
Raltitrexed:
un vecchio farmaco con un
“cuore nuovo”
Antonio Avallone
National Cancer Institute of Naples

What is Tomudex® (Raltitrexed )
Folic Acid
•Raltitrexed, a quinazoline analogue of folic acid, is a specific and direct Thymidylate
Synthase (TS) inhibitor. Its long-lasting inhibition of TS allows for a convenient 3 -weekly
schedule of administration.
•It is approved, in many countries, for the treatment of advanced colorectal cancer where
5-FU/FA regimens are either not tolerated or inappropriate.
•Raltitrexed clinical evaluation stumbled prematurely when an excess of treatment-related
mortality was observed in colorectal cancer trals.
• Is TS still a relevant target in the colorectal cancer management in the era of the
molecular therapy ?
• How can we optimise tolerability and efficacy of raltitrexed?
• Is raltitrexed really a drug with a life-threatening toxicity?
Raltitrexed
•Recent clinical data, showing raltitrexed as a safe alternative treatment option for CRC
patients with significant cardiovascular risk factor or reporting fluoropyrimidine-induced
cardiotoxicity.

Advances in CRC Treatment
0
5
10
15
20
25
30
1980 1985 1990 1995 2002 2005
Best supportive care (BSC)
5-FU Irinotecan
Oxaliplatin
Capecitabine
Cetuximab
Panitumumab
Bevacizumab
Months
Median overall survival
5-FU
G1 S G2
M
Aflibercept
Regorafenib

The response rate of patients receiving FOLFOX (45%) was higher than for those receiving IROX (35%, P .03).

Thymidylate Synthase (TS) has a Prognostic Value in CRC
Edler D. JCO 2002; 20:1721-1728 Popat S. JCO 2004; 22:529-536
Funnel plot of hazard ratios (HR) of overall survival in all advanced disease
studies associated with a high level of thymidylate synthase expression.
Funnel plot of hazard ratios (HR) of overall survival in all adjuvant studies
associated with a high level of thymidylate synthase expression.

Thymidylate synthase as an oncogene: A novel role for an essential DNA synthesis enzyme
Lambratu Rahman, Donna Voeller,Monzur Rahman, Stan Lipkowitz, Carmen Allegra, J. Carl Barrett, Frederic J. Kaye, and Maria Zajac-Kaye
Rahman et al Cancer Cell 5; 2004: 341-351

DNA dTTP dTDP dTMP dUMP
Thymidylate-Synthase
Pyrimidine (dUMP)
binding site
Folate
binding site
Raltitrexed Raltitrexed glu2-4 FPGS RFC
RNA FUTP
DPD
5-FU FUDP
F-dUMP
F-dUDP
RR
F-dUTP
FUMP
OPRT
5-DFUR
TP
5-DFCR
CyD Capecitabine
TP
F-dURD
TK
CE
FPGS RFC
cell membrane Folinic Acid 5,10-CH2 FH4 glu2.6
cell membrane
Disadvantages 5-FU •Rapid catabolism
•Competition with dUMP
•Lack of specificity
•Inconvenience and cost of 5-FU infusion
5-F-DHU
Biochemical Mechanisms of Cap, 5-FU, RTX and FA
Advantages Raltitrexed •Specificity
•No competition with dUMP
•Prolonged inhibition of TS
•Convenience of the schedule

Raltitrexed : Phase I/Pharmacokinetics trials
Clarke SJ et al JCO 1996: 14:1495-1503; Beale P et al Cancer Chemother Pharmacol 1998,42:71-76 Grem JL et al Clin Cancer Res 1999; 5:2381-2391; Cunningham D. et al European Journal Cancer 2002;38:478-486
Creatinine clearance Dose (%) Dosing interval
>65 ml/min 100 Every 3 weeks
55-65 ml/min 75 Every 4 weeks
25-54 ml/min 50 Every 4 weeks
<25 ml/min - -
Level of Bilirubin
1.25 to 3 times the normal upper
limit 100 Every 3 weeks -
Level of transaminases
3 to 10 times the normal upper
limit 100-
Every 3 weeks Every 3
weeks 0-
RD: 3 mg/m2 every three weeks (in USA 4 mg/m2 every three weeks)
DLT: Diarrhea, neutropenia, transient and reversible increase of hepatic
transaminases, malaise (asthenia, nausea, anorexia)
Half-life: 198 hours
Excretion: essentially unchanged by the kidneys

Clinical Response and Survival from Randomized Studies of Raltitrexed vs 5FU/LFA in Advanced Colorectal Cancer Patients
Cunningham D Ann Oncol 1996; 7 :961-5; Cocconi G. JCO 1998;16 : 2943-52;Pazdur R 1997 ;16(abs 801)
Study Treatment
Number
of
patients
Response (%) Median
TTP or PFSh
(months)
Median
OS
(months)
Median
treatment
duration
(weeks) PR CR SD
3 RTXa
Mayob regimen
223
216
15.7
13
3.6
3.7
35
32.4
4.7
3.6
10.3
10.3
15.2
15
10 RTXa
Mayob regimen
217
220
11.5
13.8
2.8
1.4
33.2
40
3.1
5.3*
9.7
12.7*
12.1*
22.3
12 RTXa
Machoverc regimen
245
244
15.4
14.5
3.2
3.6
51.4
52.4
3.9
5.1*
10.9
12.3
12.7*
16.9
CR06
RTXa
de Gramontd regimen
Lokiche regimen
301
303
301
17
22
24
1
2
0.4
34
37
34
4.9h
5.8h
5.8h
8.9
9.8
10.1
12
12.8
12.1
FFCD9601
RTXa
de Gramontd regimen
Id-de Gramontf regimen
AIOg regimen
72
74
75
73
10
24
20
20
0
4
1
1
53
35
53
51
4h*
5.3h*
5.4h
4.8h
12.2
13.1
17.1
14.6
12.6*
20
19.8
17
aRTX: raltitrexed 3 mg/m2 every 3-weeks; bMayo regimen: 5-FU bolus 425 mg/m2 plus folinic acid (FA) 20 mg/m2 for 5 days, repeated every 4 weeks; cMachover regimen: 5-FU bolus 425 mg/m2 plus high dose of FA 200 mg/m2 for 5 days, repeated every 4 weeks dde Gramont regimen: FA 200 mg/m2 + 5-FU bolus 400 mg/m2 and 5-FU 600 mg/m2 in 22-hour infusion on day 1 and 2, repeated every 2 weeks; eLokich regimen: daily 5-FU 300 mg/m2 continuous infusion fId-de Gramont regimen: FA 20 mg/m2 + 5-FU bolus 400 mg/m2 and 5-FU 600 mg/m2 in 22-hour infusion on day 1 and 2, repeated every 2 weeks; gAIO regimen: weekly 5-FU 2600 mg/m2 in 24-hour infusion for 6 weeks, followed by 2-week rest every 7 weeks; hPFS;
*p < 0.05

Main Severe Toxicity from Randomized Studies of Raltitrexed vs 5FU/LFA in Advanced Colorectal Cancer Patients
Cunningham D Ann Oncol 1996; 7 :961-5; Cocconi G. JCO 1998;16 : 2943-52;Pazdur R 1997 ;16(abs 801)
aRTX: raltitrexed 3 mg/m2 every 3-weeks; bMayo regimen: 5-FU bolus 425 mg/m2 plus folinic acid (FA) 20 mg/m2 for 5 days, repeated every 4 weeks; cMachover regimen: 5-FU bolus 425 mg/m2 plus high dose of FA 200 mg/m2 for 5 days, repeated every 4 weeks dde Gramont regimen: FA 200 mg/m2 + 5-FU bolus 400 mg/m2 and 5-FU 600 mg/m2 in 22-hour infusion on day 1 and 2, repeated every 2 weeks; eLokich regimen: daily 5-FU 300 mg/m2 continuous infusion fId-de Gramont regimen: FA 20 mg/m2 + 5-FU bolus 400 mg/m2 and 5-FU 600 mg/m2 in 22-hour infusion on day 1 and 2, repeated every 2 weeks; gAIO regimen: weekly 5-FU 2600 mg/m2 in 24-hour infusion for 6 weeks, followed by 2-week rest every 7 weeks;
*p < 0.05
Toxicity
Study 3 Study 10 Study 12 Study CR06 Study FFCD9601
RTXa
(n=223)
Myb
(n=216)
RTXa
(n=199)
Myb
(n=179)
RTXa
(n=230)
Mcc
(n=222)
de Gd
(n=303)
Loke
(n=301)
RTXa
(n=301)
de Gd
(n=74)
Id-de Gf
(n=75)
AIOg
(n=73)
RTXa
(n=72)
Leucopenia 14 30* 18 41 6* 13 1.8 0.4 5.1 0 1 7 11*
Neutropenia - - - - - - 2.6 0 8* 3 4 11 14*
Stomatitis 2 22* 3 10 2 16* 0.4 4.1* 1.5 3 1 5 0
Anemia 9* 2 9 4 5 2 1.5 1.5 5.1 - - - -
Increase in
transaminases 10 0 7 1 13* 9 - - - 1 1 1 6*
Nausea/
Vomiting 13 9 13 8 9 9
2.9/
3.3
5.1/
4.4
9.5*/
7.7 5 3 8 18*
Asthenia 6 2 18 10 5 2 - - - - - - -
Anorexia - - - - - - 3.3 6.2 11* - - - -
Lethargy - - - - - - 7.6 9.5 19.4* - - - -
Diarrhea 14 14 10 13 10 19 3.3 6.3 12.4* 5 7 4 14*
Thrombocytopenia 4 1 5 3 3 0 0 0 3.3* 1 1 0 3
Study 3-10-12 Raltitrexed
684 pts
Study 3-10-12 5FU/LV 680 pts
Study CR06 Raltitrexed
301 pts
Study CR06 5FU/LV 604 pts
All treatment-related deaths (%)
26 (3.8%) 17 (2.5%) 18 (5.9%)
3 (0.5%)
Deaths in pts with no appropriate dose
reduction/protocol violation (%)
17 (2.4%) 6 (0.9%) 11 (3.6%) -
Deaths in pts treated according to the protocol
(%)
9 (1.4%) 11 (1.6%) 7 (2.3%)
3 (0.5%)
Cunningham D. et al British Journal Cancer 1998; 77 (Supp. 2):15-21
Maughan T. et al Lancet 2002;359: 1555-1563
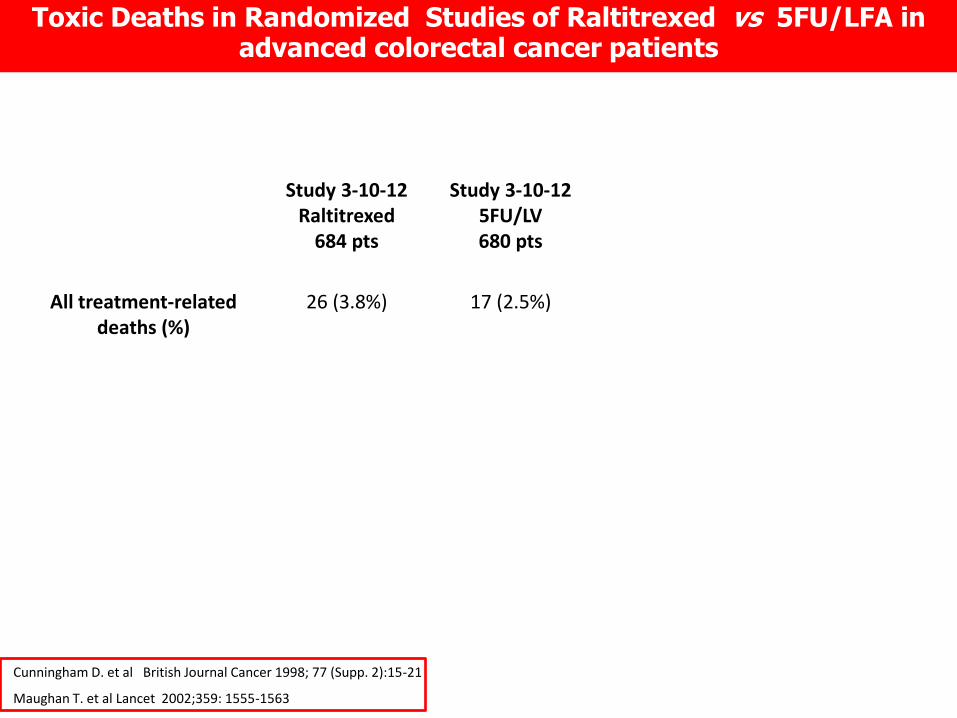
Toxic Deaths in Randomized Studies of Raltitrexed vs 5FU/LFA in advanced colorectal cancer patients

Study 3-10-12 Raltitrexed
684 pts
Study 3-10-12 5FU/LV 680 pts
Study CR06 Raltitrexed
301 pts
Study CR06 5FU/LV 604 pts
All treatment-related deaths (%)
26 (3.8%) 17 (2.5%) 18 (5.9%)
3 (0.5%)
Deaths in pts with no appropriate dose
reduction/protocol violation (%)
17 (2.4%) 6 (0.9%) 11 (3.6%) -
Deaths in pts treated according to the protocol
(%)
9 (1.4%) 11 (1.6%) 7 (2.3%)
3 (0.5%)
Cunningham D. et al British Journal Cancer 1998; 77 (Supp. 2):15-21
Maughan T. et al Lancet 2002;359: 1555-1563
Toxic Deaths in Randomized Studies of Raltitrexed vs 5FU/LFA in advanced colorectal cancer patients

• Randomization in a 1:1 ratio
– Control arm : 5FU/LV:
• LV 20 mg/m2 IV bolus Days 1-5/ 28 days;6 cycles
• 5FU 370-425 mg/m2 IV bolus
– Experimental arm: Tomudex
• Raltitrexed 3mg/m2 in 15 min.IV infusion (q3wks. 8 cycles)
Popov I. et al European Journal Cancer 2008; 44:2201-2211
• Main objectives:
– RFS and OS as a non inferiority hypothesis in adjuvant stage III CC
– HR for RFS and OS < 1.25 at 1-sided α = 0.05
• Estimated number of patients required: 2.765 patients (703 events)
• Patients recruited until trial stop: 1.921 patients (ITT population)
• Final results in 993 eligible patients (PP population) who started and completed the allocated treatment (489 5-FU/LV and n = 504 Raltitrexed)
July/1999 (1838 pts recruited): IDMC recommended to stop recruitment due to 17 deaths (1.9%), out of 911 patients, observed in the Tomudex arm. The sponsor, AstraZeneca, decided to stop patient inclusion based on the results of an unscheduled private analysis of the first 647 patients.
Clinical Response and Survival from Randomized Studies of Raltitrexed vs 5FU/LFA in Advanced Colorectal Cancer Patients

Toxicities Grade 3-4 (%) 5FU Raltitrexed
Neutropenia 27 7.9
Febrile Neutropenia 4 2.2
Diarrhea 14.9 5.4
Stomatitis 12.4 0.9
Transaminases increase 0.6 20.5
SAEs reported 18.3 16.3
Treatment-related deaths 0.9 2.1
Deaths linked with protocol deviations - 1.1
Deaths in pts treated according to the
protocol
0.9 1.0
Popov I. et al European Journal Cancer 2008; 44:2201-2211
Randomized Study of Raltitrexed vs 5FU/LFA in Adjuvant Colon Cancer: PETACC-1 Study

ITT: HR for OS: 1.04 (90% CI 0.90–1.21)
5FU RTX
5y OS 62.3% 61.9%
PETACC-1 Study: Results
Popov I. et al European Journal Cancer 2008; 44:2201-2211
ITT: HR for RFS: 1.14 (90% CI 1.01–1.29)
5FU RTX
5y RFS 50.9% 46.7%
… “failed to demonstrate non-inferiority of raltitrexed”, but omitted to stipulate that this was limited to RFS and, more importantly, that
non-inferiority was demonstrated for OS. The crisp conclusion seemed like an epitaph justifying the premature closure of the trial and
stopping further investigation of raltitrexed.

Study Treatment Lin
e
Number
of
patients
Response (%) Median
TTP or
PFSα
(months)
Median
OS
(month
s)
Main
SevereToxicity
Number
of Toxic
deaths PR CR SD
Scheithauer et al. RTX 3 mg/m2 d1
Oxa 130 mg/m2 d1 q3w 1st 42 45 2 50 9α >14.5†
Neutropenia (22%)
Diarrhea (7%) 0
Scheithaueret et al. RTX 3 mg/m2 d1
Oxa 130 mg/m2 d1 q3w 2nd 36 33 0 47 6.5α >11†
Neutropenia (23%)
Diarrhea (6%) 0
Seitz et al. RTX 3 mg/m2 d1
Oxa 130 mg/m2 d1 q3w 1st 69 52 1 32 6.2α 14.6
Neutropenia (30%)
Diarrhea (17%) 2
Cascinu et al. RTX 3 mg/m2 d1
Oxa 100 mg/m2 d1 q3w 1st 58 45 5 22 6.5 >9†
Neutropenia (10%)
Asthenia (16%) 0
Feliu et al. RTX 3 mg/m2 d1
Oxa 130 mg/m2 d1 q3w 1st 48 38 8 25 8,2 >12†
Nausea-Vomiting
(12%)
Diarrhea (8%)
1
Gravalos et al. RTX 3 mg/m2 d1
Oxa 130 mg/m2 d1 q3w 1st 92 42 4 29 7.7α 15.6
Asthenia (19%)
Diarrhea (10%) 1
Main Phase II Clinical Studies Testing Raltitrexed in Combination with Oxaliplatin in Advanced Colorectal Cancer Patients
The total rate of treatment-related deaths, reported in phase II studies with this combination, was 4 in 345
pts (1,1%) and only 0,6% if we do not consider the treatment-related deaths reported by Seitz
Scheithauer W et al Cancer 2001: 91:1264-1271; Scheithauer W et al Ann Oncol 2001: 12:709-714; Seitz JF et al Ann Oncol 2002;13:1072-179; Cascinu S et al Ann Oncol 2002;13:716-720; Feliu et British Journal Cancer 2005; 93:1230-1235; Gravalos C et al Clin Transl Oncol 2012; 14:606-612;
†Median overall survivall not reached;

RR: FOLFOX4 36.3% vs TOMOX 45.6%; p=0.003 n= 183 pts
Randomized Phase II Trial: FOLFOX4 vs TOMOX
TOMOX: 7.7 m
FOLFOX4: 8.7 m
P= 0.29
TOMOX: 15.6 m
FOLFOX4: 17.2 m
P= 0.47
Overall survival
Progression-Free survival
Gravalos C et al Clin Transl Oncol 2012; 14:606-612;

Patients Characteristic Patients n. 144
R (n.72) + TOMOX (n.72)
Median Age, years (range) 68
PS 0/1/2 (%) 18/62/19
Main reasons to choose R or TOMOX
Similar efficacy and safety to other treatments (%) 19
Convenience of the administration (%) 18
Cardiovascular disease (%) 17
Resistance to FP (%) 14
Prevoius FP inacceptable toxicity (%) 10
Old age (%) 11
Most common grade 3-4 toxicities
Neutropenia (%) 8
Diarrhoea (%) 7
Anaemia (%) 5
Hepatic toxicity 4
Nausea (%) 2
Vomiting /%) 1
Toxic deaths (%) 1.4
Tolerability of raltitrexed when it is used in monotherapy and in combination with oxaliplatin (TOMOX) as advanced CRC treatment in normal clinical practice
Constenia M et al ASCO 2013: abs n.14648
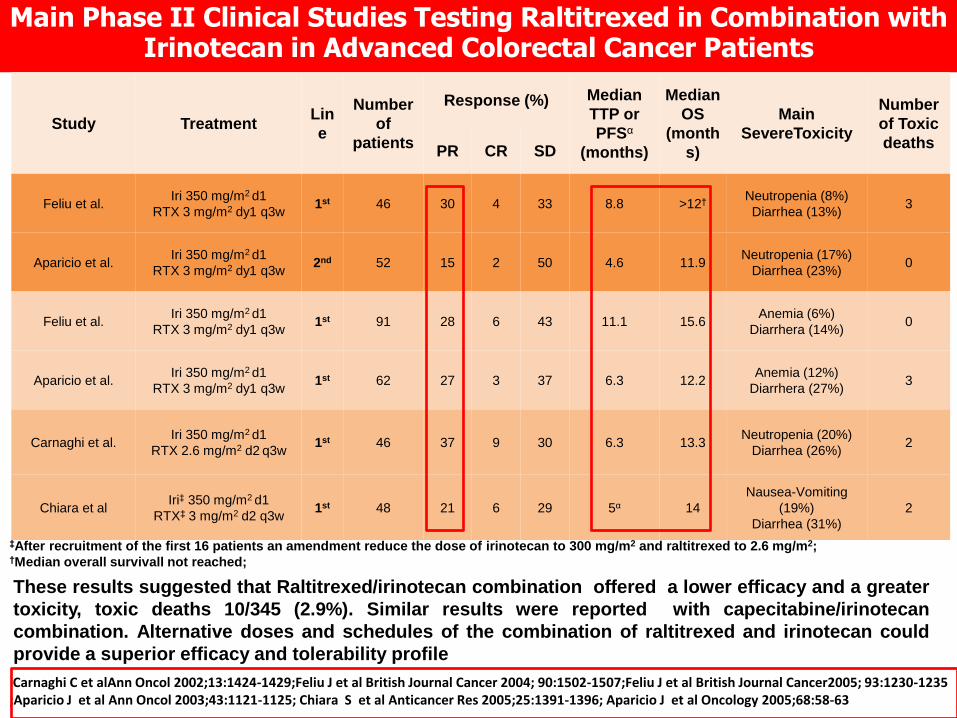
Main Phase II Clinical Studies Testing Raltitrexed in Combination with Irinotecan in Advanced Colorectal Cancer Patients
Study Treatment Lin
e
Number
of
patients
Response (%) Median
TTP or
PFSα
(months)
Median
OS
(month
s)
Main
SevereToxicity
Number
of Toxic
deaths PR CR SD
Feliu et al. Iri 350 mg/m2 d1
RTX 3 mg/m2 dy1 q3w 1st 46 30 4 33 8.8 >12†
Neutropenia (8%)
Diarrhea (13%) 3
Aparicio et al. Iri 350 mg/m2 d1
RTX 3 mg/m2 dy1 q3w 2nd 52 15 2 50 4.6 11.9
Neutropenia (17%)
Diarrhea (23%) 0
Feliu et al. Iri 350 mg/m2 d1
RTX 3 mg/m2 dy1 q3w 1st 91 28 6 43 11.1 15.6
Anemia (6%)
Diarrhera (14%) 0
Aparicio et al. Iri 350 mg/m2 d1
RTX 3 mg/m2 dy1 q3w 1st 62 27 3 37 6.3 12.2
Anemia (12%)
Diarrhera (27%) 3
Carnaghi et al. Iri 350 mg/m2 d1
RTX 2.6 mg/m2 d2 q3w 1st 46 37 9 30 6.3 13.3
Neutropenia (20%)
Diarrhea (26%) 2
Chiara et al Iri‡ 350 mg/m2 d1
RTX‡ 3 mg/m2 d2 q3w 1st 48 21 6 29 5α 14
Nausea-Vomiting
(19%)
Diarrhea (31%)
2
‡After recruitment of the first 16 patients an amendment reduce the dose of irinotecan to 300 mg/m2 and raltitrexed to 2.6 mg/m2; †Median overall survivall not reached;
These results suggested that Raltitrexed/irinotecan combination offered a lower efficacy and a greater
toxicity, toxic deaths 10/345 (2.9%). Similar results were reported with capecitabine/irinotecan
combination. Alternative doses and schedules of the combination of raltitrexed and irinotecan could
provide a superior efficacy and tolerability profile
Carnaghi C et alAnn Oncol 2002;13:1424-1429;Feliu J et al British Journal Cancer 2004; 90:1502-1507;Feliu J et al British Journal Cancer2005; 93:1230-1235 ;Aparicio J et al Ann Oncol 2003;43:1121-1125; Chiara S et al Anticancer Res 2005;25:1391-1396; Aparicio J et al Oncology 2005;68:58-63
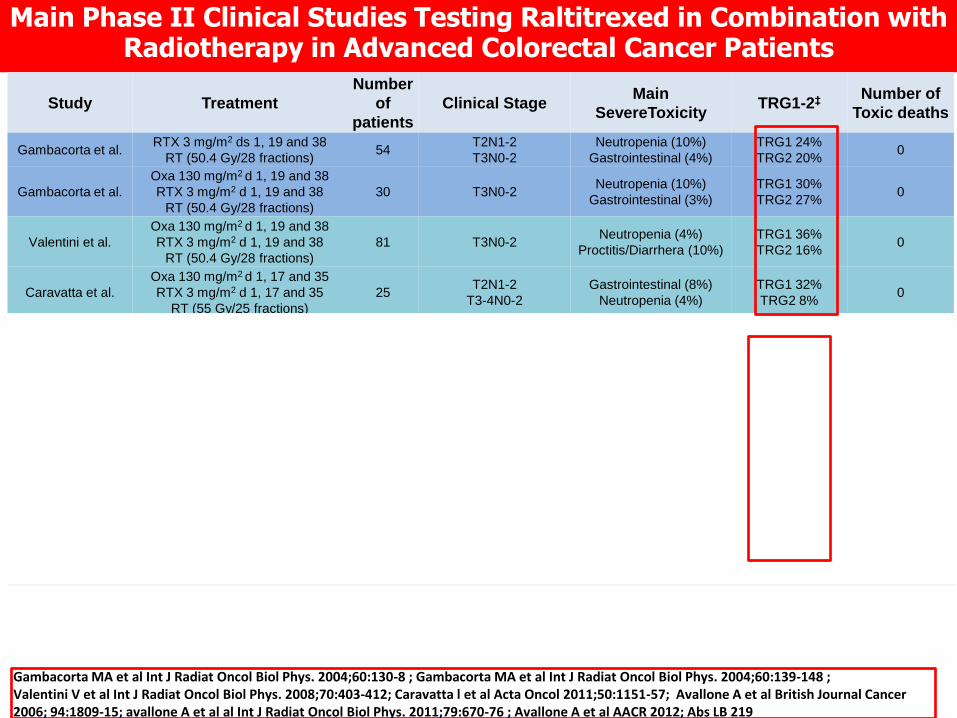
Main Phase II Clinical Studies Testing Raltitrexed in Combination with Radiotherapy in Advanced Colorectal Cancer Patients
Study Treatment
Number
of
patients
Clinical Stage Main
SevereToxicity TRG1-2‡
Number of
Toxic deaths
Gambacorta et al. RTX 3 mg/m2 ds 1, 19 and 38
RT (50.4 Gy/28 fractions) 54
T2N1-2
T3N0-2
Neutropenia (10%)
Gastrointestinal (4%)
TRG1 24%
TRG2 20% 0
Gambacorta et al.
Oxa 130 mg/m2 d 1, 19 and 38
RTX 3 mg/m2 d 1, 19 and 38
RT (50.4 Gy/28 fractions)
30 T3N0-2 Neutropenia (10%)
Gastrointestinal (3%)
TRG1 30%
TRG2 27% 0
Valentini et al.
Oxa 130 mg/m2 d 1, 19 and 38
RTX 3 mg/m2 d 1, 19 and 38
RT (50.4 Gy/28 fractions)
81 T3N0-2 Neutropenia (4%)
Proctitis/Diarrhera (10%)
TRG1 36%
TRG2 16% 0
Caravatta et al.
Oxa 130 mg/m2 d 1, 17 and 35
RTX 3 mg/m2 d 1, 17 and 35
RT (55 Gy/25 fractions)
25 T2N1-2
T3-4N0-2
Gastrointestinal (8%)
Neutropenia (4%)
TRG1 32%
TRG2 8% 0
Avallone et al.
Oxa 100 mg/m2 d 1, 15 and 29
RTX 2.5 mg/m2 d 1, 15 and 29
5-FU 900 mg/m2 d 2, 16 and 30
FA 250 mg/m2 d 2, 16 and 30
RT (45 Gy/25 fractions)
31
T3N0 with MRF† ≤ 5mm
and/or < 5cm a.v.α
T2-3N1-2
T4N0-2
Neutropenia (32%)
Diarrhea (19%)
TRG1 42%
TRG2 29%-- 0
Avallone et al.
Oxa 100 mg/m2 d 1, 15 and 29
RTX 2.5 mg/m2 d 1, 15 and 29
5-FU 800 mg/m2 d 2, 16 and 30
FA 250 mg/m2 d 2, 16 and 30
RT (45 Gy/25 fractions)
32
T3N0 with MRF† ≤ 5mm
and/or < 5cm a.v.α
T2-3N1-2
T4N0-2
Neutropenia (40%)π
Diarrhea (6%)
TRG1 38%
TRG2 22%-- 0
Avallone et al.
Bev 5 mg/Kg d -4 and 11
Oxa 100 mg/m2 d 1, 15 and 29
RTX 2.5 mg/m2 d 1, 15 and 29
5-FU 800 mg/m2 d 2, 16 and 30
FA 250 mg/m2 d 2, 16 and 30
RT (45 Gy/25 fractions)
46
T3N0 with MRF† ≤ 5mm
and/or < 5cm a.v.α
T2-3N1-2
T4N0-2
TanyM1¥
Neutropenia (30%)π
Diarrhea (6%)
TRG1 50%
TRG2 30%-- 0
π With 5-FU 800 mg/m2 grade 4 neutropenia was less pronounced compared to 5-FU 900 mg/m2 (9% vs. 22%); ¥Rectan cancer with synchronous resectable or initially unresectable metastatic disease.
Gambacorta MA et al Int J Radiat Oncol Biol Phys. 2004;60:130-8 ; Gambacorta MA et al Int J Radiat Oncol Biol Phys. 2004;60:139-148 ; Valentini V et al Int J Radiat Oncol Biol Phys. 2008;70:403-412; Caravatta l et al Acta Oncol 2011;50:1151-57; Avallone A et al British Journal Cancer 2006; 94:1809-15; avallone A et al al Int J Radiat Oncol Biol Phys. 2011;79:670-76 ; Avallone A et al AACR 2012; Abs LB 219

Phase II Study Testing Induction CT with CAPOX followed by Chemoradiotherapy in Locally Advanced Rectal Cancer
Study Treatment (DR) Number of
patients
Cardiac/Tromboembolic
Toxicity
(%)
Number
of Toxic
deaths
Chau et al.
2006
Capecitabine 2000 mg/m2 d1-14
Oxa 130 mg/m2 d1
Followed by
RT + Xeloda
79 10 4
Schou et al
2012
Capecitabine 2000 mg/m2 d1-14
Oxa 130 mg/m2 d1
Followed by
RT + Xeloda
84 6 4
Chau I et al JCO 2006, 24: 668-674; Schou JV et Ann Oncol 2012, 23:2627-2633

“One bird with two stones”
How can we optimise tolerability and efficacy of raltitrexed?
Thymidylate-Synthase
Pyrimidine (dUMP)
binding site
Folate
binding site

Raltitrexed/5-FU: schedule-dependent synergism in vitro
Combination treatment †
Combination
index † † Interpretation
Raltirexed
(24-h inc)
5-FU
(4-h inc)
5-FU
(4-h inc) Raltirexed
(24-h inc)
0.59
4.98
Strongly
synergistic
Strongly
antagonistic
† at equitoxic doses † † combinayion index at IC50 in HCT-8 colon cancer cell line
Longo et al. Clin Cancer Res 1998; 4: 469-73
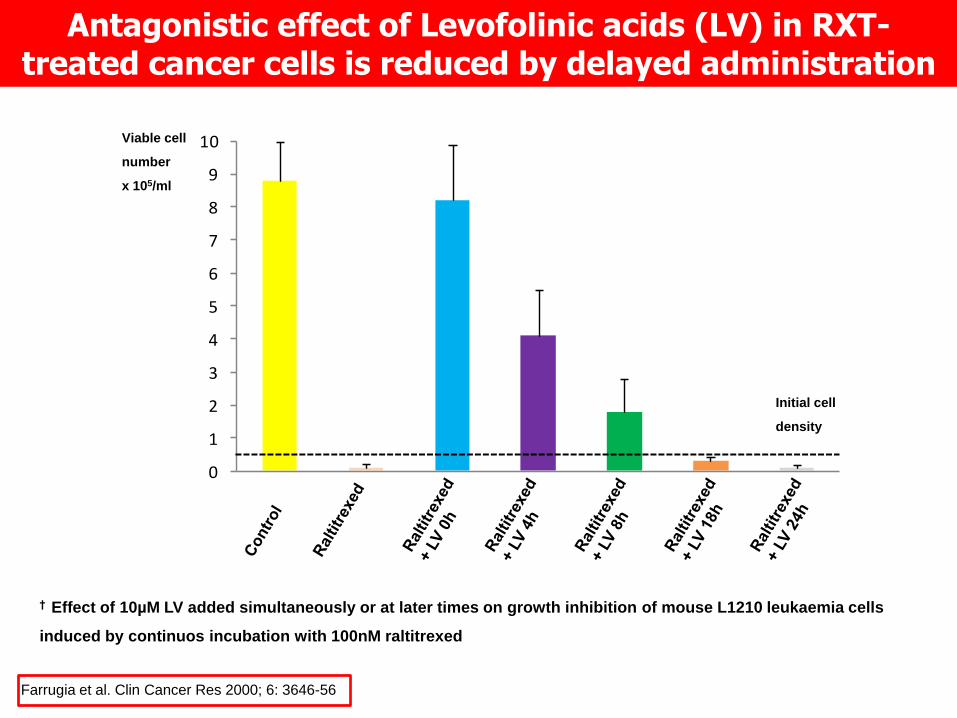
Antagonistic effect of Levofolinic acids (LV) in RXT-treated cancer cells is reduced by delayed administration
† Effect of 10µM LV added simultaneously or at later times on growth inhibition of mouse L1210 leukaemia cells
induced by continuos incubation with 100nM raltitrexed
Farrugia et al. Clin Cancer Res 2000; 6: 3646-56
0
1
2
3
4
5
6
7
8
9
10Viable cell
number
x 105/ml
Initial cell
density

Raltitrexed Polyglutamation is a Rapid Metabolic Process
Jackman AL. et al Cancer Res 1991; 51:5579-5586

Farrugia et al. Clin Cancer Res 2000; 6: 3646-56
Effect of the delayed administration of LV on BALB/c mouse

DHFR
Premetrexed Premetrexed glu2-4
FPGSRFC
Membrana
cellulare
DNAdTTPdTDPdTMPdUMP
Timidilato-Sintasi
Sito di legame delle pirimidine (dUMP)
Sito di legame del Folato
LFA 5,10-CH2 FH4 glu2.6 FH2
GARFT
5,10-CH2 FH4 glu2.6
IMP AMP
Raltitrexed Raltitrexed glu2-4
FPGSRFC
RNAFUTP
5-F-DHU
DPD
5-FU FUDP
F-dUMP
F-dUDP
RR
F-dUTP
FUMPOPRT
FPGSRFC
F-dUrd
TP
Capecitabina
5-DFCR 5-DFURTP
TK
CyDCE
Raltitrexed and Premetrexed

Channels0 50 100 150 200 250
Num
ber
060
120
180
240
CTR
Channels0 40 80 120 160 200
Num
ber
060
120
180
240
RTX
Channels0 50 100 150 200 250
Num
ber
020
4060
5FU-FA
Channels0 50 100 150 200
Num
ber
010
2030
40
RTX/5FU-FA
Channels0 50 100 150 200 250
Num
ber
010
2030
4050
60
RTX/5F
U
5FU
Channels0 50 100 150 200 250
Num
ber
010
020
030
040
050
0
Cytotoxic
Ratio
RTX/5FU-FA
HT29 LoVo
50:50
75:25
25:75
0 0 . 2 0 . 4 0 . 6 0 . 8 1 . 00
0 . 5
1 . 0
1 . 5
2 . 0
2 . 5
F r a c t io n a l E f f e c t
CI
0 0 . 2 0 . 4 0 . 6 0 . 8 1 . 00
0 . 2
0 . 4
0 . 6
0 . 8
1 . 0
F r a c t io n a l E f f e c t
CI
0 0 . 2 0 . 4 0 . 6 0 . 8 1 . 00
0 . 5
1 . 0
1 . 5
F r a c t io n a l E f f e c t
CI
0 0 . 2 0 . 4 0 . 6 0 . 8 1 . 00
0 . 5
1 . 0
1 . 5
F r a c t io n a l E f f e c t
CI
0 0 . 2 0 . 4 0 . 6 0 . 8 1 . 00
0 . 5
1 . 0
1 . 5
2 . 0
F r a c t io n a l E f f e c t
CI
0 0 . 2 0 . 4 0 . 6 0 . 8 1 . 00
0 . 5
1 . 0
1 . 5
F r a c t io n a l E f f e c t
CI
KB Cal27 HT29 LoVo
% o
f Ap
op
tosis
0
5
10
15
20
25
30 Ctr FA
RTX RTX-FA
5FU RTX-5FU
5FU-FA RTX/5FU-FA
*
*
*
*
KB Cal27 HT29 LoVo
% o
f Ap
op
tosis
0
5
10
15
20
25
30 Ctr FA
RTX RTX-FA
5FU RTX-5FU
5FU-FA RTX/5FU-FA
* *
* *
* *
* *

DNA dTTP dTDP dTMP dUMP
Thymidylate-Synthase
Pyrimidine (dUMP)
binding site
Folate
binding site
Raltitrexed Raltitrexed glu2-4 FPGS RFC
RNA FUTP
DPD
5-FU FUDP
F-dUMP
F-dUDP
RR
F-dUTP
FUMP
OPRT
5-DFUR
TP
5-DFCR
CyD Capecitabine
TP
F-dURD
TK
CE
FPGS RFC
cell membrane Folinic Acid 5,10-CH2 FH4 glu2.6
cell membrane
5-F-DHU
F-citrate
cardiotoxicity
neurotoxicity
GI toxicity
mielotoxicity
GI toxicity mielotoxicity
Catabolism 90%
Anabolism 10%
Biochemical Mechanisms of Cap, 5-FU, RTX and FA
Patients unable to tolerate fluoropyrimidine •Polymorphism in genes responsible for metabolism,
especially DPD (3-5%)
•Fluoropyrimidine-induced cardiotoxicity (4-6%)
•Fluoropyrimidine inappropriate ?%

Cardiotoxicity of Fluoropyrimidine (FP)
• Cardiotoxicity of FP is a potentially lethal toxicity.
•Asymptomatic ECG changes may occur in up to 80 % of patient.
•The mechanism is not well understood. Suggested coronary vasospasm,
direct myocardial toxicity, coronary thrombosis and autoimmune mechanism.
•Bolus of 5-FU has the lowest rate
•Risk factors are: higher doses of FP; prior chest radiation; history of
cardiovascular disease;
•The majority of events occur in the first cycle
•Cardiotoxicity is generally reversible after cessation of FP therapy
•Re-exposure risk is reported to be 80-100%, although FP dose reduction or
nitrates and calcium blockers used to prevent cardiotoxicity
Jensen S et al A Cancer Chemother Pharmacol 2006; 58: 487-493

Patients Characteristic Study
Kelly et al.84 Price et al.14
Median Age, years (range) 68 (33-83)
62 (36-81)
Diagnosis (total n. patients) 111 42
Colorectal cancer 107 (96 %) 39 (93%)
Anal cancer 2 (2%) -
Appendicular cancer 1 (1%) -
Oesophageal cancer 1 (1%) 2 (5%)
Biliary cancer - 1 (2%)
Treatment (cardiotoxic event/n. patients)
First-line raltitrexed 2/46 -
Second-line raltitrexed 3/65 0/42
Cardiotoxicity in patients treated with raltitrexed because experiencing
fluoropyrimidine-induced cardiotoxicity or having cardiac risk factors
Price T et al Ann Oncol 2012; 23 (suppl 9): abs 519; Kelly C et al Eur J Cancer 2013
In the study of Kelly 16% of patients were treated with neoadjuvant intent and 18% with adjuvant intent

Study Treatment Line Number of
patients
Raltitrexed
completed
Severe
Toxicities
Number
of Toxic
deaths
3-year
RFS
(%)
3-year
OS
(%)
Wilson et al. RTX 3 mg/m2 d1
q3w 2st
44
(42 GI/hematoxicity ;
2 cardiac toxicity)
84% 7% 0 71 84
Wilson KS et al Cancer Invest 2007; 25 : 711-714
Raltitrexed in patients with fluoropyrimidine intolerance during adjuvant treatment

Clinical Case 52 yrs Female
Dx : Colon cancer, liver metastases
CEA= 672 ng/ml ; Kras mut
No-comorbidities
ECG: N; EcoC: FE:65%
Metastatic colorectal cancer
in 1° or 2° line N=250
R A N D O M I Z E
Bevacizumab 5 mg/ Kg day 1 with + mFolfox-6/mOXXEL x 12 cycles Bevacizumab to be continued until PD
Bevacizumab 5 mg/ Kg 4 days before CT+ mFolfox-6m/OXXEL x 12 cycles Bevacizumab to be continued until PD
OBELICS
Optimization of BEvacizumab scheduLIng within Chemotherapy Scheme
EudraCT Number: 2011-004997-27
Ricerca Finalizzata 2009 – Codice RF-2009-1539464
Response evaluation will be performed at week 12, 24 after the onset of
the trial and and every 3 months thereafter, until disease progression. Early-PET; CEC;CEP;SNP-VEGF,mRNA,

Clinical Case Angina –like chest pain after 5-FU infusion of 1st cycle
ECG:N; CE and Trop T: within the limits.
We planned antianginal prophylaxis and reduced dose of 5-FU
Angina –like chest pain after 5-FU infusion of 2st cycle
ECG:with abnormalities;CE and Trop T: within the limits.

Clinical Case She switched to raltitrexed 2.5 mg/m2 + OXA biweekly with FA
supplementation (50 mg days 3-10) with 3rd cycle without BEV
Toxicities : elevated trans, asthenia,
neuropathy and nausea grade 1,
ECG:N; CE and Trop T: within the
limits.
No Angina –like chest pain
After 4 mTOMOX and 2 mFolfox6
CEA 72 ng/ml (427 ng/ml after 2 cycles mFolfox6)
Re-administered BEV

Summary
The clinical development of raltitrexed has been impaired by the treatment-related mortality reported in some large phase III studies in monotherapy in CRC. However, most of the treatment-related deaths, mainly due to a combination of gastrointestinal and myelosuppression toxicity, occurred :
a) in the absence of appropriate dose reduction or delay of the schedule (i.e. failing to measure or modify the dose for creatinine clearance as for the prescribing information);
b) when patients did not receive a prompt management of toxicity.
There has been a remarkable evolution of the treatment for colorectal cancer in the last years. However, TS inhibition remains a major target in the era of molecular therapy .
Perhaps this inappropriate management of patients was a consequence of the simplicity of raltitrexed administration that may have induced an unwarranted degree of optimism in the investigators. When the patients received appropriate raltitrexed treatment, the incidence of treatment-related deaths was comparable, if not less, with that following treatment with 5FU.
Phase II studies with oxaliplatin or irinotecan, plus raltitrexed, have yielded similar results to those obtained with these drugs plus 5FU.
However, the results of raltitrexed combinations studies have been overshadowed by the disappointing results of phase III trials.

Summary 2
Refinement of the optimal dose and schedule of 5FU has taken >30 years. The initial 5 days per month schedule has evolved to the current hybrid 5FU bolus/continuous infusion de Gramont scheme.
The devil is in the details. Refinement of the application of anti-cancer treatment should be a main topic in clinical research (combinations, schedule, dosage etc).
Our more than 10-year experience with dual TS inhibition (raltitrexed/5FU) combined with LFA potentiation and rescue is conceptually similar yet more convenient compared to the de Gramont scheme. This approach may be a more effective and manageable use of raltitrexed and provide a more suitable application of this drug.
Cardiotoxicity is an unpredictable and potential lethal side-effect, most likely understimate, of fluoropyrimidine.
Raltitrexed is a reasonable option in fluoropyrimidine intolerant CRC patients in metastatic disease but might be particularly appealing in adjuvant setting, where cure is the aim of the treatment, in patients unable to undergoing fluoropyrimidine.

Thank You for your attention





![acid dexaexilcolic,acid folic ]n dezvoltarea creer nn.pdf](https://cdn.vdocuments.mx/doc/165x107/577cb57f1a28aba7118d31d3/acid-dexaexilcolicacid-folic-n-dezvoltarea-creer-nnpdf.jpg)

