Role of the Psychiatric Mental Health Nurse Practitioner in the Future of Health Care
Kathleen R Delaney, PhD, PMH-NP Rush College of Nursing
Thank You!

Change is coming in health care
Climate for change: High spending/ poor outcomes
Affordable Care Act is the lightening rodBecomes the language everyone is speaking: Access
PreventionCost-effectiveness.
Federal government reports set the stage
Pressures on mental health care have never been greater
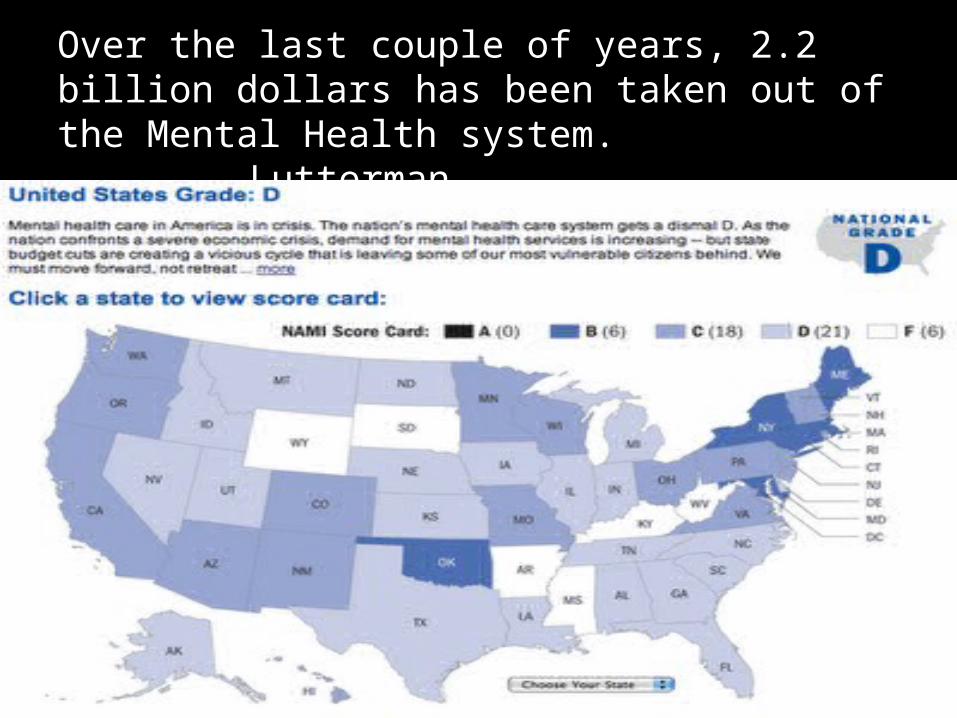
Over the last couple of years, 2.2 billion dollars has been taken out of the Mental Health system.
Lutterman
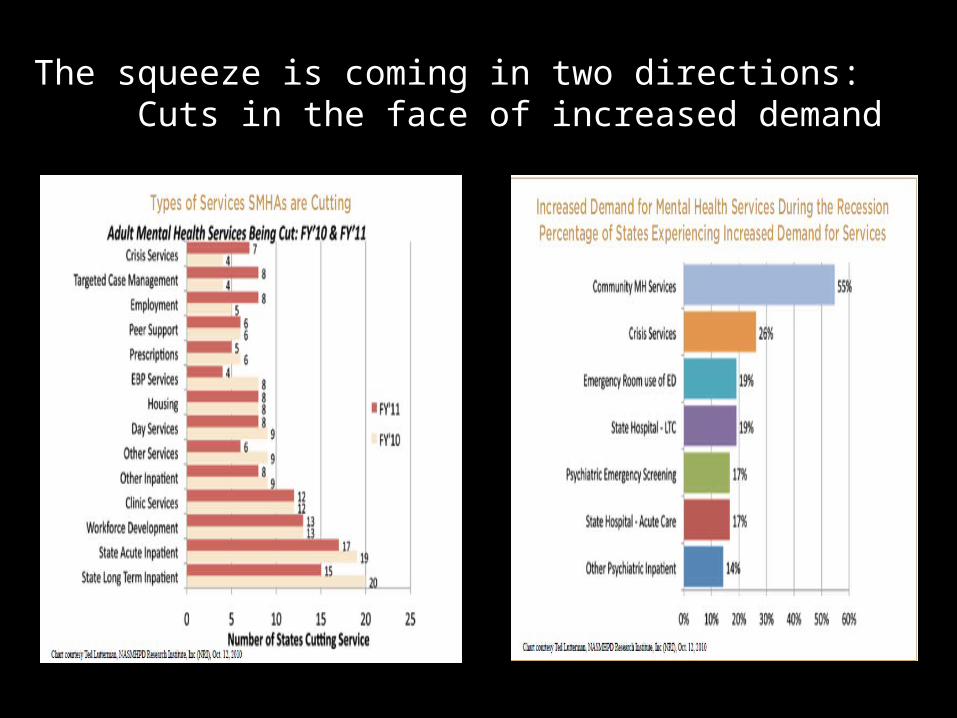
The squeeze is coming in two directions: Cuts in the face of increased demand
Major areas of Change in MH Care • Managed care will become ubiquitous in Medicaid programs in
order to improve quality and to contain costs. Self directed type management via performance adjusted care and capitation
• Integration of care will become ubiquitous in Medicaid programs, and social services will likely be included. Integration of services should be paid for through carve out funding in order to protect behavioral health services.
• Disease prevention and health promotion programs will become ubiquitous in Medicaid programs to save downstream costs, and these services will be provided to enrolled persons who do not have a current disease condition, as well as to those who do.
• Manderscheid, 2012
A good hockey player skates to where the puck is, a great hockey player plays where the puck is going to be. Wayne Gretzky
Pivotal Moment for PMH Nursing To Establish their Role In Emerging Models
Guild reason: 350,000 Behavioral Health Specialists looking to find a place
Moral reason: Have the educational preparation of make these systems effective, equitable and responsive
Premise: Armed with an understanding the reform playing field, where change is
occurring- we can effectively deliver core messages about our practice
Emphasizing why PMH nursing skills fit with emerging models in MH care
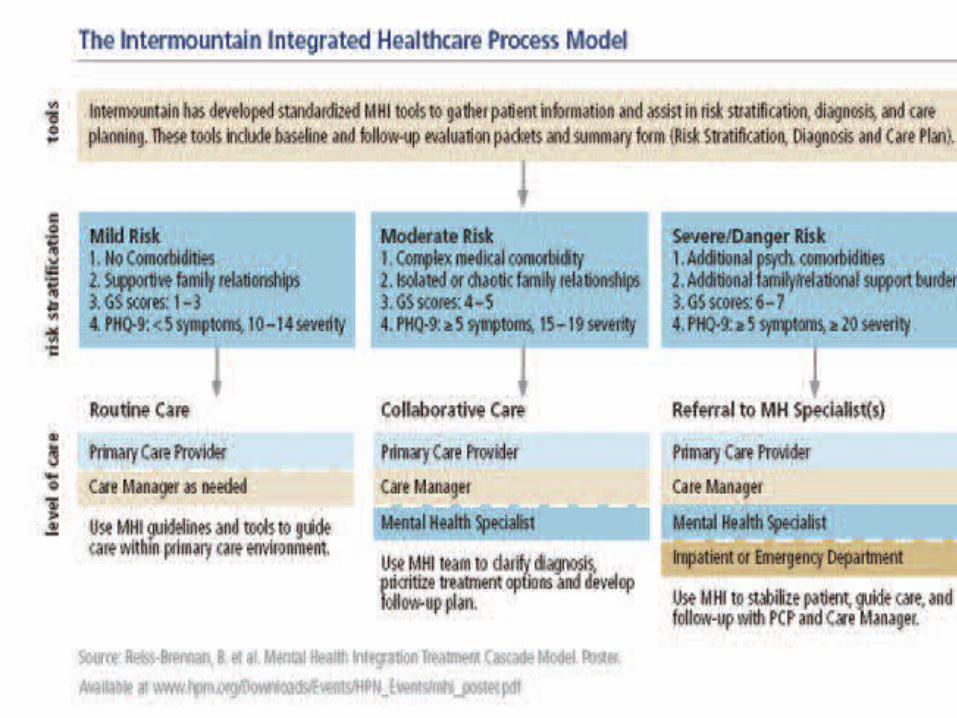
Knowing Direction of Health Care Reform: Integrated care
Who is pushing the agenda and what is their power?
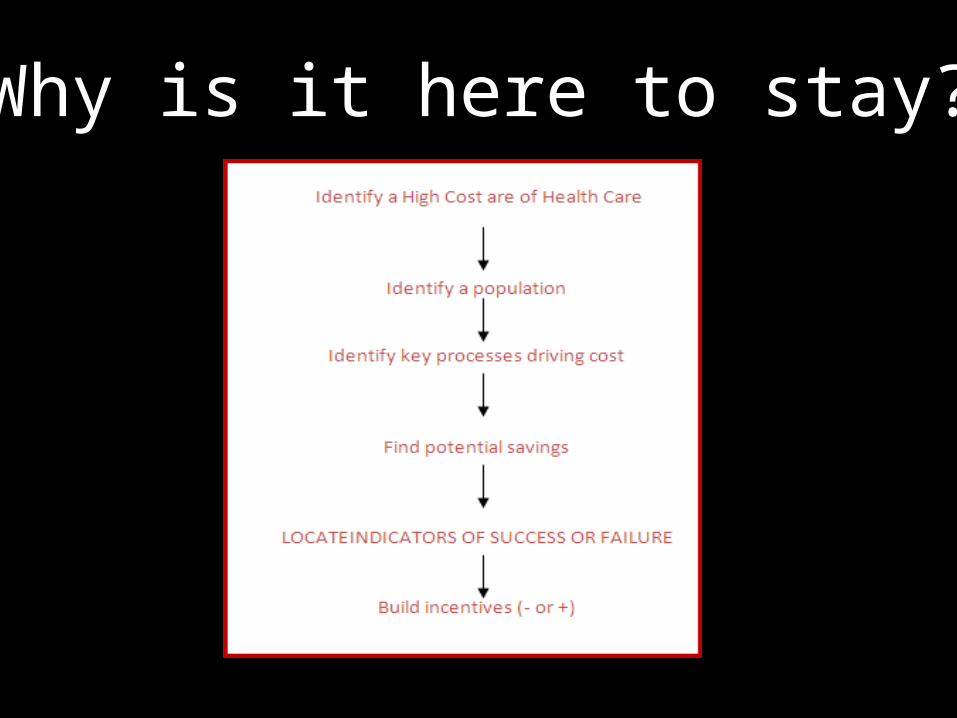
Why is it here to stay?
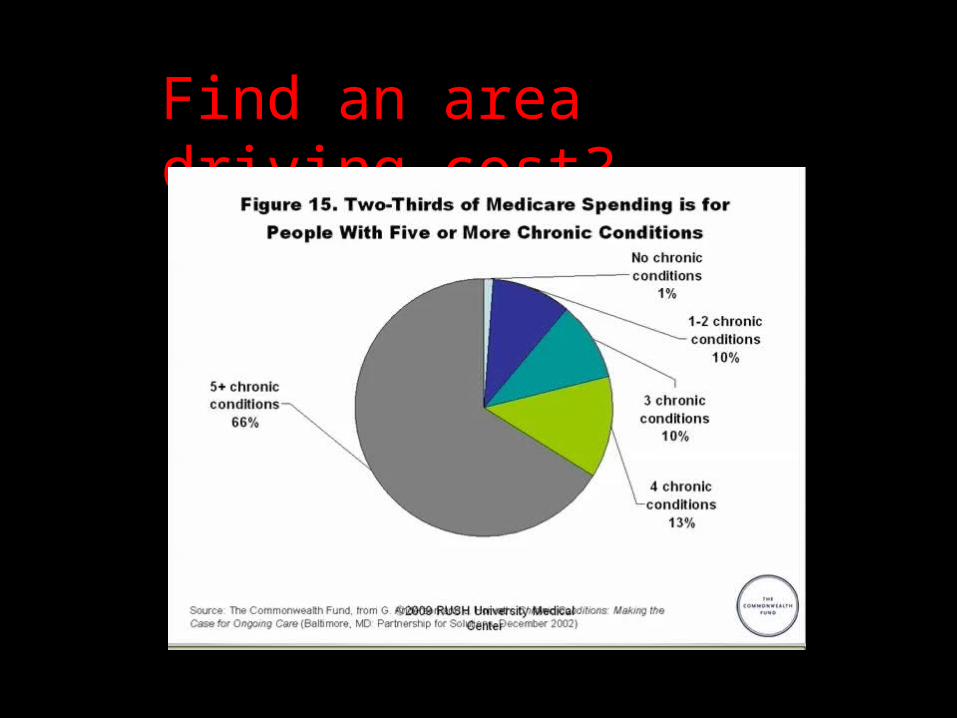
Find an area driving cost?
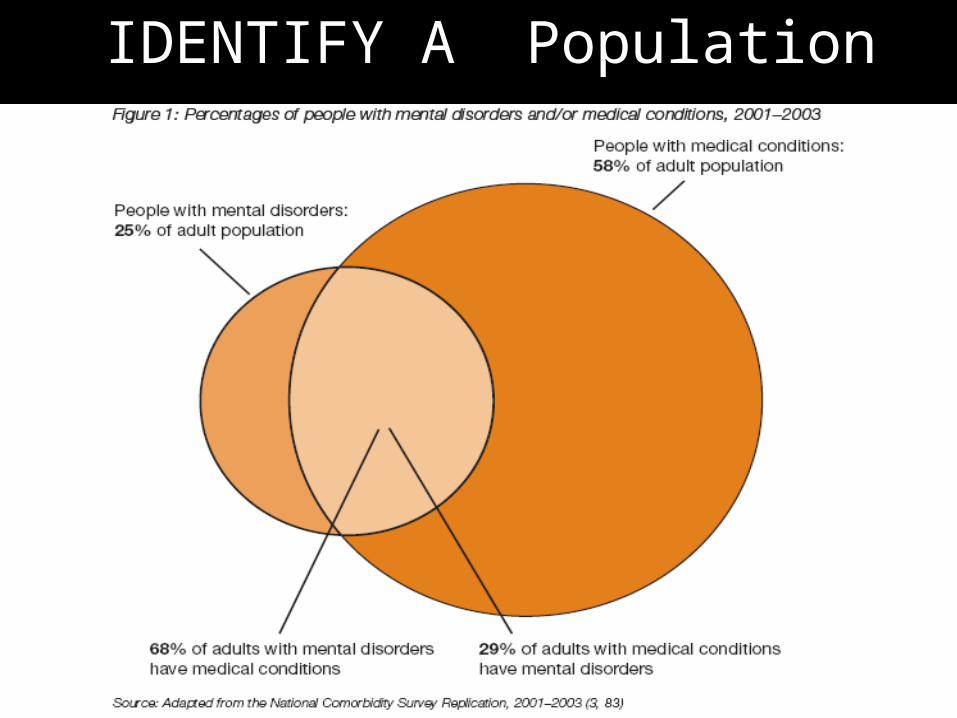
IDENTIFY A Population
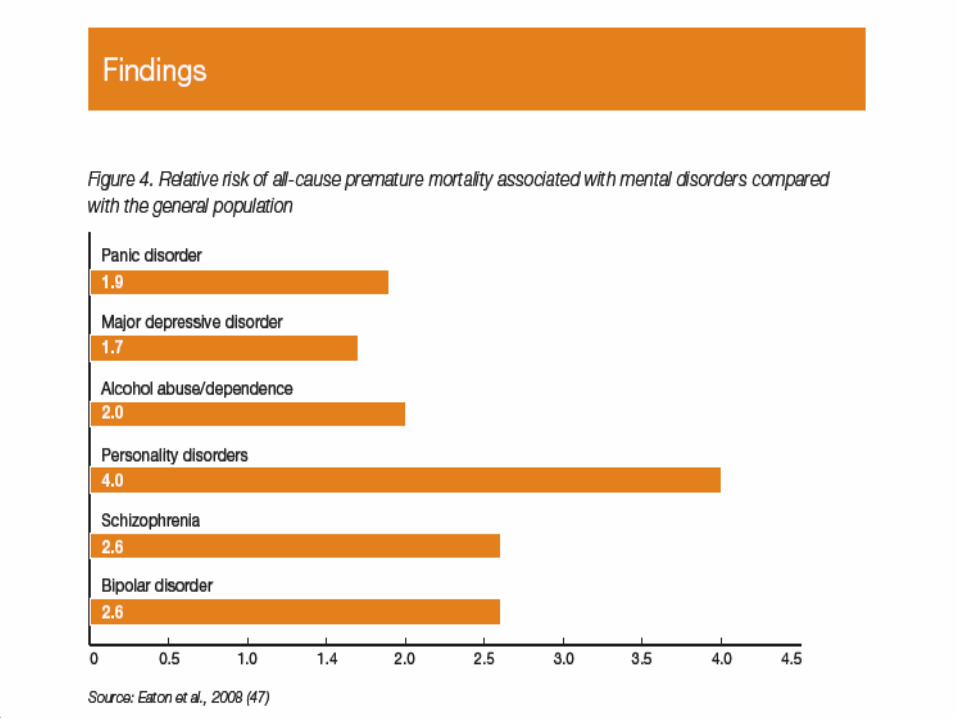
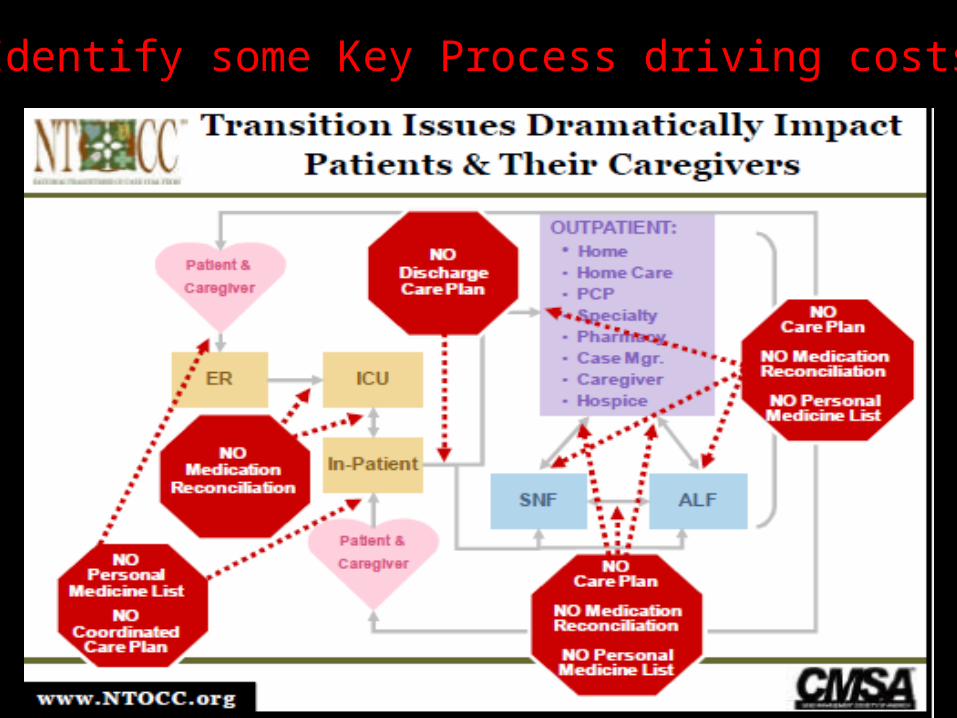
Identify some Key Process driving costs
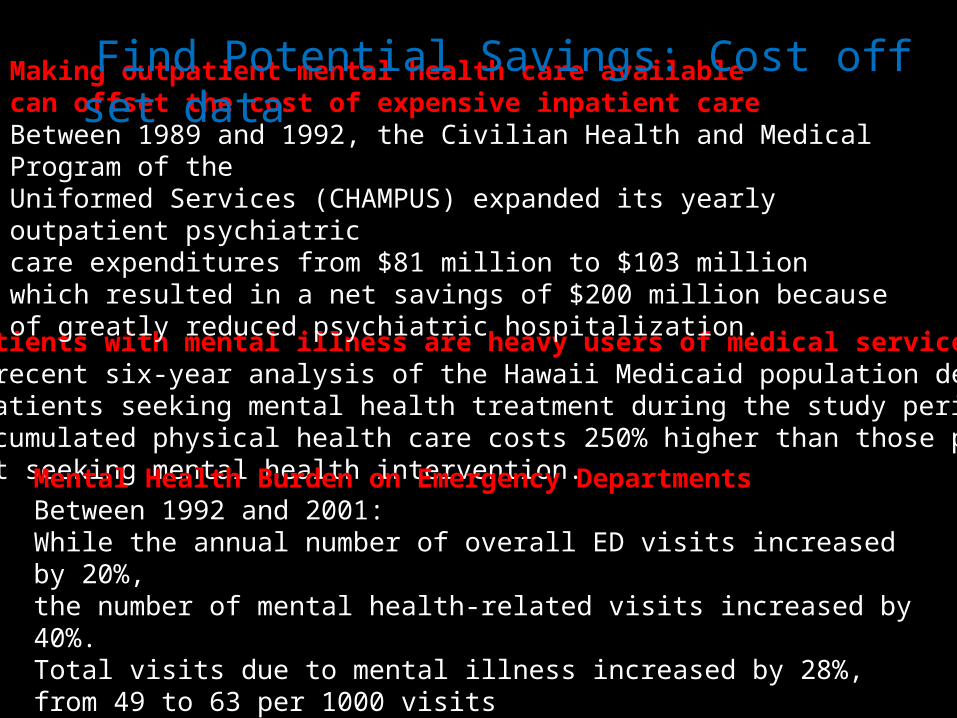
Patients with mental illness are heavy users of medical services A recent six-year analysis of the Hawaii Medicaid population demonstrated patients seeking mental health treatment during the study period aaccumulated physical health care costs 250% higher than those patients not seeking mental health intervention.
Making outpatient mental health care available can offset the cost of expensive inpatient care Between 1989 and 1992, the Civilian Health and Medical Program of the Uniformed Services (CHAMPUS) expanded its yearly outpatient psychiatric care expenditures from $81 million to $103 million which resulted in a net savings of $200 million because of greatly reduced psychiatric hospitalization.
Mental Health Burden on Emergency DepartmentsBetween 1992 and 2001: While the annual number of overall ED visits increased by 20%, the number of mental health-related visits increased by 40%. Total visits due to mental illness increased by 28%, from 49 to 63 per 1000 visits by 40%.
Find Potential Savings: Cost off set data
Locate Indicators of Success: Exemplars
Volume: In 2010 GHS served 3,202 unduplicated clients (UDC) for 17,112 visits (UDS) (40% primary diagnosis mental /behavioral health visit). Services Provided: Four integrated modalities: Primary Care; Mental Health: mental health evaluation and counseling, therapy and medication management, substance abuse group visits; Complementary Care: acupuncture, chiropractic, and HIV/AIDS: HIV risk reduction counseling, testing and linkages (CTL).
Two Indicators that demonstrated improvement in 2010:
Immunization rates from 7% of clients to 27%
Hemoglobin A1c improvements N=194 patients , Average A1c = 7.7 (down from 8.0 in June)
In 2010 Glide was funded through HRSA Bureau of Health Professionals (BHP) Division of Nursing as one of ten funded NMHCs nationally and a second grant to open a Wellness Center at GHS. In 2008 HRSA BHP Division of Nursing awarded GHS for “Expansion of GHS NMHC “(D11HPO9564) for five years (2.7 M). The total of HRSA BHP funding for the past three years is 5.7 M !
Exemplars: MARRY MESSAGE WITH DATA
Quality Improvement via Health Information Technology Patricia Dennehey, DNP, FNP, RN
Build an Incentive Structure:The federal government pays FQHCs for the cost of care they provide toMedicare and Medicaid patients, turns out to be the actual cost of care so it is a higher rate. (not a fixed rate price)
Deliver Core Message about our practice
Fit of our skills with the emerging issue
Message: Our educational preparation and core capabilities fit with the integration of health care and medical care
• Medical• Psychiatry• Relationship • Neuroscience• Psychotherapy• Prevention
Message: Why PMH NPs Fit with Integrated Care
• The broad base of sciences they operate from creates -an innate integrated science base
• Creates critical competencies for integrated care • Capable of monitoring the Axis III conditions, thus
manage an integrated treatment plan• Understand medical follow up instructions• Understand how medical and behavioral issues create
intensity of need/intensity of services • Address health issues with understanding of how SMI
brings with it behaviors that impact how issues addressed, i.e. poor sleep, poor eating.
Capable of driving a treatment culture of Person-Centered Care
Patient-centered care
Health care that establishes a partnership among practitioners, patients, and their families (when appropriate) to ensure that decisions respect patients’ wants, needs, and preferences and that patients have the education and support they need to make decisions and participate in their own care
IOM
TRIPLE AIM Improving the experience of care,Improving the health of populations, Reducing per capita costs of health care
Mental Health Care: Patient centered care is interwoven with recovery
Recovery process and methods not so developed for inpatient care
Recovery is the common language of Mental Health Care
Hope is both triggers and sustains recovery
Four key attributes of patient-centered care
"Whole-person" careCoordination and communicationPatient support and empowermentReady access
Bechtel, 2011
Recovery and Patient-Centered Care are familiar to PMH Nurses : Take a twist
Holistic
Strength-BasedRespectHope
Built on continuous healing relationships.
Provided in a healing environment of comfort, peace, and support.
Patient safety is a visible priority.
A prerequisite of any environment which aims to nurture hope is the cultivation of compassion
Spandler and Stickley, 2011
Compassion not so much a trait….
In providing Safety,CareSupportEncouragementAffection-
We create a compassion context
Vision: MH system that provides compassionate contexts so clinicians Educate -Encourage- Empower
Anthony, 2006
Bring the best and latest research to mental health consumers: never ending flow of information
Many Consumers have found the fire they need to see hope –via relationship and attitude we provide constant encouragement
Consumers can then use this information to make their own decisions- empower
The issue will be how can we kindle these elements by establishing the contexts necessary for education, encouragement and empowerment
The first characteristic of professional nursing is the focus on the patient. .. The exclusive focus on the patient is to get to know the patient’s view of self and the predicament- the way it looks to the patient- so that the patient can see it too.
Peplau
We have particular skills at creating presence and resonance
• With affect mirroring the nurse matches the patients affect
• Via eye contact and non verbal language the nurse connects to the affective level of presentation
• Via gaze and mannerisms the PMH-NP and
patient also share intent • These processes set up collaborative
communication ; the fine tuning of responses where eye contact, facial expressions and gestures are in sync, allowing both the infant and parent to “feel felt” by the other
I am here available, listening
Message: we shape opportunities for Attunement
Each moment with a patient is an opportunity for attunement, mirroring, mentalizing- pay attention on purpose to the patients state of mind
Patient Centered-Care : Appreciating how stories weave into a Patient’s narrative
Our interpersonal processes also centers on how nurses empower people by helping them tell their story: “exploring and developing the meanings and values the person attaches to or associates with his or her experience”
Phil Barker
Two Emerging Elements bring a new language to the Interpersonal Process
Patient Centered Care
Interpersonal Neuroscience
And bring us back to Peplau
Other half of the argument:PMH-APNs are well equipped to shape compassionate environments necessary for patient
centered care
• Know the patient and how to access narratives of illness, meanings and what is important
• Know how to navigate between every day needs and the broader picture of treatment
• Know how to instill the therapeutic optimism requisite for recovery
• Understand how stigma operates
PMH-NPs : Envision yourself as a disruptive influence on health care landscape
• Build effective integrative care models • Becoming a specialist in prevention and
journeying with individuals to seek health• Partner with inpatient nurses to build innovative
transition models • Bring DNP students into your practice to build
the data systems that will work for you- to demonstrate your work and build evidence for integration “done right.”
What’s Tomorrow?
• Nurse Navigators, PMH emergency room specialists- that are not necessarily APNs
• Care Coordination Roles• Bringing mental health expertise to
communities so they might build mental health • Disruptive innovations that deliver greater
access to care at reduced cost• Outcomes focused on the patient experience
Does integrated care address systemic barriers to SMI population achieving health and wellness
Do some models support better integration of services and informationAre Health Care providers’ attitudes and behaviors around stigma reduced Are the consequences of life style and medication side effects on health
effectively addressed
What are effective mechanisms for addressing these systemic issues Co-location of physical and mental health servicesUse of case managers or other staff to undertake a co-ordination or liaison role between services. Programs aimed at reducing the stigma of mental illness.
-How to respectfully consider the cognitive deficits and consequences of SMIhealthcare skills training to people with SMI peer supporters.
-How to develop population health and health promotion approaches targeted at SMI-How to deal with issues of social inclusion
Brown et al, 2010
Evidence to support effective integrated care

Pivotal moment in health care: Learn to read policy landscape
Integrated Care
Clear about our Message• What is needed in these systems of care• Message embraces our fundamentals•Articulate the fit of your skills and service system
Summary







