
Quality Report Quarter 4, 2013/14 v1.1
Contents
Section 1: Quality Introduction ..................................................................................................................... 2
Section 2: Summary Quality Issues ................................................................................................................ 1
Section 3: CQC Interventions: ....................................................................................................................... 4
Section 4: Quarterly Key Quality Issues and Action Plans (by Provider) .............................................................. 6
4.1 Guy’s & St. Thomas’s NHS Foundation Trust .................................................................................................... 7
4.2 Guy’s & St. Thomas’s NHS Foundation Trust – Community Health Services .................................................... 8
4.3 King’s College Hospital NHS Foundation Trust ................................................................................................ 16
4.4 South London & Maudsley NHS Foundation Trust .......................................................................................... 25
4.5 St George’s Hospital NHS Trust - not updated for Q3 ..................................................................................... 30
4.6 Continuing Care Providers ............................................................................................................................... 35
4.7 Primary Care (including WIC, community outpatients etc.) ........................................................................... 36
Section 5: Patient Experience ..................................................................................................................... 37
5.1 Guy’s & St. Thomas’s NHS Foundation Trust (including Community Health Services) .................................. 37
5.2 King’s College Hospital NHS Foundation Trust ................................................................................................ 39
5.3 South London & Maudsley NHS Foundation Trust .......................................................................................... 41
5.4 St George’s Hospital NHS Trust - Not updated Q3 ......................................................................................... 43
5.5 Primary Care (including WIC, community outpatients etc.) ........................................................................... 44
5.6 Friends and Family Test – Maternity ............................................................................................................... 45
Section 6: Engagement Issues and Feedback ................................................................................................ 46
Section 7: Quality Alerts ............................................................................................................................ 47
7.1 Quality Alerts: Q3 2013-14 Update .................................................................................................................. 47
Section 8: Clinical Site Visits ................................................................................................................................... 51
8.1 Clinical Site Visits ............................................................................................................................................. 51
8.2 Clinical Site Visits & Detail ................................................................................................................................ 52

Section 1: Quality Introduction
The NHS is the only healthcare system in the world with a definition of quality enshrined in legislation. An
organisation delivering high quality care will be offering care that is clinically effective, safe and delivering as
positive an experience as possible for patients.
The following Quality Report provides information pertaining to our main healthcare providers, Guy’s and St
Thomas’s NHS Foundation Trust, King’s College Hospital NHS Foundation Trust, South London and Maudsley NHS
Foundation and St Georges Healthcare NHS Trust. It covers information on key quality issues and action plans,
patient experience, patient engagement issues – specific to Lambeth CCG, quality alerts and clinical visits and
audits. This is the first of regular quarterly quality reports and in light of the Francis, Keogh and Berwick reports
and collaborative work with other regulators and our providers is likely to be amended over time to enable a
comprehensive picture of ‘quality’ within our provider services.
Lambeth Clinical Commissioning Group: Francis update
There is a CCG plan in place to focus on key identified areas highlighted in the recommendations. A Quarter 3
update of the Lambeth CCG actions will be taken to the March Governing Body.
Lambeth’s Commissioning for Quality Framework sets out the CCG approach to addressing quality and patient
safety issues and affirms our commitment to working collaboratively and to have meaningful engagement with
healthcare providers, patients, carers and their communities and other organisations. The BIG Lambeth Health
Debate in the summer and the Lambeth Quality Summit held last October are examples of this approach in
practice, with feedback informing the CCG 2 and 5 year plans. The CCG has also worked with Healthwatch
Lambeth during the past year to develop a close working relationship.
The CCG is part of the South London Quality Surveillance Group which provides a platform for sharing intelligence
with other parts of the local system. We also receive information from external data sources, including providers,
to enable triangulation of information and assessment of quality and safety in our service providers. GPs are able
to provide electronic feedback on Quality Alerts relating to all local main providers and these are shared with
providers to address systemic issues and responses shared back to GP practices. The development of reverse
Quality Alerts are in progress.
Clinicians at the CCG are committed to working together to share information and support seamless, integrated
pathways of care for patients. They lead on the CCG programmes of work which are integrated with LBL and
where relevant with Southwark CCG. The provider clinical quality review and serious incident monitoring
meetings are chaired by clinicians and provide the opportunity for the review, discussion and challenge of quality
and patient safety information, including that received from external reports e.g. national staff and patient
surveys and national audit reports. A quarterly Quality Report was developed in 2013 and provides the full
Governing Body with an overview of quality and patient safety within providers.

1
Section 2: Summary Quality Issues
Provider
Quality Issue Description of Quality Issue
Outcomes/ Actions
1
GSTT
District Nursing Service (GSTT Community) (p8)
District nurse productivity and perceived relationship with GP practices poor. Provision of continence service poor. Quality Alerts mainly due to non DN attendance. GSTT review concurs with commissioner findings.
Community Services provided report on District Nursing services to November CQRG with clear understanding of the issues to be addressed.
Community nurse improvement plan in place. Being monitored at fortnightly conference calls and at GSTT Community Services core contract meetings
Reports shared with all Lambeth GPs via locality board leads
Joint care planning CQUIN (LTC) at risk – targets amended
Risk to meeting service delivery plan – on GSTT and LCCG corporate risk registers
2
GSTT
Anti-coagulation service (GSTT Community) (p12)
Anticoagulation pathway not robust leading to poor patient management of INRs / anticoagulation therapy.
Meeting involving KCH, GSTT (Acute and community) and Medicines Management Team and chaired by John Balazs has been held. Action plan agreed. Discussed at February CQRG as action plan not implemented by GSTT. GSTT have subsequently set up internal group to take actions forward. Task and finish group continues to meet.
3
GSTT
Discharge letters to GPs (p7) The quality and timeliness of the letters has been identified as unsatisfactory.
Audit of discharge letters completed for Lambeth and Southwark (two practices) confirmed issues with both delay in sending out the discharge letters and the quality of the discharge information. This was discussed at GSTT CQRG October 2013 and Feb 2014 and will be included as a contractual requirement for 2014/15.
4
GSTT
Complaints (p7)
Complaint responses within 25 working days (Trust target) is 31%. The majority of other complaints are met with complainant agreed extension. Complaint response times remain approximately 60 working days with no reduction. The Trust quote a 97% response within agreed timescales but this is not comparable with other Trusts. Patient feedback from complaints is only sought on an annual basis rather than after each complaint.
Quarter 3 complaints report presented to the February CQRG. Issues around response times were highlighted and lack of patient feedback were discussed along with the Francis recommendation for providers to publish anonymised complaint information and responses.
Southwark CCG have recently completed a deep dive into 12/13 complaints within KCH, SLaM and GSTT at the request of their Integrated Governance Committee. It does not cover all the quality issues highlighted in this report.
A meeting to discuss complaint issues with GSTT is required

2
Provider
Quality Issue Description of Quality Issue
Outcomes/ Actions
5
GSTT
Falls (p7)
The number of major falls reported by the Trust for December was 0. However, it was noted in the Q3 Risk Management Report discussed at the February CQRG that fractures resulting from falls (which should be reported as a serious incident) differed: Q1 = 10, Q2 = 6, Q3 = 6.
The Trust has been asked to report all fall incidents resulting in fractures as a serious incident. There is a category on STEIS for this. This has been followed up in writing including the Associate Medical Director with responsibility for patient safety, Adrian Hopper.
6
GSTT
Maternity outlier alert for maternal non-elective readmissions within 42 days of delivery (17 Feb 2014 Trust letter)
Readmissions for this group have been identified by the CQC as showing a sudden increase from Q1 2013/14. Significant rates of women are being readmitted with a primary diagnosis of Z39.1 (Care and examination of lactating mother).
Investigation being undertaken by the Trust. Findings to be shared with the CQRG.
7
SLaM Discharge from secondary to
primary care (p27,29)
The December 2013 figure was 20% against target of 50% (CQUIN final figure). Currently based on % of patients to which a discharge letter has been sent to their GP within 1 week of discharged. Q3 audit into the quality of discharge plans showed improvement.
This will be replaced by a CQUIN indicator that aims to have more recovery focussed on crisis planning documentation being
sent to GPs when users transfer from secondary care.
8
SLaM
Delayed Discharge/Transfer of
Care (p27,29)
December figure 289 against target of 0. However, this is a decrease over the past 12 months (476 April and 328 July).
It is a whole-system issue including an impact to social care funding. The primary care incentive scheme for 2014-15 aims to incentivise GPs to effectively manage patients discharged from SLaM services to primary care. This also links into a CQUIN relating to the % of users on CPA in the last six months discharged with a comprehensive care plan.
3
Provider
Quality Issue Description of Quality Issue
Outcomes/ Actions
9
KCH
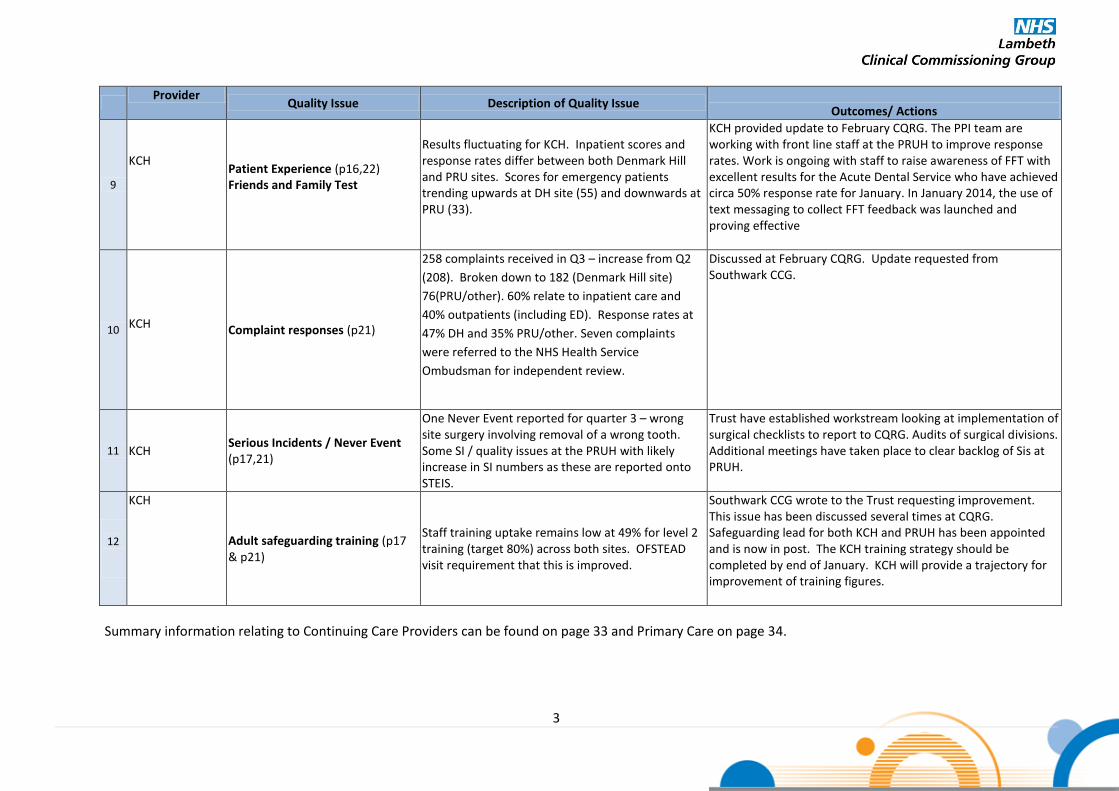
Patient Experience (p16,22) Friends and Family Test
Results fluctuating for KCH. Inpatient scores and response rates differ between both Denmark Hill and PRU sites. Scores for emergency patients trending upwards at DH site (55) and downwards at PRU (33).
KCH provided update to February CQRG. The PPI team are working with front line staff at the PRUH to improve response rates. Work is ongoing with staff to raise awareness of FFT with excellent results for the Acute Dental Service who have achieved circa 50% response rate for January. In January 2014, the use of text messaging to collect FFT feedback was launched and proving effective
10
KCH Complaint responses (p21)
258 complaints received in Q3 – increase from Q2
(208). Broken down to 182 (Denmark Hill site)
76(PRU/other). 60% relate to inpatient care and
40% outpatients (including ED). Response rates at
47% DH and 35% PRU/other. Seven complaints
were referred to the NHS Health Service
Ombudsman for independent review.
Discussed at February CQRG. Update requested from Southwark CCG.
11
KCH
Serious Incidents / Never Event (p17,21)
One Never Event reported for quarter 3 – wrong site surgery involving removal of a wrong tooth. Some SI / quality issues at the PRUH with likely increase in SI numbers as these are reported onto STEIS.
Trust have established workstream looking at implementation of surgical checklists to report to CQRG. Audits of surgical divisions. Additional meetings have taken place to clear backlog of Sis at PRUH.
12
KCH
Adult safeguarding training (p17 & p21)
Staff training uptake remains low at 49% for level 2 training (target 80%) across both sites. OFSTEAD visit requirement that this is improved.
Southwark CCG wrote to the Trust requesting improvement. This issue has been discussed several times at CQRG. Safeguarding lead for both KCH and PRUH has been appointed and is now in post. The KCH training strategy should be completed by end of January. KCH will provide a trajectory for improvement of training figures.
Summary information relating to Continuing Care Providers can be found on page 33 and Primary Care on page 34.

4
Section 3: CQC Interventions:
Name of Provider(s)
CQC Regulation Intervention Action Reported Date of CQC visit
& report Description of Agreed Improvement Plan / Trajectory
Description of CCG Assurance Process
Dulwich Care Centre
Nursing Home not compliant with CQC standard –
Outcome 9 and 21. DCC were issued 2 warning
notices relating to two CQC standards: record
keeping and management of medicines.
Follow up visit 9
th December
2013 CQC report
published 21 December 2013
CQC have removed warning notices, and confirmed that DCC are now compliant outcome 21 in relation to record keeping CQC have identified that work is required in respect of outcome 9 in relation to management of medicines On 31 December 2013 DCC provided LBL with a comprehensive Management of Medicines Action Plan in response to CQC findings
LBL and Lambeth CCG suspension on any new placements remain in place until the embargo has been lifted. CQC to meet again with DCC and LBL in February 2014 Monitored by LBL and fed back to CCG via SCMT. Director Lead: Moira McGrath
Ladywell Hospital (SLaM)
During a routine inspection the CQC identified that the standard relating to safety and suitability of premises was not met.
6 December 2013 CQC report
published 10 January 2014
The non-compliance related to inadequate maintenance of the premises. This was judged to have a minor impact on those using the service. The Trust was given until 24 January to submit a report and action plan.
Director Lead: Christine Caton To be monitored via the SLaM contract.
Princess Royal University Hospital
(PRU)
One of the pilot sites for the new inspection process. A number of regulations required actions.
2-4, 10 December CQC report published 6
February 2014
The PRU have developed an action plan which is being monitored by Bromley and Southwark CCGs.
Bromley CCG is leading the monitoring of this plan.
The Laurels Care Home
During the routine inspection, CQC identified that
LCH were failing to comply with Outcome 13 –
staffing levels and issued a warning notice. The
standard is: that there should be enough
members of staff to keep people safe and meet
their health and welfare needs.
8th
October 2013
CQC report published on 5
th
December 2013
Following the CQC inspection, LCH increased the staffing levels within the home CQC are due to revisit in January / February 2014
Monitored by LBL contract team, and feedback to SCMT Director Lead: Moira McGrath

5
Name of Provider(s)
CQC Regulation Intervention Action Reported Date of CQC visit
& report Description of Agreed Improvement Plan / Trajectory
Description of CCG Assurance Process
St Georges Healthcare NHS
Trust
During a routine inspection on 15-17 August 2013 CQC identified concerns regarding compliance with three standards:
Management of medicines
Staffing
Records
15-17 August CQC report
published 24 October 2013
The action plan has been monitored by Wandsworth CCG with some actions due in February. A verbal update will be provided to the Integrated Governance Committee.
Director Lead: Moira McGrath

6
Section 4: Quarterly Key Quality Issues and Action Plans (by Provider)
Quality Information Glossary
SHMI - The Summary Hospital-level Mortality Indicator (SHMI) is a national mortality indicator. It is a statistical
model which calculates the expected number of deaths at an individual provider and compares this to the actual
number of deaths within the period. A value of less than 1 indicates that the mortality rate is lower than would be
expected, and a figure greater than 1 would indicate that the mortality rate is higher than would be expected.
CAS Alerts - The Central Alerting System (CAS) is a web-based cascading system for issuing patient safety alerts,
important public health messages and other safety critical information and guidance. Should a trust have a CAS
alert outstanding, it means that the Trust has not yet taken the actions required to step down the alert, and that
the alert is overdue.
VTE Risk Assessments – All patients who are admitted to hospital should have a venous thromboembolism (VTE)
risk assessment completed to assess whether the preventative measures need to be taken to minimize the risk of
the patient developing a blood clot.
Friends and Family Test – From April 2013 all trusts had to implement the Friends and Family Test (FFT) and ask
patients (initially inpatients and those attending A&E) whether they would recommend A&E and inpatient wards
to their friends and family if they needed care or treatment. Trusts were set the target of achieving a 15%
response rate for Q1 (rising to 20% in Q4), and improve their scores over the course of the year. Results of the
surveys will begin to be published nationally from the end of June.
From January 2014 the NHS Friends and Family Test results for maternity services will be published on the NHS
Choices website. From December 2014 the Test will be rolled out at mental health trusts.

7
4.1 Guy’s & St. Thomas’s NHS Foundation Trust
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
Reporting of SIs The numbers of reported Serious Incidents remains consistent for GSTT. Concerns have been raised around the process of timely reporting of Maternity SIs and the CCG continues to work with the Trust to ensure robust processes are in place. Completed investigation report submission times have improved in line with changes to the pressure ulcer investigation form. GSTT acknowledge more training is needed for some investigators.
GSTFT Serious Incident Review Meetings are held monthly to allow all incidents to be reviewed appropriately and actions / themes identified and discussed in a timely manner. These meetings are chaired by the Network Clinical Quality Lead for the CCG. Lambeth CCG continues to work proactively with GSTT Patient Safety Team to speed up RCAs GSTT to hold workshops/masterclass to improve staff understanding of Root Cause Analyses (RCA).
GSTT CQRG and SI Review
Group
2
Never Events There were no new Never Events reported in Q3, 2014.
The details of any Never Events are reported in the Serious Incidents section of Integrated Governance and Performance Report
GSTT CQRG and CCG SI
Review Group
3
Falls: The number of major falls reported by the Trust for December was 0. However, it was noted in the Q3 Risk Management Report discussed at the February CQRG that fractures resulting from falls (which should be reported as a serious incident) differed: Q1 = 10, Q2 = 6, Q3 = 6.
The February CQRG requested that GSTT report all falls resulting in fractures as serious incidents for which there is a STEIS category. This was followed up in writing.
GSTT CQRG
4 Survey of in-patient experience showed patients were not satisfied with discharge information
All directorates mandated by the Director of Nursing to focus on discharge improvement. GSTT Team visited Newcastle upon Tyne as had come out top in UK re patient experience
GSTT CQRG
5
Complaints
Although number of complaints at GSTT is relatively static, there are some key problem areas in the Trust; the most frequent area for complaints was clinical care, followed by waiting times / delays / cancellations, closely followed by communication. Response times are longer than commissioners would like to see with 31% of complaints responded to within 25 working days. The majority of others have agreed extensions and meet these deadlines. Average response time is 60 working days which is not reducing.
More detailed sub categories of complaints were included in the
Q3 report but there is a lack of absolute number including analysis
of delayed responses by area. Response rates are largely
unchanged. Currently patient views on complaints process and
responses are only sought annually. It was highlighted at the
February CQRG that this should be more frequent given the delay
in the responses, with quarterly reports to the CQRG.
Complaints and patient experience will be included as a detailed
agenda item for further discussion at CQRG and a separate
conversation will be held with the Trust to discuss issues.
GSTT CQRG
6
Discharge letters to GPs The quality and timeliness of the letters had been identified as unsatisfactory. This has been on CQRG agenda for over a year. GSTT had been slow in identifying correct lead.
Audit of discharge letters for two practices completed. Findings
were that there were delays in receiving the letter and incomplete
information. Discussed at the December CQRG and working group
with John Balazs to be convened.
GSTT CQRG
7
Quality Alert Reporting More detailed Quality Alert information can be found at section 7.0. Quarter on quarter the GP Alerts have increased for GSTT from 16 (Q1) 26 (Q2) 30 (Q3). The main issues within the Acute services involve a range of appointment and communication issues between secondary and primary care. The main issue within community services relates to the failure of District Nurses to visit patients, provide the care required and communicate both with users and their GP.
The reverse quality alert system has been set up in November for the GSTT Quality Alert lead to submit Alerts. To date this have not been used and was raised at the February 2014 CQRG. A report and action plan to address identified District Nursing provision is currently monitored by the contracts meeting with updates to the CQRG. The potential impact on successful delivery of the Service Improvement plan has been added to the GSTT and Lambeth CCG corporate risk registers with a risk rating of 16.
GSTT CQRG
8
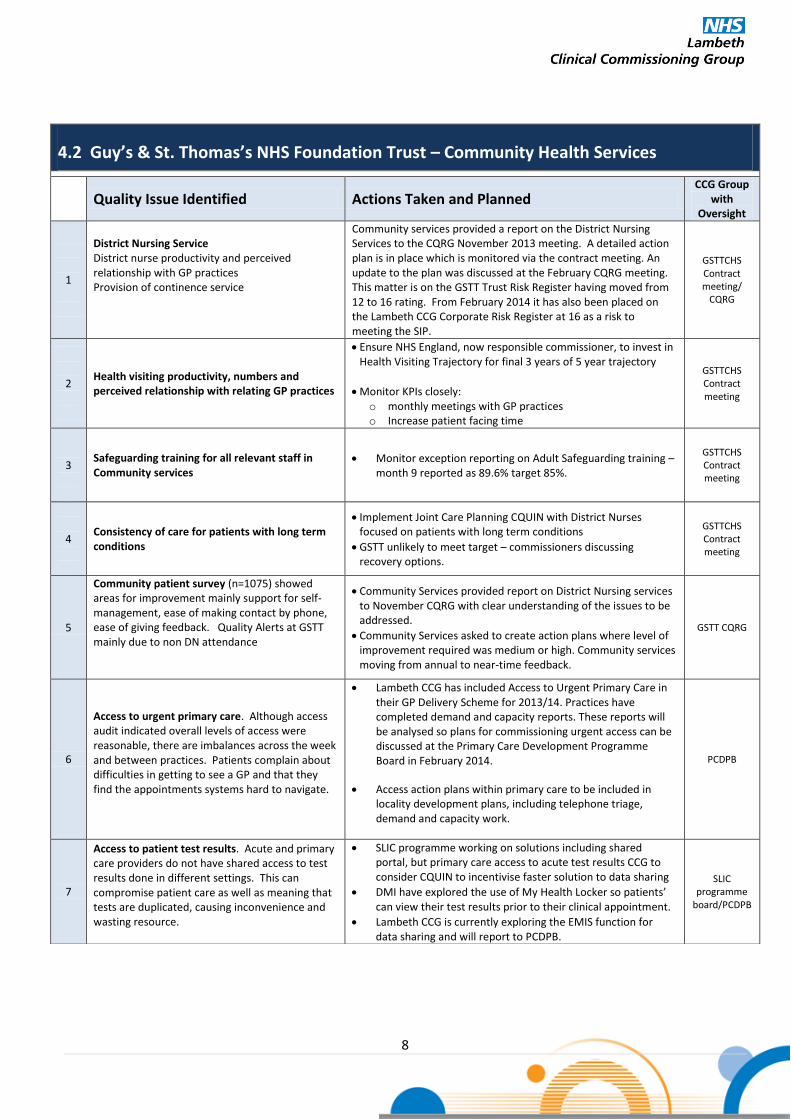
4.2 Guy’s & St. Thomas’s NHS Foundation Trust – Community Health Services
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
District Nursing Service District nurse productivity and perceived relationship with GP practices Provision of continence service
Community services provided a report on the District Nursing Services to the CQRG November 2013 meeting. A detailed action plan is in place which is monitored via the contract meeting. An update to the plan was discussed at the February CQRG meeting. This matter is on the GSTT Trust Risk Register having moved from 12 to 16 rating. From February 2014 it has also been placed on the Lambeth CCG Corporate Risk Register at 16 as a risk to meeting the SIP.
GSTTCHS Contract meeting/
CQRG
2
Health visiting productivity, numbers and perceived relationship with relating GP practices
Ensure NHS England, now responsible commissioner, to invest in Health Visiting Trajectory for final 3 years of 5 year trajectory
Monitor KPIs closely: o monthly meetings with GP practices o Increase patient facing time
GSTTCHS Contract meeting
3
Safeguarding training for all relevant staff in Community services
Monitor exception reporting on Adult Safeguarding training – month 9 reported as 89.6% target 85%.
GSTTCHS Contract meeting
4
Consistency of care for patients with long term conditions
Implement Joint Care Planning CQUIN with District Nurses focused on patients with long term conditions
GSTT unlikely to meet target – commissioners discussing recovery options.
GSTTCHS Contract meeting
5
Community patient survey (n=1075) showed areas for improvement mainly support for self-management, ease of making contact by phone, ease of giving feedback. Quality Alerts at GSTT mainly due to non DN attendance
Community Services provided report on District Nursing services to November CQRG with clear understanding of the issues to be addressed.
Community Services asked to create action plans where level of improvement required was medium or high. Community services moving from annual to near-time feedback.
GSTT CQRG
6
Access to urgent primary care. Although access audit indicated overall levels of access were reasonable, there are imbalances across the week and between practices. Patients complain about difficulties in getting to see a GP and that they find the appointments systems hard to navigate.
Lambeth CCG has included Access to Urgent Primary Care in their GP Delivery Scheme for 2013/14. Practices have completed demand and capacity reports. These reports will be analysed so plans for commissioning urgent access can be discussed at the Primary Care Development Programme Board in February 2014.
Access action plans within primary care to be included in locality development plans, including telephone triage, demand and capacity work.
PCDPB
7
Access to patient test results. Acute and primary care providers do not have shared access to test results done in different settings. This can compromise patient care as well as meaning that tests are duplicated, causing inconvenience and wasting resource.
SLIC programme working on solutions including shared portal, but primary care access to acute test results CCG to consider CQUIN to incentivise faster solution to data sharing
DMI have explored the use of My Health Locker so patients’ can view their test results prior to their clinical appointment.
Lambeth CCG is currently exploring the EMIS function for data sharing and will report to PCDPB.
SLIC programme
board/PCDPB

9
Quality Dashboard – Guy’s and St Thomas’s NHS Foundation Trust
Category Indicator Target Reporting Q1 Q2 Oct Nov Dec Jan Feb Mar S
afe
ty
Mortality: SHMI <1 Quarterly 0.8264 0.8038 0.7791 0.7791 0.7791
SIs: Number of SIs
Monthly 29 17 11 7 5
Number of Never Events 0 Monthly 1 0 0 0 0
Maternity: % women booked before 12 weeks 6 days, 90 Monthly 100 98 114 101 85
Maternity: % Caesarean Section Rate 26 Monthly 33.5 31.6 29.6 27.5 30.4
Maternity: Midwife/birth ratio 1:28 Monthly 1:26.9 1:30 1:29 1:30 1:29.6
CAS Alerts Outstanding 0 Monthly 0 0 0 0 0
Adult Safeguarding: % of staff compliant with training 80 Quarterly 86 88 87 Not
Available 86
Child Safeguarding: % of staff compliant with training –
Level 2 80 Quarterly 83 86 87 86 85
Child Safeguarding: % of staff compliant with training –
Level 3 80 Quarterly 85 87 84 84 83
Falls: Moderate Harm*
Monthly 3 8 6 0 2
Falls: Major Harm*
Monthly 4 1 2 0 0
Falls: Death
Monthly 0 0 0 0 0
Pressure Ulcers, Grade 2
Monthly 121 134 44 37 39
Pressure Ulcers, Grade 3
Monthly 26 54 17 14 11
Pressure Ulcers, Grade 4
Monthly 13 22 7 7 6
VTE Risk Assessments Completed on Admission 95% Quarterly 96.44 96.47 96.17 96.2 96.1
Experie
nce
Complaints: Number of complaints
Monthly 272 224 80 80 46
Complaints: % replied to within agreed timeframe
Monthly 96 94 96 98 96
Friends and Family Test: Net promoter score
Monthly 68 71 74 73 68 Footnote: CQUINs will be reported on quarterly in a separate report. *Falls resulting in fractures have not been reported as serious incidents (major harm) as per STEIS requirements. Information to be
updated for Q4. Fractures resulting from falls for the year are: Q1 = 10; Q2 = 6, Q3 = 6

10
Quality Commentary – Guy’s and St Thomas’s NHS Foundation Trust Changes have been made to the monitoring and management of quality standards for 2013/14 with a move to
monthly Clinical Quality Review (CQRG) meetings to support a more in depth focus on quality. A wealth of
supplementary monitoring information is available through these contractual processes, with the Integrated
Report focusing on performance at provider level for a number of key quality metrics only. It should be noted
that VTE risk assessments are reported on a quarterly basis. A summary of the key issues discussed at the most
recent CQRGs is also included in this section of the Integrated Report.
Mortality
GSTT continue to achieve a better than expected mortality rate and show an improvement on
the previous quarter. Their score of 0.7791 means that the Trust has one of the 10 lowest
SHMIs in the country.
Serious Incidents and Never Events
A total of 5 Serious Incidents required investigation in December these were primarily pressure
ulcers with the exception of one incident relating to a stillbirth of which the report is not yet
due. There were no new never events.
Maternity
12 weeks plus 6 days booking target - the December position is deterioration on the previous
month but is still meeting targets. . However, figures should be viewed in the context of GSTT’s
recording methodology (which differs from other local Trusts. The Trust measures their
compliance with the 12 weeks plus 6 days booking target in line with DH guidance. They have a
target booking number each month based on predicted births in 6 months’ time and hence if
they exceed this target their performance is in excess of 100%. Due to their case mix and
referrals of complex cases from elsewhere, this measurement has been agreed. The Trust’s
overall positive performance in this area may be linked to the fact that they see comparatively
more first time mothers with this group being most likely to respond to messages to book early.
The Caesarean section rate has increased by 3% on the previous month and is marginally higher
than the national target of 27% - noting that the national target does not take in to account the
impact of case mix in Trusts such as GSTT.
Safeguarding
GSTT have maintained consistently good performance in staff training compliance targets for
both adult and children safeguarding training throughout the year.
Adult safeguarding training compliance shows little fluctuation month on month at 86%
December performance remains consistent at 83% of staff trained on level 3 child safeguarding.
Falls and pressure ulcers
11 Grade 3 and 3 Grade 4 pressure ulcers were reported in December. Both figures however
show raw data – it is expected that the majority of these will be de-escalated as they will either
be non-attributable to the Trust or unavoidable. It may also indicate issues with pressure

11
management in the community that may be improved by the pressure ulcer work happening in
South East London.
The number of major falls reported by the Trust for December was 0. However, it was noted in
the Q3 Risk Management Report discussed at the February CQRG that fractures resulting from
falls (which should be reported as a serious incident) differed: Q1 = 10, Q2 = 6, Q3 = 6.
VTE Assessments
The Trust achieved its monthly stretch target for risk assessments carried out on admission -
exceeding 96% each month for Q3
Complaints
206 complaints were received in Q3 2013/14 compared to 223 in Q2 and 265 in Q1.
In Q3 234 complaints were closed.
Of the 234 complaints closed 97% were within the agreed timeframe. It should be noted that
the 97% performance figure cannot be benchmarked against other Trusts as it is based on
GSTT’s method of calculation. The calculation is based on what percentage of complaints
responded to in Q3 were within agreed timeframes rather than a rolling calculation which
would factor in all outstanding complaints. Only 31% of complaints were responded to within
25 working days. The majority of the others had extensions agreed with complainants.
The average response time of 60 working days is not reducing.
A consistent number of complaints are received about patient transport and actions have been
taken to alter the systems and processes to address the issues highlighted in complaints.
The Parliamentary and Health Services Ombudsman (PHSO) have requested complaint files on
two cases for assessment. One was closed and another is in progress. The outcome of four
investigations was notified to the trust - three were not upheld and the fourth was partly
upheld. The issue concerned failure in communication with a family about do not attempt
resuscitation (DNAR) and failure to ensure a call buzzer was within easy reach of the patient.
An action plan has been agreed to address the issues highlighted.
Friends and Family Test (FFT)
GSTT achieved an overall response rate for December of 18.9% (16.1% in A&E and 25.5% in
inpatients), showing continued improvement on previous months. The breakdown of net
promoter scores for December was 61 for A&E and 79 for inpatients, which shows a slight drop
in A&E performance on the previous month and also in the combined score from 73 in
November.to 68 in December.
FFT in maternity for experience during birth response rate is 22.9%. Post natal community and
post natal ward scores are 74 and 30 respectively. Response numbers for post natal ward
experience were a significantly low proportion of eligible women.

12
Clinical Quality Review Group Update - Guy’s and St Thomas’s NHS Foundation Trust Each of the SE London Trusts has now increased the frequency of their Clinical Quality Review Group (CQRG)
meetings to monthly in order to allow for issues relating to the quality of services to be discussed in more
depth. The below summaries give an overview of the areas of discussion at the last CQRG meetings and an
indication of topics due to be discussed at upcoming meetings.
Anti –coagulation Service
CCG Commissioners fed back that there had been a meeting with the Trust and Community
provider team regarding the outstanding quality and safety issues. This resulted in four pages of
actions which to date have yet to be fully implemented. The issues was raised again at the
February 2014 CQRG where it was highlighted that little or no action had been taken at GSTT.
There is a joint provider (GSTT – including community services/KCH) and commissioner
(Lambeth and Southwark) working group meeting to address the concerns. Separately GSTT
have, since the February CQRG, set up an internal group to take action.
Discharge Audit
Clinical Commissioners updated group with results from Southwark discharge audit (which were
almost identical to the audit carried out in Lambeth). The audit was performed over three
consecutive days of discharge in Nov 2013. Main results as follows;
• N=178 letters • 10% paper only • 4% were more than 30 days since patient had been seen • 17% were more than 14 days since the patient had been seen • 80% met all criteria (clear diagnosis, clear management plan with clear follow up) • 20% did not meet one of the above criteria • General points around use of abbreviations and maternity discharges overloaded with data
which makes it hard for GPs to find relevant information.
There is an outstanding action to set up a task and finish group to address quality and
timeliness of discharge summaries. Suggestion to start with A&E and inpatient discharges to
prevent readmissions. There is a timeliness issues with Frail Elderly discharges which also need
addressing.
Cancer presentation - Cancer Patient Experience Survey (CPES): positive and negative highlights
Numbers reported had been screened so that they were just Lambeth & Southwark patients.
The department were surprised with the lack of patient response from dermatology with just
14 respondents. The department uses real time feedback and it was noted that there is a
higher response from the specialities using this real time feedback as well as a difference in the
feedback given e.g., patients report a lack of information being given to them when asked in
‘real time.’ Often when they have time to reflect answers can be different.
Discussion took place regarding Q22 ‘Patient finds it easy to contact their CNS’ which is in
bottom 20%: there is still a query about understanding the time that contact is attempted (as
the CNS may be in clinic, with other patients and are therefore unable to answer their phones

13
at that point). Often patients are calling about ‘simple’ things such as changing appointment
times and this isn’t always appropriate to be via a direct call to CNS. The Trust updated that this
is part of a plan to look at wider multimedia access to free up CNS time to provide emotional
support to patients (rather than administrative tasks). KCH are currently piloting a phone line
manned by admin staff to address this issue – the Trust will wait to see progress from the KCH
pilot before committing to this model.
There was a discussion regarding performance on questions which have been in the bottom
20% for 2/3 years. (Q1) ‘Patient had to see GP once/twice before told to go to hospital’ is a
particular area to address: this relates mainly to gynaecology and upper gastro. The need for
caution was noted with regards to this indicator, as the numbers involved are small. Therefore
the Trust will need to focus on specific specialities rather than whole service.
Patients report feeling unheard about their symptoms – this is reported more in regards to
gynaecology. Action to address this is with Primary Care, who are currently working with
gynaecology.
The Trust has looked at the processes of other Trusts who have reported better results
however they do not appear to be taking any actions that are different from GSTT
Issues around staff recruitment were raised, noting that there are particular problems in
recruiting to Upper GI, head and neck and palliative care. It is also recognised that more
training is required for Practice Nurses.
The Trust has recently started publicising the consultant timetable so patients and family know
when to expect consultant ward rounds and therefore there is an opportunity for questions to
be answered. This is across all tumour groups.
It was recognised that more work needs to be done around the patient’s social needs in light of
indicators moving out of the top 20% from previous years.
In comparison with other London Trusts, GSTT is second only to The Royal Marsden which is a
specialist Cancer Hospital (which scores higher than multi-speciality sites). GSTT are opening a
new Cancer site in 2016 which they anticipate will make a difference. Commissioners
highlighted that it is quite misleading to benchmark with other Trusts as the detail of actual
scores needs to be looked at to make this comparison worthwhile and asked if the Trust will be
prioritising low scores. The Trust confirmed that they will be looking at the impact on individual
patients and using results of planned focus groups and action plans to address these.
Cancer Patient Experience Survey action plans are being used to performance manage
departments. Commissioners requested that these come to Cancer locality meetings as a
standing item and should also remain an update item on the CQRG agenda for oversight.
The Trust was requested to provide percentages on their performance against the standard for
patients to have a Holistic Needs Assessment within 31 days of diagnosis.
End of Treatment Summaries - the aim is for these are to be done during MDT but more work is
required to embed this practice and onto the electronic system. This needs to be agreed,
especially as it will form part a contract requirement.

14
Peer Review Validation - a marked difference was noted between reporting and peer review in
acute oncology and general acute. The Trust believes this is a consistency issue. KCH have the
same pathway and passed whereas GSTT failed and therefore it is not clear why. There was a
discussion regarding a serious concern around the number of Histo-pathologists, as it often
looks like GSTT are failing on the number present at MDT meetings. The Trust confirmed that
Histo-pathologists sit as a group prior to the MDT meeting which works better clinically for
GSTT but doesn’t fit into national recommendation. Commissioners accepted this explanation.
Cancer staging –it was clarified that clarified that ‘staging’ should only be reported at diagnosis
as it is used to determine the stage/progression of cancer. There is currently an issue around
how GSTT capture/report this, as it is only clinically relevant at point of diagnosis – should be
done at MDT meetings for accuracy. Haematology and skin are both expected to be at 80% but
a problem with administration has meant these have not been updated. Colorectal and urology
are two areas to work on. The aim is to achieve above 80% for all tumour groups, the highest in
the cancer alliance. In order to achieve this the Trust will be undertaking a monthly breakdown
per tumour group for a gap analysis and will look at ways that the MDT is working which
doesn’t allow staging to be recorded. As only one team is struggling with this it implies that it
isn’t a system wide issue. There is a 2015 target for staging to be recorded on COSD.
End of Life Care - There is a plan for wider roll out of Trusts alternative approach to the
Liverpool Care Pathway for EOLC. The Trust reported storing additional syringe drivers for KCH
patients to support consistent treatment for Chemotherapy. This improves patient safety as it
reduces prescribing errors by 30% and a similar approach is being sought with PRU and QE
Woolwich Hospitals.
An acute oncology service has been set up for problems post treatment. Patients used to go to
A&E for this so the service has successfully diverted urgent care activity.
Commissioners requested to be updated on progress on achieving best practice pathways. The
Trust confirmed that they are on target for breast and heart and need IT development for risk
assessment follow-up. For prostate there is a plan for discharge into community. No details
available for ovarian and colorectal cancers. It was agreed that the Trust will bring updates on
best practice pathways to locality cancer meetings for identification of priority areas.
CQUINs 2014/15
Subsequent to the CQRG the local 14/15 CQUIN areas agreed are as follows: • Prevention and wellbeing (Alcohol) • Communication and care planning (2-3 year CQUIN to facilitate sharing of care plans and
communications between secondary, community and primary care, and sharing information between health professionals and patients, including access to results)
• Quality and safety (pressure ulcers) • London quality standards (A&E)
Discussion at the CQRG confirmed that CQUINs should not incentivise the Trust for areas that
should already be mainstream particularly around ‘Falls’ which may require a different
approach.
National CQUINs include: NHS Safety Thermometer (focus on pressure ulcers); FFT and Dementia
15
Quality Alerts
The main alerts were in regards to discharge timeliness and quality, difficulties in making
follow-up appointments and provision of care by District Nurses. No reverse QAs were
reported.
SIs/Never Events, Complaints and NICE compliance
Detail on individual SI’s are covered in the SI meeting. The next report with an overview of SIs
and complaints is due at the March CQRG meeting.
The NICE compliance report was circulated with no major issues for discussion.
CQC Reports
There has been no change since last meeting. Action is still on-going regarding patient transfer
to Kent.
Performance Report
There was a discussion about the use of the performance scorecard in future – as many of the
indicators require commentary to explain current status. Some of the indicators do not match
other data reporting and will require triangulation to address this.
The performance scorecard was discussed at the February CQRG. The Trust was requested to
provide an appropriate narrative alongside the scorecard.

16
4.3 King’s College Hospital NHS Foundation Trust
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
Maternity: high numbers of women not receiving
antenatal assessment by the end of 12th
week in
pregnancy although there is improvement with
November performance at 76.6%.
Caesarian section rate is slightly above November
target of 26% at 27%.
Ongoing issue about capacity constraints leading
to lack of choice of pathway in birth and disjointed
experience in labour due to space constraints on
labour ward and need to move women between
rooms/areas.
Trust developed action plan encouraging earlier patient booking,
with CCG support. Trust to write out to GPs outlining importance
of encouraging earlier booking. Communication materials to be
revived.
Midwifery led rooms opened early December. Other changes to
use of space being made to improve maternal experience
CQRG
2
Patient Experience:
Many Patient Experience indicators saw
deterioration in Quarter 2. Numbers of complaints
and PALS activity at KCH rose, and response rates
remain below target. “How are We Doing” patient
survey in-patient results have been below target
for two out of the three months, though the
outpatient score achieved or exceeded benchmark
in 2 of the 3 months.
Friends and Family Test (FFT) survey results for
King’s Denmark Hill for Q2 were also disappointing
with average score out of 100 for inpatients of 62,
61 and 62, and 32, 43 and 40 for emergency
patients. Response rates in the Emergency
Department remain a challenge. FFT for maternity
was also launched on both Denmark Hill and the
PRUH sites on 1st October.
Themes from complaints investigated in Dec CQRG agenda.
CCG undertaking deep dive into patient experience data to look
into trends and underlying causes.
KCH not meeting emergency waiting times standards and there is
pressure on bed capacity, and these pressures will impact on
patient experience. Trust action plan for ‘red shifts’. Emergency
capacity being addressed through variety of actions, including
additional capacity, redesign of emergency pathway etc.
Further investigation into problem wards where F&F scores are
particularly low. CCG site visits in planning stage, target these
wards
CQRG
3
Complaints
258 complaints received in Q3 – increase from Q2
(208). Broken down to 182 (Denmark Hill site)
76(PRU/other). 60% relate to inpatient care and
40% outpatients (including ED). Response rates at
47% DH and 35% PRU/other. Seven complaints
were referred to the NHS Health Service
Ombudsman for independent review.
Analysis of complaints by subject matter and ward incorporated
into Francis work was reported to CQRG in December and
February. Cancellations of surgery and waiting times are a major
theme, linked to capacity constraints and problems in meeting 18
week RTT targets. Staff attitude another theme.
There are a high rate of complaints related to renal, liver and
surgery services and a 50% increase in the number of gynaecology
complaints.
KCH have reviewed findings of the Clywd report and made some
immediate changes. A NED has been appointed as Patient
Experience Champion, and the style of complaint response has
been changed to a more succinct letter with a table of actions
taken. KCH are considering introducing a Serious Complaint
Committee, parallel to their Serious Incident Committee.
Complaints are shared with department staff where issue
occurred, as part of learning from direct feedback.
Trust requested to provide plan for improving response times and
CQRG
17
is reconfiguring complaints service following PRUH acquisition; a
PALS service has been established at the PRUH.
4
Serious Incidents and Never Events
23 serious incidents reported December 2013 and
1 Never Event (wrong site surgery involving
removal of a wrong tooth). Incidents involving
major harm/ death less than 1% total reported for
PRUH and Denmark Hill.
Serious incidents at PRUH likely to be understated
in the data.
The Trust established a workstream looking at implementation of
surgical checklist which reported to November CQRG. Audits of
surgical divisions has led to range of actions, including learning
sessions, rationalisation of checklists, mandate to theatre nurses
to enforce completion of checklists. Further report to CQRG in
2014.
Additional meetings being set up to clear backlog of Sis at PRUH.
These are currently being uploaded onto STEIS and therefore
numbers will increase.
KCH reported to the CQRG about their project underway to
address failure to address deteriorating patients.
CQRG
5 Falls and pressure ulcers
Increase in grade 3 and 4 pressure ulcers Q3.
Actions being implemented to reduce incidence of pressure ulcers
include: specialist tissue viability nurses commencing at PRUH;
staff awareness event; Safer Care Forum set up to review pressure
ulcer root cause analyses (RCA)
Analysis of serious falls RCAs has identified lack of 1:1 nursing for
patients at high risk of falls. This is being addressed by an increase
in establishment of the Falls Team. Falls risk assessments and care
planning sometimes incomplete or inaccurate. This document is
currently under review to ensure consistency across both sites.
CQRG
6
Adult Safeguarding
Staff uptake of safeguarding training remains low
at 54% for level 2 training (target 80%). This
indicates that staff may not be aware of
safeguarding issues. Requirement of OFSTED visit
that this is improved.
Issue has been discussed several times at CQRG, but there has
been no improvement. CCG to write to Trust requesting
improvement.
CQRG

18
Quality Dashboard – King’s College Hospital NHS Foundation Trust (Denmark Hill site)
Fig 1. Quality Dashboard
Footnote : CQUINs will be reported on quarterly in a separate report . * Data has not been validated.
Indicator Target Reporting Q1 Q2 Oct Nov Dec Jan Feb Mar Mortality: SHMI <1 Quarterly 0.9255 0.9146 0.8629 0.8629 0.8629
SIs: Number of SIs
Monthly 25 35 17 12 10
Number of Never Events 0 Monthly 2 0 1 2 1
Maternity: % women booked before 12 weeks 6 days, 90 Monthly 72.7 75.1 71.0 76.6 78.6
Maternity: % Caesarean Section Rate 26 Monthly 26.5 25.8 24.6 27.0 26.5
Maternity: Midwife/birth ratio 1:28 Monthly 1:26 1:28 1:29 1:28 1:28
CAS Alerts Outstanding 0 Monthly 1 1 1 1 1
Adult Safeguarding: % of staff compliant with training 80 Quarterly
Not available 50% 55% 55% 56%
Child Safeguarding: % of staff compliant with training – Level 2 80 Quarterly 74 71% 73% 73% 74%
Child Safeguarding: % of staff compliant with training – Level 3 80 Quarterly 76 79% 79% 82% 78%
Falls: Moderate Harm
Monthly 4 2 4 1 3
Falls: Major Harm
Monthly 1 8 2 1 2
Falls: Death
Monthly 0 0 0 0 0
Pressure Ulcers, Grade 2 - NHS Safety Thermometer
Monthly 93 101 35 67 50
Pressure Ulcers, Grade 3
Monthly 10 27 3 16 11
Pressure Ulcers, Grade 4
Monthly 6 8 5 8 4
VTE Risk Assessments Completed on Admission 95% Quarterly 97.79 98.46 98.47 99.01 98.88
Complaints: Number of complaints
Monthly 202 208 59 73
Not available
Complaints: % replied to within agreed timeframe
Monthly 54.5 54.4
Not
available 29 Not
available
Friends and Family Test: Net promoter score
Monthly 51 49 55 54 56

19
Quality Dashboard – King’s College Hospital NHS Foundation Trust (PRU site)
Category Indicator Target Reporting Oct Nov Dec Jan Feb Mar S
afe
ty
Mortality: SHMI <1 Quarterly N/A N/A N/A
SIs: Number of SIs
Monthly 5 7 2
Number of Never Events 0 Monthly 1 0 0
Maternity: % women booked before 12 weeks 6 days, 90 Monthly Not
available Not available Not available
Maternity: % Caesarean Section Rate 26 Monthly Not
available Not available Not available
Maternity: Midwife/birth ratio 1:28 Monthly Not
available Not available Not available
CAS Alerts Outstanding 0 Monthly 0 0 0
Adult Safeguarding: % of staff compliant with training 80 Quarterly N/A Not available Not available
Child Safeguarding: %of staff compliant with training – Level 2 80 Quarterly N/A Not available Not available
Child Safeguarding: %of staff compliant with training – Level 3 80 Quarterly N/A Not available Not available
Falls: Moderate Harm
Monthly 2 4 1
Falls: Major Harm
Monthly 1 1 0
Falls: Death
Monthly 1 0 0
Pressure Ulcers, Grade 2 - NHS Safety Thermometer
Monthly
Not
available 10 27
Pressure Ulcers, Grade 3
Monthly
Not available 3 1
Pressure Ulcers, Grade 4
Monthly
Not available 0 0
VTE Risk Assessments Completed on Admission 95% Quarterly N/A N/A N/A
Experie
nce
Complaints: Number of complaints
Monthly 30 22 Not available
Complaint responses ≥ 25 working days
Monthly 15 21 Not available
Friends and Family Test: Net promoter score
Monthly Not
available Not available Not available Footnote: CQUINs will be reported on quarterly in a separate report

20
Quality Commentary – King’s College Hospital NHS Foundation
Trust reconfigurations as a result of TSA recommendations were fully implemented in October 2013 and (where
available) quality data has been reported on a site basis. Monthly CQRGs continue to provide a Trust wide
overview of quality issues. The Integrated Report focusses on performance at provider level for a number of key
quality metrics only. It should be noted that VTE risk assessment performance is reported and assessed on a
quarterly basis. A summary of the key issues discussed at the most recent CQRGs is also included in this section of
the Integrated Report.
Mortality
SHMI scores are reported on a Trust wide basis and cover a whole quarter, therefore once both
Trust site’s data are combined the position may differ by the end of the quarter. On a Trust basis
KCH had better SHMI scores than SLHT – however it is not possible to disaggregate the SLHT SHMI
on a site basis. Denmark Hill site shows an improved SHMI score on the previous 2 quarters.
Serious Incidents and Never Events
12 Serious Incidents were reported in December and 1 Never Event. The never events was a
wrong site surgery in Dental where the wrong tooth was extracted
Incidents involving major harm/death were less than 1% of total incidents reported at both the
PRUH and Denmark Hill
Serious incidents at the PRUH site are likely to be understated in the data, as currently under
investigation pressure ulcer SIs are still being uploaded on to STEIS – more accurate data will be
available after the end of the quarter.
CAS Alerts
Denmark Hill site currently has one safety alert outstanding relating to implementation of safer
spinal and epidural devices. The Trust is currently piloting these new devices and progress is being
monitored by the Patient Safety Committee.
Maternity
Early booking performance against the 12 week, 6 day 90% booking target has shown positive
improvement with November performance at 76.6%. However, as previously reported these
figures are unadjusted and do not take into account the number of referrals of women who are
already more than 13 weeks into their pregnancy.
The Caesarean section rate is slightly over the target of 26% for November at 27% which has been
the highest rate year to date (YTD).
Safeguarding
KCH undertakes real time reporting of safeguarding compliance. Figures stated are the Trust
position at the time of writing this report.
Compliance with Adult and Children’s safeguarding training is still falling significantly short of the
required targets. Current performance is largely static on the previous month for Denmark Hill.

21
Trust reporting systems were unable to establish a position for staff based at PRUH in time for
this report.
Falls and pressure ulcers
There has been an increase in grade 3/4 pressure ulcers, including those which were considered
avoidable. Actions being implemented to reduce incidence of pressure ulcers include:
Specialist tissue viability nurses commencing at the PRUH who will be working to reduce
pressure ulcer incidence there and ensure that grade 2 pressure ulcers do not develop
into grade 3/ 4s
A pressure ulcer awareness event for staff is being held to raise awareness of Pus
A Safer Care Forum has been setup which will review pressure ulcer RCAs to ensure that
actions are being implemented to reduce pressure ulcer incidence.
Pilot work being done on 2 wards around nursing culture and decision making and how
“hearts and minds” can be captured to ensure zero-harm care delivered
5 serious falls were reported at Denmark Hill in the quarter (3 fractured neck of femurs; 1 sub-
dural bleed; 1 fractured right trochanter)
3 serious falls reported ta the PRUH (2 fractured neck of femurs and 1 sub-dural bleed resulting
in death)
An analysis of root cause root causes of serious falls has highlighted the following common
factors:
A lack of availability of 1:1 nursing for patients assessed at high risk of falls - which is
being addressed by an increase in establishment of the Falls Team across the whole
organisation
Falls risk assessments & care planning sometimes incomplete or inaccurate - falls risk
assessment documentation is being reviewed to ensure consistency in approach between
sites
Complaints
The number of complaints received at KCH continues to fluctuate and shows a marked increase at
Denmark Hill but a decrease at PRUH on the previous month. Trust responsiveness within agreed
timescales is poor across both sites and is subject to an improvement plan.
258 complaints received in Q3, which is an increase from Q2 (208). Broken down to 182 Denmark
Hill site and 76 PRU/other sites. Response rates were 47% DH and 35% PRU/other.
60% of complaints relate to inpatient care while 40% relate to outpatients (including ED).
Outpatient complaints have reduced for a consecutive quarter.
7 complaints were referred to the Health Service Ombudsman for independent review. The Trust
has been advised of 3 investigations and 4 cases were closed after assessment. In Q3
Outpatient complaints fell to its lowest level YTD.

22
Proportionally the number of complaints to actual patient activity is reducing.
The ratio of inpatient complaints to activity remain static despite increasing activity
Trends at the PRUH:
74 legacy cases transferred to King’s in October 2013, of which 17 complaints remain open and 2
resolution meetings are scheduled.
Of the complaints received in the Qtr 3, (24) relate to services, treatment and care provided since
October 2013; of these 6 concern care provided by the Accident & Emergency Department
Friends and Family Test (FFT)
The KCH December combined response rate shows marked improvement on the previous month
at 15.2%. However response rates at PRUH site are poor in both A&E and Inpatients at 8.6% and
8.5% respectively. An FFT action plan has been developed for PRUH to address the performance
issues there.
KCH overall net promoter scores have been largely consistent YTD. The Trust continues to trial
new methods to increase participation. The breakdown of net promoter December scores was 51
for A&E and 62 for inpatients which is similar to the previous month.
FFT in Maternity for experience during birth response rates have shown positive progress at
13.4% in Denmark Hill and 10.9% at PRUH. Post natal Community and Post natal ward scores are
100 and 30 respectively. These scores are the result of very low numbers of eligible women being
surveyed.

23
Clinical Quality Review Group Update – King’s College Hospital NHS Foundation Trust
Mental Capacity Act and Learning Disability SAF
The KCH LD Lead is providing alerts to the community LD team if a client with LD attends A&E
and/or is admitted and the team are starting some work to review these admissions to see if with
a different approach admission could have been prevented. She is also having discussions with
the Community LD team and the Southwark GP Clinic Lead for LD on support to Primary Care in
flagging LD needs on referral letters.
Emergency pathway
A mobile CDU unit started at Denmark Hill on 30th Dec and another will open at PRUH in the first
week of Feb.
Transition issues
A&E – Impact of current performance on patient experience, safety and outcomes
Commissioners made a further explicit request for a written brief from KCH on the impact of
current A&E performance on patients rather than oral feedback. KCH reps reflected the difficult
timing of the meeting in terms of producing a brief which would be very soon superseded and
noted that a full discussion in Feb should provide better assurance
SI reporting - It was noted that SIs reported as part of the A&E performance at PRUH were graded
as moderate, although the numbers reported had increased. The Trust has acknowledged
uncertainty in the robustness of information collected before acquisition in October.
Commissioners were keen to get a better understanding of the type of incident being reported -
the main problem areas are pressure ulcers from the community and the Pathology service to
A&E. It was agreed more in-depth analysis was required, and could be picked up via the PRUH
Quality sub-group.
Quality Alerts
Bromley, Southwark and Lambeth CCGs had met to progress consistency in the QA process. The meeting
demonstrated that all the CCGs had somewhat different QA systems in place, although there were also many
points of similarity. It was agreed that discussions now need to include KCH. The Trust has identified a lead for
Quality Alerts.
Mental Capacity Act & Learning Disabilities SAF - it was recognised that there was a need for
commissioners and Trust to discuss an effective approach to flagging LD community patients. Also
more development was needed with General Practice and Community teams. Commissioners
requested a Trust update for the January CQRG to also cover reporting.
Adult Safeguarding - commissioners requested clarification on the KCH Trust action plan for
improving performance and promoting training as no update on the KCH action plan had been
received

24
Key Quality Alert themes:
• Choose & Book - this is a CQUIN for 13/14 which is helping to address poor DoS/ DB performance.
• Quality and timeliness of written communications sent by the Trust to practices - work has started with
the PRUH to identify root causes and Trust consultants wish to review the discharge process. The Trust is
willing to work with practices on this.
• Correspondence addressed to the incorrect GP practice - the Trust acknowledged that this has been an
issue for a long time and there are a number of causes. The Outpatient Appointments teams should be
checking they have the right address as well as checking this face to face with the patient. A&E is proving
more difficult. KCH is aware that the Consultants’ secretaries are not always using the right data base and
this is recognised as a hospital wide system issue. All returned letters are coming back to the data team to
correct them. The Trust recognised this as a serious governance challenge for both KCH and PRUH.
M8 Performance report
A&E (Emergency Department) - performance was a key issue and that this had not changed
significantly since November. In early January there had been seventeen 12 hour trolley breaches
that had prompted another visit by NHSE and the CQC. Commissioners noted this as a key area to
keep under review. Bromley CCG/KCH to meet in early January for a PRUH-specific meeting to
look at emerging Quality issues, as well as addressing any outstanding handover issues.
Immediate actions agreed by KCH with NHSE & CQC to improve performance were to go out by
letter to CEOs of the CCGs.
The Trust CEO has written to CCGs regarding both sites. The Trust updated on the following key
actions being undertaken:
• PRUH: Opened PIU to provide extra capacity and had the potential to open another 6 beds if needed
• Day surgery at Orpington: a “drop in” Day Surgery theatre will be opened to free up more surgical beds
• Additional staff are being recruited including matrons and consultants for ED • Performance Manager role in ED at Denmark Hill will be replicated at the PRUH • Delayed discharges are being reviewed as an opportunity for improvement • CDU – will be opened on early February • Urgent Care Centre is to become 24/7
Repatriation - the repatriation of patients to their originating hospital caused delayed discharges
MRSA - It was noted that there have been two MRSA cases in December 2013 at KCH and CDiff
has gone over its planned trajectory. However, it was not the Trusts’ belief that this was
indicative of any overall breakdown in the system. They did however acknowledge that there
were potentially issues around cleaning and the process for sample testing needed to be
improved. Commissioners requested to see learning coming out of the Root Cause Analysis (RCAs)
for these cases. It was agreed that lessons learnt would be brought back to CQRG.
There had been four CDiff cases at the PRUH but this is within trajectory. An Infection Control
Card at ward level is being introduced.
Never Events – Commissioners requested timescales for reporting on the Dental episode (wrong
tooth extraction). The Trust will be reviewing the use of surgical check lists later in the year.

25
4.4 South London & Maudsley NHS Foundation Trust
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
Numbers of patient’s receiving physical health checks
SLaM required to perform physical health checks on all new admissions and additional tests on patients receiving anti-psychotic medication as part of 2013/14 CQUIN.
Baseline at Q1 for new admission is 22% and for those who receive antipsychotic medication is 56% has been established. Q2 targets for both indicators are 40% and 60% respectively. SLaM achieved both Q2 targets – for new admissions they achieved 66% and for those already receiving antipsychotic medication they achieved 83% (BW). In Q3 the target for new admissions was 50% - SLaM achieved 78%. In relation to users receiving antipsychotic medication the target at Q3 was 70% - SLaM achieved 100%. SLaM has responded well to this CQUIN.
LSLC (4- borough)
2
Quality of patients assessment and triage, Primary Care access to Assessment Service and demand for in-patient beds
In response to the mixed quality of provision and fragmented assessment process Lambeth’s Living Well Collaborative has developed a service offer which seeks to develop a front end assessment function that intends to integrate primary care, social care, and voluntary sector into a coordinated hub that acts as a gateway to secondary mental health services.
A coordinated hub that integrates key assessment functions will potentially better manage demand into Lambeth’s inpatient services which are presently struggling to meet local demand as well as provide a coordinated and transparent approach to bed management, delivery of treatment interventions, and discharge into the community.
Lambeth CCG
3
Dementia assessment’s needed to be carried out in 2013/14 to achieve national target
Patients over the age of 65 on anti-psychotic medication without a dementia assessment identified as key group to target and will be raised with individual practices. PLT event held in January 2014
Review of current memory service pathway and capacity to meet increase in demand as a result of dementia CQUIN and raising awareness work carried out by Clinical Lead for Dementia with low referring practices.
Lambeth and Southwark CCG
4
Numbers of patients receiving copies of their care plans and GPs experience of referral process
The Easy In / Easy Out CQUIN aims to increase the number of users who when discharged who have a Discharge Summary comprising of discharge and crisis support elements from the over-arching Recovery and Support Plan sent to their GP within 7 working days.
SLaM will also work to improve response rate to GP questionnaires and develop action plan to identify how they will improve GP satisfaction
This CQUIN is linked to the 2013/14 Lambeth Living Well Collaborative initiative which established the community options service which aims to provide effective support to patients discharged from secondary to primary care identifying the necessary support provision that will enable them to be effectively managed within primary care.
LSLC

26
5
Improve quality of talking therapies service inadequate
Review of first six months of Integrated Talking Therapy Service has been successfully undertaken and findings to be presented to the LCCB. The overall findings of the evaluation were positive and the integrated service model has improved the access and quality of talking therapy services in Lambeth. It is proposed that a development plan be implemented to build on the good work undertaken so far. The implementation plan will be monitored via the stakeholder board. It is proposed that 2014/15 CQUIN schemes that align specifically with developments detailed in the implementation plan will be agreed with the provider. It is anticipated that CQUINs will focus on BME experience of service provision and access to post treatment support groups.
Lambeth CCG
6
Southwark CCG note that the quality of Serious Incident reports received from SLaM are often poor with many not clearly identifying the Root Causes of the issue, and consequent recommendation/actions to address. Southwark CCG has raised this with SLaM who acknowledged the issue.
Southwark CCG raised this with the SLaM patient safety team and clinicians at the SI meeting. The new Patient Safety lead in post at SLaM has reviewed their processes.
Lambeth SI meetings have continued to monitor effectively both Serious Incident report completion within 45 and 60 day deadline, the quality of the reports as well as the successful implementation of action plans. Serious incidents meetings are held involving relevant clinicians.
A meeting involving all four CCGs (LSLC) and SLaM is to be held in February to discuss this issue.
SLaM SI meetings

27
Quality Dashboard – South London and Maudsley NHS Foundation Trust
Category Indicator Reporting Period
Target Jul Aug Sept Oct Nov Dec Data source
Safe
ty
Mortality: SHMI* / HSMR Quarterly <1 HSCIC
SIs: Number of SIs reported [TOTAL Lambeth SIs] Monthly 29 (April –
Sept) 2 0 5 STEIS
Number of Never Events Monthly 0 0 0 0 0 0 0 STEIS
CAS Alerts Outstanding Monthly 0 0 0 NPSA
Adult Safeguarding: % of staff compliant with training Quarterly 68% 76% TBC
Child Safeguarding: %of staff compliant with training – Level 2 Quarterly 60% 96% TBC
Child Safeguarding: %of staff compliant with training – Level 3 Quarterly N/A 88% TBC
Exp
eri
en
ce
Complaints: Number of complaints Monthly 11 7 7 11 13 30 Trust Data
Complaints: % replied to within 25 days Monthly - - - - - - Trust Data
Clin
ical
Eff
ecti
ven
ess
inp
atie
nts
Delayed Discharge/Transfer of Care Target(s) set for the number of patients delayed in their discharge of care, as well as the number of OBDs lost due to delayed discharge
Monthly 0 discharge
delays or days lost
268 269 261 269 300 289 Trust Data
Acute Overspill Target(s) set for number of acute overspill placements and the total number of acute overspill OBDs
Monthly 0 overspill
placements or days lost
18 11 15 30 26 27 Trust Data
Readmissions [M1-M6 13/14 total 44 readmissions] Number of patients readmitted to inpatient services with 28 days of discharge
Monthly 9 9 13 7 3 2 Trust Data
Physical Health Number of AMH and MHOA new admissions who have received PH checks on admission.
Quarterly Q2 40% Q3 50% Q4 75%
83% 78% CQUIN
Physical Health Those on medication who have received PH checks within four months
Quarterly Q2 60% Q3 70% Q4 85%
66% 100% CQUIN

28
C
linic
al E
ffec
tive
nes
s C
om
mu
nit
y
Seven day discharge follow-ups Proportion of users on CPA discharged who are seen within 7 days
Monthly 95% 100% 100% 100% 95% 94% 97% Trust Data
Recovery and support plans % of AMH CPA caseload who have support and recovery plans.
Quarterly 55% Q2 24% Q3 33% CQUIN
Peer Supporters Proportion of service users on SLaM caseload who are peer supporters
Ad hoc TBC
Q2 no peer
supporters
recorded
TBC Trust Data
Discharge from secondary to primary care % users on CPA last six months discharged with discharge planning documentation which includes early warning signs, crisis plans etc.
Quarterly 50%
N/A 20% CQUIN
Discharge from secondary to primary care % patients to which a discharge letter has been sent to their GP within 1 week of discharge
Monthly 95%
Q1 = 71% Q2 = 70% 99% 98% 96% Trust Data
Personal health budget Proportion of users on CPA who have a personal health budget
TBC TBC
Sept 2013
baseline c110 TBC Trust Data

29
Quality Commentary – South London and Maudsley Hospital NHS Foundation Trust
Serious Incidents and Never Events
29 Serious Incidents were reported on the national STEIS system for the first 6 months of 2013/14
for all residents. There were no Never Events. The Trust reviews Lambeth resident serious
incidents (SI) with governance and clinical leads at Lambeth CCG. SI trends were discussed in the
first 4-borough clinical quality review meeting on 13th December 2013.
CAS Alerts
Of 97 alerts issued between 1 April 2013 and 30 September 2013 the majority were completed on
time (60% DH Estate Alerts and 70% MHRA Alerts). There are no Alerts currently outstanding.
Clinical Effectiveness Data:
Peer Supporters
Higher numbers were previously reported under CQUIN because they were not limited to the
positions directly supervised by Trust staff with responsibility for the activity concerned, or to activity
that was funded by the Maudsley Charity to be carried out by a partner organisation for the benefit of
SLaM service users. A report prepared for Q3 highlights this where in Lambeth there are no peer
supporter positions directly being provided by SLaM. While this is the case, SLaM supports the
borough wide initiative to develop peer support which is directly provided in Lambeth by the
voluntary sector.
Discharge from secondary to primary care
Currently this report is based on a monthly % of patients to which a discharge letter has been sent to
their GP within 1 week of discharge but should be replaced in time by a CQUIN indicator that aims to
have more recovery focussed on crisis planning documentation being sent to GPs when users transfer
from secondary care. An audit into the quality of discharge plans at Q3 highlighted areas of
improvement which SLaM are actively working on to improve the quality of discharge plan
documentation, by ensuring that all key sections are completed.
Clinical Quality Review Meetings
The first 4-borough clinical quality review meeting took place Friday 13th December. Lewisham CCG is
managing the administration of these. More detailed quality information will be included in
subsequent Quality Reports.
Delayed Discharge/Transfer of Care
This metric has decreased over the past 12 month (476 April 2013 and 328 July 2013). It is a whole-
system issue including an impact to social care funding. The primary care incentive scheme for 2014-
15 aims to incentivise GPs to effectively manage patients discharged from SLaM services to primary
care. This also links into a CQUIN relating to the % of users on CPA in the last six months discharged
with a comprehensive care plan.
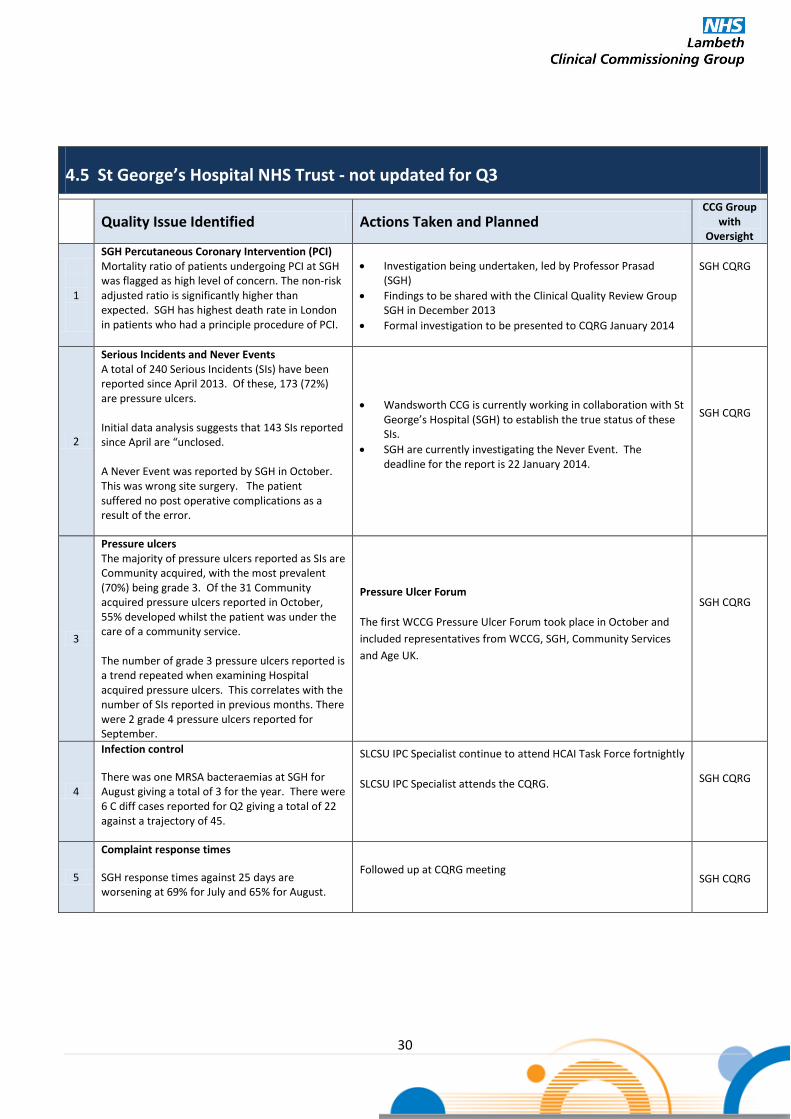
30
4.5 St George’s Hospital NHS Trust - not updated for Q3
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
SGH Percutaneous Coronary Intervention (PCI) Mortality ratio of patients undergoing PCI at SGH was flagged as high level of concern. The non-risk adjusted ratio is significantly higher than expected. SGH has highest death rate in London in patients who had a principle procedure of PCI.
Investigation being undertaken, led by Professor Prasad (SGH)
Findings to be shared with the Clinical Quality Review Group SGH in December 2013
Formal investigation to be presented to CQRG January 2014
SGH CQRG
2
Serious Incidents and Never Events A total of 240 Serious Incidents (SIs) have been reported since April 2013. Of these, 173 (72%) are pressure ulcers. Initial data analysis suggests that 143 SIs reported since April are “unclosed. A Never Event was reported by SGH in October. This was wrong site surgery. The patient suffered no post operative complications as a result of the error.
Wandsworth CCG is currently working in collaboration with St George’s Hospital (SGH) to establish the true status of these SIs.
SGH are currently investigating the Never Event. The deadline for the report is 22 January 2014.
SGH CQRG
3
Pressure ulcers The majority of pressure ulcers reported as SIs are Community acquired, with the most prevalent (70%) being grade 3. Of the 31 Community acquired pressure ulcers reported in October, 55% developed whilst the patient was under the care of a community service. The number of grade 3 pressure ulcers reported is a trend repeated when examining Hospital acquired pressure ulcers. This correlates with the number of SIs reported in previous months. There were 2 grade 4 pressure ulcers reported for September.
Pressure Ulcer Forum
The first WCCG Pressure Ulcer Forum took place in October and
included representatives from WCCG, SGH, Community Services
and Age UK.
SGH CQRG
4
Infection control
There was one MRSA bacteraemias at SGH for August giving a total of 3 for the year. There were 6 C diff cases reported for Q2 giving a total of 22 against a trajectory of 45.
SLCSU IPC Specialist continue to attend HCAI Task Force fortnightly
SLCSU IPC Specialist attends the CQRG.
SGH CQRG
5
Complaint response times
SGH response times against 25 days are worsening at 69% for July and 65% for August.
Followed up at CQRG meeting
SGH CQRG

31
Quality Dashboard – St George’s Hospital NHS Trust
Fig 3. Quality Dashboard *Data has Figure 3 Quality Dashboards *Data has not yet been validated. CQUINS will be reported on a quarterly basis in a separate report

32
Quality Commentary – St Georges Hospital NHS Trust
CQC Visit
The Trust had a CQC inspection on Monday 10th February, and are expecting an unannounced visit
in the two weeks following this.
Healthcare Acquired Infections
C-Difficile: There was 1 additional C.Diff case in January, with a total of 27 total cases.
MRSA: There have been 9 cases of MRSA to date.
Complaints
52% of complaints in December were responded to within 25 days, compared to 61% in
November.
Pressure Ulcers
There were a total of 7 Grade 3 & 4 pressure ulcers in January. In Quarter 1 there were 41 Grade
3 & 4 pressure ulcers compared to 29 in Quarter 2. The total for Quarter 3 is 25.
CQUINs
The Q1 CQUIN amount has been agreed as part of the Q1 reconciliation. The Trust achieved
£993k worth of CQUINs against a maximum value of £1040k .
CQUINs with a Q2 target achieved - Acute:
NHS Safety Thermometer – Submit a complete survey to the information centre VTE Root Cause Analysis – RCA initiated for 90% of HAT, 70% of RCA completed with
consultant report. (Don’t receive payment due to failure of VTE assessment) End of Life Ongoing Education – Description of education programme and course content. End of Life Extension of CMC or equivalent – Provide agreed data on CMC patients and
number of patients placed on CMC. Alcohol Misuse – Targeted screening of inpatients, 60% A&E, 90% Allingham, 77%
Richmond, baseline for Holdsworth & Gunning Ward and Pre-op patients. Alcohol Misuse – Development of improvement programme. Alcohol Misuse – 60% of all relevant information communicated to GPs Smoking cessation – Recruitment of 2 WTE CNS. Maternity Midwife ratio – Achieve a ratio of 1:27 Maternity supernumerary midwife cover 24hrs, 7 days – 96% cover Maternity Consultant Cover – 98 hours per week cover for Q1 COPD Development of the tiered model – Agree the clinical parameters for the tiered
model COPD Admissions – Identify the % who have respiratory specialist input and the % under
care of respiratory specialist.
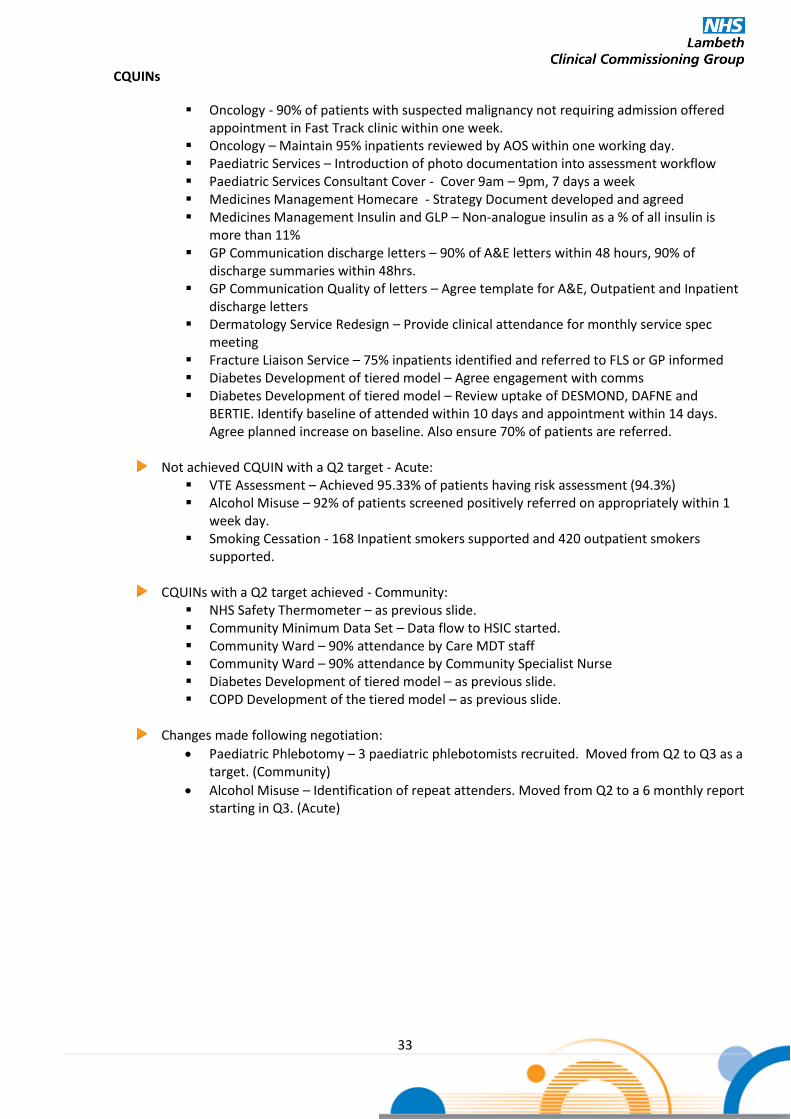
33
CQUINs
Oncology - 90% of patients with suspected malignancy not requiring admission offered appointment in Fast Track clinic within one week.
Oncology – Maintain 95% inpatients reviewed by AOS within one working day. Paediatric Services – Introduction of photo documentation into assessment workflow Paediatric Services Consultant Cover - Cover 9am – 9pm, 7 days a week Medicines Management Homecare - Strategy Document developed and agreed Medicines Management Insulin and GLP – Non-analogue insulin as a % of all insulin is
more than 11% GP Communication discharge letters – 90% of A&E letters within 48 hours, 90% of
discharge summaries within 48hrs. GP Communication Quality of letters – Agree template for A&E, Outpatient and Inpatient
discharge letters Dermatology Service Redesign – Provide clinical attendance for monthly service spec
meeting Fracture Liaison Service – 75% inpatients identified and referred to FLS or GP informed Diabetes Development of tiered model – Agree engagement with comms Diabetes Development of tiered model – Review uptake of DESMOND, DAFNE and
BERTIE. Identify baseline of attended within 10 days and appointment within 14 days. Agree planned increase on baseline. Also ensure 70% of patients are referred.
Not achieved CQUIN with a Q2 target - Acute: VTE Assessment – Achieved 95.33% of patients having risk assessment (94.3%) Alcohol Misuse – 92% of patients screened positively referred on appropriately within 1
week day. Smoking Cessation - 168 Inpatient smokers supported and 420 outpatient smokers
supported.
CQUINs with a Q2 target achieved - Community: NHS Safety Thermometer – as previous slide. Community Minimum Data Set – Data flow to HSIC started. Community Ward – 90% attendance by Care MDT staff Community Ward – 90% attendance by Community Specialist Nurse Diabetes Development of tiered model – as previous slide. COPD Development of the tiered model – as previous slide.
Changes made following negotiation:
Paediatric Phlebotomy – 3 paediatric phlebotomists recruited. Moved from Q2 to Q3 as a target. (Community)
Alcohol Misuse – Identification of repeat attenders. Moved from Q2 to a 6 monthly report starting in Q3. (Acute)

34
Clinical Quality Review Group Update St George’ Healthcare NHS Trust
OOH Surgery Cover
In response to a Junior Doctor Survey comment questioning the safety of cover at night for
surgery, an overview of the Trust’s out of hours surgery cover arrangements was given; out of
hours cover is from 8pm – 8am on weekdays, and is 24 hours a day on the weekends.
The Trust’s current arrangements involving Advance Nurse Practitioners (ANPs) and Specialist
Advanced Nurse Practitioners (SNAPs) are the result of ongoing work by the Trust to ensure the
safe replacement of the historical system in which Junior Doctors would work out of hours.
Out of hours mortality data to be discussed at the February CQRM.
Paediatric Oncology Update
The paediatric oncology action plan under discussion was developed in response to a clinical
incident in 2010 involving SGH, Kingston Hospital (KHT) and Royal Marsden (RMH) in which a
patient died.
The delay in declaring the incident as an SI (declared in 2013) was due to declaration taking place
following that of the other two involved Trusts, who had been more involved with the patient’s
care than SGH.
It was shared that as a result of the incident:
Antibiotics are administered within 2 hours of admission
Early Warning System and escalation protocols were reviewed
Paediatrics training took place
The suitability of the interaction between Paediatric Oncology Shared Care Units (POSCU) and
Primary Treatment Centres (PTC) within the Specialised Children’s Networks (SCN) model was
discussed.
An updated action plan is to be shared for information at the February CQRM.
Cancer 62 Day Breaches
November performance was under the 85% target at 80.8%.
Following a reallocation due to late referrals by Croydon and Kingston Hospitals, performance
was slightly increased although still below target at 83.1% in accordance with the London Cancer
Alliance protocol.
Urology TWR clinic patients attending Queen Mary’s Roehampton (QMR) will have an MRI at
QMR in the same week, in order to avoid delays at the SGH site.
A report will be presented at the February CQRM.
Serious Incidents
Three closure reports were discussed, regarding a delayed diagnosis, breach of patient
confidentiality and a patient death following a fall. The first of the Trust’s quarterly reports on
incidents not declared as SIs was circulated.
Post-Natal Clinic Audit
The audit (using 50 randomly selected sets of postnatal records of women who had delivered between September
and December 2013) was undertaken in order to ascertain the appropriateness of the postnatal clinic service in
terms of risk assessment.
80% of women had the home visit within 24 hours of discharge from hospital, with those not seen
within 24 hours having been discharged late in the day and one patient requested a later visit for
religious reasons.
24% of notes revealed risk factors had been identified by the visiting midwife; 100% of patients
with identified risk factors had a plan made for a home visit.

35
4.6 Continuing Care Providers
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
Monitoring the quality of care in nursing homes in Lambeth
Framework to support improvement in quality and contract monitoring.
Develop joint contract monitoring mechanism with Lambeth ACS
Scope out collaborative commissioning approach to health offer for care homes with Southwark CCG
SCMT
2
Monitoring the quality of care in out of borough nursing homes
Use of the AQP Framework to monitor quality in homes outside the borough
Implementation of the Winterbourne action plan
MM
3
Maintaining improvements in end of life care
Supporting the implementation of the CMC Register, including GP outcome targets for CMC and preferred place of death
Supporting the continued roll out of the Care Home GSF
Analysis of acute admissions at end of life (Lambeth and Southwark) to identify opportunities to support admission avoidance
Analysis of place of death information
Unplanned care
programme board

36
4.7 Primary Care (including WIC, community outpatients etc.)
Quality Issue Identified Actions Taken and Planned CCG Group
with Oversight
1
Reducing Variation in quality and outcomes in primary care
Support for practices - virtual clinics, training, clinical facilitators, referral checklists
Cycle of Practice visits to discuss QP Indicators
Practice Development Plans (CBC Strategy)
Development of Primary Care Development Networks
PCDPB
2
Improving access to GP services GP Delivery Scheme 2013/14 and developing new scheme for
2014/15 PCDPB
3
Delivering better Integrated Care
Primary Care Development Strategy workplan
Implementation of Community Based Care Strategy
SLIC development – LES etc
Risk Profiling Enhanced Service development and implementation
PCDPB
4
Walk In Centre – inappropriate service use (substitution of regular GP appointments)
Review of Gracefield Gardens WiC weekend cover so intelligent commissioning decision can be made re: Walk-in Centre provision for 2014/15. Report due to be taken to relevant boards by end of April 14.
PCDPB

37
Section 5: Patient Experience
5.1 Guy’s & St. Thomas’s NHS Foundation Trust (including Community Health Services)
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
1
Complaints
At Q3 only 31% of complaints were responded to within 25/35 working days. The latter figure is for more complex complaints. The majority of complaints had extensions agreed with complainants. The top four themes within complaints are consistent: - Standard of clinical care, especially negative impact of procedure (50%) - Waiting times / delays / cancellations (34.16%) - Poor communication/ information (23.11%) - Staff attitude and behaviour, especially disinterest and uncaring staff
(15%) Sub subject data was presented however, some validation work is required. Patient experience of the complaints process is only monitored on an annual basis by GSTT, via survey. This was raised at the February 2014 CQRG. Complaints handling is a key area of focus with the Trust. Southwark CCG completed a ‘deep dive’ looking at complaints across KCH / GSTT and SLaM in February 2014. This will be discussed with providers. Commissioners are to seek further assurance around actions to improve performance.
GSTT currently only review complainant feedback on an annual basis. They have been asked to monitor complainant feedback following each complaint, and provide reports on a quarterly basis. It is proposed that this will be included within the 2014/15 contract.
GSTT CQRG
2
Francis Report GSTT Response
Significant engagement has occurred throughout Trust to hear staff views through focus groups and surveys. An action plan is in place to address Francis recommendations relevant to the Trust.
GSTT Board update on Francis actions were discussed at the February 2014 CQRG. Details are available via the GSTT website November Board papers. http://www.guysandstthomas.nhs.uk/about-us/publications/board-papers/2013-board-papers.aspx#na Response to the October Lambeth Quality Summit recommendations currently being reviewed by the new Director of Quality. Having started with staff views GSTT were encouraged by HealthWatch to widen their feedback loop to patients. Response to this request is awaited.
GSTT CQRG

38
5.1 Guy’s & St. Thomas’s NHS Foundation Trust (including Community Health Services)
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
3a
Friends and Family A&E and inpatients
GSTT achieve an overall response rate for December of 18.9% (16.1% A&E and 25.5% inpatients). This is a continued improvement on previous months. Breakdown of net promoter scores for December was 61 A&E and 79 inpatients. This is a slight drop in A&E performance on the previous month and also in a combined score from 73 in November to 68 in December.
To form part of a national CQUIN for 2014-15 GSTT CQRG
3b Friends and Family Maternity
The FFT in maternity for experience during birth had a response rate of 22.9%. Postnatal community and postnatal ward scores are 74 and 30 respectively. Response numbers for post natal ward experience were a significantly low proportion of eligible women.
This is the first set of FFT maternity results. Work will be required to increase response rates and review issues raised. Maternity issues to be followed up at a CQRG maternity topic.
GSTT CQRG
3c Patient feedback, In-patient survey ( GSTT Community Services)
Near patient Experience CQUIN in place for 13/14 and 14/15 as long term plan to replace annual patient survey. Areas included include: Children’s – Occupational Therapy, Physiotherapy, SALT, Paediatrics and Health Visiting Adults – Inbedded Units, District Nursing, Foot Health and Reproductive Sexual Health service Main Area covered in reports include: Directorate, Period of audit, Number of questionnaires submitted, Combined result from all questionnaires, How likely would you recommend the service / ward to friends and family, cleanliness, treated with privacy and dignity. All Q3 reports show above 80% returns
Community Quarterly contract meeting to have sight of patient feedback Full copy of reports can be obtained from Mahroof Kazi Commissioning Manager Lambeth CGG. [email protected]
GSTT Community
Contract Group (Chaired by
Lambeth CCG)
4
Discharge letters
The quality and timeliness of patient discharge letters has been raised via the GP Quality Alert system and an audit undertaken at two GP practices. The findings confirmed that there were issues relating to timeliness of letters being sent and the quality of the information.
GSTT CQRG
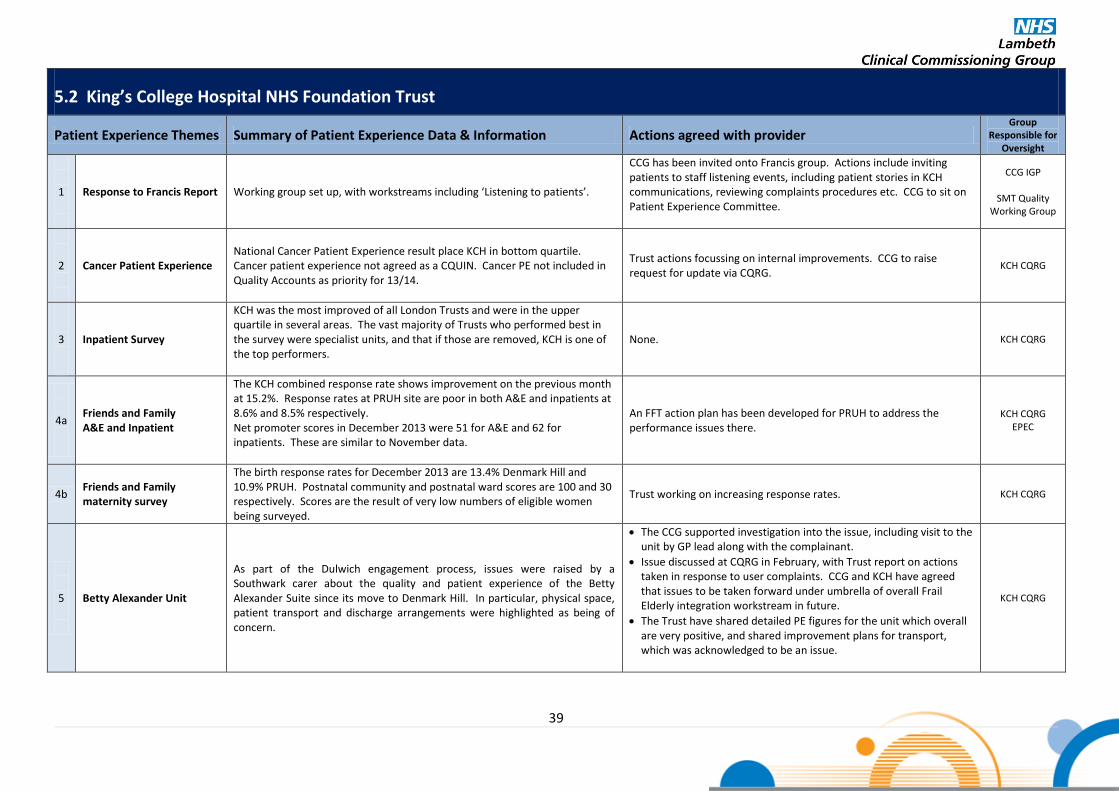
39
5.2 King’s College Hospital NHS Foundation Trust
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
1
Response to Francis Report Working group set up, with workstreams including ‘Listening to patients’.
CCG has been invited onto Francis group. Actions include inviting patients to staff listening events, including patient stories in KCH communications, reviewing complaints procedures etc. CCG to sit on Patient Experience Committee.
CCG IGP
SMT Quality Working Group
2
Cancer Patient Experience National Cancer Patient Experience result place KCH in bottom quartile. Cancer patient experience not agreed as a CQUIN. Cancer PE not included in Quality Accounts as priority for 13/14.
Trust actions focussing on internal improvements. CCG to raise request for update via CQRG.
KCH CQRG
3
Inpatient Survey
KCH was the most improved of all London Trusts and were in the upper quartile in several areas. The vast majority of Trusts who performed best in the survey were specialist units, and that if those are removed, KCH is one of the top performers.
None. KCH CQRG
4a
Friends and Family A&E and Inpatient
The KCH combined response rate shows improvement on the previous month at 15.2%. Response rates at PRUH site are poor in both A&E and inpatients at 8.6% and 8.5% respectively. Net promoter scores in December 2013 were 51 for A&E and 62 for inpatients. These are similar to November data.
An FFT action plan has been developed for PRUH to address the performance issues there.
KCH CQRG EPEC
4b Friends and Family maternity survey
The birth response rates for December 2013 are 13.4% Denmark Hill and 10.9% PRUH. Postnatal community and postnatal ward scores are 100 and 30 respectively. Scores are the result of very low numbers of eligible women being surveyed.
Trust working on increasing response rates. KCH CQRG
5
Betty Alexander Unit
As part of the Dulwich engagement process, issues were raised by a Southwark carer about the quality and patient experience of the Betty Alexander Suite since its move to Denmark Hill. In particular, physical space, patient transport and discharge arrangements were highlighted as being of concern.
The CCG supported investigation into the issue, including visit to the unit by GP lead along with the complainant.
Issue discussed at CQRG in February, with Trust report on actions taken in response to user complaints. CCG and KCH have agreed that issues to be taken forward under umbrella of overall Frail Elderly integration workstream in future.
The Trust have shared detailed PE figures for the unit which overall are very positive, and shared improvement plans for transport, which was acknowledged to be an issue.
KCH CQRG
40
5.2 King’s College Hospital NHS Foundation Trust
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
6 Complaints
The internal performance target for responding to complaints continues to be below 70% within 25 working days. Year to date position - 43%. (Feb 2014). This position is being monitored through the weekly Performance Improvement Group and Divisions have been supported in targeting the backlog of overdue cases. Performance is tracked in monthly performance report and scorecard (Trust and Divisional level). Complaints performance and quality of responses to be reviewed by the Serious Complaints Committee chaired by Non-Executive Director (first meeting in February). Complaints handling is a key area of focus with the Trust. Southwark CCG completed a ‘deep dive’ looking at complaints across KCH / GSTT and SLaM and the report was discussed at the February 2014 CQRG. .
Trust responsiveness within agreed timescales is poor across both sites and is subject to an improvement plan.
KCH CQRG

41
5.3 South London & Maudsley NHS Foundation Trust
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
1
Complaints
There were 551 complaints recorded from 1 April 2012 to 31 March 2013. This is a very slight decrease (<1%) from the previous year 2011/12 in which the Trust received 555 complaints. In Q1 for 2013/14 there were 21 complaints and 25 in Q2. In Q3 there were 30 complaints.
SLaM complaints and compliments are monitored on a monthly basis via core contract monitoring meetings.
CCG contract meeting
2
SLaMs Single Equality Scheme
1. Targeted mental health promotion working with groups at greatest risk.
2. Improving engagement with BME communities.
3. Improving employment opportunities for service users
1. Involvement with BME groups to work with young people in care on improving ambition and life chances.
2. Mental Health Promotion team and Spiritual and Pastoral Care
service deliver training to local faith leaders and groups on mental health, wellbeing and spirituality
3. SLaM supports service users to participate in peer support,
volunteering and time bank schemes with some of these opportunities being financially reimbursed.
CCG contract meeting
3
Eliminating mixed sex accommodation
The Trust remains complaint with EMSA requirements and there were no breaches in FY 2012/13.
Mixed Sex Accommodation included as a Quality Indicator in the 2013/14 contract where it’s reported monthly with a sanction of £250 per patient per day.
CCG contract meeting
4
2013/14 CQUIN - SLaM The SLaM Patient and Public Involvement (PPI) team will run focus groups with ward link workers to identify the top 5 issues which they feel need to be improved.
The patient experience CQUIN will establish a baseline in Q1 of areas that need to be improved with SLaM producing an action plan in Q2 and progress against this action plan evaluated by focus groups in Q3. The action plan was successfully produced at Q2 and identified clearly areas of improvement across all key quality domains. Final results of areas that evidence improvement will be reported in Q4.
CCG contract meeting
5
Patient Experience SLaMs PPI team undertake regular, anonymous surveys of patient experience which is fed back to CAGs to make improvements.
This initiative very much links to the 2013/14 patient experience CQUIN described above.
CCG contract meeting

42
5.3 South London & Maudsley NHS Foundation Trust
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
6
Recovery and Support Plan CQUIN
The CQUIN incentivises the implementation of the new recovery and support plan that places the service user at the centre of the care/support planning process where they are supported to define their own goals based on their personal needs and aspirations.
A baseline for this CQUIN will be established at Q1. A target for Q4 will be agreed which seeks to significantly improve on the number of support and recovery plans completed within Adult Mental Health. In addition, the CQUIN requires SLaM to produce an implementation plan that identifies the specific initiatives introduced to increase the number and quality of support and recovery plans completed. The evidence that this plan has been successfully implemented will be evaluated. A target for Q4 has been agreed for Q4 which is 55%
CCG contract meeting
7
Summary of Complaints (Key themes)
145 complaints received in Q4 2012/13. 65 for treatment and care, 31 for attitude and behaviour and 9 for communication.
SLaM has a panel which meets at the end of the year to look at trends and analyse complaints across all CAGs. They agree actions and feedback to SCCG which will influence Mental Health commissioning intentions for 2014/15.
CCG contract / quality meeting

43
5.4 St George’s Hospital NHS Trust - Not updated Q3
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
1 Francis report
Two approaches to the Francis Report agreed
To complete a response to the 290 recommendations in the report applicable to the trust
To consider the high level corporate commitments that the Trust Board will make in response to the key findings of the report to improve quality for patients.
7 high level corporate commitments agreed. Action plan developed.
Presented poster information at the Lambeth Quality Summit on 2 October 2013
Action plan to be monitored by SGH Quality and Risk Committee and reviewed by SGH Trust Board and by Wandsworth CCG
Nursing to focus on the 30 recommendations in the report focused on Nursing in conjunction with the CQC report and national strategy for compassionate care
WCCG CQRG
44
5.5 Primary Care (including WIC, community outpatients etc.)
Patient Experience Themes Summary of Patient Experience Data & Information Actions agreed with provider Group
Responsible for Oversight
1
Improve access Annual Patient Survey
46 providers with various access issues
Practice Action Plans to be implemented over Summer 2013
Patient participation groups (PPGS) currently under development within practices.
Primary & Community
Care Strategy Group
2
Reducing Variation in quality and outcomes in primary care
QoF data 48 providers with various issues
Ongoing monthly submissions by practices
Primary & Community
Care Strategy Group
3
Access to diagnostic services at each practice
Out of Hospital Event
46 providers with various services
Phlebotomy Service Review to be completed Spring 2014
Primary care commissioning services (PCCS) website to be updated November 2013
Primary & Community
Care Strategy Group
Commissioning Strategy Group

45
5.6 Friends and Family Test – Maternity
The first results of the Friends and Family Test (FFT) for NHS-funded maternity services across England were published 30 January 2014 alongside the latest FFT results for A&E and
Inpatient departments. Summary findings for each acute provider are included in the Patient Experience section above.
The data comprises feedback from thousands of pregnant women and mothers of new-born babies who, since October 1, 2013, have been giving their views on the services they receive
throughout their pregnancy.
The Friends and Family Test asks women up to four questions at three stages during their pregnancy, seeking feedback about antenatal services, the labour ward/ birthing unit or home
birth services, the postnatal ward and the postnatal community services. Key findings for providers are included under the Quality
They are asked whether they would recommend maternity services to their nearest and dearest based on their own experience. Their responses will build into the most comprehensive
feedback exercise ever undertaken with pregnant women and involves 138 trusts and more than 200 maternity sites nationally.
Results suggest the FFT for maternity services is working well:
Over the first three months, more than 93,600 pieces of feedback were gathered from pregnant women and mums.
The response rates for their feedback on the services offered at the birth of their child topped more than 19 per cent for each of the three months October to December – out
performing the target level of 15 per cent.
138 NHS trusts (all expected organisations) submitted data for November and December. Only one organisation did not submit data for October due to difficulties collating the
data.
In December there were 175 (plus 44 community) sites covered for question one, for question two it was 205 (plus 44 community) and for question three 202 (plus 6
community). Question four responses were collected at trust level only and data was received for all 138 trusts.
At site level, the total number of most positive scores (+100) has risen from 70 in November to 93 in December.
The number of sites with the most negative score of -100 decreased from three in November to just two in December across questions one to three.
The real strength of the Friends and Family Test lies in the rich source of views that can be used locally to highlight and address concerns much faster than more traditional survey methods.
Comments from women are rapidly available to frontline maternity staff, so practical action can be taken to address problems that concern patients in a prompt “You said – we did”
response.

46
Section 6: Engagement Issues and Feedback
The following information includes a brief summary of how Lambeth Clinical Commissioning Group (LCCG) has engaged with members and clinical network leads to support the delivery of LCCG objectives and developments.
CareConnect a new system currently being piloted via NHS Choices for service users to report issues and receive responses was launched on 1 August 2013. GSTT and St Georges are taking part as pilot sites. There is not enough data at present to identify themes. A meeting has been arranged with the HSCIC lead for the system to discuss the system and possible developments.
Area of
engagement
Summary of engagement
Actions Identified
1
All Practice Event
The All Practice Event was held on 4th February. Over 136 people attended with representatives from 44 out of our 48 practices. The afternoon provided a good opportunity for member practices to:
for local primary care development
and influence local priorities
membership and engagement
The event included a ‘market place’ of stalls which included:
Council
values
Progress since the Big Lambeth Health Debate and how this links to the development of the CCG strategic and operational planning was shared. Members had an opportunity to participate in group discussions regarding the development and implementation of some of the key strategic priorities including: Acute Contracting – with a focus on integration and repatriation from hospitals outside of the borough; mental health ‘alliance’ contracting; long-terms conditions – diabetes and respiratory disease; prevention – ‘fitness for surgery’
2
Clinical Network Event
Ash Soni, Clinical Network lead, led the first Clinical Network event on 16th January. This was an opportunity for members of the Network to meet, get to know each other, learn more about the local system and strategy and what colleagues are involved in, and how members can all be part of the network’s development. The event was well attended by over 20 members.
The key actions to come out of the event were: • A network development plan informed by a meeting with every network member to be published
• The publication of a directory of network members
• Regular communication between members (ideally virtual) for members to share updates on their network activities and share expertise will be established
• A draft induction pack for clinical network members to be developed.
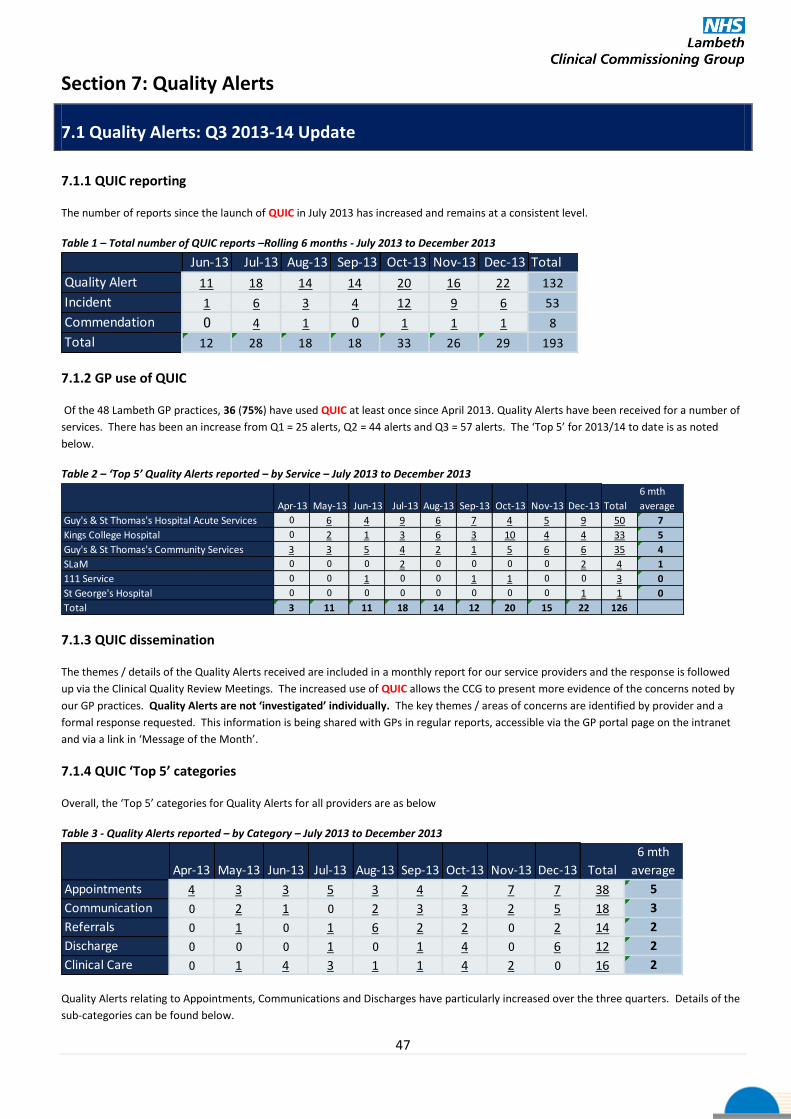
47
Section 7: Quality Alerts
7.1 Quality Alerts: Q3 2013-14 Update
7.1.1 QUIC reporting
The number of reports since the launch of QUIC in July 2013 has increased and remains at a consistent level.
Table 1 – Total number of QUIC reports –Rolling 6 months - July 2013 to December 2013
Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
Quality Alert 11 18 14 14 20 16 22 132
Incident 1 6 3 4 12 9 6 53
Commendation 0 4 1 0 1 1 1 8
Total 12 28 18 18 33 26 29 193
7.1.2 GP use of QUIC
Of the 48 Lambeth GP practices, 36 (75%) have used QUIC at least once since April 2013. Quality Alerts have been received for a number of
services. There has been an increase from Q1 = 25 alerts, Q2 = 44 alerts and Q3 = 57 alerts. The ‘Top 5’ for 2013/14 to date is as noted
below.
Table 2 – ‘Top 5’ Quality Alerts reported – by Service – July 2013 to December 2013
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
6 mth
average
Guy's & St Thomas's Hospital Acute Services 0 6 4 9 6 7 4 5 9 50 7
Kings College Hospital 0 2 1 3 6 3 10 4 4 33 5
Guy's & St Thomas's Community Services 3 3 5 4 2 1 5 6 6 35 4
SLaM 0 0 0 2 0 0 0 0 2 4 1
111 Service 0 0 1 0 0 1 1 0 0 3 0
St George's Hospital 0 0 0 0 0 0 0 0 1 1 0
Total 3 11 11 18 14 12 20 15 22 126
7.1.3 QUIC dissemination
The themes / details of the Quality Alerts received are included in a monthly report for our service providers and the response is followed
up via the Clinical Quality Review Meetings. The increased use of QUIC allows the CCG to present more evidence of the concerns noted by
our GP practices. Quality Alerts are not ‘investigated’ individually. The key themes / areas of concerns are identified by provider and a
formal response requested. This information is being shared with GPs in regular reports, accessible via the GP portal page on the intranet
and via a link in ‘Message of the Month’.
7.1.4 QUIC ‘Top 5’ categories
Overall, the ‘Top 5’ categories for Quality Alerts for all providers are as below
Table 3 - Quality Alerts reported – by Category – July 2013 to December 2013
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
6 mth
average
Appointments 4 3 3 5 3 4 2 7 7 38 5
Communication 0 2 1 0 2 3 3 2 5 18 3
Referrals 0 1 0 1 6 2 2 0 2 14 2
Discharge 0 0 0 1 0 1 4 0 6 12 2
Clinical Care 0 1 4 3 1 1 4 2 0 16 2
Quality Alerts relating to Appointments, Communications and Discharges have particularly increased over the three quarters. Details of the
sub-categories can be found below.

48
7.1.5 Quality Alert sub categories
Issues around appointments for April to December 2013 for all providers include:
Table 4 – Appointments Quality Alerts – by Quality Alert sub-category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
Failure of service to visit patient 3 (7.89%) 2 (5.26%) 1 (2.63%) 1 (2.63%) 1 (2.63%) 1 (2.63%) 0 (0%) 3 (7.89%) 4 (10.53%) 16 (42.11%)
Follow-up appointment not
made for patient 0 (0%) 0 (0%) 2 (5.26%) 2 (5.26%) 0 (0%) 0 (0%) 1 (2.63%) 2 (5.26%) 0 (0%) 7 (18.42%)
Delay / length of time receiving
appointment 0 (0%) 0 (0%) 0 (0%) 1 (2.63%) 0 (0%) 0 (0%) 0 (0%) 2 (5.26%) 3 (7.89%) 6 (15.79%)
Increased administration and/or
work for practice following up
appointment 0 (0%) 0 (0%) 0 (0%) 1 (2.63%) 1 (2.63%) 1 (2.63%) 1 (2.63%) 0 (0%) 0 (0%) 4 (10.53%)
Patient issues with DNA letters
and/or re-referrals 0 (0%) 1 (2.63%) 0 (0%) 0 (0%) 1 (2.63%) 1 (2.63%) 0 (0%) 0 (0%) 0 (0%) 3 (7.89%)
Other 1 (2.63%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (2.63%) 0 (0%) 0 (0%) 0 (0%) 2 (5.26%)
Total 4 (10.53%) 3 (7.89%) 3 (7.89%) 5 (13.16%) 3 (7.89%) 4 (10.53%) 2 (5.26%) 7 (18.42%) 7 (18.42%) 38 (100%)
Issues around communications for April to December 2013 for all providers include:
Table 5 – Communications Quality Alerts – by Quality Alert sub-category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
Poor quality communication 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (5.56%) 2 (11.11%) 1 (5.56%) 1 (5.56%) 5 (27.78%)
Communications not received and/or
acted on 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (5.56%) 1 (5.56%) 0 (0%) 1 (5.56%) 1 (5.56%) 4 (22.22%)
Communication / contact information
out of date / incorrect 0 (0%) 0 (0%) 1 (5.56%) 0 (0%) 1 (5.56%) 0 (0%) 0 (0%) 0 (0%) 1 (5.56%) 3 (16.67%)
Other 0 (0%) 2 (11.11%) 0 (0%) 0 (0%) 0 (0%) 1 (5.56%) 0 (0%) 0 (0%) 0 (0%) 3 (16.67%)
Unable to contact service / calls not
returned 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 2 (11.11%) 2 (11.11%)
Failure to attend meetings etc with
clinical teams 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (5.56%) 0 (0%) 0 (0%) 1 (5.56%)
Total 0 (0%) 2 (11.11%) 1 (5.56%) 0 (0%) 2 (11.11%) 3 (16.67%) 3 (16.67%) 2 (11.11%) 5 (27.78%) 18 (100%)
Issues around referrals for April to December 2013 for all providers include:
Table 6 – Referrals Quality Alerts – by Quality Alert sub-category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
Referral to Hospital Services 0 (0%) 0 (0%) 0 (0%) 1 (7.14%) 5 (35.71%) 2 (14.29%) 2 (14.29%) 0 (0%) 2 (14.29%) 12 (85.71%)
Other 0 (0%) 1 (7.14%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (7.14%)
Issues with referral to District Nursing 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (7.14%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (7.14%)
Total 0 (0%) 1 (7.14%) 0 (0%) 1 (7.14%) 6 (42.86%) 2 (14.29%) 2 (14.29%) 0 (0%) 2 (14.29%) 14 (100%)
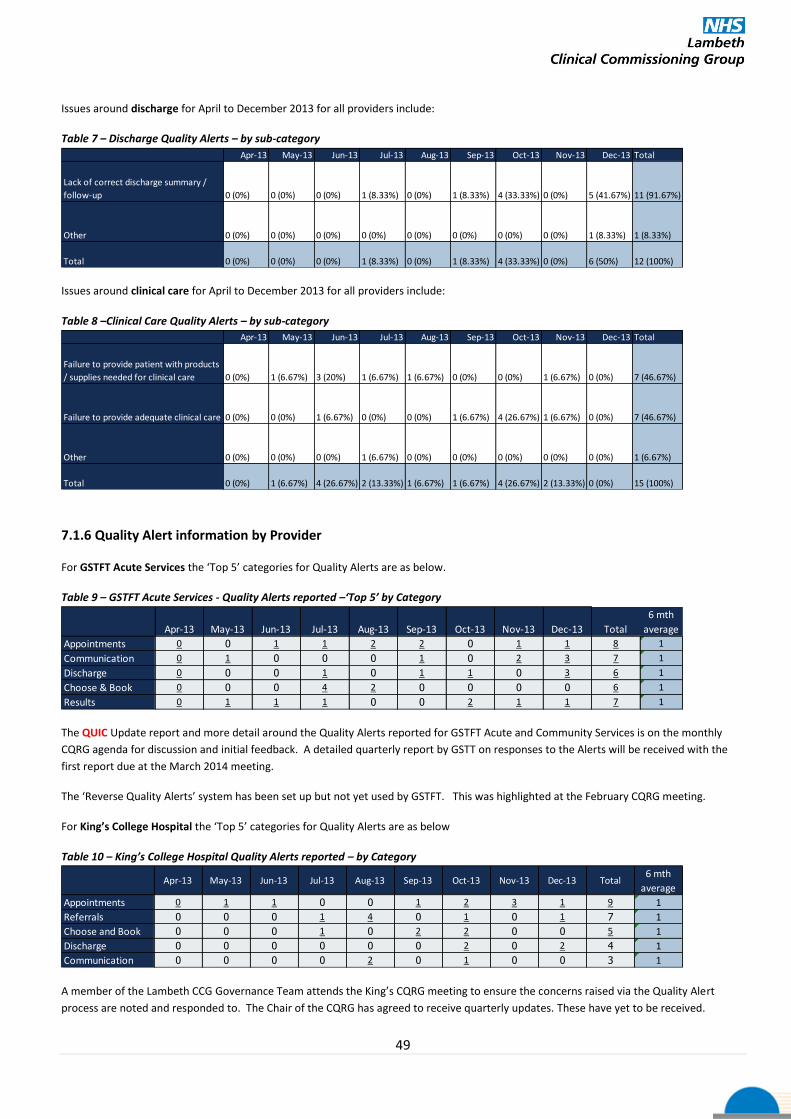
49
Issues around discharge for April to December 2013 for all providers include:
Table 7 – Discharge Quality Alerts – by sub-category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
Lack of correct discharge summary /
follow-up 0 (0%) 0 (0%) 0 (0%) 1 (8.33%) 0 (0%) 1 (8.33%) 4 (33.33%) 0 (0%) 5 (41.67%) 11 (91.67%)
Other 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (8.33%) 1 (8.33%)
Total 0 (0%) 0 (0%) 0 (0%) 1 (8.33%) 0 (0%) 1 (8.33%) 4 (33.33%) 0 (0%) 6 (50%) 12 (100%)
Issues around clinical care for April to December 2013 for all providers include:
Table 8 –Clinical Care Quality Alerts – by sub-category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
Failure to provide patient with products
/ supplies needed for clinical care 0 (0%) 1 (6.67%) 3 (20%) 1 (6.67%) 1 (6.67%) 0 (0%) 0 (0%) 1 (6.67%) 0 (0%) 7 (46.67%)
Failure to provide adequate clinical care 0 (0%) 0 (0%) 1 (6.67%) 0 (0%) 0 (0%) 1 (6.67%) 4 (26.67%) 1 (6.67%) 0 (0%) 7 (46.67%)
Other 0 (0%) 0 (0%) 0 (0%) 1 (6.67%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (6.67%)
Total 0 (0%) 1 (6.67%) 4 (26.67%) 2 (13.33%) 1 (6.67%) 1 (6.67%) 4 (26.67%) 2 (13.33%) 0 (0%) 15 (100%)
7.1.6 Quality Alert information by Provider
For GSTFT Acute Services the ‘Top 5’ categories for Quality Alerts are as below.
Table 9 – GSTFT Acute Services - Quality Alerts reported –‘Top 5’ by Category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
6 mth
average
Appointments 0 0 1 1 2 2 0 1 1 8 1
Communication 0 1 0 0 0 1 0 2 3 7 1
Discharge 0 0 0 1 0 1 1 0 3 6 1
Choose & Book 0 0 0 4 2 0 0 0 0 6 1
Results 0 1 1 1 0 0 2 1 1 7 1
The QUIC Update report and more detail around the Quality Alerts reported for GSTFT Acute and Community Services is on the monthly
CQRG agenda for discussion and initial feedback. A detailed quarterly report by GSTT on responses to the Alerts will be received with the
first report due at the March 2014 meeting.
The ‘Reverse Quality Alerts’ system has been set up but not yet used by GSTFT. This was highlighted at the February CQRG meeting.
For King’s College Hospital the ‘Top 5’ categories for Quality Alerts are as below
Table 10 – King’s College Hospital Quality Alerts reported – by Category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total6 mth
average
Appointments 0 1 1 0 0 1 2 3 1 9 1
Referrals 0 0 0 1 4 0 1 0 1 7 1
Choose and Book 0 0 0 1 0 2 2 0 0 5 1
Discharge 0 0 0 0 0 0 2 0 2 4 1
Communication 0 0 0 0 2 0 1 0 0 3 1
A member of the Lambeth CCG Governance Team attends the King’s CQRG meeting to ensure the concerns raised via the Quality Alert
process are noted and responded to. The Chair of the CQRG has agreed to receive quarterly updates. These have yet to be received.

50
For GSTFT Community Services the ‘Top 5’ categories for Quality Alerts are as below.
Table 11 – GSTFT Community Services - Quality Alerts reported –‘Top 5’ by Category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total
6 mth
average
Appointments 3 2 1 3 1 1 0 3 4 18 2
Clinical Care 0 0 4 1 1 0 3 2 0 11 1
Communication 0 0 0 0 0 0 1 0 2 3 1
Prescribing 0 0 0 0 0 0 0 1 0 1 0
Results 0 1 0 0 0 0 0 0 0 1 0
The issues of particular concern within the GSTFT Community Services relates to the failure of District Nurses to visit patients, provide the
care required and communicate both with users and their GP. This was discussed at the November GSTFT Clinical Quality Review Group
meeting (CQRG) and an action plan is being monitored via the contract meeting. An update on this plan was provided to the February CQRG
meeting and discussed. This will have an impact on the successful delivery of the Service Improvement Plan and for that reason has been
added to both the GSTT and Lambeth CCG corporate risk registers. Originally graded risk 12 by GSTT this has recently been reassessed at 16.
Table 12 – 111 Service - Quality Alerts reported –‘Top 5’ by Category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total6 mth
average
Communication 0 0 1 0 0 1 1 0 0 3 0
Table 13 – SLaM - Quality Alerts reported –‘Top 5’ by Category
Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sep-13 Oct-13 Nov-13 Dec-13 Total6 mth
average
Appointments 0 0 0 1 0 0 0 0 1 2 0
Referrals 0 0 0 0 0 0 0 0 1 1 0
Clinical Care 0 0 0 1 0 0 0 0 0 1 0
The Governance Team at the CCG are currently liaising with the KCH, SLaM, 111 and Seldoc for access and use of the QUIC system to receive
and report on Quality Alerts, Incidents and Commendations. This QUIC Update report and more detail around the Quality Alerts reported
for each provider organisation is sent to each organisation for information and to obtain feedback.
7.1.7 Quality Alerts Summary and Next Steps
District Nursing: Concerns about appointments are the top reporting issue relating mostly to the failure of District nurses to visit patients at
home. This has increased over the three quarters and also links to failures in clinical care, specifically, to ensuring patients are provided with
products / supplies needed for clinical care e.g. incontinence pads, and the failure to provide adequate clinical care when making home
visits.
Failings in this service have been acknowledged by GSTFT who have put into place an action plan to address the identified issues. This is
being monitored through the contract meeting but with updates going to the clinical quality review meetings.
Follow up appointments: There are issues with patients not being sent follow up appointments adding to referrals and administrative work
on the primary care level remains an issue, increasing in quarter 3. Feedback on actions taken at GSTFT to address this issue are awaited.
Communications: There are concerns about the poor quality of communications, and communications not received or acted on. Some of
this is specific to the poor quality of discharge summary information which has been confirmed in a practice audit of discharge letters and
discussed with GSTFT at the October 2013 and January clinical quality review meetings. Feedback on actions being taken by GSTFT
specifically to address these issues are awaited. It is proposed to include specific discharge documentation requirements within the
contract for 2014/15.
Next Steps: Overall, the reporting of Quality Alerts by Practices has increased from 25 in Q1 to 57 in Q3. Dr Aysha Butt, Network Clinical
Quality Lead is continuing to visit practices in the borough to obtain feedback about QUIC and address problems and concerns. Feedback
to GPs on QUIC information and actions taken by providers and development work around establishing use of the QUIC system by providers
other than GSTT will continue.

51
Section 8: Clinical Site Visits
8.1 Clinical Site Visits
To date (19 February 2014) there are reports for 1207 GP Care Quality Commission inspections available. Seven of
these are within the M35 from Enfield to Ewell. There have been no reported inspections for GP practices in
Lambeth. Updates will be provided in this section of the Quality Report.
Provider Audited / Visited Organisation undertaking the Audit /Visit
Audit date RAG status
Holistic Community Care Limited Care Quality Commission
19 December 2013
Southside Partnership –Ambleside Avenue
Care Quality Commission 18 December 2013
Lambeth Hospital Care Quality Commission
13 December 2013
Collingwood Court Nursing Home Care Quality Commission
10th
December 2013
Dulwich Care Centre – Follow up inspection
Care Quality Commission 9 December 2013
Ladywell Hospital (SLaM) Care Quality Commission
6 December 2013
Princess Royal University Hospital (PRU) Care Quality Commission
2-4, 10 December 2013
St Mary’s Care Home Care Quality Commission
25th
November 2013
Marie Curie Cancer Care – Nursing and Domiciliary Care Service
Care Quality Commission 18 November 2013
St Thomas’s Hospital (GSTT) Care Quality Commission
11-12 November 2013
Maudsley Hospital (SLaM) Care Quality Commission
29 October 2013
Limetrees Care Centre Care Quality Commission
17 October 2013
The Laurels Care Home Care Quality Commission
8th
October 2013
St Georges Healthcare NHS Trust Care Quality Commission
15-17 August 2013
The Care Quality Commission (CQC) began using a new approach to inspect acute hospitals from September 2013. Inspections are a mixture of announced and unannounced visits. The aim is to get to the heart of the patients’ experiences by looking at the quality and safety of the care provided. The CQC will look at whether the service is: safe, effective, caring, responsive to people’s needs and well-led. As part of the inspection model the CQC will analyse and review data and information they hold about the trust the will be inspecting. This includes information from local and voluntary groups, people who use the services, other stakeholders and the trust. Trigger indicators are also considered including: avoidable infections e.g. MSSA, MRSA and e-coli; notification of deaths and abuse; never events; mortality rates; information from ‘your experience form’ on the CQC website; information from patient and staff surveys and complaints. The inspection teams are led by an experienced CQC manager and chaired by a senior NHS clinician or executive. They will always include: professional and clinical staff, experts by experience; patients, carers. Inspections involve focus groups with staff, listening event for public, patient and carer/relative discussions and observations.

52
8.2 Clinical Site Visits & Detail
Provider Audited/Visited:
Holistic Community Care Limited 19 December 2013 - Reported 25 January 2014
Name and Purpose of Audit/ Visit:
Unannounced Inspection by the CQC
Description of Audit / Visit and Key Findings
Holistic Community Care Limited provides personal care to people living in their own homes. It currently provides care to more than 200 people living in London boroughs of Merton, Lambeth, Ealing and Wandsworth. The agency office is located in the London borough of Lambeth. Two Lambeth residents use these services. The CQC looked at the personal care or treatment records of people who use the service, carried out a visit on 19 December 2013, observed how people were being cared for and checked how people were cared for at each stage of their treatment and care. They talked with people who use the service, talked with carers and / or family members, talked with staff and reviewed information given to us by the provider. They reviewed information sent by commissioners of services, talked with commissioners of services and used information from local Healthwatch to inform their inspection. They were supported on this inspection by an expert-by-experience. This was a person with personal experience of using or caring for someone who uses this type of care Service.
The following standards were inspected and found to have been met: Respecting and involving people who use services – people should be treated
with respect, involved in discussions about their care and treatment and able to influence how the service is run.
Care and welfare of people who use services – people should get safe and appropriate care that meets their needs and supports their rights.
Supporting workers – staff should be properly trained and supervised, and have the chance to develop and improve their skills.
Assessing and monitoring the quality of service provision – the service should have quality checking systems to manage risks and assure the health, welfare and safety of people who receive care.

53
Provider Audited/Visited:
Southside Partnership – Ambleside Avenue
18 December 2013 – Reported 5 February 2014
Name and Purpose of Audit/ Visit:
Unannounced Inspection – CQC
Description of Audit / Visit and Key Findings
15 Ambleside Avenue provides care for six people with learning disabilities, some of whom have additional physical disabilities and sensory impairments. Lambeth CCG have one service user using this service.
The CQC looked at the personal care or treatment records of people who use the service and observed how people were care for at each stage of their treatment and care. The CQC used a number of different methods to help understand the experiences of people as the people using the service had complex needs which meant they were not able to tell the CQC their experiences. The CQC observed how people with risks associated with eating and drinking had their safety promoted. Staff felt more confident in their roles, they had received role related training and followed recommendations made by health professionals to support people with remaining safe. Staff had extensive input from health and social care professionals and were supported by management in their personal and professional development. Practices were monitored closely to ensure they followed recommendations made by health professionals. People were treated with warmth and respect by staff. The CQC observed that staff supported people needing assistance to transfer safely and ensured their modesty and dignity was promoted. The CQC also talked with people who use the service, carers and / or family members, staff and reviewed information given to them by the provider and commissioners of services.
The following standards were inspected and found to have been met: Care and welfare of people who use services – people should get safe and
appropriate care that meets their needs and supports their rights.
Notification of other incidents - the service must tell us about important events that affect people's wellbeing, health and safety
Records - people's personal records, including medical records, should be accurate and kept safe.
At the previous inspection 12th July 2013 the CQC found inaccuracies in people's records with a lack of consistency in how the records were completed. The current visit found that personal records were stored securely and could be located promptly when needed. Record keeping had improved and daily records were up to date. and confidential

54
Provider Audited/Visited:
Lambeth Hospital (SLaM) 13 December 2013 - Reported 19 January 2014
Name and Purpose of Audit/ Visit:
Unannounced Inspection by the CQC
Carried out in response to concerns that one or more of the essential standards of
quality and safety were not being met.
Description of Audit / Visit and Key Findings
The CQC looked at the personal care or treatment records of people who use the service and talked with staff. The CQC focussed on the care and welfare provided to the people using the service, and how the service worked with other providers to ensure people received the appropriate care and treatment because of the concerns raised. They found that people were appropriately assessed and received care and treatment in line with their individual needs. People had a care co-ordinator allocated to them and from the records they saw people had regular contact with their care co-ordinator. People also had contact with their consultant psychiatrist as frequently as required. The care co-ordinator ensured that people's mental and physical health needs were met, and supported people to manage their finances and access their benefits, if appropriate. They also ensured that people had appropriate accommodation and liaised with local housing services if there were any concerns. The CQC also saw that staff liaised with other providers to ensure the health, safety and welfare of people using the service. Staff remained in contact with their patients when they were residing on inpatient wards or were in prison. The staff also had regular contact with the patient's GP to ensure their physical health needs were being met. There was contact between the service and the local pharmacy service to ensure that people were receiving the required blood tests and monitoring in line with their clozapine medication.
The following standards were inspected and found to have been met: Care and welfare of people who use services – people should get safe and
appropriate care that meets their needs and supports their rights.
Cooperating with other providers – people should get safe and coordinated care when they move between different services.

55
Provider Audited/Visited:
Collingwood Court Nursing Home
10 December 2013 – Reported 21st December 2013
Name and Purpose of Audit/ Visit:
Routine Inspection – CQC
Description of Audit / Visit and Key Findings
Collingwood Court Nursing Home is a BUPA care home, located in Clapham with 80
nursing beds. The CCG currently has CHC patients in the home
CQC’s previous inspection on 26 July 2013 found that it was unclear from the
records whether a person had been assessed as having the capacity to consent to
decisions about their care and therefore it was unclear as to whether they had
been appropriately involved in their care choices. During this inspection on 10
December 2013, CQC found that a person’s capacity to consent to decisions about
their care had been reviewed and it was clear from the records as to which
decisions they had been involved in
The following standards were inspected and found to have been met:
Respecting and involving people who use services
Care and welfare of people who use services
Safety and suitability of premises
Staffing
Complaints
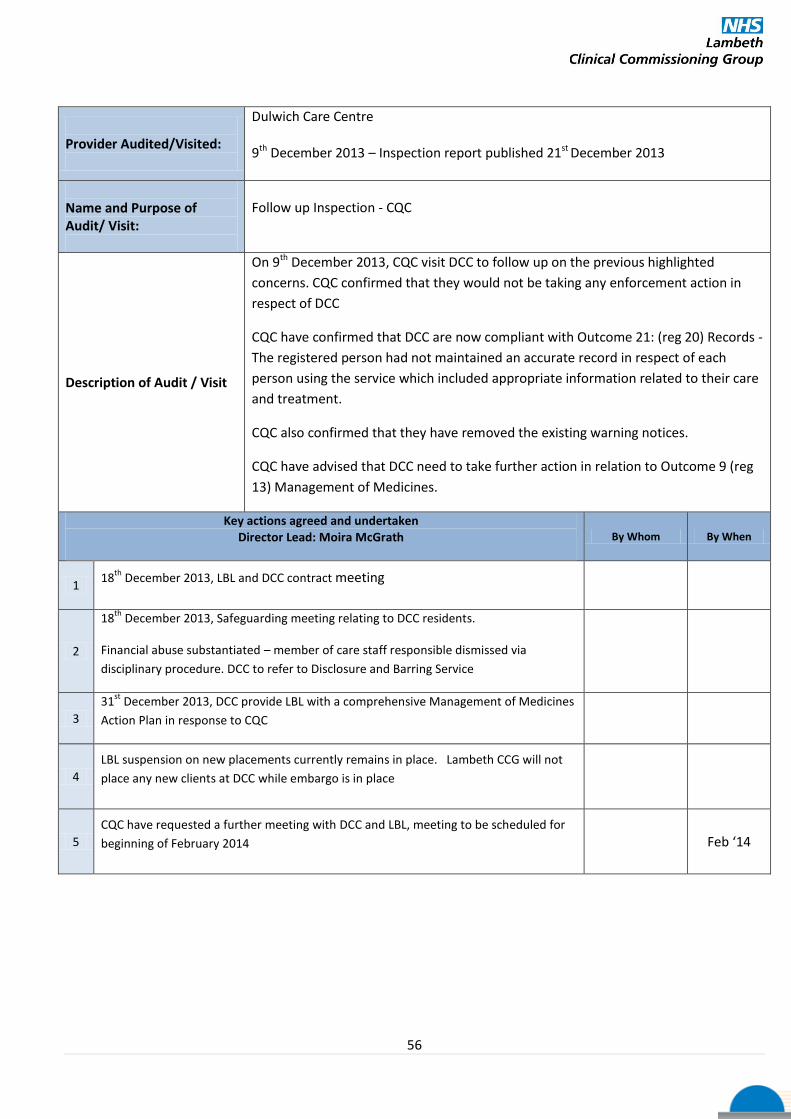
56
Provider Audited/Visited:
Dulwich Care Centre
9th December 2013 – Inspection report published 21st December 2013
Name and Purpose of Audit/ Visit:
Follow up Inspection - CQC
Description of Audit / Visit
On 9th December 2013, CQC visit DCC to follow up on the previous highlighted
concerns. CQC confirmed that they would not be taking any enforcement action in
respect of DCC
CQC have confirmed that DCC are now compliant with Outcome 21: (reg 20) Records -
The registered person had not maintained an accurate record in respect of each
person using the service which included appropriate information related to their care
and treatment.
CQC also confirmed that they have removed the existing warning notices.
CQC have advised that DCC need to take further action in relation to Outcome 9 (reg
13) Management of Medicines.
Key actions agreed and undertaken Director Lead: Moira McGrath By Whom By When
1 18
th December 2013, LBL and DCC contract meeting
2
18th
December 2013, Safeguarding meeting relating to DCC residents.
Financial abuse substantiated – member of care staff responsible dismissed via
disciplinary procedure. DCC to refer to Disclosure and Barring Service
3
31st
December 2013, DCC provide LBL with a comprehensive Management of Medicines
Action Plan in response to CQC
4
LBL suspension on new placements currently remains in place. Lambeth CCG will not
place any new clients at DCC while embargo is in place
5
CQC have requested a further meeting with DCC and LBL, meeting to be scheduled for
beginning of February 2014 Feb ‘14
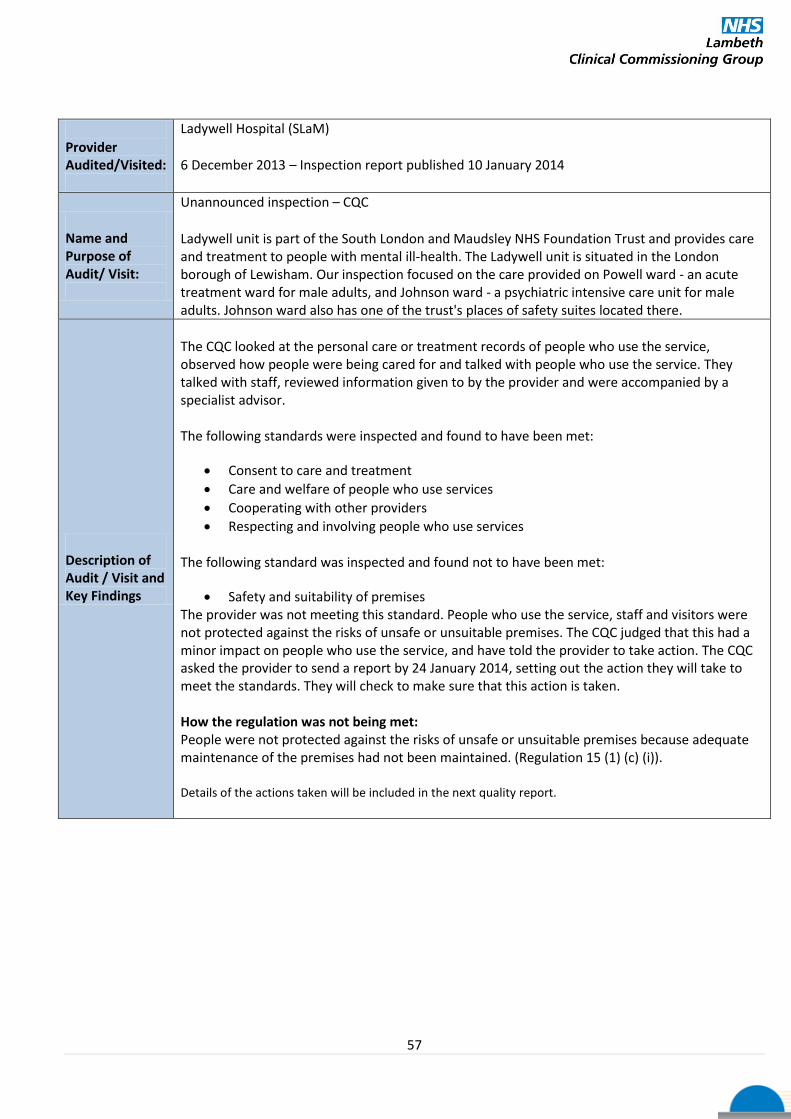
57
Provider Audited/Visited:
Ladywell Hospital (SLaM)
6 December 2013 – Inspection report published 10 January 2014
Name and Purpose of Audit/ Visit:
Unannounced inspection – CQC
Ladywell unit is part of the South London and Maudsley NHS Foundation Trust and provides care and treatment to people with mental ill-health. The Ladywell unit is situated in the London borough of Lewisham. Our inspection focused on the care provided on Powell ward - an acute treatment ward for male adults, and Johnson ward - a psychiatric intensive care unit for male adults. Johnson ward also has one of the trust's places of safety suites located there.
Description of Audit / Visit and Key Findings
The CQC looked at the personal care or treatment records of people who use the service, observed how people were being cared for and talked with people who use the service. They talked with staff, reviewed information given to by the provider and were accompanied by a specialist advisor. The following standards were inspected and found to have been met:
Consent to care and treatment
Care and welfare of people who use services
Cooperating with other providers
Respecting and involving people who use services
The following standard was inspected and found not to have been met:
Safety and suitability of premises The provider was not meeting this standard. People who use the service, staff and visitors were not protected against the risks of unsafe or unsuitable premises. The CQC judged that this had a minor impact on people who use the service, and have told the provider to take action. The CQC asked the provider to send a report by 24 January 2014, setting out the action they will take to meet the standards. They will check to make sure that this action is taken. How the regulation was not being met: People were not protected against the risks of unsafe or unsuitable premises because adequate maintenance of the premises had not been maintained. (Regulation 15 (1) (c) (i)). Details of the actions taken will be included in the next quality report.

58
Provider Audited/Visited:
Princess Royal University Hospital
2-4 December 2013, 10 December 2013 – Inspection report published 6 February 2014
http://www.cqc.org.uk/sites/default/files/media/reports/20140205__cqc_princess_royal_university
_hospital_report_final.pdf (full report)
Name and Purpose of Audit/ Visit:
Unannounced inspection – CQC
This visit followed the new inspection model. All main areas of the trust were inspected including:
accident and emergency; medical care (older persons);surgery; intensive/critical care; maternity and
family planning; children’s care; end of life; outpatients. Five questions were asked.
Issues highlighted
Hand hygiene Staff identification Access to medical records and appointment delays PRUH consultant engagement and medical leadership Emergency department pathway Discharge arrangements poor Staffing levels within surgery Equipment shortages within maternity
Key Findings Are services safe? Many of the services are safe but some require improvements, including the A&E department, medical wards and the outpatient departments. There were long waiting times in A&E, inaccurate recording (on the medical wards) of some patients who were not for resuscitation. Lack of availability of medical records in some outpatient clinics meant some patient were either having their appointment cancelled on the day or undergoing fairly complex procedures without their full medical notes being available. Not all staff in all clinical areas were using the alcohol hand gel, and hand-washing sinks were not available in every area. Although some staff reported incidents, and the trust was putting in place arrangements to improve how it investigates incidents and providing feedback to staff, they did not always receive feedback about any action that had been taken.
Are services effective? Some areas such as the critical care unit were able to demonstrate that they provided effective care through the collection and analysis of data. However, we were unable to obtain this data for many areas. Other areas, such as the A&E department, had clinical pathways for managing patients with specific conditions but these were not always adhered to. Participation in audits was variable across the services and staff groups.
Are services caring? Patients and relatives were positive about the care they received and good interactions between staff and patients were observed. However, this was another area where limited data was available due to the recent acquisition. People who came to the listening event were generally positive about their experience of the hospital. Information from Bromley Healthwatch highlighted some areas of good practice and areas that needed improvement, including discharge planning.
Are services responsive to people’s needs? Many of the areas inspected need to improve how they respond to patients’ needs. The movement of patients through the hospital was hampered by delayed discharges, which in turn was causing pressure in the A&E department as well as other areas such as the critical care unit and theatres. Services had responded to complaints but there was very little information about learning and changes as a result of complaints.
Are services well-led? Many staff were positive about the hospital being acquired by King’s College Hospital NHS Foundation Trust and told us about recent improvements as a result. In some areas it was clear that some senior staff had not taken action to try and address some of the longstanding problems and staff told us that, until recently, there had been little support for them. Over the last few years, under the previous trust, the systems to monitor the quality of care provided have been significantly reduced.

59
Key actions agreed
By Whom By When
The CQC required the hospital to take the following actions to improve:
Engagement and support of all senior medical staff.
Ownership for improvement must be embedded at every level in the hospital.
The trust must address its discharge planning and patient flow problems and ensure all action is taken to minimise the risk of elective surgery being cancelled and improve capacity
The trust must take action to urgently address the long waiting times in the A&E department.
Problems with accessing and availability of medical records must be addressed urgently.
Nursing documentation, including fluid balance charts, must be accurately completed.
Decisions related to patients’ resuscitation status must be regularly reviewed and accurately recorded and shared with staff.
Develop and embed systems for monitoring performance, quality and safety of care at all levels in the hospital.
Ensure staff use the alcohol hand gel.
Training, appraisals and support for all staff.
Appropriate training and sufficient staff to provide care for children who require high dependency care and improved planning for elective surgery for children.
Recruitment of new staff should continue to ensure that reliance on bank (in-house overtime staff) and agency staff is reduced, and this should be prioritised by areas of greatest need.
KCH have drawn up an action plan which is being monitored by Southwark and Bromley CCGs.

60
Provider Audited/Visited:
St Mary’s Care Home
25 November 2013 – Reported 20th December 2013
Name and Purpose of Audit/ Visit:
Routine Inspection - CQC
Description of Audit / Visit and Key Findings
St Mary’s Care Home is a nursing home located in Tooting Bec, with 39 nursing beds.
The CCG currently has two residents in the home. It is not on the current AQP list.
The CQC service found there were procedures in place to identify whether people
using the service had the capacity to make decisions about their care. Where
people did have capacity they were involved in their care planning and
identification of their support needs. The provider liaised with a person’s relative
to discuss care needs if the person was unable to do this themselves. Care plans
were put in place with information about how to support a person to maintain
their safety and welfare. The care planning process addressed people’s physical
and mental health, their social needs, and their spirituality. The provider liaised
with other health and social care professionals to ensure people were provided
with the care and treatment they required. The service liaised with specialists for
advice and further support if they had concerns about a person’s health. Staff felt
well supported and there were supervision processes in place to regularly discuss
their performance. Staff received a range of training and were able to attend
additional training to ensure they had the skills and knowledge to support people
using the service and aid career progression. The manager regularly took time to
speak with the people using the service, their relatives and the staff to obtain
feedback about the service and identify areas for development. There were
processes in place to manage and monitor complaints and incidents. One person
using the service told CQC, “I’m very thankful to be here.” Another person said,
“The staff are very kind.”
The following standards were inspected and found to have been met:
Respecting and involving people who use services
Care and welfare of people who use services
Safety and suitability of premises
Staffing
Complaints

61
Provider Audited/Visited:
Marie Curie Nursing and Domiciliary Care Service
18 November 2013 – Reported 5 February 2014
Name and Purpose of Audit/ Visit:
Unannounced Inspection – CQC
Description of Audit / Visit and Key Findings
Marie Curie Nursing and Domiciliary Care Service [MCNS] provides a nursing and personal care service to people who are ill with life limiting or terminal illnesses and wish to be cared for in their own home. The service operates nationwide and has a network of 2115 Marie Curie Nurses and healthcare assistants who provide the service. In 2013 Marie Curie Nursing Services cared for 30,000 people up to the end of November 2013. The CQC looked at the personal care or treatment records of people who use the service and checked how people were cared for at each stage of their treatment and care and spoke with one or more advocates for people who use services. They talked with people who use the service, carers and / or family members, staff and reviewed information given to them by Marie Curie Cancer Care, commissioners of services, other regulators and the Department of Health, reviewed information sent by local groups of people in the community or voluntary sector and talked with other authorities. The CQC spoke with 42 people who had experience of Marie Curie Nursing and Domiciliary Care Services, 6 were people currently using the service, and 36 were close relatives of people who had received the service from MCNS. People’s views and experiences were taken into account in the way the service was provided and delivered in relation to their care. Care and treatment was planned and delivered in a way that was intended to ensure people's safety and welfare. MCNS staff worked closely with statutory services in order to deliver appropriate care to people in their own homes. A person caring for their terminally ill parent said "I am very happy with the way they look after my mother, the first night’s sleep I’ve had in weeks." A person who was cared for by their spouse said "I am extremely pleased with the way the nurses look after me. They are very professional. My wife is not a patient, but the nurses also give her some help because she is so weary caring for me." A district nurse told us, “I have worked closely with MCNS staff for many years, I find staff from MCNS particularly good in their roles, they all seem so capable and competent, they adapt to each individual situation appropriately and provide the emotional and practical support people require."
The following standards were inspected and found to have been met: Respecting and involving people who use services – people should be treated
with respect, involved in discussions about their care and treatment and able to influence how the service is run.
Care and welfare of people who use services – people should get safe and appropriate care that meets their needs and supports their rights.
Supporting workers – staff should be properly trained and supervised, and have the chance to develop and improve their skills.
Assessing and monitoring the quality of service provision – the service should have quality checking systems to manage risks and assure the health, welfare and safety of people who receive care.

62
Provider Audited/Visited:
St Thomas’s Hospital (GSTFT)
11-12 November 2013 – Inspection report published on 21 December 2013
Name and Purpose of Audit/ Visit:
Unannounced inspection - CQC
Description of Audit / Visit and Key Findings
The focus of this inspection was patients who were being admitted for, or had undergone, surgery. The CQC visited the pre-assessment clinic, the surgical admissions lounge, the main operating theatres, the recovery room, three surgical wards and the Intensive Care Unit. They spoke with 16 patients and two relatives and met staff of different professions.
Patients told the CQC they were provided with the information they needed to consent to surgery. When appropriate, mental capacity was assessed and decisions about treatment agreed by a multi-disciplinary team. The effectiveness of the treatment of surgical patients was enhanced by putting in place an individualised care pathway at an early stage. The risks of giving unsafe treatment were reduced by appropriate preparation for surgery and by communication between the members of the theatre teams. Patients were monitored closely in the recovery room and on the wards after their operation. Nursing staff were observed to be responsive to patients’ needs and one patient told the CQC, “They’re always popping in.” Patients said that ward staff were “friendly and informative”. The professions on the wards worked together to make sure patient discharge was prompt and safe. Surgical patients were protected from the risks of dehydration and inadequate nutrition by appropriate monitoring and risk assessments. Staff in theatres, the Intensive Care Unit and the wards said they had the equipment required to monitor patients and to provide care and treatment. The CQC saw that equipment was well maintained. There was an effective system for monitoring the quality of service provision. This included systems for investigating incidents and complaints, and communicating lessons learned. There were regular audits to look at service performance and appropriate action plans were put in place to address any areas for improvement.
The following standards were inspected and found to have been met:
Consent to care and treatment
Care and welfare of people who use services
Meeting nutritional needs
Safety, availability and suitability of equipment
Assessing and monitoring the quality of service provision
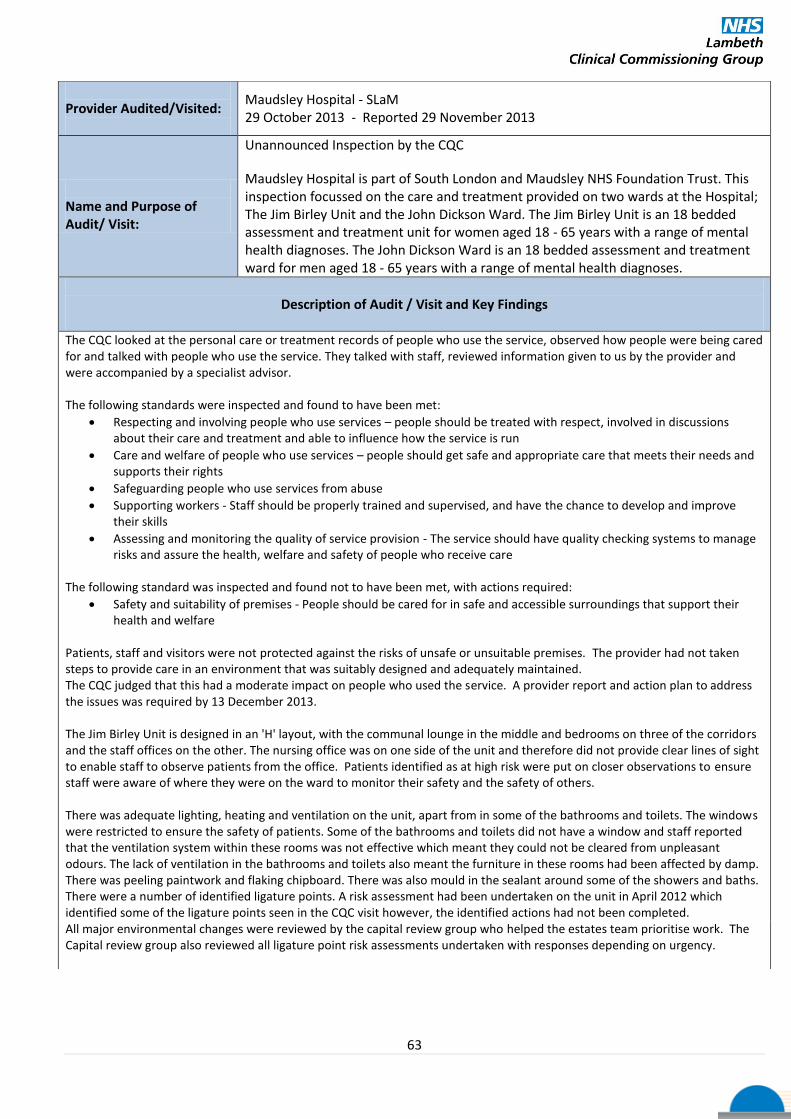
63
Provider Audited/Visited:
Maudsley Hospital - SLaM 29 October 2013 - Reported 29 November 2013
Name and Purpose of Audit/ Visit:
Unannounced Inspection by the CQC
Maudsley Hospital is part of South London and Maudsley NHS Foundation Trust. This inspection focussed on the care and treatment provided on two wards at the Hospital; The Jim Birley Unit and the John Dickson Ward. The Jim Birley Unit is an 18 bedded assessment and treatment unit for women aged 18 - 65 years with a range of mental health diagnoses. The John Dickson Ward is an 18 bedded assessment and treatment ward for men aged 18 - 65 years with a range of mental health diagnoses.
Description of Audit / Visit and Key Findings
The CQC looked at the personal care or treatment records of people who use the service, observed how people were being cared for and talked with people who use the service. They talked with staff, reviewed information given to us by the provider and were accompanied by a specialist advisor. The following standards were inspected and found to have been met:
Respecting and involving people who use services – people should be treated with respect, involved in discussions about their care and treatment and able to influence how the service is run
Care and welfare of people who use services – people should get safe and appropriate care that meets their needs and supports their rights
Safeguarding people who use services from abuse
Supporting workers - Staff should be properly trained and supervised, and have the chance to develop and improve their skills
Assessing and monitoring the quality of service provision - The service should have quality checking systems to manage risks and assure the health, welfare and safety of people who receive care
The following standard was inspected and found not to have been met, with actions required:
Safety and suitability of premises - People should be cared for in safe and accessible surroundings that support their health and welfare
Patients, staff and visitors were not protected against the risks of unsafe or unsuitable premises. The provider had not taken steps to provide care in an environment that was suitably designed and adequately maintained. The CQC judged that this had a moderate impact on people who used the service. A provider report and action plan to address the issues was required by 13 December 2013. The Jim Birley Unit is designed in an 'H' layout, with the communal lounge in the middle and bedrooms on three of the corridors and the staff offices on the other. The nursing office was on one side of the unit and therefore did not provide clear lines of sight to enable staff to observe patients from the office. Patients identified as at high risk were put on closer observations to ensure staff were aware of where they were on the ward to monitor their safety and the safety of others. There was adequate lighting, heating and ventilation on the unit, apart from in some of the bathrooms and toilets. The windows were restricted to ensure the safety of patients. Some of the bathrooms and toilets did not have a window and staff reported that the ventilation system within these rooms was not effective which meant they could not be cleared from unpleasant odours. The lack of ventilation in the bathrooms and toilets also meant the furniture in these rooms had been affected by damp. There was peeling paintwork and flaking chipboard. There was also mould in the sealant around some of the showers and baths. There were a number of identified ligature points. A risk assessment had been undertaken on the unit in April 2012 which identified some of the ligature points seen in the CQC visit however, the identified actions had not been completed. All major environmental changes were reviewed by the capital review group who helped the estates team prioritise work. The Capital review group also reviewed all ligature point risk assessments undertaken with responses depending on urgency.

64
Provider Audited/Visited:
Limetrees Care Centre
17 October 2013 – Reported 11 December 2013
Name and Purpose of Audit/ Visit:
Routine Inspection - CQC
Description of Audit / Visit and Key Findings
Limetree Care Centre is a purpose built care home located in Tulse Hill, South West
London. There are 92 bedrooms, all of which have en-suite facilities. Limetree Care
Centre provides residential and nursing care for older people, some of whom may
have dementia. Lambeth CCG currently fund 6 residents.
The CQC found the service was well organised and there were sufficient staff to care
for people's individual needs. The relatives of the people they spoke with were happy
with the home and told that CQC that their family members were well looked after.
There was evidence of good care during the morning activities ranging from
supervised breakfast with a choice of menu to the daily activities such as music,
massage, crocheting and reading. The people the CQC spoke to said they enjoyed the
food and there was evidence of choice in the menu together with the facility for
special requests. A person said, "They always fetch a good meal here". The care
planning was found to be systematic and detailed with evidence of people
contributing to their care plans. The CQC saw that staff dealt with an emergency and
made prompt arrangements for the transfer of the person to hospital. The staff
spoken to had access to a wide range of training which was monitored ensuring that
statutory training was completed. The majority of the people spoken to were happy
with the service and felt able to raise their concerns with the staff or the Manager.
There was evidence that the complaints were fully investigated and that change to
practice took place as a result of complaints.
The following standards were inspected and found to have been met:
Respecting and involving people who use services
Care and welfare of people who use services
Safety and suitability of premises
Staffing
Complaints
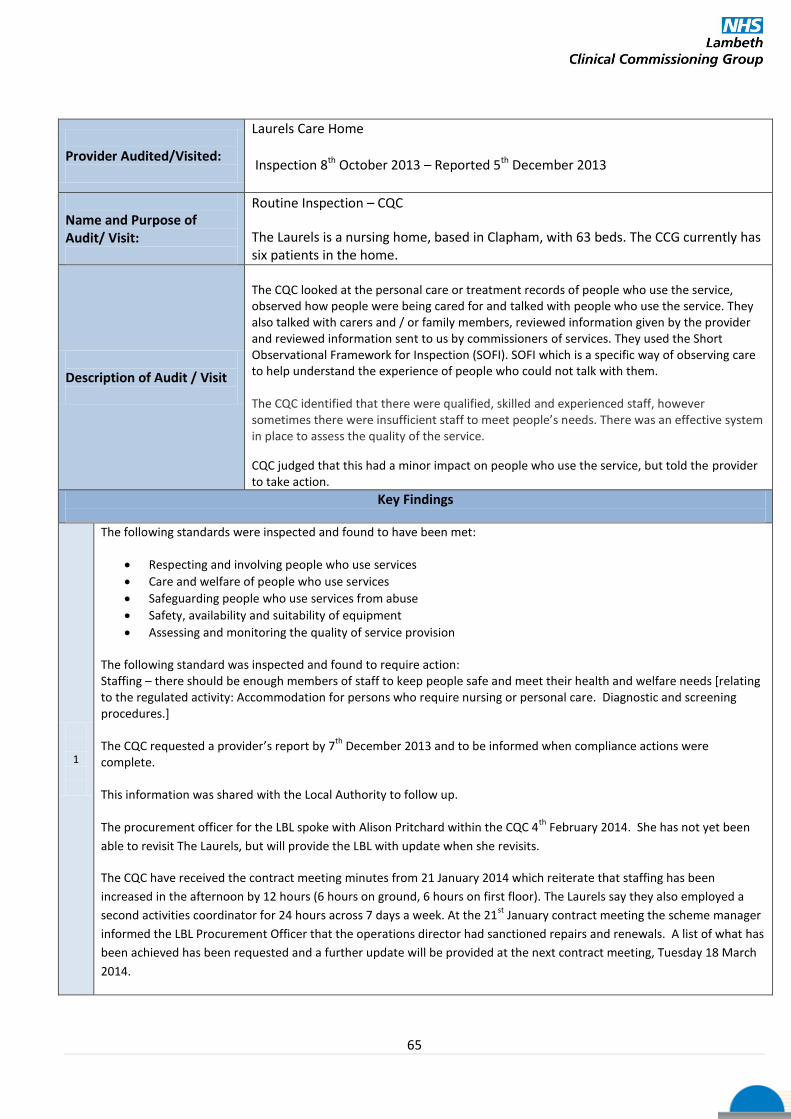
65
Provider Audited/Visited:
Laurels Care Home
Inspection 8th October 2013 – Reported 5th December 2013
Name and Purpose of Audit/ Visit:
Routine Inspection – CQC
The Laurels is a nursing home, based in Clapham, with 63 beds. The CCG currently has six patients in the home.
Description of Audit / Visit
The CQC looked at the personal care or treatment records of people who use the service, observed how people were being cared for and talked with people who use the service. They also talked with carers and / or family members, reviewed information given by the provider and reviewed information sent to us by commissioners of services. They used the Short Observational Framework for Inspection (SOFI). SOFI which is a specific way of observing care to help understand the experience of people who could not talk with them. The CQC identified that there were qualified, skilled and experienced staff, however sometimes there were insufficient staff to meet people’s needs. There was an effective system in place to assess the quality of the service.
CQC judged that this had a minor impact on people who use the service, but told the provider to take action. There should be enough members of staff to people needs
Key Findings
1
The following standards were inspected and found to have been met:
Respecting and involving people who use services
Care and welfare of people who use services
Safeguarding people who use services from abuse
Safety, availability and suitability of equipment
Assessing and monitoring the quality of service provision
The following standard was inspected and found to require action: Staffing – there should be enough members of staff to keep people safe and meet their health and welfare needs [relating to the regulated activity: Accommodation for persons who require nursing or personal care. Diagnostic and screening procedures.] The CQC requested a provider’s report by 7
th December 2013 and to be informed when compliance actions were
complete. This information was shared with the Local Authority to follow up. The procurement officer for the LBL spoke with Alison Pritchard within the CQC 4
th February 2014. She has not yet been
able to revisit The Laurels, but will provide the LBL with update when she revisits.
The CQC have received the contract meeting minutes from 21 January 2014 which reiterate that staffing has been
increased in the afternoon by 12 hours (6 hours on ground, 6 hours on first floor). The Laurels say they also employed a
second activities coordinator for 24 hours across 7 days a week. At the 21st
January contract meeting the scheme manager
informed the LBL Procurement Officer that the operations director had sanctioned repairs and renewals. A list of what has
been achieved has been requested and a further update will be provided at the next contract meeting, Tuesday 18 March
2014.

66
Provider Audited/Visited:
St Georges Healthcare NHS Trust - Tooting 15-17 August 2013 - Reported 24 October 2013
Name and Purpose of Audit/ Visit:
Routine Inspection –CQC
Description of Audit / Visit and Key Findings
The CQC visited Accident and Emergency Department, Paediatrics, Stroke Unit, Senior Health Wards, Renal Unit, Richmond Ward, Thomas Young Ward, Trevor Howell Ward and Day Unit, Ruth Myles Ward, Caroline Ward, Vernon Ward and Gray Ward looking at the personal care or treatment records of people who use the service. Patients and relatives felt they were given enough information and were involved in decisions about their care. The CQC saw that patients were in general being treated with respect but identified that the dignity and privacy of patients on the Trevor Howell Ward and Day Unit was not always being respected. Most of the areas visited were visibly clean and improvements had been made since the previous CQC visit. Medication records were up to date but there were concerns identified with the monitoring of the temperature of fridges and medication storage areas on some wards. The trust provided evidence that they had identified these issues before the CQC inspection but had not fully implemented the action plan. On the majority of wards the CQC visited the care plans were current and patient focused but on Caroline ward the CQC identified issues with the individualisation of the plans. The majority of patients the CQC team spoke with were happy with the food being provided and there appeared to be systems in place to identify patients who needed additional support during mealtimes. Most wards had adequate levels of staff but the CQC identified concerns regarding staffing levels on the Thomas Howell Ward and Day Unit. During our visit the CQC saw that the trust had suitable systems in place to assess and monitor the quality of care being provided. The records on Brodie Ward and Caroline Ward were found to be incomplete and did not protect patients from the risks of unsafe or inappropriate care and treatment. The following standards were inspected and found to have been met:
Respecting and involving people who use services
Care and welfare of people who use services
Meeting nutritional needs
Cleanliness and infection control
Assessing and monitoring the quality of service provision The following standards were inspected and found to require action:
Management of medicines
Staffing
Records

67
Key actions agreed –to be reviewed at SGH CQRG 18 Dec 2013
By Whom By When
1
Management of medicines Pharmacy Department to lead and manage a thermometer calibration service for all drugs fridges. Standard Operating Procedures to be implemented to cover temperature monitoring, action in response to out of range readings, de-frosting, Ward Manager sign-off and escalation process. Existing quarterly meetings between Pharmacy and Ward Managers to have drug fridge monitoring on their agenda so that it becomes embedded into everyday clinical practice. Compliance will be monitored through existing medication safety visits, audit of safe and secure handling of medicines and included in the quarterly review meeting between the ward manager and ward pharmacist.
Chris Evans, Chief Pharmacist
St Georges CQRG End Dec 2013
2
Staffing Co-ordinated and prioritised recruitment campaign to fill all vacancies developed. Recruitment actions now all completed but ongoing actions as part of a retention plan. Status at 6.11.13: Trevor Howell Day Unit: one outstanding post - to be filled by end of Nov 2013 Trevor Howell ward: 3 band 6s still vacant but to be filled by end of Jan 2014. Staffing levels will be assessed and recorded daily and reported to Head of Nursing. Monitoring of PALS enquiries / comments, complaints, friends & family test, vacancy levels, staff turnover.
Alison Hughes.
Divisional Director of Nursing.
Medicine & Cardiovascular
St Georges CQRG
End Jan 2014
3
Records (1) Daily review of 6 sets of nursing records at 14.00 by nurse in charge. In the event that a patient has triggered on Early Warning Score (EWS) the nurse in charge will review the medical notes to ensure appropriate escalation has occurred Ward sister reviewing nursing documentation on a daily basis as part of the handover process Quality ward rounds completed regularly by senior staff which includes a review of EWS scores and documentation. EWS competencies to be re-assessed EWS to be a regular item on the neurosciences education programme Performance management of staff who fail to meet competency.
Helene Anderson
Divisional Director of Nursing. Surgery, Theatres, Neuro & Cancer
St Georges CQRG
End Dec 2013
68
4
Records (2) Identified concerns with documentation discussed widely at team and care group meetings to raise awareness. Monthly documentation audits in place. Spot checks of documentation during senior nurse quality rounds. Pathways being created for conditions often associated with thoracic procedures / illnesses that can be individualised. Staffing levels reviewed and establishment increased to enable less reliance on bank and agency. Electronic documentation being introduced Feb 2014.
Alison Hughes.
Divisional Director of Nursing.
Medicine & Cardiovascular
St Georges CQRG
End of Dec 2013 End of Feb 2014
(Electronic documentation)
69
http://www.cqc.org.uk/directory/1-144273944
Trinity Hospice: Inspection Report published 11 February 2014
We use this facility – patients in and out – numbers not kept

70
Section 9: Quality Surveillance Group (QSG) Update
QSGs were set up in response to the Francis Enquiry and the new commissioning landscape that was created post
April. There was recognition that because of the different structures that had been created there was a danger that
quality could suffer through lack of clarity as to whose role it was to address quality issues. By collectively
considering and triangulating information and intelligence, QSGs will work to safeguard the quality of care that
people receive. The group’s membership consists of Chief Officers of CCGs, Monitor, the TDA, CQC, HealthWatch
and the CSU.
QSG Trust templates
The meeting was the first using the new format of commissioner completed templates highlighting
positive aspects of provider quality performance and areas for improvement. Key issues to note on a
Trust basis detailed below:
Kings College Hospital
Safety:
• Kings methodology for reviewing SIs now rolled out to PRUH site with reporting rates for SIs noted to be
increasing.
• Funding for additional staff posts to a) bring to safe levels and b) introduce specialist posts such as tissue
viability.
• Some problems identified in recruiting staff. The CQC and NHSE reports outline issues in ED.
• It was recognised that there is a need for better engagement with local stakeholders (community provider
and local authority) around pressure ulcers.to collate information to analyse what data is being looked at and
which areas can be benchmarked.
Effectiveness:
Relevant targets are being robustly reported
Engagement in development of Quality Account priorities
Demonstrable adherence to NICE guidance and other national or London standards to demonstrated
through CQRG
Experience
Engagement events with Bromley public (recruiting governors, CQC inspection)
Culture
Nursing culture consistently reported as good and enthusiastic
Open reporting and discussion at CQRG.
Engagement of medical consultant colleagues remains a challenge.
Guys & St Thomas’ Hospitals
Safety:
Cancer first treatment 62 days screening – October 71% against performance tolerance of 85%.
Infection control – Cdiff within targets. MRSA – The Trust has reported 2 cases ytd (to November 2013 ) 1 in
April and 1 in July.
71
MRSA screening on admission 98% against target of >95% for October.
The number of serious patient falls is low (benchmarking against Shelford Group). Falls is a clinical theme in
SLIC.
Effectiveness:
Diagnostic waits require improvement
Cancer first treatment 62 days screening – October 71% against performance tolerance of 85%
Community nursing and health visiting productivity and quality. District Nurse and health visiting recruitment in
inner city London continues to be a challenge.
Quality Alerts relating to GSTT mainly concern DN non attendance, discharge summaries and requests for GPs to
follow up results requested by GSTT staff.
Experience
GSTT have amended pressure ulcer investigations so that the patient / family get a copy of an investigation
within 10 working days of any incident rather than the 45 working day grade 1 serious incident report timescale.
Community services moving from annual to near-time patient experience feedback.
Culture
District Nursing action plan being followed up at contract meetings
GSTT continuing to work with staff to improve staff understanding of incident investigations and root cause
analysis.
Lambeth CCG is continuing to work with GSTT Patient Safety Team to speed up RCAs.







