
Report to Trust Board – 3 March 2016Report Title Vanguard programme – value propositionReport from Johanna MossPrepared by Karen ReevesList of attached appendices (ifapplicable)
Moorfields value proposition 2016/17
Reference documents (e.g.previous reports orappendices NOT attachedherewith)
1. Brief Summary of ReportFurther to its successful application to become an Acute Care Collaboration vanguard site,Moorfields submitted an initial value proposition seeking funding for the remainder of2015/16. We were successful in receiving the full amount sought (£155k).
On 8 February the Trust submitted a second value proposition for 2016/17. This documentreflects our progress since December, including further detail of the individual work streamsand development of a hypothesis tree for our vanguard programme. The total amount offunding requested for 2016/17 is £1.9m.
The national programme team will confirm funding allocations to each vanguard site in mid-March.
Moorfields’ has appointed a Vanguard Programme Director (Karen Reeves) and will beinterviewing for a Vanguard Clinical Lead in the next few weeks. Until 2016/17 funding isconfirmed, work is progressing with interim support in other programme roles. The first keymilestone is to complete a review of previous satellite mobilisations in order to collatelearning and identify key themes which matter most to staff and patients. This will bedelivered by the end of March.
2. Action Required/RecommendationThe Trust Management Board is asked to note the content of the value proposition,anticipating confirmation of any funding awarded for 2106/17 by mid-March.
Item 5(i)

Vanguard programme:
Acute care collaboration
Value proposition 2016-17
8 February 2016

ACC Vanguard: Moorfields Eye Hospital Value Proposition 2
Contents
Section Page
Section 1: Introduction 3
Section 2: Our context 4
Section 3: Vanguard aims, outputs, programme logic model and value hypothesis tree 8
Section 4: Our programme 12
Section 5: Financial impact and costs 16
Section 5: Our proposed support package 23
Section 6: Summary and conclusion 25
Appendix 1: Workstream logic models 26
Appendix 2: Value generation assessment 29

ACC Vanguard: Moorfields Eye Hospital Value Proposition 3
Section 1: Introduction
Moorfields Eye Hospital NHS Foundation Trust
Moorfields is the leading provider of eye health services in the UK and a world-class centre of excellence for
ophthalmic research and education. Our main focus is the treatment and care of NHS patients with a wide
range of eye problems from common complaints to rare conditions that require treatment not available
elsewhere in the UK. Our unique patient case-mix and the number of people we treat mean that our
clinicians have expertise in discrete ophthalmic sub-specialties. In 2014/15 we saw more than half a million
patients in our outpatient services and carried out almost 40,000 surgical procedures, making Moorfields the
largest ophthalmic provider in the UK. We also provided care to 96,000 patients in our A&E department. We
treat people in 32 locations in and around London enabling us to provide expert treatment closer to patients’ homes. We also operate commercial
divisions that provide care to private patients in both London and the Middle East.
Moorfields’ innovative approach to delivering care across multiple satellite sites has been explicitly referenced in recent national policy. The Five
Year Forward View highlighted the benefits of our model in helping to sustain local hospital services and enable smaller hospitals to remain viable.
The Dalton Review categorised our approach as a contractual arrangement which it described as a service-level chain. More recently, the
Moorfields@ model has been cited as an example of franchising or networked care. Terminology will be important as we seek to describe the
models that could be replicated across the NHS. In this value proposition we use the term ‘networked care’ to describe the generic model of
collaboration between providers and the term ‘satellite model’ to describe the approach currently delivered by MEH.
Rationale for our vanguard
Acute hospitals face increasing challenges to deliver safe and cost effective care, especially in smaller clinical specialties such as ophthalmology
which often lack the benefits of scale in a local setting. In the absence of a critical mass of patient numbers or specialty workforce, provision of
care may become clinically or financially unsustainable. These difficulties are often compounded by competition generated by local commissioners
and other providers. Moorfields has developed a satellite model that provides clinically and financially sustainable local access to high quality
ophthalmic care and a sustainable model of specialist treatment. We believe that the Moorfields satellite model has potential replicability across
the acute healthcare system and a key part of our vanguard will be to gather data to test this view. The aim of our vanguard is to consolidate our
learning in delivering networked care so that we and the wider NHS can develop a clear understanding of when and how this model of care can
enable acute hospitals to become clinically and financially sustainable.
We want to describe what good looks like for networked care and how it can be implemented successfully across the NHS.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 4
Section 2: Our context: ophthalmology as a case study of the sustainability challenge
Moorfields was an early adopter of the principle that where appropriate clinical services should be provided within local communities, establishing
high quality local eye centres where possible. We are recognised as an exemplar of a specialist provider working in a new and innovative way to
deliver local services to residents outside the acute hospital environment. We now treat people at 32 sites in and around London, which are shown
on the following map and described on page 6.
Ophthalmology in the NHS has a particular set of sustainability and quality challenges which can be described in terms of the three ‘gaps’:
Finance and efficiency: Most ophthalmology care is provided in acute hospitals where it is a relatively small speciality where small volumes of sub-
speciality care can mean there are critical mass issues. Many commissioners have sought to drive down costs and increase competition for cataract
services (the most common surgical treatment) which has resulted in a proliferation of sub-scale, poorly co-ordinated and unsustainable services. The
challenges to sustainable local ophthalmology services include rising costs, poorer access and lack of improvement in care.
Care and quality: There is evidence of variation in the clinical outcomes and effectiveness of eye care across acute hospitals that is not always
revealed or improved through local clinical governance arrangements that focus on multiple specialities. Opportunities to develop new treatments and
participate in research can be missed.
Health and wellbeing: Eye disease is linked with ageing and eye care is particularly important to older people. Any loss of local services, travelling
further for care and poorer support to chronic care will have a considerable negative impact on older people.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 5
Contains: Ordnance Survey data © Crown copyright and database right 2012, Royal Mail data © Royal Mail copyright and database right 2012
Contains: Ordnance Surv ey data © Crown copy right and database right
2012, Roy al Mail data © Roy al Mail copy right and database right 2012
Bedford
South
Bedford
North
Contains: Ordnance Surv ey data © Crown copy right and database right
2012, Roy al Mail data © Roy al Mail copy right and database right 2012

ACC Vanguard: Moorfields Eye Hospital Value Proposition 6
The Moorfields satellite model provides eye care from 32 sites
City Road campus
Provides comprehensive general and specialist outpatient, diagnostic
and surgical services, emergency surgery and a 24-hour A&E.
5 Moorfields@ district hubs
Co-located with general hospital services, these eye centres provide
comprehensive outpatient and diagnostic care as well as more
complex eye surgery.
6 Moorfields@ surgical centres
Providing more complex outpatient and diagnostic services alongside
day-case surgery for the local area.
15 Moorfields@ community outpatients
Focusing on outpatient and diagnostic services in community-based
locations closer to patients’ homes
5 Moorfields@ partnerships
Providing medical and professional support to eye services managed
by other organisations, as well as providing clinical leadership to
various diabetic retinopathy screening services
Our satellite model has grown in a largely unplanned way, driven by
commissioner and provider requests. Our approach to assessing
each new business opportunity and implementing our satellite model
has not been standardised.
We have been approached by several organisations to provide advice
to their eye units, including some who explicitly request
implementation of the Moorfields@ model. We recognise that
extending our satellite model is not appropriate in all circumstances
and therefore tailor our input. As a result, we also have extensive
experience of providing advice and consultancy to partner
organisations.
There is clinical and managerial consensus that we would benefit
from standardising our approach to assessing new business
opportunities and implementing our satellite model. Some progress
has been made in codifying our clinical pathways as well as
developing an opportunity analysis template.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 7
Wider applicability of the Moorfields satellite model across the NHS
The issues described above in relation to ophthalmology are often applicable to other clinical specialties. The pressures facing smaller district
general hospitals are often complex. It is increasingly difficult for these organisations to afford to deliver high quality care across all clinical
specialties and sub-specialties. Understandably, smaller clinical specialties are rarely a high strategic or operational priority in such hospitals. The
sustainability of some smaller clinical services can be called into question by a range of factors which relate to the size and scale of the service;
Low patient volumes
This will often mean an organisation is not able to provide a full range of sub-specialty expertise, resulting in patients being referred to another
provider for more complex diagnosis or treatment. This can mean patients wait longer for treatment as well as travelling further to access
care. Low patient volumes for certain conditions can be associated with poorer outcomes.
Isolated workforce
Any service which requires specialist staff to deliver complex care on a small scale is placing pressure on its workforce. There are limitations
on the peer support available for clinicians (including training and clinical case review), issues of de-skilling planned and unplanned staff
absence can threaten the sustainability of the service. This can impact on professional development as well as the quality of care provided.
Investment in capital equipment.
For equipment-intensive specialties, it can be difficult for smaller organisations to justify the financial investment in specialist equipment.
Despite these challenges, patient and commissioner expectation is that wherever possible a comprehensive range of services should continue to
be provided locally. It is important to note that while delivering networked care can present a solution to many of these issues it can also create
new challenges to safety and the balance between standardisation and local flexibility. Our vanguard programme will examine these issues.
Opportunistic commissioning and provider competition can create barriers to transforming services as finance tends to be favoured over
sustainability and competition over co-ordination. Without a plan to adequately fund and develop specialist and tertiary services, the proliferation of
these sub-scale and potentially unsustainable services takes no account of the impact this is likely to have in the longer term.
The aim of our vanguard is to consolidate our learning in delivering networked care so that we, and the wider NHS, can develop a clear
understanding of when and how this new model of care can support hospitals in becoming clinically and financially sustainable.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 8
Section 3: Vanguard aims and outputs
What are we trying to achieve? We want to consolidate our learning in delivering networked care so that:
the NHS can develop a clear understanding of:
(a) when and how this new model of care can support acute hospitals in becoming clinically and financially sustainable
(b) the implications of extending models of networked care more widely across the service
we, as Moorfields, can deliver sustainable ophthalmology services that meet the needs of local populations and are delivered in an effective
network
We have identified three long-term impacts that our vanguard programme will deliver:
1. Patients will have greater access to locally delivered, clinically sustainable services
2. Acute hospitals will become more sustainable by working with partners in a network model(s)
3. Networked care will be supported by effective and sustainable governance structures, underpinned by a strong organisational culture.
We want to undertake further analysis of the factors that make us more effective in some settings. We’re keen to learn what makes the biggest
difference for patients, staff and partner organisations in getting things right first time when establishing a service in a new setting. By learning from
other NHS organisations, as well as our own, we will codify the optimal approach to establishing and sustaining networked care. This will enable
the NHS to implement such models at pace and scale, realising the benefits of clinical and financial sustainability across the system more quickly.
We will undertake a comprehensive assessment of the opportunities and risks associated with an extended networked care model, learning from
our own and others’ experience. This will consider both increasing the number of satellite sites as well as widening the geographic reach of the
organisation.
We will describe, evaluate and share the learning from our work so that it can be replicated and used across the NHS.
ACC Vanguard: Moorfields Eye Hospital Value Proposition 9
The outputs of our work Our programme will deliver two key outputs, which will deliver benefits for the wider NHS, and for Moorfields:
A toolkit that codifies best practice in establishing the need for and implementing networked care and describes the critical success factors
required for it to succeed.
A publication outlining how the models of networked care can be extended while delivering clinically and financially sustainable services that meet
the needs of local populations.
From our experience to date, we anticipate that this will include recommendations on how to:
ensure consistent quality of care (including clinical outcomes, safety and patient experience) across multiple sites
deliver a sustainable workforce model
develop equitable educational and research opportunities for staff and patients
maintain effective partnership working with numerous providers and commissioners
protect organisational reputation
sustain the local delivery of subspecialist activity in a way which is both clinically and financially viable
balance the need to centralise (to achieve standardisation) and devolve (to achieve localisation)
For the wider NHS our programme will deliver:
a description of what good looks like for networked care
a toolkit that can be used to establish successful models of networked care in other locations
a summary of the implications of extending models of networked care more widely across the NHS.
The analysis will be available to inform national policy development and implementation in relation to viable smaller hospitals.
For Moorfields these outputs and the wider vanguard programme will enable us to determine the next phase of our service planning including:
where we should provide services in the future, how we can work with stakeholders to plan for all of the eye care for a population, how we should
partner and work with other providers, the governance arrangements required for high quality services across growing and dispersed networks,
and the organisational structures that can support this new model of care to be high performing, with a good culture and good reputation.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 10
Logic models for the three workstreams are included at appendix 1.
Activities Outputs
Network Analyses Identify the conditions under which networked
care works well and when it doesn’t. We will work with new systems in different parts of the country
to explore how Moorfields could support the
planning and delivery of networked care
Toolkit that codifies best practice in establishing the need for and implementing networked care
Analysis of how networked care is responsive to and meets the needs of local populations
A publication outlining how the networked care model can be extended whilst still delivering
clinically and financially sustainable services
Outcomes
Rationale District general hospitals are facing increasing challenge to deliver safe and cost effective care, especially in smaller clinical specialties which often lack the benefits of scale in a local setting. In the absence of critical mass of
patient numbers or specialty workforce, provision of care may become clinically or financially unsustainable. These difficulties are often compounded by competition generated by local commissioners and other providers.
Moorfields’ satellite network model has potential replicability across the acute healthcare system. The aim of our vanguard is to consolidate our learning in delivering networked care, in collaboration with other NHS and commercial
providers, so that the NHS can develop a clear understanding of when and how this new model of care can support DGHs and health economies to be clinically and financially sustainable for small specialties like ophthalmology.
Impacts
Understand existing models Describe and define the different models of
networked care already in place in Moorfields and those used elsewhere across the NHS.
Assess existing models Assess and review the existing Moorfields models
of networked care related to clinical quality and operational effectiveness, accessibility, patient
experience, staff wellbeing, organisational culture
and activity levels
Review international networks Research and/or visit examples of successful
networks in healthcare and other industries.
Undertake stakeholder review Engage with stakeholders, including patients,
staff, provider partners and commissioners in order to assess the quality and reputation of the
existing models of networked care in Moorfields
Detailed market analysis Map activity levels and patient flow at a provider
and commissioner level across the Moorfields network, and compare the output with local
population needs assessments
Review networked care opportunities
Test the feasibility and implications of stretch
Accelerated establishment of satellite networks across the NHS
Better care for patients delivered by standardising care, improving accessibility and
minimising waste across the system
Reduction in start-up costs to establish a satellite network
More efficient use of resources through establishing satellite networks
Better decision making for organisations considering a networked care model
Replicability of best practice in delivering networked care
Widespread understanding of the benefits arising from different forms of networked care
Delivery of sustainable ophthalmology services that meet the needs of local populations and are
delivered in an effective network
Networked care will be supported by effective and sustainable governance structures, underpinned
by a strong organisational culture
Patients will have greater access to locally delivered, clinically sustainable services
Acute hospitals will become more sustainable by working with partners in a network
Critical success factors that need to be in place across a network in order for it to succeed
Better understanding of the commissioning implications arising from widespread adoption of
networked care
Moorfields vanguard programme logic model

ACC Vanguard: Moorfields Eye Hospital Value Proposition 11
Value generation hypothesis tree
The value generation assessment is included at appendix 2.
Clinical outcomes will be improved through replicating
best clinical practice across a
network.
Our vanguard will evaluate and consolidate learning from examples of networked care to identify the conditions which need to exist to make it effective and develop a toolkit which will enable the NHS to benefit from a more accelerated approach to setting up network models of care.
Patient experience will be enhanced by standardising
care and improving access
across a network model.
Safety and quality will be assured through setting and
spreading best practice
across the network.
Resource requirement of additional ~£1.959m in
16/17 is reasonable to
deliver the outputs and
generate the value of the programme.
Sustainability for the NHS will be improved through the
utilisation of the outputs by
organisations considering a
network care model.
• Describing and publishing the benefits of networked
care for safety and patient
experience will allow:
§ systems to understand and replicate best practice for patient
experience.
• £1.959m is the cost of delivering the programme
activities: § Programme management £651k
§ Existing models £43k
§ Assess existing models £745k
§ Stakeholder review £53k
§ International review £48k
§ Network analysis £218k
§ Network opportunities £201k
• £12.9m is the value of the knowledge, experience,
expertise and time being contributed to the national
vanguard programme.
• Disseminating lessons on safety and quality learnt
across the network will
ensure: § wider reach and application of
speciality specific lessons, resulting in faster adoption of
any changes to practice.
• Providing a clear, systemised approach to
spreading best clinical
practice across other sites
will allow:
§ systems to understand and
replicate best clinical practice.
• Providing a clear set of critical success factors for networked
care and comprehensive ‘how
to’ guide toolkit will result in:
§ reduced time for trusts to appraise options for forming or joining networks
of care.
§ more effective design and
implementation of a networked care proposal.
Impact
of
outp
uts
of
vanguard
pro
gra
mm
e
Impact
of im
ple
menting a
netw
ork
ed m
odel of care
• Ensuring consensus across the network of the
standards expected of all
services and staff will put
in place:
§ a clear set of speciality standards
that are comparable with best
published international evidence
§ improved clinical outcomes for
patients eg reduced post surgical infections.
§ Networked care allows staff to see the right volume of patients to
develop and maintain
expertise, resulting in:
§ critical mass of clinical skill across
network deployed to ensure standards are met
§ clinical skills developed to meet
future requirements for best
outcomes.
• Increasing access to care locally for patients results
in:
§ reduced travel time
§ increased patient satisfaction.
• Improving access to subspecialty expertise for
patients will mean:
§ tertiary expertise is available closer
to patients’ homes.
§ reduced inter-specialty referrals
and waiting times.
• Consensus across the network of the patient
experience standards
expected will put in place
§ clear set of patient experience
standards based on best practice across the network.
§ standards built into staff
behaviours.
• Providing standardised safety reporting which is
bespoke to single clinical
specialty will enable:
§ robust processes in place for identifying incidents and near
misses.
§ benchmarked reporting across
network eg infection rates.
§ active “worry list” of issues receiving
attention.
• Networked care allows sites
to access greater depth and breadth of speciality
experience, enabling:
§ Thorough, standardised approach to
investigating safety issue.
§ Investigations completed more
quickly and effectively.
§ A greater number of relevant safety
and safety issues identified and addressed.
• Implementing a networked model of care
with effective clinical
governance will result in:
§ reduced variation in service delivery.
§ reduced corporate overhead
costs.
§ economies of scale.
§ avoiding future cost of failure/unsustainable services.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 12
Section 4: Our programme
Programme activities Our programme is based upon seven related activities to create the outputs listed on page 9.
Activity Description
1 Understanding
existing models
We will describe and define the different models of networked care within the Moorfield’s satellite model and those
that are used elsewhere across the NHS other sectors.
2 Assess existing
models
We will assess and review the existing Moorfield’s models of networked care in terms of clinical quality and
operational effectiveness and in relation to other aspects of the service including accessibility, patient experience, staff
wellbeing, organisational culture and activity levels.
3 Undertake
stakeholder review
We will engage with key stakeholders, including patients, staff, provider partners and commissioners in order to
assess the quality and reputation of the existing models of networked care in Moorfields and elsewhere.
4 Review lessons
from other sectors
and oversees
We will build on the research undertaken as part of the Dalton review, researching and/or visiting examples of
successful networks in other sectors and from healthcare in other countries.
5 Network analyses We will consider the themes arising from our review and identify the conditions under which networked care works
well and when it doesn’t. We will work with new systems in different parts of the country to explore how Moorfields
could support the planning and delivery of networked care.
6 Detailed market
analysis
We will map activity levels and patient flow at a provider and commissioner level across the Moorfield’s satellite model
and compare the output with local population needs assessments.
7 Review networked
care opportunities
We will test the feasibility and implications of stretch – in terms of geography and number of sites - for a networked
care model.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 13
Programme timeline and key milestones

ACC Vanguard: Moorfields Eye Hospital Value Proposition 14
Programme management and governance
As illustrated in the programme timeline on page 14, the research phase of the programme runs from January-September 2016, with three key
milestones: a review of recent Moorfields’ satellite mobilisations (by April 2016) and research into national and international models and an in-depth
review of the current Moorfields satellite model (by September 2016). To deliver this research phase, three workstreams have been established:
Workstream 1: Moorfields’ satellite mobilisation review: reviewing four recent satellite mobilisations and a specialist service transfer into
Moorfields to identify lessons learned and to create a satellite mobilisation template for the toolkit and to share with other NHS organisations
Workstream 2: Moorfields network review: assessing the existing Moorfields models of networked care, including a series of
comprehensive site visits and overseeing the development of the market assessment
Workstream 3: National and international network review: Exploring the experience of other acute networks in the NHS, to triangulate and
build our understanding of how effective networked care is delivered. Reviewing the international evidence and experience of multi-site
organisations in health and other sectors.
The figure opposite summarises the governance arrangements that are in place to
manage the programme. A vanguard programme board has been established to take
overall responsibility for the delivery of the Moorfields vanguard programme. The
programme board is chaired by the director of strategy and business development, who is
the executive sponsor and is accountable to the trust board for the delivery of the
programme. Other members of the programme board include:
programme director – a full-time position reporting to the director of strategy and
business development, who takes day-to-day responsibility for the programme
clinical sponsor – seconded part time to the programme to provide advice and
leadership to clinical workstreams and engagement
engagement & communications lead
patient representation – from the trust membership council, ensuring patient interests are considered throughout the research and delivery
phase
the national team new care models programme lead will have a standing invitation to attend any board meeting.
Qualified clinical, nursing, allied professional and admin staff will be employed on a fixed-term basis or seconded to the programme as and when
required to meet the activities needed to produce the outputs.
Trust management board
Programme board Executive sponsor
Programme director
Clinical sponsor
Patient representative
Engagement and communications lead
Vanguard programme
director
Moorfields satellite
model review
National and international
network review
Moorfields satellite
mobilisation review
National vanguard
team - NHSE
Workstream lead Workstream lead Workstream lead
Trust board

ACC Vanguard: Moorfields Eye Hospital Value Proposition 15
Empowering patients and communities
The premise that patients and communities benefit from networked care is central to our vanguard programme. We will test whether and how
patients can benefit from improved access, improved outcomes and greater confidence in the reputation of their network provider. We will analyse
how networked services can respond to the needs of the local population while providing consistently high quality care and good customer service.
We will capture this in our publication, codifying best practice in the toolkit. Patients will have representation on our programme board to help
ensure their interests are considered throughout the research and delivery phases
We are developing an engagement and communication strategy which will include a sub-workstream to provide expert and dedicated time to
leading this part of our vanguard programme. This sub-workstream will undertake engagement with key stakeholders including patients, staff,
provider partners and commissioners in order to assess the quality and reputation of the existing Moorfields satellite model and elsewhere.
The national and international network review workstream will research the evidence and capture best practice in empowering patients and
communities and delivering benefits in other NHS networks, international health networks and other sectors.
Programme evaluation and replication
Our programme is focused on building the evidence for when and how networked care can support sustaining local services in addition to
developing a toolkit that supports its effective replication. Our evaluation programme will be based on gathering the evidence described in our
value hypothesis tree and evaluating the programme outcomes described in our programme logic model and workstream logic models.
Although at an early stage, we have identified a number of hypotheses that our evaluation programme will test:
networked care delivers better clinical outcomes
networked care is safer
networked care improves access for patients
patient experience is improved by networked care
best practice and service improvement are better disseminated through networked care
this programme can improve and accelerate acute trusts’ decisions to and implementation of networked care
networked care reduces variation and generates financial savings
networked care avoids service failure (unable to maintain the service) and generates financial savings
We will continue to work with the national evaluation team in light of the recently issued guidance to ensure the outputs of our vanguard can be
used both locally and nationally. We will also seek to appoint an evaluation partner who will ensure our evaluation findings contribute to the
national vanguard programme goals.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 16
Section 5: Financial impact and costs
Hypothesis We anticipate that our vanguard programme will deliver benefits to the wider health system which can be described and quantified in two distinct
categories.
1. Benefits realised from the outputs of our vanguard
These benefits will be realised as a direct result of the outputs of our programme and will enable other organisations to make well-informed
and timely decisions about the appropriateness of implementing their own networked models of care. The toolkit will help organisations to
design and implement a network model more quickly and/or to assess and decide whether to join one. These benefits are available for all
specialities that can be networked in the 142 general acute trusts and 12 specialist trusts.
2. Benefits to be realised from implementing a networked model of care
These are the quality and financial benefits that can be realised when care is delivered through an effective NHS network.
The value generation hypothesis tree (page 12) and assessment (appendix 2) have distinguished between these two types of benefit. The
following pages provide more detail on each of these.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 17
1. Benefits to be realised from the outputs of our vanguard programme
The outputs of our vanguard programme, including the toolkit that will codify best practice in establishing networked care and critical success
factors, will enable other organisations to make well-informed and timely decisions about the appropriateness of implementing networked models
of care. The toolkit will also help organisations to design and implement a network model more quickly and effectively. The table below
summarises the benefits we expect other organisations will realise as a direct result of using the outputs of our vanguard programme.
Benefit Hypothesis Benefit savings (£)
Reduced time
required to
research and
develop
networked care
proposals
Other organisations will have access to a comprehensive summary of existing models of networked
care, both in the NHS and commercial sector, which will reduce the time they need to spend
researching this approach to partnership working. Providing a clear set of critical success factors that
need to be in place across a network in order for it to succeed will mean organisations understand the
things they need to put in place in order set up a sustainable network model. This will reduce the time
required to develop a proposal for a new network arrangement and will reduce the risk of failure.
Assuming the annual cost of developing a networked care strategy and proposal is £500k, the time
taken can be reduced by three to six months. No attempt has been made at this stage to quantify the
benefit of reducing the risk of failure.
Up to £250k saving
for each trust using
the outputs locally.
If five trusts use the
toolkit each year for
the next five years
c. £6.25m saving for
NHS.
If 10 trusts use the
toolkit each year for
the next five years
c. £12.5m saving
for NHS.
Better informed
decision-making
Other organisations will better understand the things they need to put in place in order set up a
sustainable network model. Sharing the critical success factors that need to be in place across a
network, delivering a publication outlining how the networked model can be extended and analysis of
how networked care is responsive to the needs of a local population will aid timely decision-making
No attempt has been
made at this stage to
quantify this benefit

ACC Vanguard: Moorfields Eye Hospital Value Proposition 18
and reduce the risk of failure.
More effective
design and
implementation of
a networked care
proposal
Organisations will have access to a comprehensive toolkit which will offer a detailed ‘how to’ guide,
with appropriate document templates, to enable easy implementation of a networked model. This will
accelerate replication of networked care models, will make more efficient use of resources and will
avoid the need to endlessly ‘reinvent the wheel’. The benefits of the toolkit will include improved:
financial assurance: a structured planning and mobilisation guide for setting up a network
which clearly identifies likely implementation costs and likely areas for delivering economies of
scale
legal and regulatory assurance: a clear guide to the various consultations and notifications
required when implementing a network
risk assurance: a detailed list of potential risks which will need to be managed and mitigated
during mobilisation
quality assurance: a summary of ‘what good looks like’ in relation to patient engagement,
clinical due diligence and quality metrics during implementation
board assurance: a comprehensive process developed by an acknowledged leader in the field
of network models of care through local, national and international collaboration and research
to guide organisations through the implementation phase
Assuming the annual cost of a programme to deliver a networked care model is £300k, the time taken
can be reduced by three to six months
Up to £150k saving
for each trust using
the outputs locally.
If five trusts use the
toolkit each year for
the next five years
c. £3.75m saving
for NHS.
If 10 trusts use the
toolkit each year for
the next five years
c. £7.5m saving for
NHS.
There are 154 NHS trusts that could benefit from using our outputs in multiple specialities – an assumption that they will be used 10
times a year for the next five years could generate £20m savings in the cost and time taken to lead organisations and deliver sustainable
improvement.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 19
2. Benefits to be realised from implementing a networked model of care
As part of our vanguard programme we will also seek to describe and quantify the clinical and financial benefits of implementing a networked
model of care. These benefits will apply to individual providers, local health economies and the wider NHS. The table below summarises the
benefits we have identified in our hypothesis, along with existing examples provided by other organisations, which support our current thinking. All
these benefits will be described and quantified more fully as an integral part of our vanguard programme.
Benefit Hypothesis Existing examples
Reduced variation Establishing networked models of care will reduce the variation
in the quality of care delivered by different providers. This is
particularly applicable in smaller clinical specialties which are
rarely a high strategic or operational priority in district general
hospitals.
The reduced variation will result in better clinical outcomes and
improved patient experience. There will also be more
equitable patient access (localised and timely) to sub-specialist
expertise.
The cost of variability in orthopaedic outcomes as detailed
in National Orthopaedic Alliance value proposition:
The improved outcomes in stroke care resulting from the
reorganisation of stroke pathways in London cited in BMJ
2013;347:f4954
Evidence that poor care is expensive (eg £4K for HCAI
(NPSA); £10.5k for grade 4 pressure ulcer and £2.5k for
grade 4 fall (Health Foundation).
Evidence from claims and litigations – mean cost of
ophthalmology claim is £32K (Moorfields research).
Reduced corporate
overhead costs
By sharing executive and operational leadership across a
network, there will be an overall reduction in overhead costs
across the system. This will also apply to corporate functions,
including governance teams.
These costs will be estimated through the vanguard
programme
Economies of
scale
Creating a network will result in better utilisation of specialist
workforce (in particular clinical staff) and equipment across the
health system.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 20
Avoid future cost
of failure/
unsustainable
services
Where clinical services in their current configuration are
clinically and/or financially unsustainable, a networked model
may provide a solution that enables the continued provision of
those services locally and avoids the cost and impact of the
failure of those services.
Case study 1: Surgicentre, a privately-run NHS elective
surgical centre at Lister Hospital. The service was closed
after the CQC found the unit failed four out of five
standards. There had been three unexplained deaths
following low-risk orthopaedic surgery. Referrals for
ophthalmology and joint surgery were stopped and a local
service lost. The Department of Health had to pay £53m
to transfer the service to an NHS provider, plus £3.7million
redundancy costs, £3m contractual financial fees and
underwriting a £1m deficit.
Case study 2: Ophthalmology service at Croydon
University Hospital. There were multiple clinical and
operational challenges facing the service. Only two
consultants were employed for a service requiring five;
trainee doctors were removed because of inadequate
support; subspecialties were provided by people without
the required training and the workforce was demoralised
with poor teamwork. The service was transferred to
Moorfields, becoming a new satellite. This resolved the
staffing issues and the satellite now has a programme of
service development and improvement including a network
of community outpatient clinics for communities around
Croydon.
There is evidence that networked care can have a considerable positive impact on the cost of care, its quality and the experience of
patients but more needs to be done to quantify it and understand how it can be delivered and replicated. Our programme aims to build
this knowledge for the NHS and turn it into practical advice that can be used by all trusts to avoid local services failing, improve quality
and cost of care and improve patient experience.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 21
Moorfields’ contribution to the national vanguard programme
In addition to the resources identified in our value proposition submission of 30 November 2015, Moorfields Eye Hospital NHS Foundation Trust is
making additional contributions to the national vanguard programme for which we are seeking no financial recompense. These are summarised in
the table below.
Description of contribution 2016/17
Contribution
Time devoted to the national programme:
Executive team time invested to support the vanguard programme
Attendance at national and local vanguard programme meetings
Organisational input and expert advice
£41k
£24k
£32k
Subtotal £97k
Value of historical knowledge and expertise
As its network has grown and developed, Moorfields has gained
experience and expertise that generates the value and benefits
described in this value proposition. The financial value of this could
be described as the saving we expect to generate each time our
toolkit is used (£400k) multiplied by the 32 sites in our network so far.
This is the value that we are offering to share with the NHS and turn
into practical application.
£12.8m
TOTAL £12.9m

ACC Vanguard: Moorfields Eye Hospital Value Proposition 22
Financial resources required in 2016/17 The table below summarises the resources required in 2016/17 to deliver the programme.
Activity 2015/16
funding
allocated
Programme management and production of outputs* £651k
1. Understand existing models £43k
2. Assess existing models £745k
3. Undertake stakeholder review £53k
4. Review international networks £48k
5. Network analyses £218k
6. Detailed market analysis -
7. Review networked care opportunities £201k
TOTAL £1.959m
*includes the costs of developing and maintaining the toolkit online to make it easily accessible across the NHS.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 23
Section 6: Non-financial support package
The table below summarises the support we are seeking from the new care models programme and national organisations
Support package element Initial view of the support in 2016/17
Designing new models of care Care Quality Commission (CQC): help to establish whether a community thinks that a change to their
service would be an improvement, making sure a networked care model is what the local community wants
and needs
NHS England: sustainable improvement team
support to capture of knowledge to aid learning and the spread and replication of our care model
network toolkit and other resources to help network leaders and users manage their networks effectively
National voices:
building understanding of what matters to patients, service users and carers
building understanding of the evidence for what works to engage people in their care and support
building understanding of what works in engaging citizens and community organisations, in
governance, service design, and implementation.
Evaluation and metrics New Care Model (NCM): support for development of the local evaluation strategy and appointment of a
suitable evaluation partner.
Integrated commissioning and
provision
NCM: understanding what models are being developed and their potential impact/learning for the network
toolkit. Support us to consider how the network toolkit can be replicated across other programmes and
adapted for wider use.
New operating model Working with our collaborative partners, the National Orthopaedic Alliance and the Walton Centre
NCM, to help assess other new models which may have implications for the proposed network care model –

ACC Vanguard: Moorfields Eye Hospital Value Proposition 24
best practice, lessons learned, what can be shared.
Governance, accountability
and provider regulation
NCM: help us assess the implications for network for different types of network arrangement with different
geographical spread.
Empowering patients and
communities
Health Education England (HEE): factoring into our research and the toolkit, the principles and key success
factors for delivering long-lasting behaviour change across staff, patients and the wider public, with a
particular focus on supporting self-care and wider person-centered care.
Harnessing technology NCM:
access to published examples of what good looks like for digital success
nationally agreed standard templates for information governance
available technical and strategic support for connected digital solutions and information handling in
different clinical scenarios
Workforce redesign HEE and working with workforce redesign specialists locally.
Local leadership and delivery Currently reviewing and will confirm.
Communication and
engagement
NICE consultancy support: using QS15: Patient experience in adult NHS services to drive patient
engagement.
NCM: examples of good external stakeholder engagement processes including patient engagement.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 25
Section 7: Summary and conclusion
Moorfields is the leading provider of eye health services in the UK and a world-class centre of excellence for ophthalmic research and education.
Our main focus is the treatment and care of NHS patients with a wide range of eye problems, from common complaints to rare conditions that
require treatment not available elsewhere in the UK. We treat people from 32 core locations in and around London, which enables us to provide
expert treatment closer to patients’ homes.
Acute hospitals are facing increasing challenges to deliver safe and cost effective care, especially in smaller clinical specialties such as
ophthalmology which often lack the benefits of scale in a local setting. In the absence of critical mass of patient numbers or specialty workforce,
provision of care may become clinically or financially unsustainable. Moorfields has developed a satellite model that provides clinically and
financially sustainable local access to high quality ophthalmic care, and a sustainable model of specialist treatment. We believe that the
Moorfields’ satellite model has potential replicability across the acute healthcare system. The aim of our vanguard is to consolidate our learning in
delivering networked care so that we, and the wider NHS, can develop a clear understanding of when and how this new model of care can enable
acute hospitals to become clinically and financially sustainable.
We want to consolidate our learning in delivering networked care so that:
the NHS can develop a clear understanding of when and how this new model of care can support acute hospitals in becoming clinically and
financially sustainable and the implications of extending models of networked care more widely across the service
we, at Moorfields, can deliver sustainable ophthalmology services that meet the needs of local populations and are delivered as an effective networked care model.
Our programme will deliver two key outputs, which will deliver benefits for the wider NHS, and for Moorfields:
a toolkit that codifies best practice in establishing the need for and implementing networked care and describes the critical success factors
required for it to succeed.
a publication outlining how the models of networked care can be extended while delivering clinically and financially sustainable services that
meets the needs of local populations.
This value proposition requests funding of £1.959m to support the delivery of the programme in 2016/7. Moorfields is committed to
contributing its time, experience, expertise and knowledge to the national vanguard programme, at a value of £12.89m. The quantifiable
financial benefits of 10 trusts a year using the outputs from our programme locally to make decisions about implementing networked
care could save £20m over five years. Our programme will build the evidence and understanding of the further value and benefits of
networked care to quality, experience and cost and turn it into practical advice on how to realise and replicate it.kare

ACC Vanguard: Moorfields Eye Hospital Value Proposition 26
Appendix 1: Three workstream logic models (1/3)
Activities Outputs Outcomes
Rationale
To carry out an internal review of our most recent satellite mobilisations in order to analyse the generic themes and critical success factors which underpin the way in which we manage the
mobilisations in current form. To use this information to develop a Toolkit which other organisations can use to set up a network model of care (replicate this model elsewhere within the NHS)
Impacts
Accelerated
establishment of
satellite networks
across the NHS
Reduction in start-
up costs to
establish a satellite
network
More efficient use
of resources
through
establishing
satellite networks
Networked care will be
supported by effective and
sustainable governance
structures, underpinned by a
strong organisational culture
Patients will have greater access
to locally delivered, clinically
sustainable services
Acute hospitals will become
more sustainable by working
with partners in a network
Moorfields ACC vanguard: Moorfields satellite model mobilisation review 1/3
Document showing differences
between the planned and delivered
service created by April 2016.
Compare current service configuration against the agreed business case signed off by TMB.
Elements included, but not limited to:
• clinic timetable
• staffing per session • appointment profile per session
• activity achieved per session
• capital equipment
• rooms occupied per session
Revised and improved satellite
mobilisation checklist/plan created by
April 2016
Conduct survey with staff that have experienced the mobilisation. Elements included:
• Did they feel involved?
• Able to raise concerns?
• Were concerns dealt with? • Were they communicated during the process?
• Was the information provided helpful and
informative?
• Lessons learned and best practices
Anonymised mobilisation staff feedback
document created by April 2016
Mobilisation lessons learned and best
practices document created by April
2016
Develop business case template for setting up a satellite site linked to the revised checklist/
mobilisation plan
Notional Business case template
document created by April 2016
Review and compare mobilisation plans
Revise and update the mobilisation template to
provide a detailed and complete project plan
which represents what ‘looks good’ for effective
mobilisation planning for a new service onto an
existing site or a new satellite site entirely
Review and compare mobilisation plans against
the draft satellite checklist
Replicability of best
practice in
delivering
networked care
Better decision
making for
organisations
considering a
networked care
model

ACC Vanguard: Moorfields Eye Hospital Value Proposition 27
Appendix 1: Three workstream logic models (2/3)
Activities Outputs Outcomes
Impacts
Accelerated establishment of
satellite
networks across
the NHS
Better care for patients
delivered by
standardizing
care, improving accessibility and
minimizing
waste across
the system
Reduction in start-up costs to
establish a satellite
network
Better decision making for
organisations
considering a
networked care model
Replicability of best practice in
delivering
networked care
Delivery of sustainable
ophthalmology
services that
meet the needs of local
populations and
are delivered in
an effective
network
Networked care will be supported by effective and sustainable governance
structures, underpinned by a strong
organisational culture
Patients will have greater access to locally delivered, clinically sustainable services
Acute hospitals will become more sustainable by working with partners in a
network
Rationale To carry out a deep dive internal review of our existing satellite model in order to analyse the generic themes and critical success factors which underpin the way in which our network operates
successfully in its current form. To use this information to develop a Toolkit which other organisations can use to set up a network model of care (replicate this model elsewhere within the NHS)
Moorfields ACC vanguard: Moorfields internal satellite model review logic model 2/3
Conduct full review of Moorfields eye centre@Moorfields eye unit@, and
Moorfields community eye clinic@
Conduct desktop review of smaller Moorfields eye clinic@
Estimate onward referral value to Moorfields partnership@
Review savings of Moorfields shared care cataract pathway
Satellite premises review
Satellite patient profile review
Satellite, sub-specialty and clinic activity review
Satellite, sub speciality & clinic clinical governance review
Satellite competitor analysis
Satellite, sub specialty & clinic workforce review
Satellite, sub specialty & clinic financial stability review
Conduct stakeholder review
NHS Toolkit, including critical success factors, opportunity analysis, comms plan, demand
based service schedule, service and network
checklist, clinical governance framework,
policies reporting and monitoring, outcomes benchmark, mobilization plan, costing template
and business case template completed by
March 2017
Conduct comparative eye network review
Review satellite IT connectivity and interoperability
Review patient care impact of Croydon take-over.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 28
Appendix 1: Three workstream logic models (3/3)
Activities Outputs Outcomes
Rationale
The aim of our national and international workstream is to consolidate and share our learning in delivering networked care, in collaboration with other NHS and commercial providers, so that
the NHS can develop a clear understanding of when and how this new model of care can support DGHs and health economies to be clinically and financially sustainable for small
specialties like ophthalmology.
Impacts
Better decision making for organisations
considering a networked care model
Replicability of best practice in delivering networked care
Widespread understanding of the benefits arising from different forms of networked care
Networked care will be supported by effective and sustainable governance structures, underpinned
by a strong organisational culture
Patients will have greater access to locally delivered, clinically sustainable services
Acute hospitals will become more sustainable by working with partners in a network
Better understanding of the commissioning implications arising from widespread adoption of
networked care
Moorfields ACC vanguard: national & international network review logic model 3/3
Conduct market analysis: • review overall market position based
on hospital activity data
Report on activity levels and patient flows at provider and CCG Level produced by April 2016
.
Populated template/tool which enables the trust to review its overall position in the market produced
by April 2016
Report on activity and market share trends providing intelligence on opportunities and risks in
the market, and a standard way of assessing the
market on a regular and ongoing basis produced
by May 2016 (To include detail on patient flows for the top eye treatments in London as a whole and
in SE England. (Using HES data)
Market analysis template produced by June 2016.
Research and identify lessons from other networks in the NHS and internationally
Template with set of consistent research questions/ key lines of enquiry that will be
used for all of the network reviews produced by
March 2016.
.
Desktop review and/or physical visits to 16-25 sites.
Site reports produced by August 2016. .
Review research and evidence on national and International networks to understand
applicability for our programme publication
and toolkit.
Key elements : • understand the structure of the service
provided – single site, multiple,
network, other
• market context (catchment/
competitors/partners)
• understand the challenges the Trust faces – commissioners and financial
• clinical governance structure in
codifying & spreading good practice
across the network
• identify similarities with Moorfields ophthalmic or generic themes
• identify opportunities for sharing
learning and innovation
• explore commissioning models
National and International network analysis review produced by end of September, 2016..
NHS publication produced by March 2017.

ACC Vanguard: Moorfields Eye Hospital Value Proposition 29
Appendix 2: Value generation assessment (1/5) - Clinical Primary
assertion Sub-assertion Evidence available Further evidence to
be gathered Metrics Target
Cli
nic
al
Clinical outcomes will
be improved
through
replicating best clinical practice
across a
network.
• Providing a clear, systemised approach to
spreading best clinical
practice across other sites
will allow:
§ systems to understand and replicate best clinical practice.
• Large investment in clinical governance half-days as a
protected forum for sharing
lessons and best practice.
• Research trial activity.
• Sub-speciality service improvement plans
• Review effectiveness of existing clinical
governance structure
in codifying and
spreading good practice across the
satellite model
• Review how other networks share and
adopt best practice.
• Variation in clinical practice
across the
satellite model
reviewing performance
against 30
core quality
standards.
• Identify and describe how
networked care
can improve the
adoption of best practice.
• Ensuring consensus across the network of the standards expected of all
services and staff will put in
place:
• a clear set of specialty standards
that are comparable with the best
published international evidence.
• improved clinical outcomes for patients eg reduced harm such as post surgical infection.
• Clinical outcomes measured against 30 core outcomes for best ophthalmology practice.
• Clinical effectiveness
supported by a
comprehensive list of policies, guidelines and protocols for
best ophthalmology practice.
• 200+ audits to review clinical
practice for effectiveness and
outcomes.
• Update 30 clinical outcome standards to ensure they
continue to represent
best international practice.
• Review how other networks set and
review standards for
clinical outcomes.
• Clinical outcome standards
across the
satellites - reviewing
performance
against 30
core quality
standards.
• Specify expectation with relation to
setting clear
clinical outcome standards
across a
network.
• Networked care allows staff to see the right volume of
patients to develop and
maintain expertise,
resulting in:
• critical mass of clinical skills within the network are deployed to
ensure standards are met.
• clinical skills developed to meet future requirements for best outcomes.
• summary of the secondary and tertiary clinics across the
satellite model and the clinical
expertise providing them.
• Determining right volume mix at local
level.
• Review how other networks deploy staff
to maintain and
improve access.
• Measures of casemix and
complexity.
• Vanguard output will provide gap
analyses of
network v non –
network benefits and approach to
deploying clinical
specialists across
a network.
)
A
Impact
of outp
uts
of
vanguard
pro
gra
mm
e
Impact
of im
ple
menting a
netw
ork
ed m
odel of
care
ACC Vanguard: Moorfields Eye Hospital Value Proposition 30
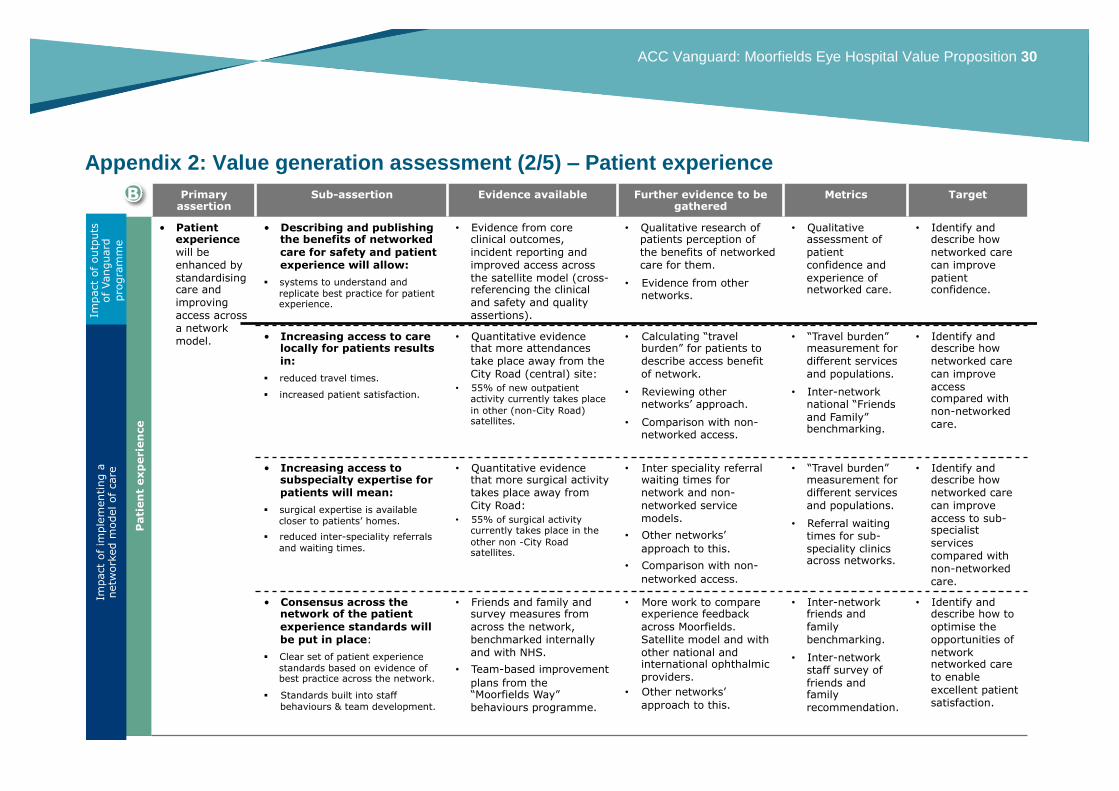
Appendix 2: Value generation assessment (2/5) – Patient experience
Primary assertion
Sub-assertion Evidence available Further evidence to be gathered
Metrics Target
Pati
en
t exp
erie
nce
• Patient experience
will be
enhanced by
standardising care and
improving
access across
a network
model.
• Describing and publishing the benefits of networked
care for safety and patient
experience will allow:
§ systems to understand and replicate best practice for patient experience.
• Evidence from core clinical outcomes,
incident reporting and
improved access across
the satellite model (cross-referencing the clinical
and safety and quality
assertions).
• Qualitative research of patients perception of
the benefits of networked
care for them.
• Evidence from other networks.
• Qualitative assessment of
patient
confidence and
experience of networked care.
• Identify and describe how
networked care
can improve
patient confidence.
• Increasing access to care locally for patients results
in:
§ reduced travel times.
§ increased patient satisfaction.
• Quantitative evidence that more attendances
take place away from the
City Road (central) site:
• 55% of new outpatient activity currently takes place
in other (non-City Road) satellites.
• Calculating “travel burden” for patients to
describe access benefit
of network.
• Reviewing other networks’ approach.
• Comparison with non-networked access.
• “Travel burden” measurement for
different services
and populations.
• Inter-network national “Friends
and Family” benchmarking.
• Identify and describe how
networked care
can improve
access compared with
non-networked
care.
• Increasing access to subspecialty expertise for
patients will mean:
§ surgical expertise is available
closer to patients’ homes.
§ reduced inter-speciality referrals
and waiting times.
• Quantitative evidence that more surgical activity
takes place away from
City Road:
• 55% of surgical activity currently takes place in the
other non -City Road satellites.
• Inter speciality referral waiting times for
network and non-
networked service
models.
• Other networks’
approach to this.
• Comparison with non-
networked access.
• “Travel burden” measurement for
different services
and populations.
• Referral waiting times for sub-
speciality clinics across networks.
• Identify and describe how
networked care
can improve
access to sub-specialist
services
compared with
non-networked
care.
• Consensus across the network of the patient
experience standards will
be put in place:
§ Clear set of patient experience standards based on evidence of best practice across the network.
§ Standards built into staff
behaviours & team development.
• Friends and family and survey measures from
across the network,
benchmarked internally
and with NHS.
• Team-based improvement
plans from the “Moorfields Way”
behaviours programme.
• More work to compare experience feedback
across Moorfields.
Satellite model and with
other national and international ophthalmic
providers.
• Other networks’
approach to this.
• Inter-network friends and
family
benchmarking.
• Inter-network staff survey of
friends and family
recommendation.
• Identify and describe how to
optimise the
opportunities of
network networked care
to enable
excellent patient
satisfaction.
Impact
of outp
uts
of Vanguard
pro
gra
mm
e
B
Impact
of im
ple
menting a
netw
ork
ed m
odel of care

ACC Vanguard: Moorfields Eye Hospital Value Proposition 31
Appendix 2: Value generation assessment (3/5) – Safety and quality Primary
assertion Sub-assertion Evidence available Further evidence to be
gathered Metrics Target
Safe
ty a
nd
qu
ality
• Safety and quality will
be assured
through
setting and spreading
best practice
across the
network.
• Disseminating lessons on safety and quality learnt
across the network will
ensure:
• wider reach an application of speciality specific lessons, resulting in faster adoption of any
changes to practice.
• Aggregate and themed analysis comparing all
incidents, complaints and
claims across whole
network.
• Local quality forums held
across the network designed to review quality,
supported by dedicated role
of network quality partners.
• Themes arising from other organisations
(ophthalmology and
other).
• What learning is shared.
• Evidence that lessons learnt reach all satellite
sites.
• Evidence from other networks.
• Incident reporting
outputs.
• Staff survey measures of
safety
processes and lessons
learned.
• Analyses as to whether a
network offers a
better learning
opportunity
• Analyses as to
whether learning leads
to long-term
action/change
• Providing standardised safety reporting which is
bespoke to a single clinical
specialty will enable:
• robust processes for identifying safety incidents and near misses
• benchmarked reporting across
the network, eg infection rates
• an active “worry list” of the top
quality and safety issues receiving attention in the
network.
• In 2014/15 there were 6,575 reported safety
incidents across the
network.
• Approximately half of these incidents occurred at City
Road and the rest across
the other satellites.
• Infections following
cataracts and intravitreal
injections are monitored for all sites.
• Undertake comparison of quality and safety
assurance with a “good”
CQC-rated DGH to further
assess and understand the benefits of a single
speciality network.
• Evidence from other networks.
• Safety incident reporting.
• Infection rates following
cataract
surgery and
intravitreal surgery.
• Analyses as to whether
network model
improves
quality and safety
reporting.
Where there is
evidence that it
does – how is
this best achieved?
• Networked care allows all sites to access greater
depth and breadth of
speciality experience
enabling:
• thorough standardised approach to investigating safety issues
• investigations completed more
quickly and effectively.
• a greater number of quality and safety issues relevant to sites.
• The quality and safety assurance model sets out
the incident investigating
and reporting system for
the network.
• The regular global quality
and safety report details the
themes and lessons for the
network.
• Individual investigation
reports detail the findings
and lessons.
• Undertake comparison of quality and safety
assurance with a “good”
CQC rated DGH to further
assess and understand the benefits of a single
speciality network.
• Measure timeliness of completion of
investigations across the network.
• Evidence from other networks.
• Adherence to standard
safety
investigation
guidelines and timescales
• Analyse differences
across different
organisations
(single specialty in DGH/single
specialty
network/multi
specialty DGH /
multi - network
C
Impact
of outp
uts
of
vanguard
pro
gra
mm
e
Impact
of im
ple
menting a
netw
ork
ed m
odel of
care

ACC Vanguard: Moorfields Eye Hospital Value Proposition 32
Appendix 2: Value generation assessment (4/5) - Resource requirements
Primary assertion Sub-assertion Evidence available Further
evidence to be
gathered
Metrics Target
Resou
rce r
eq
uir
em
en
ts
• Resource requirement of
additional ~
£1.959m in
16/17 is reasonable to
deliver the
outputs and
generate the
value of the
programme
• £1.959m is the cost of delivering the
programme activities: • Programme management
£651k
• Existing models £43k
• Assess existing models
£745k
• Stakeholder review £53k
• International review £48k
• Network analysis £218k
• Network opportunities £201k
• £12.9m is the value of the knowledge,
experience, expertise
and time being contributed to the
national vanguard
programme.
• Detailed costing undertaken of all of the activities required to deliver the
outputs for year 1 of the vanguard
by March 2017
• Programme management include the costs of developing and maintaining
the toolkit as an on-line tool that is easily accessible across the NHS
• As its network has grown and developed, Moorfields has gained
experience and expertise that generates the value and benefits
described in this value proposition.
The financial value of this could be
described as the saving we expect to
generate each time our toolkit is used (£400k) multiplied by the 32
sites in our network so far. This is
the value that we are offering to
share with the NHS and turn into
practical application.
Achieve milestones and
deliver
outputs.
D

ACC Vanguard: Moorfields Eye Hospital Value Proposition 33
Appendix 2: Value generation assessment (5/5) - Sustainability
Primary assertion
Sub-assertion Evidence available Further evidence to be gathered
Metrics Target
Su
sta
inab
ilit
y
Sustainability for the NHS will be
improved by
supporting NHS
organisations to evaluate,
implement and
deliver the
benefits of
networked care
faster.
• Providing a clear set of critical success factors
for networked care and
a comprehensive ‘how
to’ guide toolkit will result in:
• reduced time for trusts to appraise options for
forming or joining networks
of care
• more effective design and implementation of a
networked care proposal.
• Anecdotal evidence that it can take a year or more for trusts
to appraise network options
and make a strategic decision
to proceed. Trust boards can be concerned about whether
they have sufficient
information to proceed and
implement a new network.
• Anecdotal evidence that implementation of networks
can take a year or longer to implement.
• Whether there is empirical evidence of
the time it takes
trusts to decide to
network and the subsequent success
rate in implementing
networked care.
• Whether there is empirical evidence of
how long it takes to
implement new networks.
N/A • >£400K per organisation and per speciality saving
based on reduced decision
taking time and reduced
time to design and implement.
• 154 trusts have potential to
use outputs for multiple
specialties.
• 5 trusts a year over 5 years
saves> £10m.
• 10 trusts a year over 5
years saves > £20m.
• Implementing a networked model of
care with effective
clinical governance will
result in:
• reduced variation in service
delivery
• reduced corporate
overhead costs
• economies of scale
• avoiding future cost of
failure and/or unsustainable services.
• There is evidence that poor care is expensive:
• A hospital acquired infection adds
£4,000 to cost of care (NPSA).
• A grade 4 pressure ulcer costs
£10,500 and a grade 4 fall £2,500 (Health Foundation).
• Average litigation cost at
Moorfields is £32k.
• Case study of service failure at
Lister hospital cost DH £7.7m.
• Case study Croydon
ophthalmology services taken over by Moorfields, resolved
staffing crisis and improved care
and access.
• Examples and evidence of the link
between networked
care and quality and
cost.
• Gather further
evidence of risks of sustainability in small
providers and whether
networked care
provides an
alternative and avoids the cost of failure.
N/A
• Savings could be considerable across the NHS
– and the programme will
seek to identify and
estimate the potential savings.
• The cost of service failure is
considerable – cost, quality,
access and experience.
• Could apply to the 30
smallest and 45 small general acute trusts
identified by Monitor.
Impact
of
outp
uts
of
vanguard
pro
gra
mm
e
Impact
of im
ple
menting a
netw
ork
ed m
odel of care


![Moorfields Eye Hospital NHS Foundation Trust | - … 5... · Web viewOf the 256 doctors the numbers of completed appraisals within the appraisal year 2013-2014 were 207 [80.9%]. This](https://cdn.vdocuments.mx/doc/165x107/5e90d39759e30262e36dcef4/moorfields-eye-hospital-nhs-foundation-trust-5-web-view-of-the-256-doctors.jpg)




