Practical Approaches to Atrial Fibrillation Management
Answers to Your Everyday Questions
H. Mark Guo, MD, FACC, FHRS Clinical Cardiac Electrophysiology Oregon Heart & Vascular Institute

Disclosure SYSTEMS OF CARE SYMPOSIUM 2015
Care of Your Patient in the Era of Population Health Hongsheng Mark Guo, MD, FACC, FHRS
• I use free pens from all industrials. • I have no other financial relationships
to disclose.
Thursday 8 am: 63 yo man calls from MSP
• In “AF” at least since Tuesday morning • Had breakfast in Indianapolis at 5:00am • Flight changed to 7:00pm to continue trip • Insists on not delaying trip any later • Previous episode in 5/2004 (metoprolol and
propafenone) • Cardioversion scheduled 4:00pm
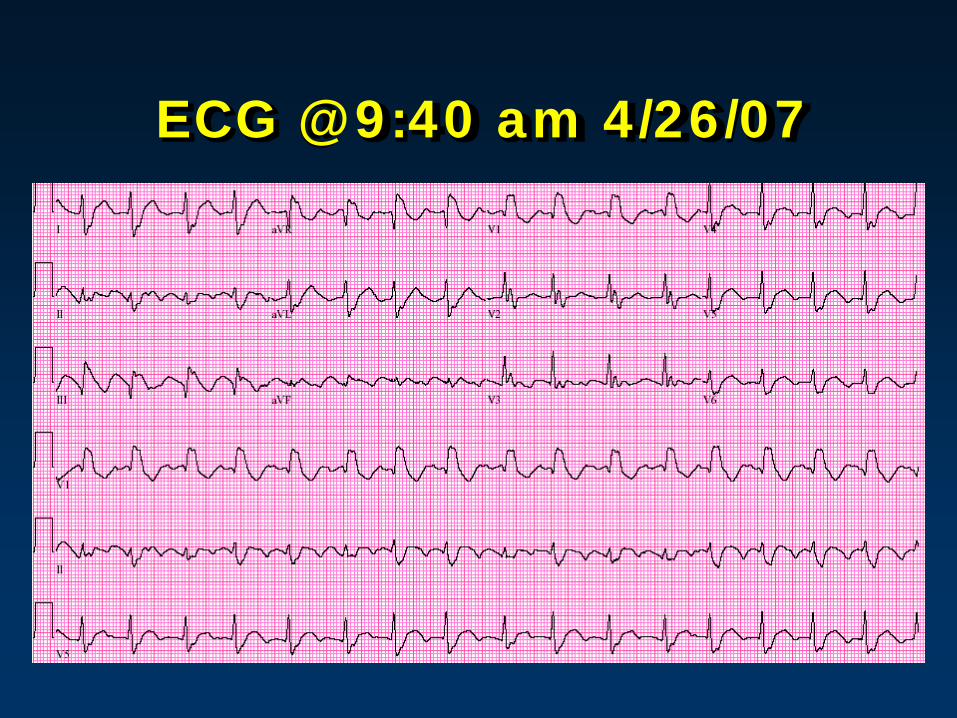
ECG @ 9:40 am 4/26/07
What would you do?
A. Cardioverte and catch flight B. Cancel cardioversion, titrate BB, start
coumadine, cardioverte after trip C. Cardioverte, start lovenox and
coumadine, f/u with ACC D. Cancel cardioversion, titrate BB, start
coumadine, ablation after 3-4 weeks AC E. Start NOAC, TEE, cardioverte if no clot

What is AF?
• AF is the most common sustained arrhythmia.
• Prevalence: 0.4% to 1% in general population, increasing with age to 12% for those > 75 yrs.
• Stroke rate: < 1% to > 15% annually, depending on comorbid risk factors.
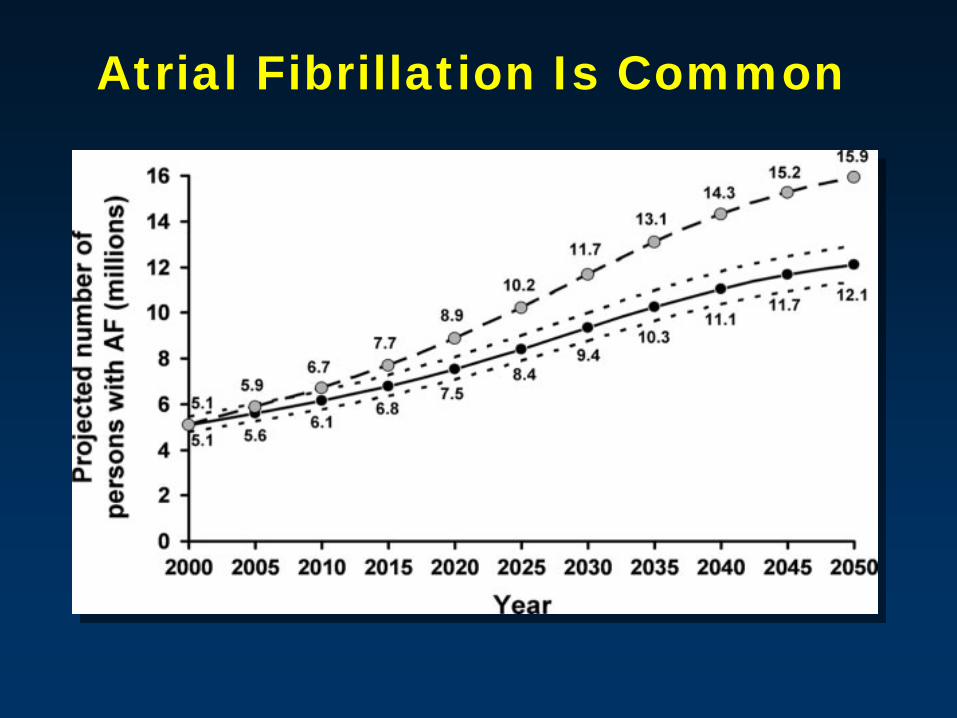
Atrial Fibrillation Is Common

Adapted from Feinberg WM. Arch Intern Med. 1995;155:469-473.
U.S. population
Population with atrial fibrillation
Age, yr
<5 5- 9
10- 14
15- 19
20- 24
25- 29
30- 34
35- 39
40- 44
45- 49
50- 54
55- 59
60- 64
65- 69
70- 74
75- 79
80- 84
85- 89
90- 94
>95
U.S. population x 1000
Population with AF x 1000
30,000
20,000
10,000
0
500
400
300
200
100
0
Atrial Fibrillation Demographics by Age
What is the Pathophysiology of AF?
• AF may be triggered by a focal source of rapid atrial electrical depolarization, often in the pulmonary veins.
• It is sustained by the presence of multiple reentrant wavelets or spiral wave re-entrant circuits (rotors).
Theories (Too Simple to be perfect) Wishes and dreams.
Clueless!
What causes my AF?
• Acute and temporary causes (triggers) – alcohol intake (holiday heart) – surgery (particularly cardiac surgery) – MI, pericarditis, myocarditis, CHF – pulmonary embolism – hyperthyroidism.
• Concurrent treatment of the underlying disorder and management of AF
Other Causes of AF
• Triggered by other arrhythmias – atrial tachycardia – atrial flutter – Wolff-Parkinson-White (WPW) syndrome – AV nodal reentrant tachycardia.
• Associated with chronic disorders – sleep apnea – hypertension – obesity
How to establish an accurate diagnosis of AF?
• Symptoms maybe absent Not Reliable • “Irregularly irregular rhythm” • ECG
– 12-lead – Ambulatory: Holter, Event monitor, ILR – Device interrogation
• Should be distinguished from – atrial flutter, – multifocal atrial tachycardia – reentrant SVTs, such as AV nodal reentry; – sinus rhythm (SR) with multiple premature atrial complexes.
Are all AFs the same?
• Paroxysmal – terminates spontaneously within 7 days of onset
• Persistent – sustained > 7 days – longstanding persistent: continuous AF > 12
months duration.
• Permanent • Lone AF
Are all AFs treated in the same way?
• Hemodynamically unstable: – Immediate cardioversion, sedate if possible – Refractory, IV amiodarone, ibutilide, or procainamide.
• Hemodynamically stable: – Cardioversion: newly diagnosed, onset within 48 hours – Rate control, anticoagulation if indicated – Cardioversion after 3-4 weeks anticoagulation or no
clot on TEE and therapeutic anticoagulation initiated.
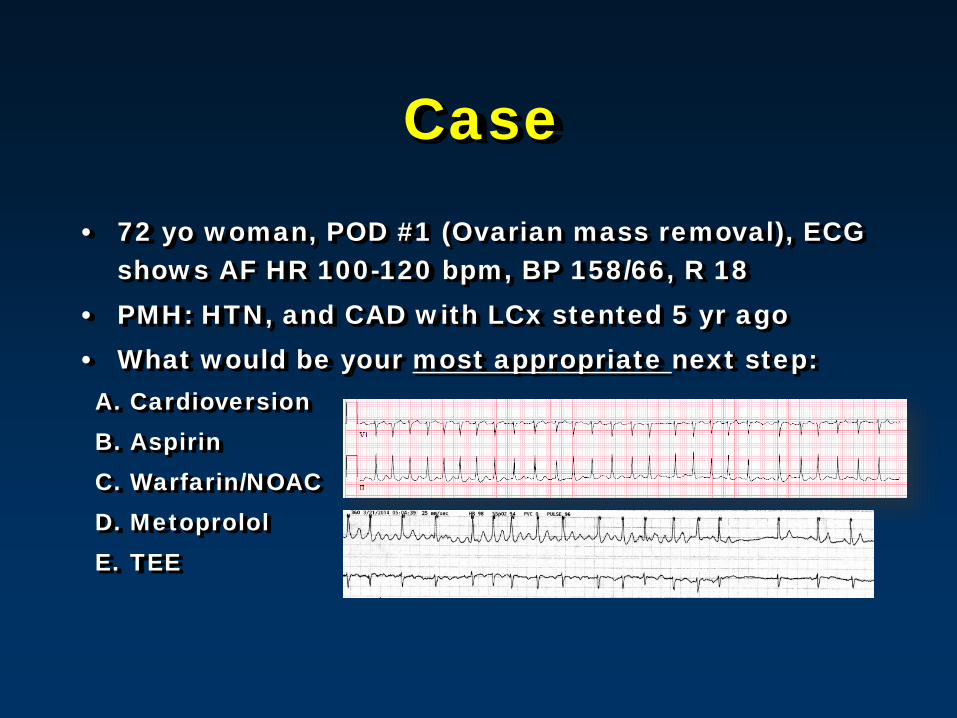
Case • 72 yo woman, POD #1 (Ovarian mass removal), ECG
shows AF HR 100-120 bpm, BP 158/66, R 18 • PMH: HTN, and CAD with LCx stented 5 yr ago • What would be your most appropriate next step: A. Cardioversion B. Aspirin C. Warfarin/NOAC D. Metoprolol E. TEE
CASE
• TEE is performed. Most likely result you predicted is:
A. LAA thrombus B. Spontaneous echo contrast (smoke) in LA C. Clear LAA D. Annual stroke risk is 1-2% E. Annual stroke risk is 3-5% F. Annual stroke risk is 5-9%
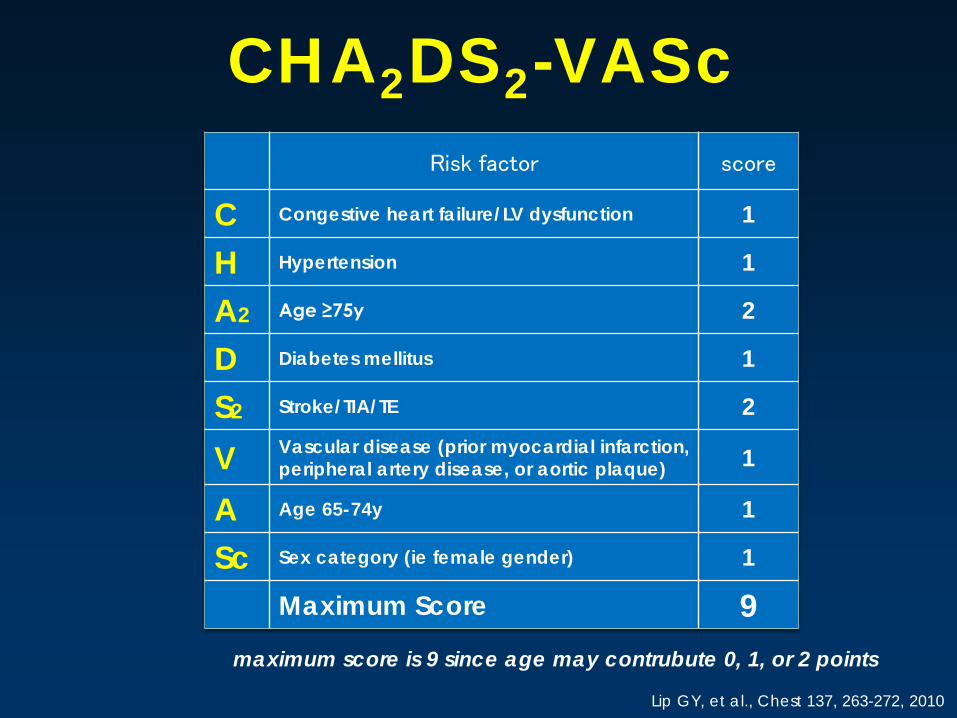
Risk factor score
C Congestive heart failure/LV dysfunction 1
H Hypertension 1
A2 Age ≥75y 2
D Diabetes mellitus 1
S2 Stroke/TIA/TE 2
V Vascular disease (prior myocardial infarction, peripheral artery disease, or aortic plaque) 1
A Age 65-74y 1
Sc Sex category (ie female gender) 1
Maximum Score 9
Lip GY, et al., Chest 137, 263-272, 2010
maximum score is 9 since age may contrubute 0, 1, or 2 points
CHA2DS2-VASc
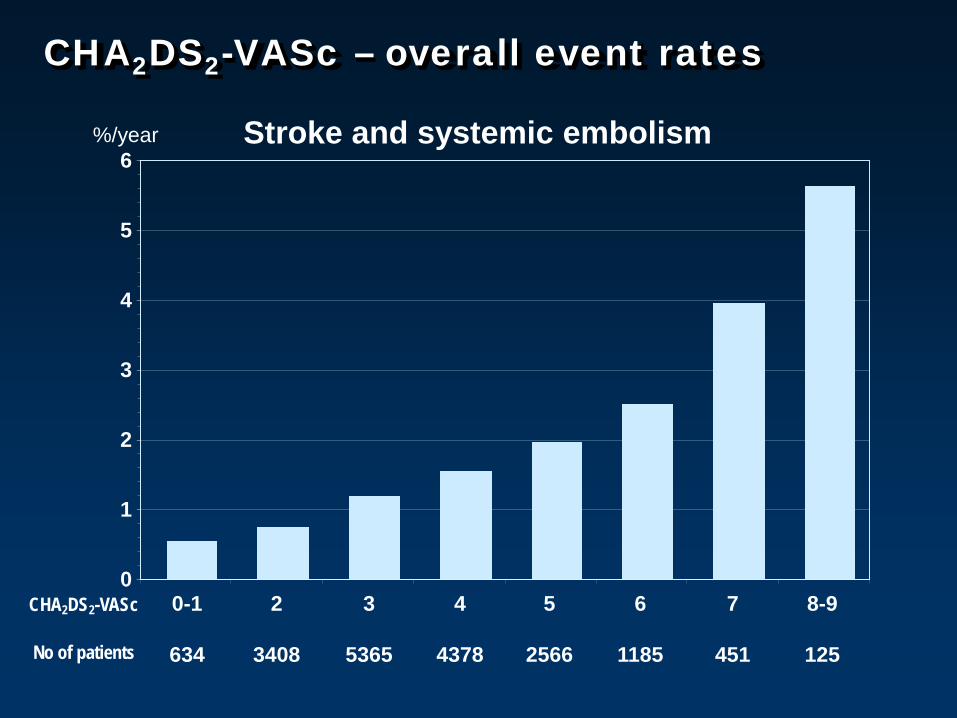
CHA2DS2-VASc – overall event rates
%/year
CHA2DS2-VASc 0-1
634
2
3408
3
5365
4
4378
5
2566
6
1185
7
451
8-9
125 No of patients
Stroke and systemic embolism
0
1
2
3
4
5
6
Marine JE. JAMA. 2007; 298(23): 2368-2778
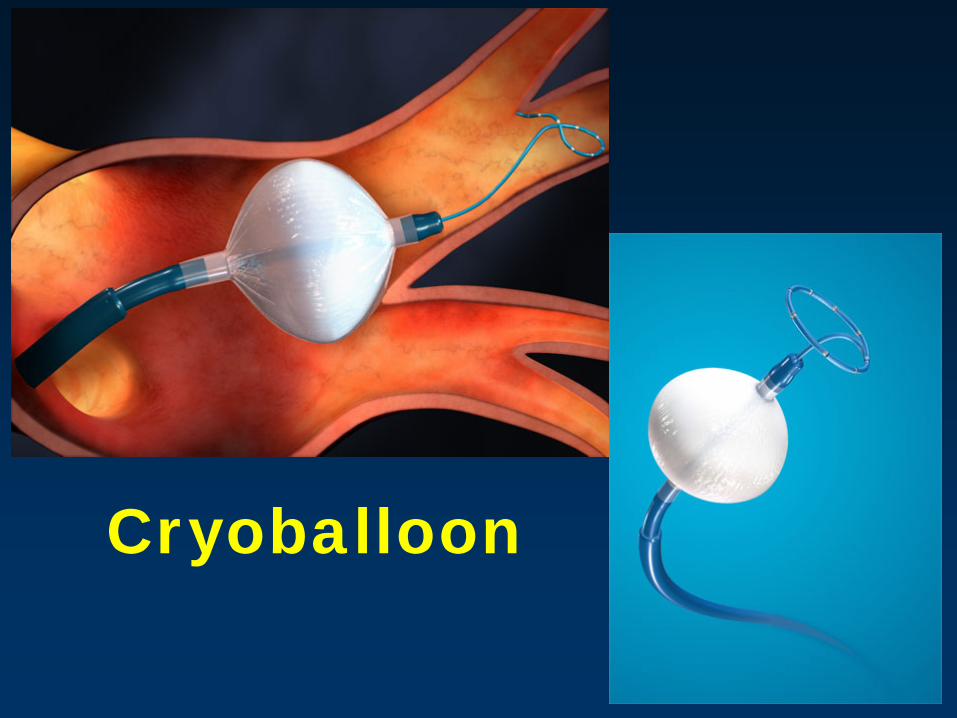
Cryoballoon
Atrial Fibrillation Ablation: Success & Repeat Procedures
• 50 – 70% success with a single procedure • Up to 50% will require a second procedure to
achieve success • 50% will have early recurrence within the
first couple days to weeks – 50% of these will resolve within few weeks and still
have success

Atrial Fibrillation Ablation: Long Term Outcome
Free of antiarrhythmic drugs and free of arrhythmia symptoms at 6 months
• Paroxysmal – 70 to 90%
• Persistent (lasts > 7 days, up to 1 year) – 60 to 80%
• Long standing persistent (> 1 year) – 50 to 70%
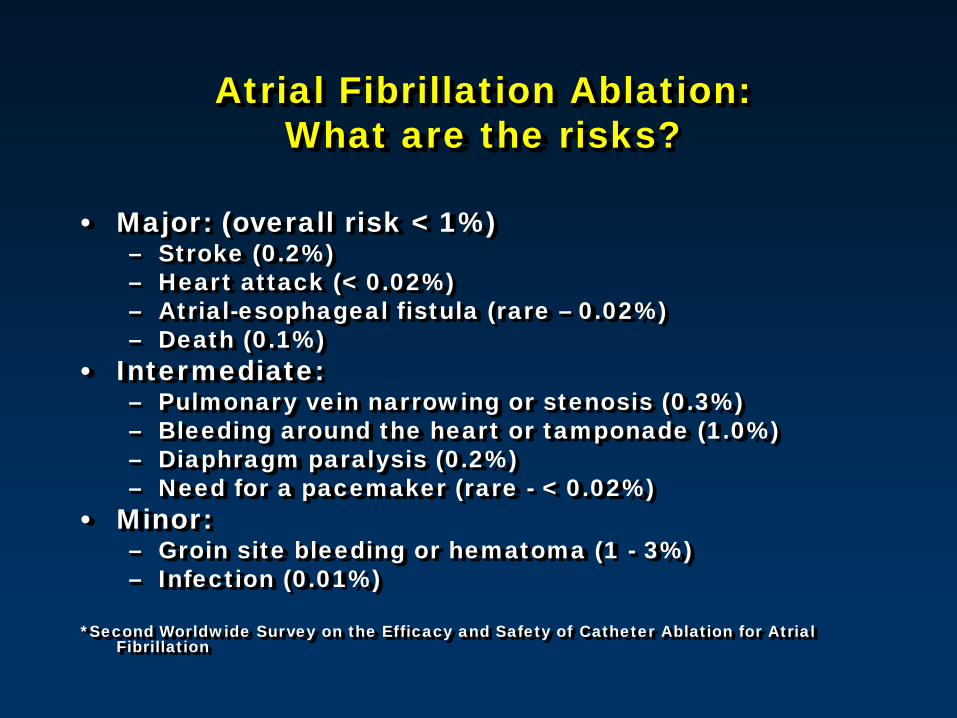
Atrial Fibrillation Ablation: What are the risks?
• Major: (overall risk < 1%) – Stroke (0.2%) – Heart attack (< 0.02%) – Atrial-esophageal fistula (rare – 0.02%) – Death (0.1%)
• Intermediate: – Pulmonary vein narrowing or stenosis (0.3%) – Bleeding around the heart or tamponade (1.0%) – Diaphragm paralysis (0.2%) – Need for a pacemaker (rare - < 0.02%)
• Minor: – Groin site bleeding or hematoma (1 - 3%) – Infection (0.01%)
*Second Worldwide Survey on the Efficacy and Safety of Catheter Ablation for Atrial Fibrillation

Atrioesophageal Fistula
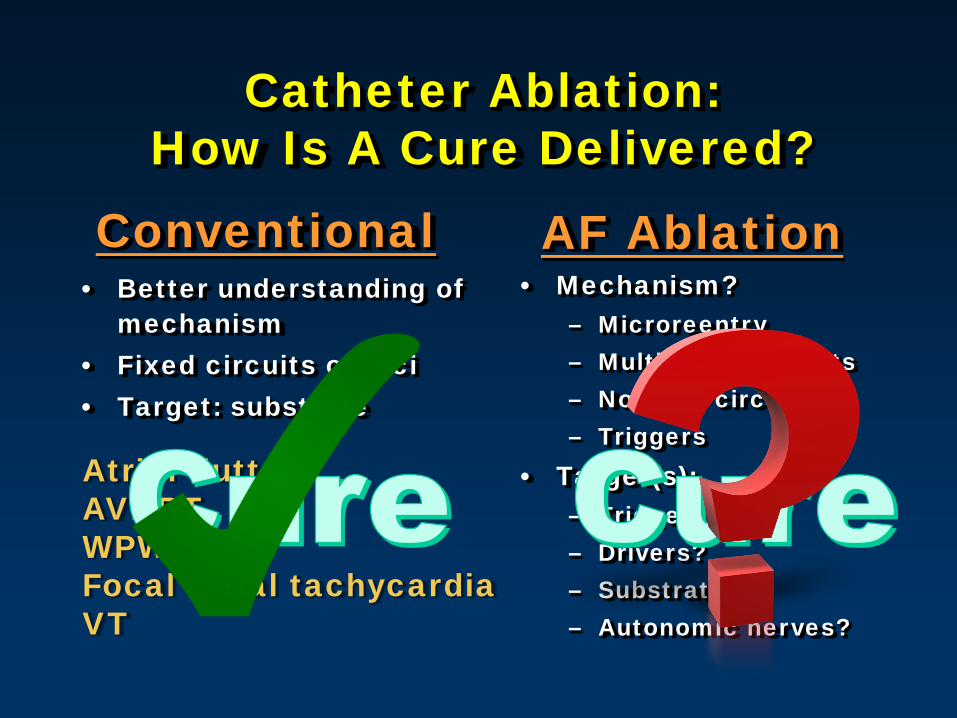
Catheter Ablation: How Is A Cure Delivered?
• Better understanding of mechanism
• Fixed circuits or foci • Target: substrate
• Mechanism? – Microreentry – Multiple wavefronts – No fixed circuit – Triggers
• Target(s): – Triggers? – Drivers? – Substrate? – Autonomic nerves?
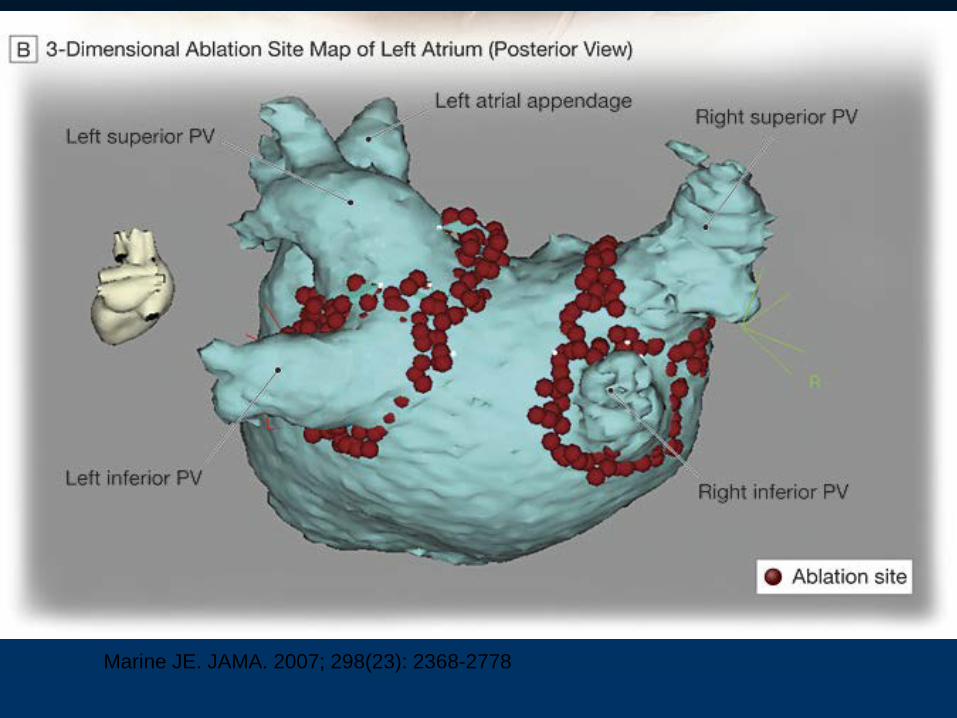
Conventional AF Ablation
Atrial flutter AVNRT WPW Focal atrial tachycardia VT
“What Is EP?”
• Precision
• Perfection
Cure Satisfaction
• Delicacy
• Exquisiteness
• Elegance
精致优雅 高雅 精确
完美 精巧
“What Is EP?”
• Precision
• Perfection
Cure Satisfaction
• Delicacy
• Exquisiteness
• Elegance
• Destructiveness
• Nastiness
• Massiveness
• Excessiveness
Deviating
• Reckless
粗糙 邋遢
毁坏 多余
鲁莽
When to offer a therapy as first-line?
•Safety •Effectiveness •Need from patient
AF Ablation Summary
• AF ablation is an AF ablation, still. • There are many uncertainties. • More data is needed. • It is still too early to be offered to most
patients as a first-line therapy. • Catheter ablation might be the right
answer for some patients.
“Priority of Care”
• Rate Control • Anticoagualtion • Rhythm Control

2/15/06, ER: 58 yo Man, Day Before EPS
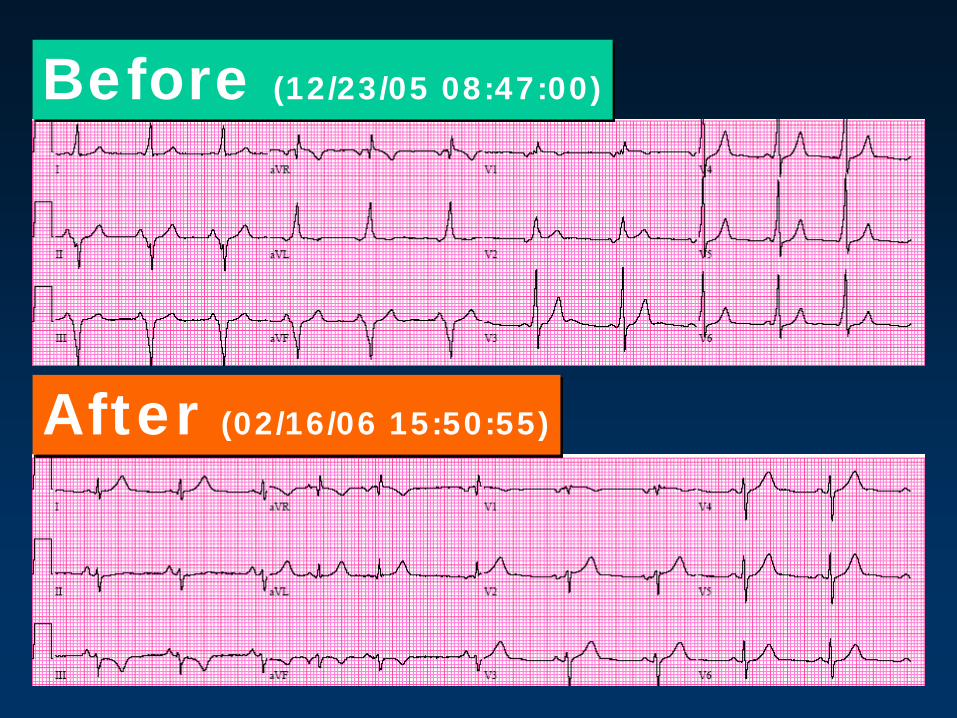
Before (12/23/05 08:47:00)
After (02/16/06 15:50:55)
What’s New in 2015?
• Stroke risk assessment: CHA2DS2-VASc • New oral anticoagulants:
– Dabigatran – Rivaroxaban – Apixaban – Edoxaban
• Ablation: targeting substrates • Digoxin: associated with worse outcome

Stroke Prevention in 2015
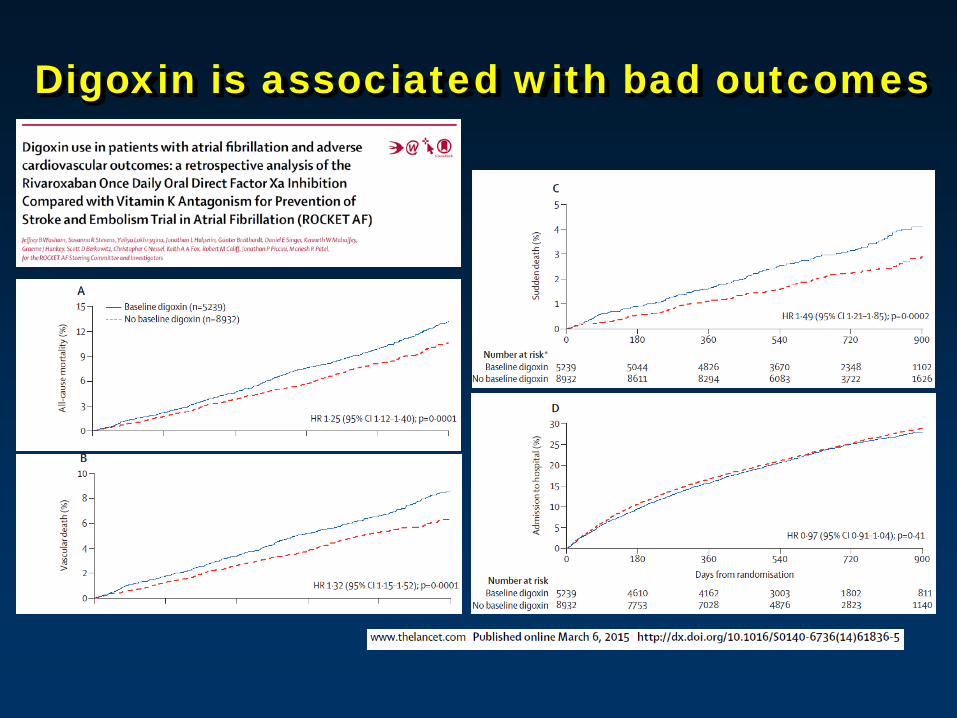
Digoxin is associated with bad outcomes
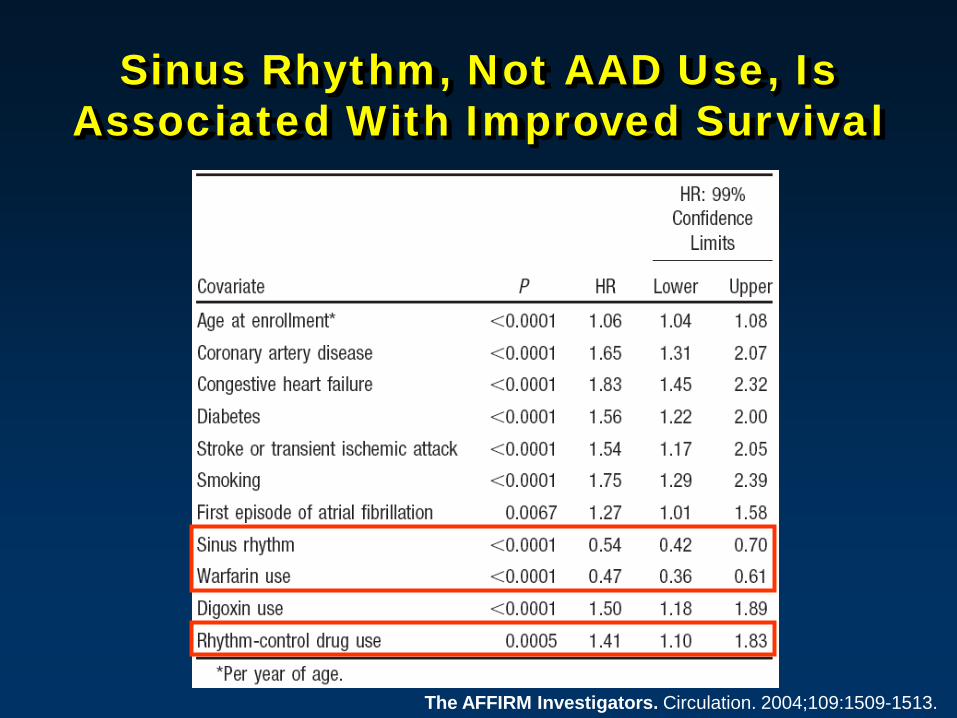
Sinus Rhythm, Not AAD Use, Is Associated With Improved Survival
The AFFIRM Investigators. Circulation. 2004;109:1509-1513.

AF Ablation in 2015 Targeting Substrates
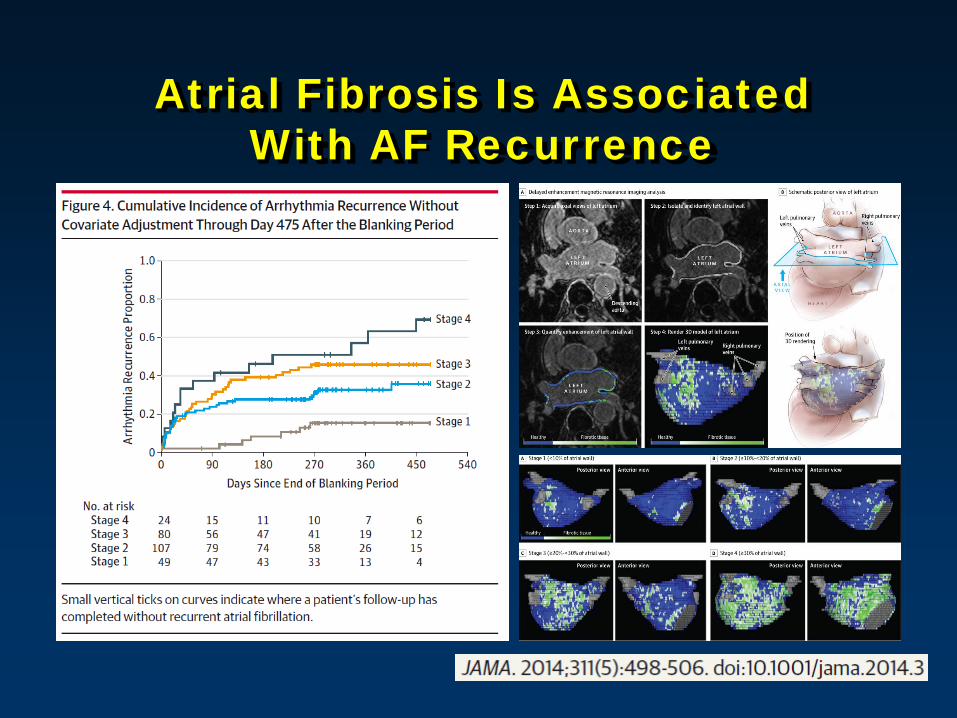
Atrial Fibrosis Is Associated With AF Recurrence
Summary
• AF is common, with different clinical presentations. • AF is a complicated arrhythmia and our
understanding regarding the exact mechanism remains limited.
• Catheter ablation, although based on imperfect theory, may help selected patients.
• AF is a manageable arrhythmia, and options are available for all patients to minimize risks for complications and to improve quality of life.