/2015
4
• Pressure ulcers
skin on top of
buttocks cleft
• Patient was
supine at time of
pressure
– This is a DTI that
occurred in the
OR
Examine the location of the ulcer at discovery
• This patient’s
head was
elevated when
pressure
applied
– DTI nearer to
sacrum
Ulcer location

2/17/2015
5
• This patient was
lying on his side
when DTI
developed
– Ulcer on the side
of heel
Location of pressure ulcer
• If due to pressure, what preventive practices
were carried out?
– Turning? How often? What angle was the patient
off the surface?
• If the patient could not be turned was the surface
upgraded?
– Were heels elevated? Was elevation continuous?
– Was the surface upgraded due to high risk?
• Was the patient turned regardless of the surface?
• Is the surface working?
– Was the patient repositioned hourly in a chair?
• Was a chair cushion used?
• Was the cushion working?
RCAs continued

2/17/2015
6
• If due to microclimate…
• Was the skin kept clean and dry?
– Was incontinent urine and stool quickly
removed?
• Was the method of skin cleansing nonabrasive?
• Was the skin protected against next exposure?
– Was the skin moisturized?
– Was an incontinent brief removed for several
hours each day?
– Was a low air loss or microclimate surface
used?
RCAs continued
• If due to shear…
• Was the body areas subjected to shear
protected?
– Dressings on sacrum in HOB up patients?
– Padding in chair if patient slouches or is in
recliner chair
RCAs continued
2/17/2015
7
• If due to protein calorie malnutrition
– Was the patient hydrated and fed at the
dietician’s recommendations?
• Were supplements consumed?
• Was swallowing addressed?
• If not, was the deviation explained?
• E.g., Advanced Directives
RCAs continued
Looking at Human Roots
• Difficult aspect– beware of bias
• Consider competing priorities
– What is the unit of origin
• Predominately in ICU?
– How many actually started in OR? ER?
– Is the ICU bed designed for prevention?
• Examine training/competencies
– Are skin care/pressure ulcer competencies
done annually?
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org14

2/17/2015
8
Consider the patient
• If the patient is aware of the ulcer
– Does he know when it started?
– Does he know why it happened?
– Did he tell anyone?
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org15
This patient's DTI was
discovered when her stockings
were removed
What does she know about this
ulcer?
• Defined as volatile blood pressure and/or
oxygen saturation with movement
– It is not simply the use of vasopressive meds
– Concerns arise when document shows
patient moved for diagnostics or care, but
cannot be turned
• Can turning be done slowly?
• Can heels be elevated?
– Was surface upscaled to reduce pressure,
shear and microclimate?
– When on lateral rotation surface
• Was patient turned at all?
• Did bed do all the turning?
A closer look at hemodynamic instability
2/17/2015
9
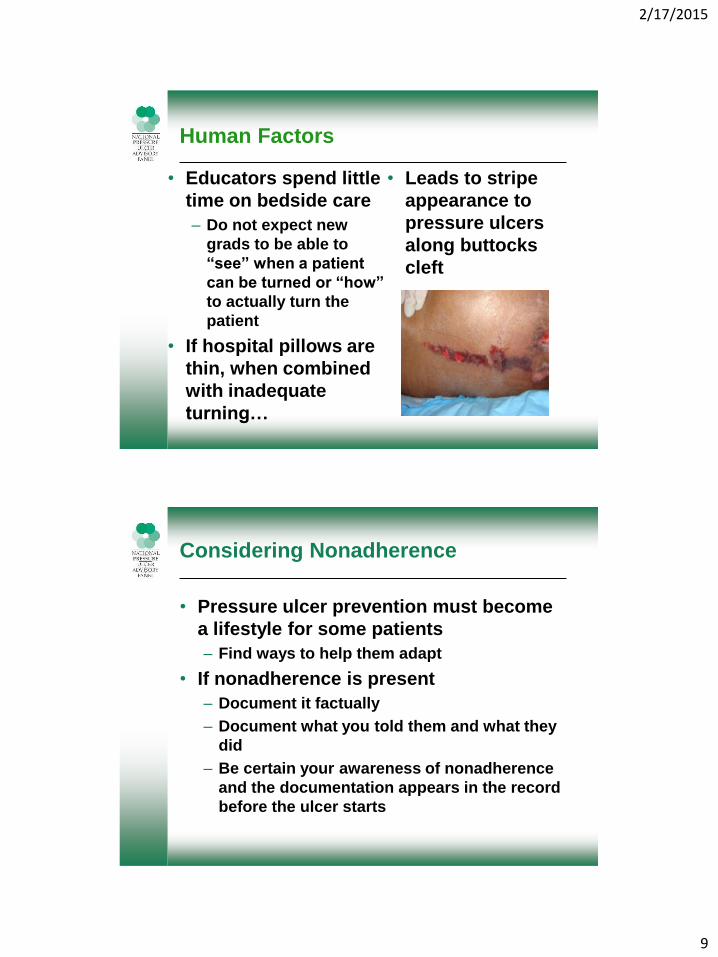
Human Factors
• Educators spend little
time on bedside care
– Do not expect new
grads to be able to
“see” when a patient
can be turned or “how”
to actually turn the
patient
• If hospital pillows are
thin, when combined
with inadequate
turning…
• Leads to stripe
appearance to
pressure ulcers
along buttocks
cleft
• Pressure ulcer prevention must become
a lifestyle for some patients
– Find ways to help them adapt
• If nonadherence is present
– Document it factually
– Document what you told them and what they
did
– Be certain your awareness of nonadherence
and the documentation appears in the record
before the ulcer starts
Considering Nonadherence
2/17/2015
10
• Classify as quality improvement to
reduce discovery
• Use the location and stage at discovery
to find the timing of the ulcer
– What was happening to patient at that time?
• Was pressure ulcer prevention possible?
• If yes, was it carried out? Documented?
Using RCA data
What are the latent roots in your pressure ulcer prevention system?
• Over reliance on beds
– Creating narrow ulcers along gluteal cleft
• PrU prevention not a priority
– “We are saving lives, we can’t worry about
skin”
– Under appreciation for seriousness of ulcers
• Lack of expectation for complete skin
assessment
– Ulcers beneath medical devices
– Ulcers found at more advanced stages
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org20

2/17/2015
11
Other Root Causes
• Lack of awareness and accountability for
– Policies and guidelines
• Prevention bundle
• Braden scale scoring
– Proper staging of ulcers
– Availability of supplies/devices
– Documentation issues
• Insufficient
• EMR issues
– Communication issues
• Nurse to nurse
• Nurse to others From Prince, 2010©2015 National Pressure Ulcer Advisory Panel | www.npuap.org21
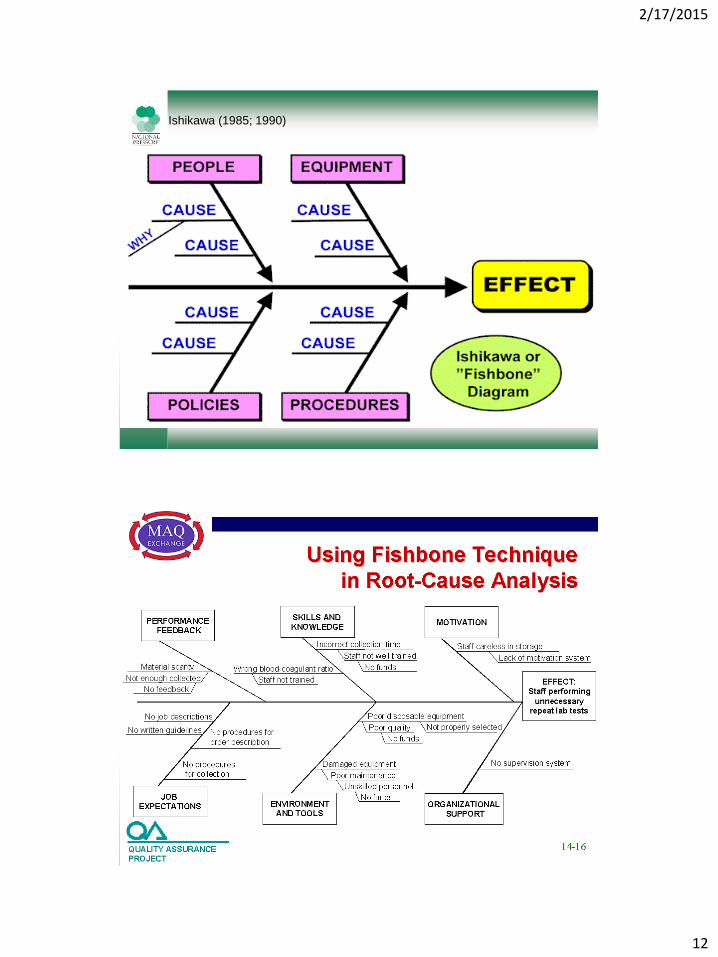
Bringing it all together
• Fishbone diagram helps to examine
– Performance and Feedback
• Are your unit pressure ulcer rates posted?
– Skills and knowledge
• Are you including skin in yearly competencies?
– Motivation
• Are staff recognized for “a job well done”?
– Job expectations
• Are policies and procedures current? Accessible?
– Environment and tools
• How old are your beds on the units?
– Organizational support
• IS CNO on board?©2015 National Pressure Ulcer Advisory Panel | www.npuap.org22
2/17/2015
12
Ishikawa (1985; 1990)
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org24

2/17/2015
13
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org
Root cause analysis has to be done with rigor in order to find the true roots
©2015 National Pressure Ulcer Advisory Panel | www.npuap.org25







