
Product PortfolioPrimary IOLs

Reliable optical outcomes and a low rate of post-operative complications
Rayner’s Anti-Vaulting Haptic (AVH) Technology® provides proven rotational and centrational stability, and excellent fixation in the capsular bag1
• Superb centration
– Maximum offset of only 1mm 3 months after surgery2
• Excellent rotational and torsional stability2
Optimal visual quality in all lighting conditions
Aspheric optic technology reduces spherical aberration:3,4
• Excellent contrast sensitivity and retained depth of field from aberration-neutral aspheric optic3,4
• Available in two optic sizes; 5.75mm or 6.25mm
When considering an intraocular lens, what’s important to you?
0
1
2
3
4
5
6
7
8
9
10
3 months1 month1 week1 day
Lens
rota
tion
(deg
rees
)
2.072.51
3.553.11
Post operative assessmentsAdapted from Reference 2.
Only 3 degrees difference between planned toric IOL axis and post-operative outcomes at 3 months
Rayner Primary IOL Platform

Peace of mind with low rates of posterior capsular opacification (PCO)
Rayner’s 360° Amon-Apple Enhanced Square Edge creates a physical barrier to prevent epithelial cell migration7
An IOL free from vacuoles and glistenings8
• Single piece IOLs created from Rayacryl®
• Compressible material for delivery through a small incision
• Excellent handling characteristics with controlled unfolding within the capsular bag
• Low silicone oil adherence9
• Excellent uveal biocompatibility16
• Hydrophilic acrylic material with low inflammatory response10
• Low refractive index (1.46) linked to low incidence of glare and external reflections17
ND:YAG CAPSULOTOMY RATES7 MEAN TIME TO ND:YAG CAPSULOTOMY7
At 12 months 0.6% 9.3 ± 5.5 months
(range 2.6 - 22.7 months)
Follow-up period: 5.3 – 29 monthsAt 24 months 1.7%
Study of 3,461 patients receiving Rayner C-flex 570C IOLs over a 24 month period, Nd:YAG capsulotomy rates were
extremely low and comparable with hydrophobic acrylic lenses with square-edge optics.7
Ray
ner I
OL
Pla
tform
C-flex® AsphericSuperflex® Aspheric
T-flex® Aspheric
M-flex® Aspheric
M-flex® T
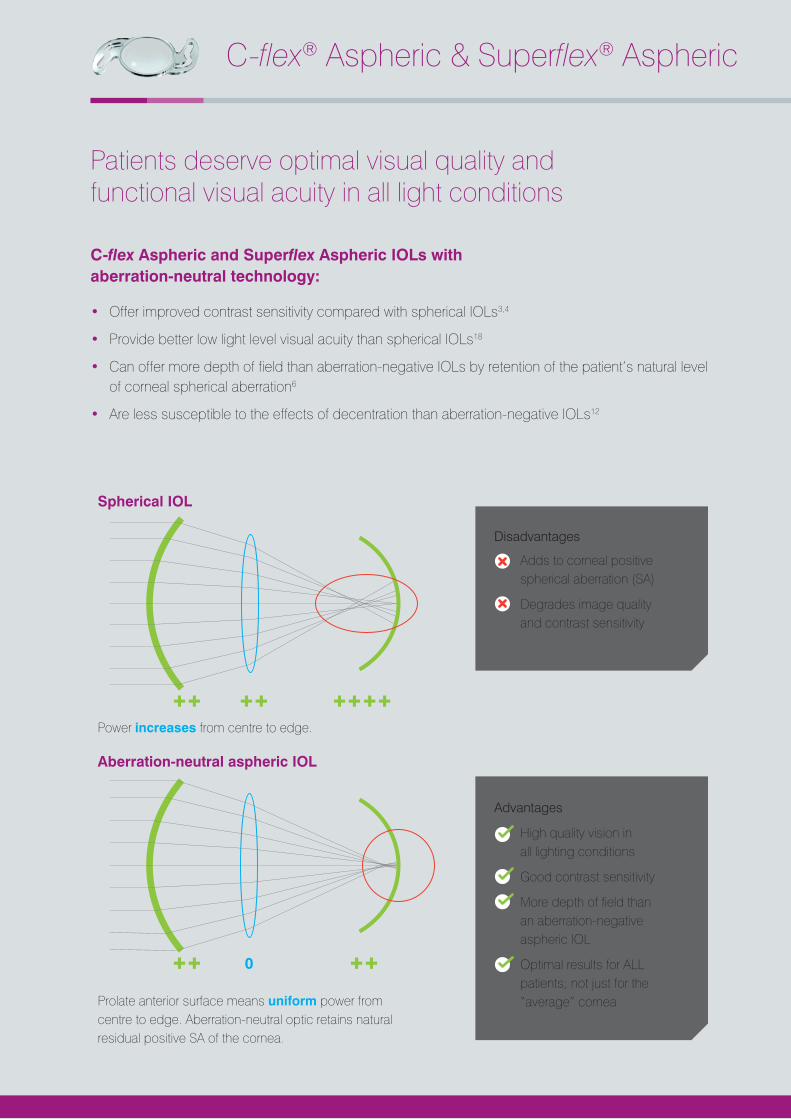
Patients deserve optimal visual quality and functional visual acuity in all light conditions
C-flex Aspheric and Superflex Aspheric IOLs with aberration-neutral technology:
• Offer improved contrast sensitivity compared with spherical IOLs3,4
• Provide better low light level visual acuity than spherical IOLs18
• Can offer more depth of field than aberration-negative IOLs by retention of the patient’s natural level of corneal spherical aberration6
• Are less susceptible to the effects of decentration than aberration-negative IOLs12
C-flex® Aspheric & Superflex® Aspheric
Spherical IOL
Aberration-neutral aspheric IOL
Prolate anterior surface means uniform power from centre to edge. Aberration-neutral optic retains natural residual positive SA of the cornea.
Power increases from centre to edge.
0
Disadvantages
Adds to corneal positive spherical aberration (SA)
Degrades image quality and contrast sensitivity
Advantages
High quality vision in all lighting conditions
Good contrast sensitivity
More depth of field than an aberration-negative aspheric IOL
Optimal results for ALL patients; not just for the “average” cornea
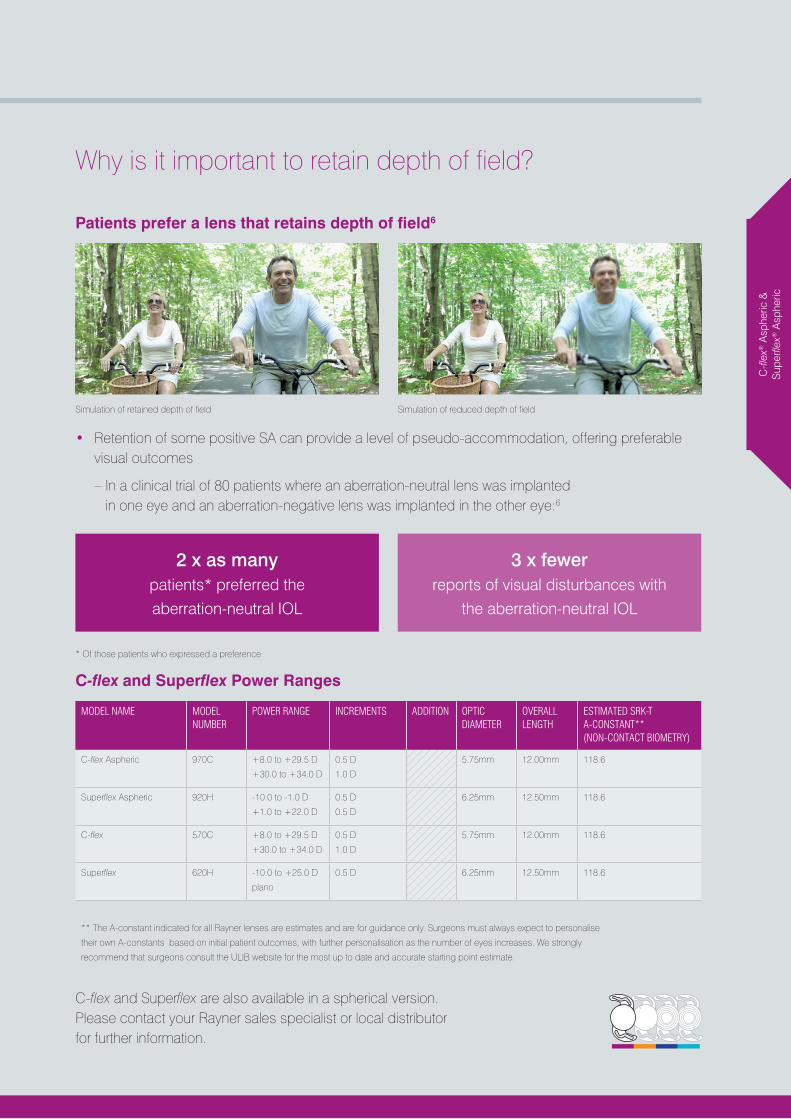
Why is it important to retain depth of field?
Patients prefer a lens that retains depth of field6
• Retention of some positive SA can provide a level of pseudo-accommodation, offering preferable visual outcomes
– In a clinical trial of 80 patients where an aberration-neutral lens was implanted in one eye and an aberration-negative lens was implanted in the other eye:6
* Of those patients who expressed a preference
C-flex and Superflex Power Ranges
MODEL NAME MODEL NUMBER
POWER RANGE INCREMENTS ADDITION OPTIC DIAMETER
OVERALL LENGTH
ESTIMATED SRK-T A-CONSTANT** (NON-CONTACT BIOMETRY)
C-flex Aspheric 970C +8.0 to +29.5 D
+30.0 to +34.0 D
0.5 D
1.0 D
5.75mm 12.00mm 118.6
Superflex Aspheric 920H -10.0 to -1.0 D
+1.0 to +22.0 D
0.5 D
0.5 D
6.25mm 12.50mm 118.6
C-flex 570C +8.0 to +29.5 D
+30.0 to +34.0 D
0.5 D
1.0 D
5.75mm 12.00mm 118.6
Superflex 620H -10.0 to +25.0 D
plano
0.5 D 6.25mm 12.50mm 118.6
** The A-constant indicated for all Rayner lenses are estimates and are for guidance only. Surgeons must always expect to personalise
their own A-constants based on initial patient outcomes, with further personalisation as the number of eyes increases. We strongly
recommend that surgeons consult the ULIB website for the most up to date and accurate starting point estimate.
C-fl
ex® A
sphe
ric &
S
uper
flex®
Asp
heric
2 x as many patients* preferred the aberration-neutral IOL
3 x fewer reports of visual disturbances with
the aberration-neutral IOL
Simulation of retained depth of field Simulation of reduced depth of field
C-flex® AsphericSuperflex® Aspheric
T-flex® Aspheric
M-flex® Aspheric
M-flex® T
C-flex and Superflex are also available in a spherical version. Please contact your Rayner sales specialist or local distributor for further information.
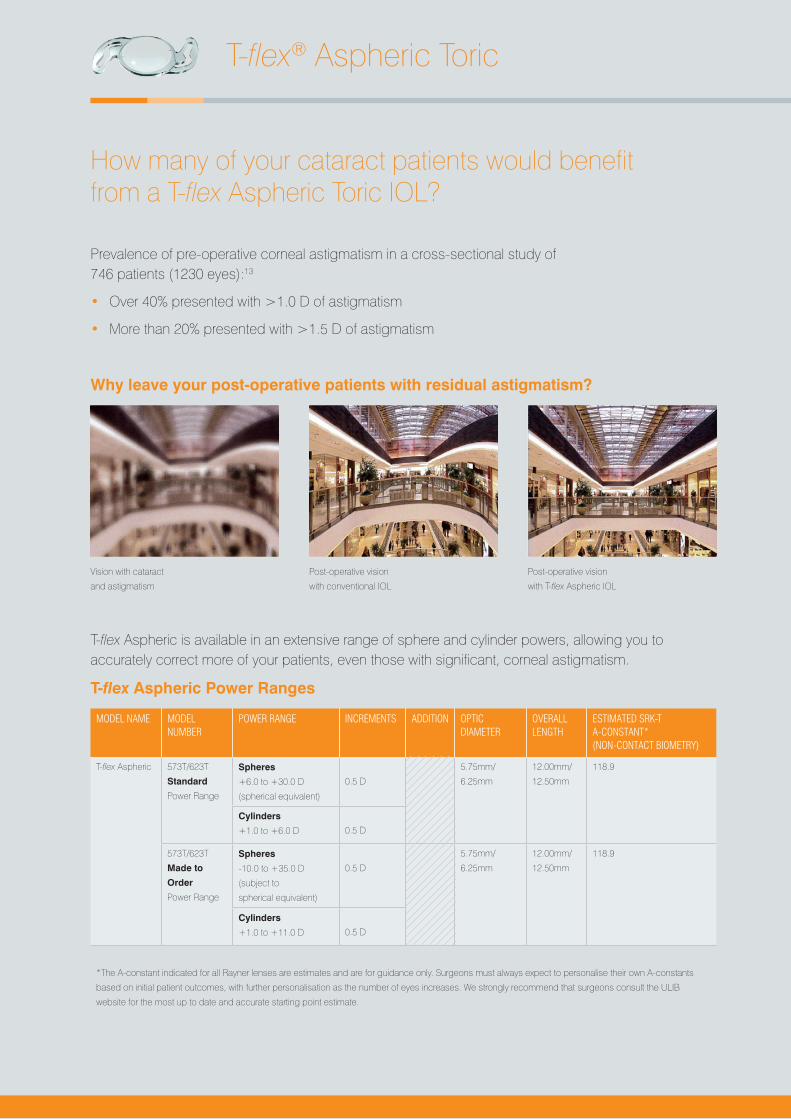
How many of your cataract patients would benefit from a T-flex Aspheric Toric IOL?
Prevalence of pre-operative corneal astigmatism in a cross-sectional study of 746 patients (1230 eyes):13
• Over 40% presented with >1.0 D of astigmatism
• More than 20% presented with >1.5 D of astigmatism
Why leave your post-operative patients with residual astigmatism?
T-flex Aspheric is available in an extensive range of sphere and cylinder powers, allowing you to accurately correct more of your patients, even those with significant, corneal astigmatism.
T-flex Aspheric Power Ranges
MODEL NAME MODEL NUMBER
POWER RANGE INCREMENTS ADDITION OPTIC DIAMETER
OVERALL LENGTH
ESTIMATED SRK-T A-CONSTANT* (NON-CONTACT BIOMETRY)
T-flex Aspheric 573T/623T
Standard
Power Range
Spheres
+6.0 to +30.0 D
(spherical equivalent)
0.5 D
5.75mm/
6.25mm
12.00mm/
12.50mm
118.9
Cylinders
+1.0 to +6.0 D
0.5 D
573T/623T
Made to
Order
Power Range
Spheres
-10.0 to +35.0 D
(subject to
spherical equivalent)
0.5 D
5.75mm/
6.25mm
12.00mm/
12.50mm
118.9
Cylinders
+1.0 to +11.0 D
0.5 D
*The A-constant indicated for all Rayner lenses are estimates and are for guidance only. Surgeons must always expect to personalise their own A-constants
based on initial patient outcomes, with further personalisation as the number of eyes increases. We strongly recommend that surgeons consult the ULIB
website for the most up to date and accurate starting point estimate.
T-flex® Aspheric Toric
Vision with cataract
and astigmatism
Post-operative vision
with conventional IOL
Post-operative vision
with T-flex Aspheric IOL

Proven rotational stability2 with predictable, sustainable and accurate visual results
Designed with AVH Technology® for excellent fixation within the capsular bag:1
• Progressively taking up the forces generated within the contracting capsular bag
• Maintaining excellent centration with rotational, torsional and directional stability
In a prospective study of 27 eyes in 22 consecutive patients with >1.5 D regular corneal astigmatism, at 3 months post-operatively, variations from intended axis were:2
Stability achieved through advanced haptic design
Raytrace® - Online Specialist IOL Calculator
Accurate and predictable results in a fast and convenient interface
• Easy to use, straightforward step-by-step data entry
• Fast and accurate results with calculations performed instantly
• Convenient and predictable outcomes with estimated post-operative refraction and SIA accounted for
• Flexible calculator tool that can be used for T-flex Aspheric, M-flex, M-flex T and Sulcoflex IOLs
Visit: www.rayner.com/raytrace
3.1° mean variation
100% were ≤12°
93% of IOLs were ≤10°
Percentage cylinder reduction of
81% (-2.70 ±0.94 to -0.52 ±0.63 D)
T-fle
x® A
sphe
ric T
oric
Outer haptics begin to take up the compression
forces of post-operative capsular contraction
Outer haptics engage the inner haptics Haptic tips gently meet the IOL optic and are
effectively locked into position
C-flex® AsphericSuperflex® Aspheric
T-flex® Aspheric
M-flex® Aspheric
M-flex® T
How would your patients benefit from our multifocal IOLs?
6 months after binocular implantation of M-flex +3.0 D:
% patients with functional vision without the need for spectacles14
M-flex Multifocal IOLs offer your presbyopic patients the chance of spectacle independence for distance, intermediate and near activities.14
Select the correct multifocal option to match your patient’s lifestyle:
• M-flex +3.0 D add for patients that predominantly participate in intermediate and distance activities i.e. intermediate activities such as computer work or seeing a vehicle dashboard
• M-flex +4.0 D add for patients that predominantly participate in near and distance activities i.e. near activities such as reading or applying make-up
M-flex® Multifocal
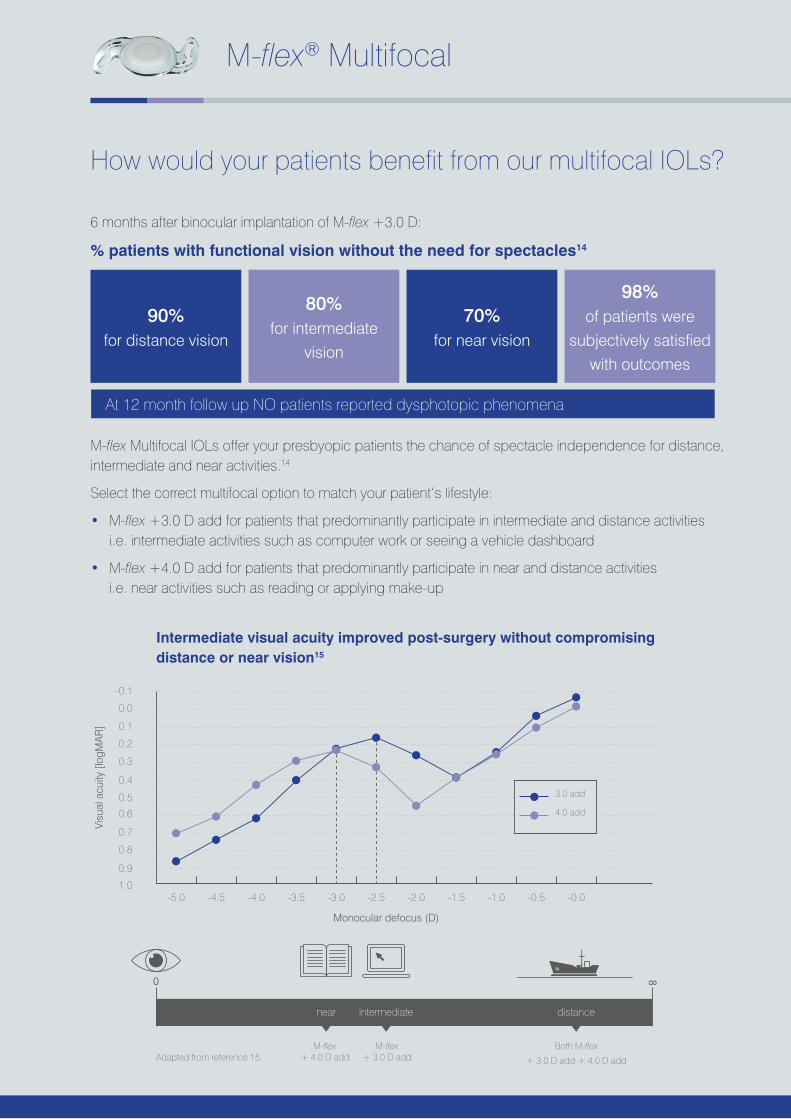
Intermediate visual acuity improved post-surgery without compromising distance or near vision15
-0.1
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0-5.0 -4.5 -4.0 -3.5 -3.0 -2.5 -2.0 -1.5 -1.0 -0.5 -0.0
Visu
al a
cuity
[log
MA
R]
Monocular defocus (D)
3.0 add
4.0 add
M-flex+ 4.0 D add
M-flex+ 3.0 D add + 3.0 D add + 4.0 D add
Both M-flex
intermediate distancenear
80
Adapted from reference 15.
90% for distance vision
70% for near vision
80% for intermediate
vision
98% of patients were
subjectively satisfied with outcomes
At 12 month follow up NO patients reported dysphotopic phenomena

Wouldn’t your presbyopic, astigmatic patients also like the opportunity to live without glasses?
With M-flex T Multifocal Toric IOLs, patients with astigmatism need no longer be excluded from the lifestyle advantages of multifocality.
M-flex T offers all the benefits of the M-flex and effectively corrects corneal astigmatism with a large range of cylinder power options (1 to 6 Dioptres).
Multi-zone refractive optic technology
Aberration-neutral aspheric optic
360° Amon-Apple Enhanced Square Edge design reduces PCO
AVH Technology for excellent centration
M-flex and M-flex T Power Ranges
MODEL NAME
MODEL NUMBER
POWER RANGE INCREMENTS ADDITION OPTIC DIAMETER
OVERALL LENGTH
ESTIMATED SRK-T A-CONSTANT* (NON-CONTACT BIOMETRY)
M-flex 630F +14.0 to +25.0 D 0.5 D +3.0 D add far dominant 6.25mm 12.50mm 118.6
630F +10.0 to +25.0 D 0.5 D +4.0 D add far dominant 6.25mm 12.50mm 118.6
580F +25.5 to +30.0 D 0.5 D +3.0 D add far dominant 5.75mm 12.00mm 118.6
580F +25.5 to +30.0 D 0.5 D +4.0 D add far dominant 5.75mm 12.00mm 118.6
M-flex T 588F/638F
Standard
Power Range
Spherical
Equivalent
+14.0 to +32.0 D
0.5 D
+3.0 D or +4.0 D
add far dominant
5.75mm/
6.25mm
12.00mm/
12.50mm
118.6
Cylinders
+1.0 D, +2.0 D
+3.0 D, +4.0 D
588F/638F
Made to
Order
Power Range (excluding powers described within Standard range)
Spherical
Equivalent
+14.0 to +32.0 D
0.5 D
+3.0 D or +4.0 D
add far dominant
5.75mm/
6.25mm
12.00mm/
12.50mm
118.6
Cylinders
+1.0 to +6.0 D
0.5 D
*The A-constant indicated for all Rayner lenses are estimates and are for guidance only. Surgeons must always
expect to personalise their own A-constants based on initial patient outcomes, with further personalisation as
the number of eyes increases. We strongly recommend that surgeons consult the ULIB website for the most
up to date and accurate starting point estimate.
M-flex® Multifocal
M-fl
ex®
Mul
tifoc
al
M-fl
ex® T
M
ultif
ocal
Tor
ic
M-flex® T Multifocal Toric
C-flex® AsphericSuperflex® Aspheric
T-flex® Aspheric
M-flex® Aspheric
M-flex® T

Rayner System Pack
The Rayner System Pack conveniently packages together a Single Use Soft-Tipped Injector with each IOL across the range
• Streamlined ordering process
• Reduced chances of mistakes in the operating room
• Validated injector for use with all Rayner IOLs
• Single-use injector – for increased patient safety
Single Use Soft-Tipped Injector
• Single handed technique that leaves one hand free for IOL manipulation
• Continuous smooth action for good control and predictable IOL deployment
• Ergonomically optimised hand grip enhances control and confidence
• Exclusively designed and manufactured by Rayner for optimised delivery across the full range of IOL models
To watch videos of experts loading the injectors, posters and more, visit www.rayner.com

Ray
ner S
yste
m P
ack,
S
oft -
Tipp
ed In
ject
or, R
ayvi
sc
References: 1. Claoué C. Clinical and Surgical Ophthalmology 2008; 26(6): 198-2002. Alberdi R et al. J Refract Surg. 2012; 28(10):696-7003. Nanavaty MA et al. J Cataract Refract Surg. 2009; 35:663–6714. Yagci R et al. Eur J Ophthalmol. 2014 Jul 24; 24(5):688-92 5. Vyas AV et al. J Cataract Refract Surg 2007; 33:81-876. Johansson B et al. J Cataract Refract Surg. 2007; 33:1565–15727. Mathew RG and Coombes AGA. Ophthalmic Surg Lasers Imaging.
2010 Nov-Dec; 41(6):651-58. Rayner. Data on File. White paper9. McLoone E et al. Br J Ophthalmol. 2001; 85:543–54510. Richter-Mueksch S et al. J Cataract Refract Surg. 2007; 33:1414–1418
11. Claoué C. Clinical and Surgical Ophthalmology 2008; 26(10):353-35612. Altmann GE et al. J Cataract Refract Surg. 2005; 31(3): 574-58513. Khan M and Muhtaseb M. JCRS 2011; doi: 10.1016/j.jcrs.2011.04.02614. Cezón Prieto J and Bautista MJ. J Cataract Refract Surg. 2010; 36:
1508-151615. Rasilber T et al. J Cataract Refract Surg. 2013; 39:350-55716. Tomlins PJ et al. J Cataract Refract Surg. 2014; 40:618–62517. Erie JC et al. J Cataract Refract Surg. 2001; 27:614–62118. Pepose JS et al. Graefes Arch Clin Exp Ophthalmol. 2009 Jul;
247(7):965-73
For optimal visual quality and reliable outcomes choose Rayner IOLs
C-flex® Aspheric and Superflex® Aspheric, aberration-neutral, monofocal IOLs for optimal visual quality in all lighting conditions
• Improved contrast sensitivity compared with conventional lenses3,4
• Retain more depth of field than aberration-negative IOLs6
• Less susceptible to the effects of de-centration than aberration-negative IOLs12
T-flex® Aspheric Toric IOLs for reliable outcomes with peace of mind
• Proven rotational stability2 with predictable, sustainable and accurate visual results
– 3.1° mean variation at 3 months post-operatively2
M-flex® Multifocal and M-flex® T Multifocal Toric IOLs to improve your patients’ quality of life
• M-flex® Multifocal IOLs offer your presbyopic patients spectacle independence for distant, intermediate and near activities14
– M-flex® T Multifocal Toric IOLs extend multifocal option to astigmatic patients
C-flex®, Superflex®, T-flex®, M-flex®, Sulcoflex®, AVH Technology®, Rayacryl®, Raytrace® and Rayvisc® are registered trademarks of Rayner Intraocular Lenses Limited. Not all Rayner products are approved for sale in every country. Please contact your local Rayner distributor for details of which products are available in your area.
GLOBAL HQ & UK OFFICERAYNER INTRAOCULAR LENSES LIMITED10 Dominion WayWorthing, West SussexBN14 8AQ. United Kingdom
Tel: +44 (0) 1903 258 900Email: [email protected]: rayner.com
UK CUSTOMER SERVICETel: +44 (0) 1903 854 560Email: [email protected]
GERMANY CUSTOMER SERVICETel: +49 30 6290783 - 0Email: [email protected]
ITALIAN CUSTOMER SERVICETel: +39 800 972485Email: [email protected]
SPANISH CUSTOMER SERVICETel: +34 910 480055Email: [email protected]
Regulatory restrictions may apply in certain markets.©2016 Rayner Intraocular Lenses Limited.EC-2016-125 12/16







