
Prof. Dr.dr.Hertanto W Subagio,MS,SpGK (K)• Tempat dan tanggal lahir : Semarang, 20 Pebruari 1954
• Institusi asal :
- Universitas Diponegoro , Fakultas Kedokteran, Departemen Ilmu Gizi Klinik
• Pendidikan :
- Dokter Umum - 1979
- Doktor Ilmu Kedokteran-2002
- Sp Gizi Klinik Konsultan – 2004
- Guru Besar Ilmu Gizi - 2006
• Riwayat Pekerjaan :
- Dosen FK Undip 1980 – sekarang.
- WD1 FK Undip : 2007-2010
- WR1 Undip : 2001-2015
- Majelis Wali Amanah Undip 2016 - 2020
- Wakil Ketua II PP Perhimpunan Dokter Gizi Klinik Indonesia 2015-2018
- Ketua Kolegium Gizi Klinik Indonesia 2019-2021.

Physiology and Metabolic Change in Geriatric-
Its Influence on Nutritional Therapy
Prof.Dr.dr.Hertanto W.S,M.S,Sp.GK (K)

CHANGES ASSOCIATED WITH AGEING
•Physiological Changes
•Socio Psychological Changes
CHANGES ASSOCIATED WITH AGEING
Physiological Changes
Socio Psychological Changes

Physiological Changes
• Diminished sense of taste and smell
• Impaired hearing and failing vision
• Loss of Teeth
• Decreased Neuromuscular coordination
• Anorexia
• Physical Discomfort
• Change in Body Composition
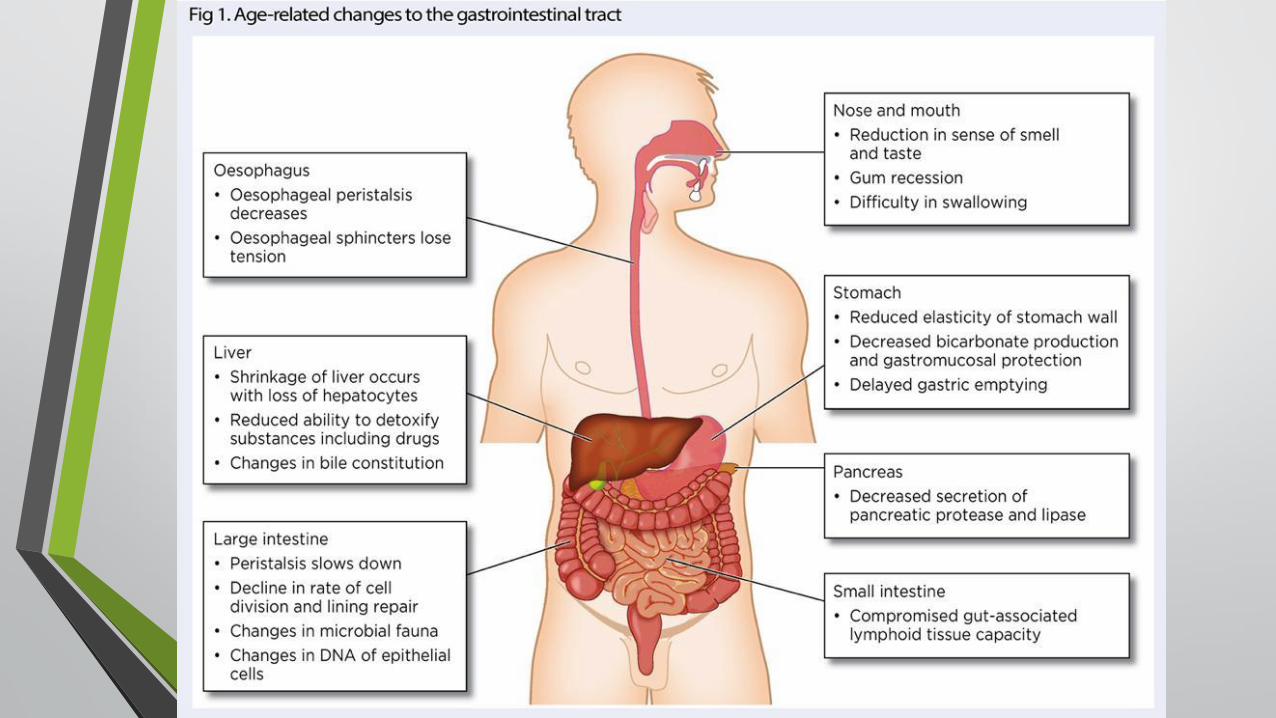
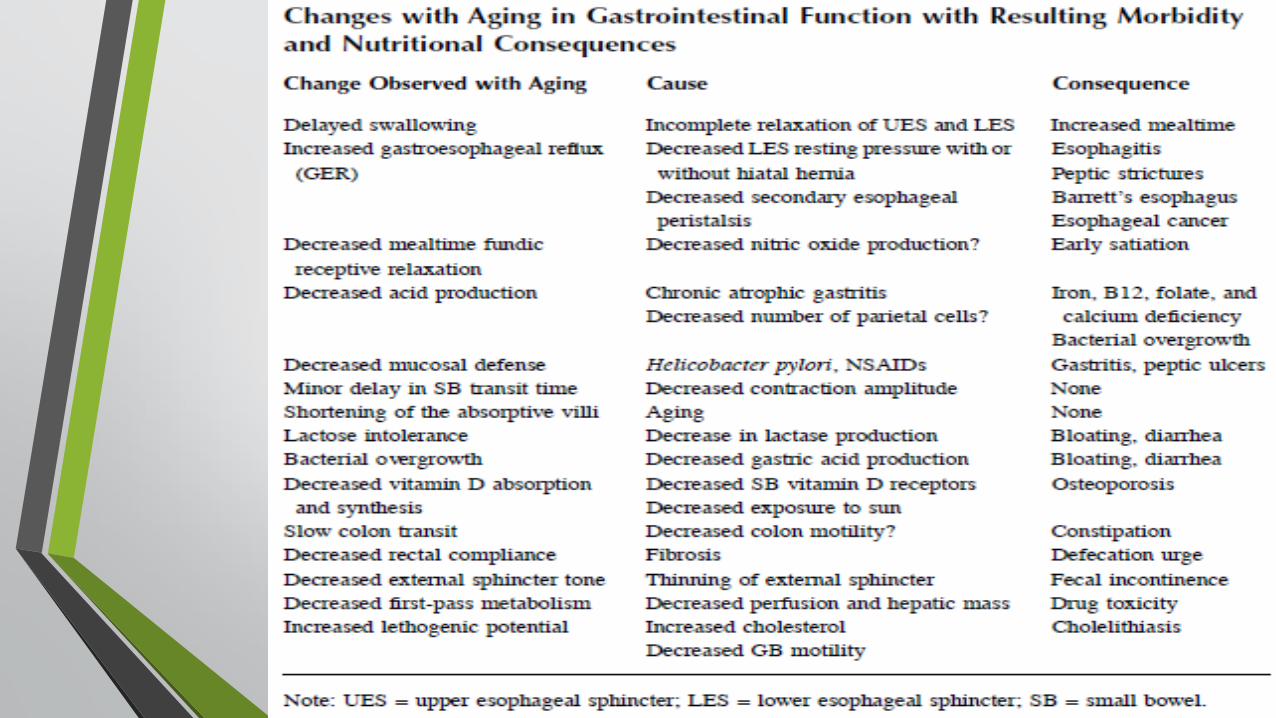
• Change in gastro-intestinal tract
• Change in cardiovascular system
• Change in respiratory function
• Change in respiratory function
• Change in skeletal tissue
Socio Psychological Changes
• Food habit
• Economic aspects
• Loneliness
• Lack of nutritional knowledge
•Depression
• Anxiety
• Loss of self-esteem
• Loss of independence

Declines in physiological function with aging.

Age-related changes in body composition, food intake
and energy expenditure.

Factors influencing nutritional inadequacy in the elderly population
Physiologic Pathologic Sociologic Psychologic
Decreased taste Dentition Ability to shop for food Depression
Decreased smell Dysphagia,swallowing problems Ability to prepare food Anxiety
Dysregulation of satiation
Diseases ( cancer, CHF, COPD,diabetes, ESRD, thyroid )
Financial status low socioeconomic
Loneliness
Delayed fastricemptying
Medications ( diuretic, antihypertensive, dopamine agonist, antidepressant, antibiotic, antihistamine )
Impaired activities of daily living skills
Emotionally stressful life events
Decreased gastric acid Alcoholism Lack of interactions with others at mealtime
Grief
Decreased lean body mass
Dementia Dysphoria
CHF : congestive heart failure ; COPD : Chronic Obstructive Pulmonary Disease ; ESRD : End Stage Renal Disease

Mechanisms of Anorexia of Aging
1. Smell and Taste
2. Hormones
3. Gastrointestinal Function
4. Inflammation
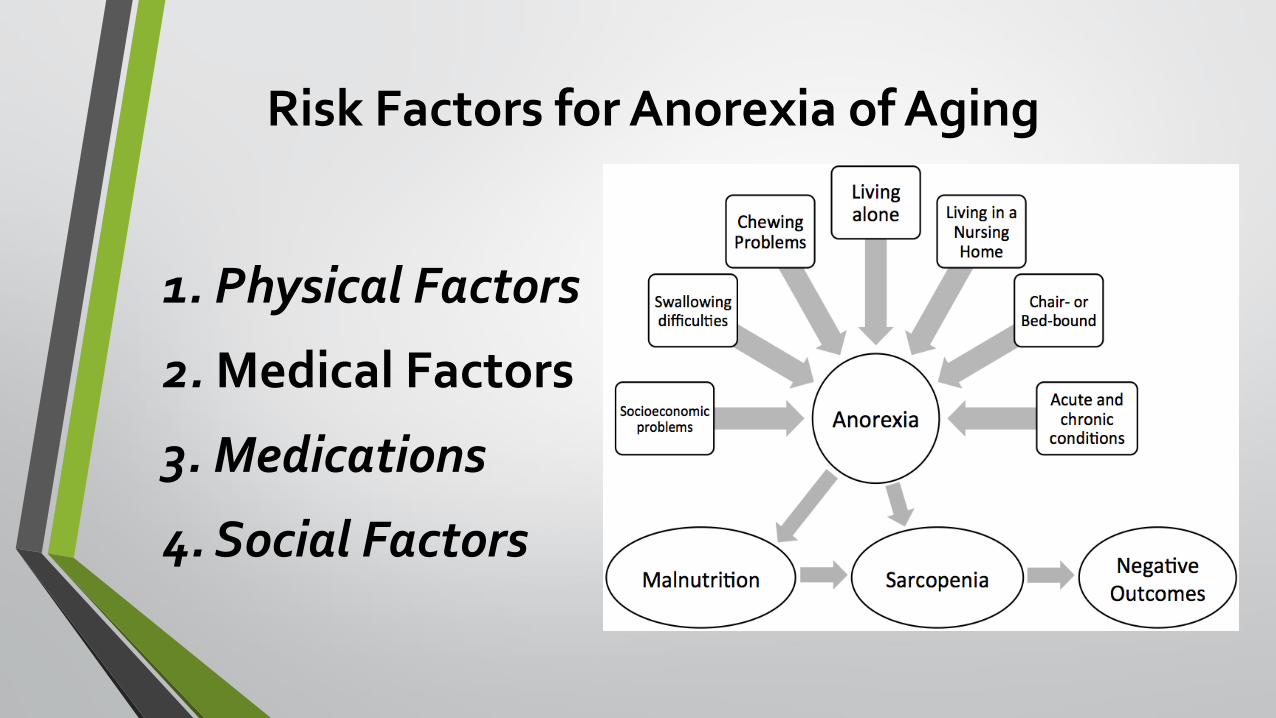
Risk Factors for Anorexia of Aging
1. Physical Factors
2. Medical Factors
3. Medications
4. Social Factors

Source : Adapted from Pilgrim et al (2015)
Hormone Produced by Function Change with age
Ghrelin Stomach in response to fasting
Increase appetite Secretion decreases ( Di Francesco et al, 2008)
Peptide tyrosine tyrosine ( PYY )
Ileum and colon in response to food intake
Supresses appetite Level increase ( Hickson et al, 2016)
Cholecystokinin ( CCK) Small intestine in response to presence of fat and protein
Supresses appetite Secretion increases ( de Boer et al,2013) and responsiveness to it increases
Insulin Pancreas in response to high blood glucose
Supresses appetite Production decreases, effect declines ( Gong and Muzumdar,2012 )
Leptin Adipose tissue ( secretion linked to body mass index )
Inhibits hunger Levels are believed to rise (( de Boer et al,2012) but evidence is conflicting
Age-related changes in appetite hormones

Nutritional Requirement for Elderly

Energy
• Energy requirement reduces
• Basal metabolic rate decreases (15-20%) due to reduced muscle mass and other metabolically active tissue mass.
• Reduced physical activity
• Increase in fatty tissue
Carbohydrate
• Requirement reduces.
• Impaired glucose intolerance can lead to hypoglycemia, hyperglycemia, and type II diabetes mellitus.
• Insulin sensitivity can be enhanced by balance energy intake, weight management and regular physical activity.

Protein
• Decreased skeletal tissue mass.
• Decrease in store of protein is inadequate to meet the need of protein synthesis.
• Intake of 1.0 g/kg is safe during old age.
• Consume less protein which may lead to edema, anemia, and low resistance to infections.

Lipid
• Dementia and CVD may share risk factors like high intake of dietary total fat.
• Emphasis should be placed on reducing the intake of saturated fat and choosing mono saturated or poly saturated fat sources.
• Sufficient intake of ω-3 fatty acids helps in visual acuity, hair loss, tissue inflammation, improper digestion, poor kidney function and mental depression.

Calcium
• Elderly : Total intake decreases
• Ca absorption decreases after age 65
•May increase Ca RDI for elderly :
1200 mg/d - elderly men, and
women over age 70

Iron (Fe)• Iron deficiency anemia less
common in older adults
•Deficiency due to inadequate intake or reduced non heme iron absorption secondary to hypochlorhydria of atrophic gastritis
•Deficiencies linked to chronic blood loss from disease/medications; poor Fe absorption

Zinc (Zn)
• Deficiency due to low intake, leading to reduced immune function
• Low-dose (20 mg/d) zinc supplementation allows restoration, at least partially of nutritional status (Boukaiba, 1993)

Vitamin D
• Elderly are at risk of Vitamin D deficiency due to decreased exposure to sunlight or decrease in renal mass.
•Dietary supplements with calcium and vitamin D improves bone density and prevent fractures.

Vitamin C
• The antioxidant vitamins such as vitamin C, carotinoids and vitamin E enhances health of elderly.
• Stress, smoking, and medication can increase vitamin C requirement.
• Vitamin C may be protective against cataract at an intake level of b/w 150-250 mg/day.
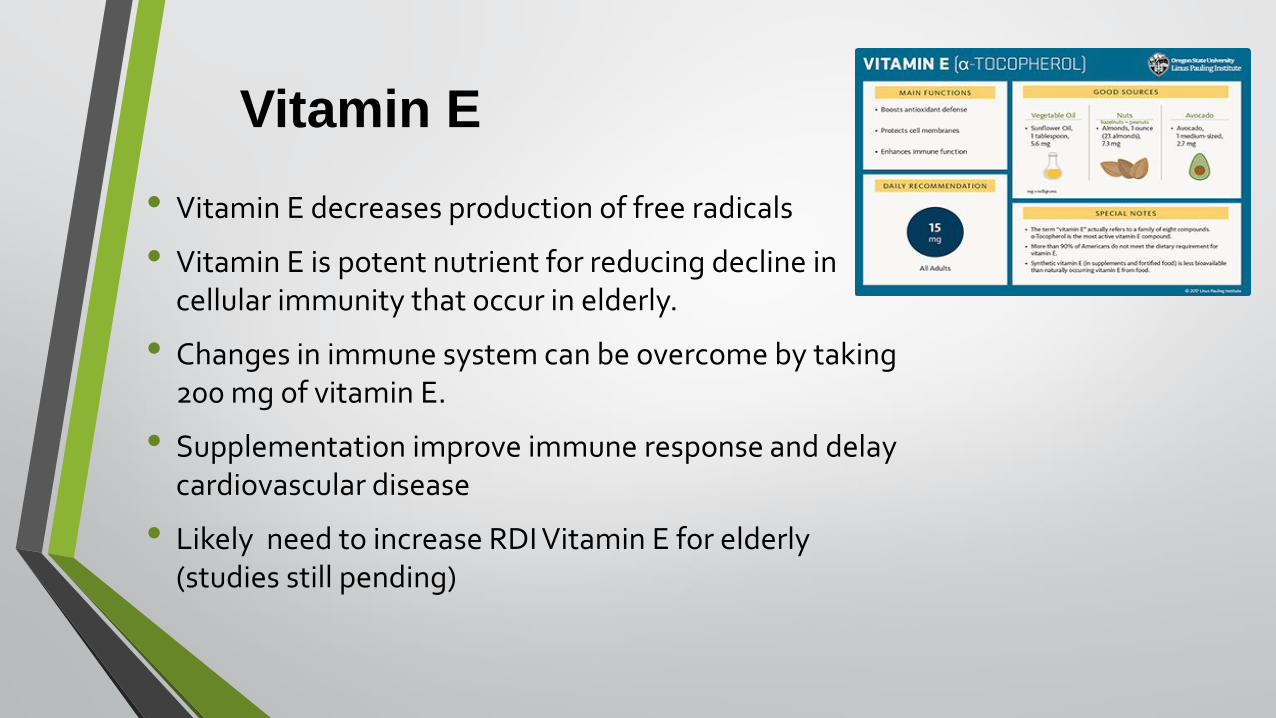
Vitamin E
• Vitamin E decreases production of free radicals
• Vitamin E is potent nutrient for reducing decline in cellular immunity that occur in elderly.
• Changes in immune system can be overcome by taking 200 mg of vitamin E.
• Supplementation improve immune response and delay cardiovascular disease
• Likely need to increase RDI Vitamin E for elderly (studies still pending)
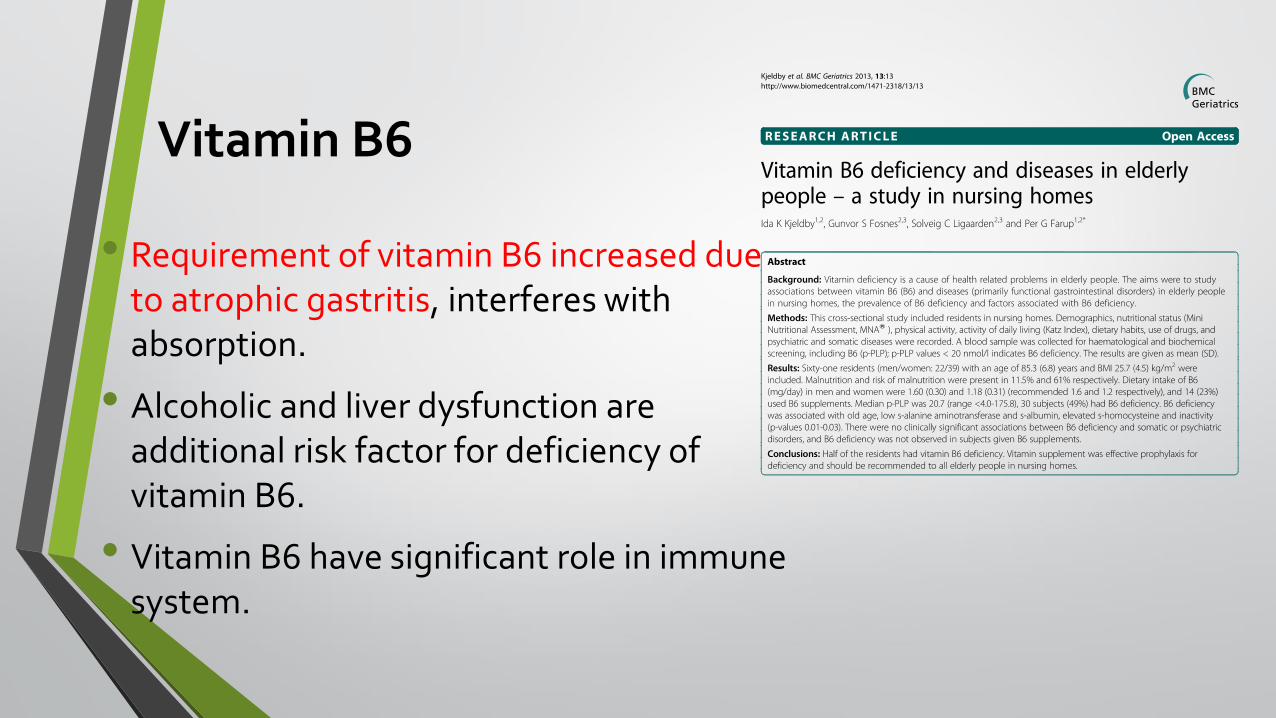
Vitamin B6
• Requirement of vitamin B6 increased due to atrophic gastritis, interferes with absorption.
• Alcoholic and liver dysfunction are additional risk factor for deficiency of vitamin B6.
• Vitamin B6 have significant role in immune system.

Folate & Vitamin B12
• Atrophic gastritis decreases absorption of folate
• Alcoholism is a risk factor for folate deficiency.
• Severe deficiency of folic acid may result macrocytic anemia and elevated serum homocystein level which is a risk for cardiac diseases.
• Consumption of folate rich food is needed. RDI may increase for elderly (400 mg)
• Causes for vitamin B12 deficiency are atrophic and bacterial overgrowth, which decreases absorption and leads to pernicious anemia.

Water
• Dehydration goes unrecognized, result of
• decreased thirst sensitivity
• immobility
• Inadequate intake leads to
• Dehydration
• Hypertension
• Elevated BP
• Constipation
• Nausea and vomiting
• Dryness of mucosa
• Decreased urine excretion
• Mental confusion
Conclusion: A range of effective interventions is available to support adequate nutrition and hydration in older persons in order to maintain or improve nutritional status and improve clinical course and quality of life. These interventions should be implemented in clinical practice and routinely used.

Summary of the nutrient concerns of aging

Modified My Pyramid for Older Adults

Terima Kasih







