
CHAPTER -VII
POVERTY ASSESSMENT TO DETERMINE THE FACTORS OF
HEALTH IN RURAL AREAS
CHAPTER-VII
POVERTY ASSESSMENT TO DETERMINE THE FACTORS OF HEALTH IN RURAL AREAS
(Trends, Policies and Health Services).
I-Trends in Poverty
It had been made clear in the previous chapter that the common poor
of the rural areas remained indifferent to the developments and health policies
even after the whole hearted support of the elite Indians. As their root
problem was poverty, their only want was food to satisfy hunger, work to
satisfy needs and shelter to live in.
There were millions of people who did not comprise enough food to
eat, did not have drinking water within their reach, did not have land of their
own to cultivate or enough work to do. The problem was never taken
seriously by the then government. Even today we have approx 32% people
who are living below poverty line as suggested by the Planning Commission
of India 2009-2010.1
It becomes urgent for us to understand the term poverty so as to
determine the health factors, particularly in rural areas. As discussed in the
previous chapters Poverty and health are intertwined with each other’, we
can assess the term poverty in socio – economic perspective:
1 Excerpted from, The Hindu, (Daily News paper) 21.04.2011.

158
‘Poverty occurs when sources, to satisfy the wants and
needs of the people, are not available to them in sufficient
and appropriate mode’.
If the resources are not available to the people, they may fall into
moral depression which according to Indian Famine Commission 1901 is:
‘A greatest evil which may lead to physical deterioration’2
It is this dimension that enables us to define poverty in terms of
caloric measures and per capita income, and thus we may identify a poor
person as he, who does not have enough resource to provide himself and his
family with the primary requirements. Planning Commission has also
estimated poverty, based on the formula suggested by the Tendulkar
Committee for computing the number of poor. It had suggested that the
poverty should be estimated on the basis of the consumption based on the
cost of living index3 instead of caloric intake only. It should also include
services such as health and education.4
However, while defining poverty all basic and fundamental human
needs such as, proper nutrition, drinking water, shelter, hygiene clothing,
education etc., need to be accounted for. Nutritional deficiency is also a
leading cause for disease.
2 Report of the Indian Famine Commission 1901, op.cit., p.11. 3 Living Index however includes daily expenditure on food, housing, clothing etc. 4 Excerpted from, The Hindu (Daily News Paper) 24.04.2011.

159
According to UNICEF 2005:
‘Malnutrition limits development and capacity to learn. It
also costs life about 50% of all childhood deaths – Lack of
vitamin leads to scurvy and disorder and muscle
weaknesses’.5
Thus we need a proper analysis of poverty, as it is not simply a matter of
physical or material deprivation, but a much more complex social phenomenon.
In Colonial India (19th Century) most poverty stricken areas were out of the
reach of government. The government never tried to find out the health
problems of the peasants. Their basic health problems were, mal-nourishment
and under nourishment. Many progressive measures were done, new
technologies were introduced and researches were done, but the fact remains
that there was economic exploitation which compelled the people to live in
most deadly situation. The situation was well understood by the economists of
that time.
Dadabhai Naoroji said:-
‘…I do not for a movement mean to ignore the very bright
side of British rule, and the many blessings of law and
order which it has conferred on India … My object now is
to show that under the present system of administration
5 Information on the Impact of Nutrition Deficiency, from- MSN, Encarta
Encyclopedia (2005).
160
India is suffering seriously in several ways … and is
sinking in poverty’.6
The Acts and Committees were no doubt set up to check out the
problems but the things were not implemented properly. Indian Famine
Commission 1901, after its experience of the previous situations recommended
for the extension of the duties of a hospital assistant on a relief work in this
manner.
- Daily inspection of the sanitary arrangements and water supply.
- Periodical inspection of the food offered for sale and prohibition of the
sale of injurious grain.
- Periodical inspection of all persons on works with special attention to
new comers, weekly gangs and nursing mothers.
- Distribution of quinine on the works to prevent malarial fever and the
supply of anti scorbuties on the appearance of scurvy.7
The Indian Famine Commission of 1880-1885 recommended classifying
the Indian villages into different categories so as to perform the inspections
properly.8
6 Naoroji Dadabhai, Poverty and Un British Rule in India .op.cit. p.1. 7 Report of the Indian Famine Commission-1901, op.cit. p.59. 8 Indian Famine Commission 1880-85 also insisted that the country should be
divided into circles of convenient size, each of which placed under its proper officers with a regular gradation of authority, and with a clear definition of duties’, Report of the Indian Famine Commission 1880-85, part-1, Famine Relief, op.cit.p.48.
161
Dr. Cunningham, the Sanitary Commissioner with the Government of
India writes in 1878, ‘Prevalence of disease means either, Generally unhealthy
year from causes which are extremely obscure, in sanitary conditions of the
locality, or Unfavorable conditions of the people themselves’.9
However, these steps taken by the Government were not sufficient. It is
therefore rural areas remained isolated areas and the rural poor could hardly
avail the facilities provided by the Government. It was only after the
independence when Planning Commission of India took the initiative of
improving the general living conditions of the people specially the rural people.
The Bhore Committee in its report of 1945 considered the needs of rural India
and planned for introducing progressive health measures in rural areas. It
recommended:
‘We have taken the countryside as the focal point of our
main recommendations; for it is the tiller of the soil on
whom the economic structure of the country eventually
rests …… we need no further justification for making him
the chief beneficiary under our proposals. The essential
aim of our proposals is to ensure the health of the masses
through the effective working of the centres, we are
recommending for rural areas’.10
Such unfavorable conditions were created by economic factors along
with environmental factors. The statistical records showing the decline of
9 Report of the Indian Famine Commission – 1888, op.cit., p.185. 10 Report of the Health Survey and Development Committee 1945, Vol.-II,
(Recommendations), Government of India Press- 1946- p.5.
162
Indian industries and towns suggest that poverty had not been an unfortunate
accident it had been linked with the development process that is continued even
today. Still the Medical and Communication Services had not been provided to
the rural sector. The records also suggest that Gross National expenditure on
the basic needs as health, education and medical measures is still very little.11
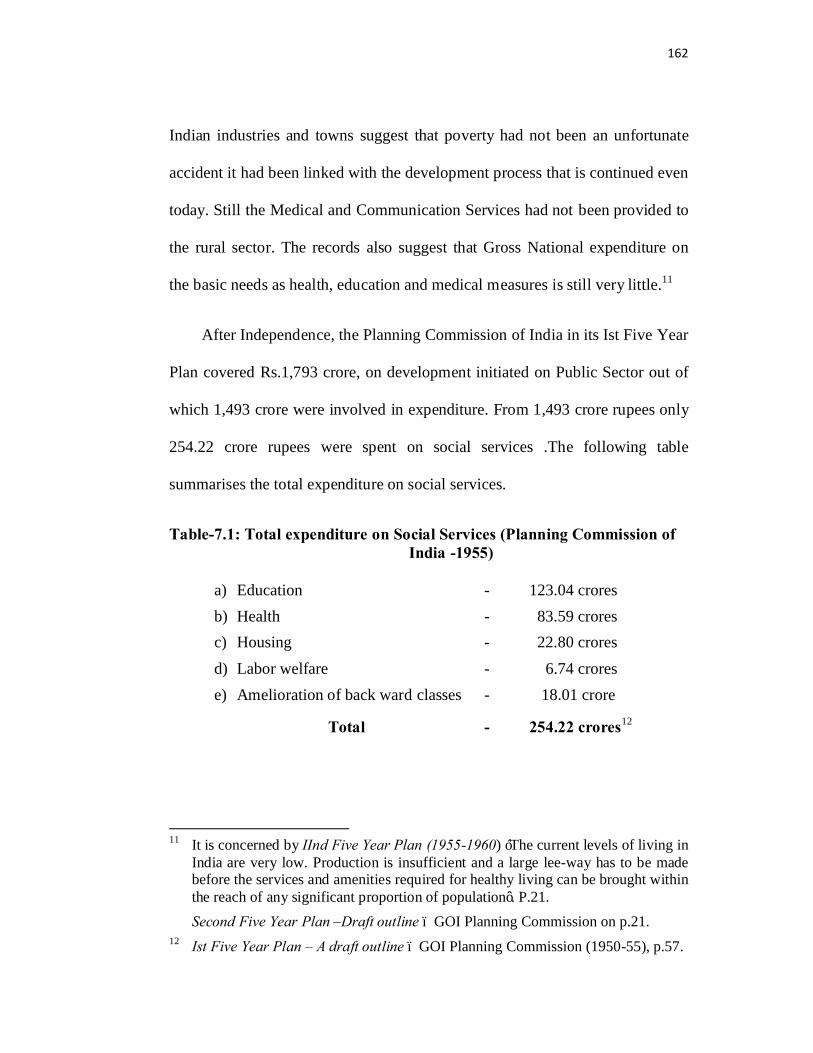
After Independence, the Planning Commission of India in its Ist Five Year
Plan covered Rs.1,793 crore, on development initiated on Public Sector out of
which 1,493 crore were involved in expenditure. From 1,493 crore rupees only
254.22 crore rupees were spent on social services .The following table
summarises the total expenditure on social services.
Table-7.1: Total expenditure on Social Services (Planning Commission of India -1955)
a) Education - 123.04 crores b) Health - 83.59 crores c) Housing - 22.80 crores d) Labor welfare - 6.74 crores e) Amelioration of back ward classes - 18.01 crore
Total - 254.22 crores12
11 It is concerned by IInd Five Year Plan (1955-1960) ‘The current levels of living in
India are very low. Production is insufficient and a large lee-way has to be made before the services and amenities required for healthy living can be brought within the reach of any significant proportion of population’. P.21. Second Five Year Plan –Draft outline – GOI Planning Commission on p.21.
12 Ist Five Year Plan – A draft outline – GOI Planning Commission (1950-55), p.57.

163
The above table suggests that even in the Independent India Health is
not being taken as a major problem. Though the constitution of India in
Articles 36-51 has enunciated in (the Directive Principles of state policy)
‘To regard the raising of the level of nutrition and the
standard of living of the people, as among its primary
duties’.
(II)
M.K.Gandhi and his Constructive Programme:
After his first Satyagraha in India in 1917 to end the cruelties of Indigo
planters on Champaran Kisans, he opened the model national schools there to
educate the poor people, having the vision that the programme would further
be launched across the country. Gandhi asked his assistants to spread the
gospel of health and sanitation among the poor.
We see initiative of poverty reduction and health improvement in M.K.
Gandhi’s Constructive program .Gandhi pleaded for building a village republic
that is a self sufficient and autonomous village. He said:
‘The village should be a self sufficient as far as its basic
needs food, clothing and other necessities are concerned.
Its economy should be planned with a view to provide full

164
employment to all the adults of the village so that no one
is forced to migrate to the towns’13
After independence the Planning Commission on India also had the
same initiative and in its (Ist five year plan) suggested in its approach to
planning:
‘In the reduction of unemployment and under
employment, cottage and small scale industries have an
important part to play’.14
Gandhi felt strongly the need for including nutrition, sanitation, and
health care in the agenda of the Congress which incorporated village nutrition,
and sanitation work as a means of improving health status.
Gandhiji said:
‘The present programme is the foundation of all round
improvement in the tottering conditions of the Seven
Lacks of Indian villages. It is the work that is long
overdue, no matter what Indian political condition is’.15
13 Shan Ghanshyam, ‘De- Centralised planning in a Centralized Economy: A study
of Sarrodya Programms’, in Petter Robb (Edited) ,Rural South Asia : Linkages change and development’ Pub. 1986. p.205.
14 Ist Five year plan 1950-55, op.cit. p.57. 15 Collected works of Gandhi, No.60, p.415.

165
He insists that health is a key to happiness he says:
‘To a true servant of humanity the question never arises as
to the best form of service when we have realized the
majesty of the moral law, we shall see how little our
happiness or unhappiness depends on health, and success,
and fame, and the like’.16
Along with health issues, village sanitation and education in health and
hygiene were also an integral part of his plan of rural reconstruction Gandhi
lamented that a sense of national and social sanitation was non-existent among
the villagers of India. He apprehended if the rules of personal domestic and
public sanitation are strictly observed and due care is taken in the matters of
health and hygiene, illness or disease would not have any occasion. Hence
Kasturba Gandhi, Ankitabai Gokhle, Anandi Bai, Manibehn Parekh and Durga
Desai organized classes in village Champaran to give the villagers lessons in
cleanliness, hygiene and sanitation besides primary education.17
Gandhi held government responsible for famines uncured in India.18
According to him heavy export of food grains and forest cutting resulted to
famines. He also urged for the promotion of small scale industries for self
employment .He opposed Industrialisation because it was creating slums.
16 Quoted from ; M.K.Gandhi, ‘Voluntary Poverty’ Compiled Ravindra Kelekar.
Pub. Navjeevan Press Ahmadabad-1961. P.30. 17 M.K.Gandhi, An Autobiography: The Story of My Experiments with Truth,
Ahmadabad, Navjeevan Publishing house, Pub. 1976p.350. 18 ‘HARIJAN’, 31st March, 1946, also HARIJAN,19th May, 1946.

166
Along with his constructive program All India Village, Industries,
Association, was also involved and Gandhi introduced the workers of AIVA
about implementing the use of unpolished rice and also regarding rural
hygiene.19
Regarding sanitation he said ‘Poverty is no bar to sanitation’. He told a
group of Shanti Nikatan students –
‘The conditions of the inhabitants of the villages would
continue to be symbolized by the garbage dumps one finds
in the villages, ‘so long as enough attention is not paid to
sanitation’.20
(III)
Poverty Reduction Strategies in Urban and Rural Areas:
After independence, in response to the poverty incidences in India many
poverty reduction strategies are adopted by the Government. India’s Poverty
Alleviation Programmes (PAPs) are run by the Government of India, the State
Governments, and the district and local authorities. Since India’s independence,
the approach to poverty alleviation has taken shape through the five-year plans.
19 ‘Hindustan Times’,(News paper) Sept., 1946. 20 C.W. 87, pp.229-30 (7 April, 1947). Amit Mishra has elaborated the Gandhian
Constructive program nicely. Please see Amit Mishra ‘Public Health Issues and Freedom Movement: Gandhi on Nutrition, Sanitation Infections, Diseases and Health Care’ in Kumar Deepak, Disease and medicine in India, op.cit., pp.249-262.

167
The Fifth Five-Year Plan (1974-79) finally addressed poverty removal as a
principal objective.
The Sixth Plan recognized the limits of the ‘income growth’ approach to
poverty alleviation. The Ninth Plan identified the importance of basic services
in poverty alleviation and placed major emphasis on basic services as (safe
drinking water, primary health facilities, universal primary education, nutrition
to school children, and shelter for the poor, road connectivity for all villages
and habitations, and the Public Distribution System).
While urban growth can be seen as positive for economy, it has many
serious problems. With the growth of cities the slum areas also grow rapidly.
Rural migrants come to the cities in search of work and settle here which
aggravates the housing problem and water supply also become adequate.
Government’s urban poverty reduction strategies have three dimensions –
Livelihood, (housing) employment, health and education.
1. Livelihood/housing:
India’s first initiative to eradicate urban poverty was the Subsidized
Industrial Housing Scheme (SIHS) in 1952. Another important development in
1954 was the establishment of National Building Organisation (NBO), the
United Nation’s regional housing centre for Economic and Social Commission
for Asia and the Pacific (ESCAP). The Slum Areas Improvement and
Clearance (SAIC) Programme was launched in 1856 for Class III and IV

168
government employees, including scavengers, gardeners and sweepers, The
Valmiki Ambedkar Malin Basti Awas Yojana (VAMBAY), 2001 tried to
identify and meet the shelter needs of the urban poor.
2. Employment:
Swarna Jayanti Shahari Rozgar Yojana (SJSRY) was launched during
the Ninth Plan. The key objective was to provide employment opportunities to
the urban poor and the jobless by encouraging them to set up self-employment
ventures or by providing different possibilities of wage employment. Many
other schemes are being run with the help of Government. The Swarna Jayanti
Shahari Rozgar Yojana was launched in 1997. The SJSRY Urban Self
Employment Programme (USEP) targeted the urban poor BPL in all towns,
unemployed and underemployed youth, 30% of which are women, and 3%
disabled. The following self-employment programmes are being run in India in
present period:-
SGSY: Swarna Jayanti Gram Swarozgar Yojna was launched with effect
from Ist. April, 1999.
JGSY: Jawahar Gram Swarozgar Yojna was introduced in April 1999.
EAS: Employment Assurance Scheme was started on 2nd October, 1993.
Food For Work Programme: was launched in February 2001.
SGRY: Swarna Jayanti Gram Rozgar Yojna was launched in September, 2001.
Annapurna: Scheme came into effect from 1st. April, 2000

169
3. Health and Education:
Cities without Slums (CWS) Programmes were developed in July 1999.
The main purpose of the CWS initiatives is to eradicate slums by upgrading
them, it also attempts to bring about better social, economic, environmental and
governance conditions within poor urban communities. Thus the CWS
initiative seeks to:
• Constructing or rehabilitating community facilities including health
centres, children’s nurseries and public open space.
• Improving access to health care, education, and social support
programmes to address issues such as security, violence, and
alcoholism and drug abuse.
At least more than 80% population is residing in rural areas. So the
percentage of poor in rural areas is far greater. Agricultural wage earners, small
and marginal farmers and casual workers engaged in non-agricultural activities,
constitute the bulk of the rural poor. Poor educational base and lack of other
vocational skills also increase poverty. The creation of employment
opportunities for the unskilled workforce has been a major challenge for
development planners and administrators. So poverty reduction strategies of the
Indian Government, in rural areas, have some dimensions i.e. providing self
employment, food (health) and land reforms.

170
Providing Self Employment:
The Integrated Rural Development Programme (IRDP) was started from
1978-79 which included training of rural youth for self employment, supply of
improved tool kits to rural artisans.
Swarnajayanti Gram Rozgar Yogna (SGRY) was started in 1999 which
aimed at organizing rural poor into self held groups. In the same years Jawahar
Gram Samridhi Yojna (JGSY) was started for the creation of rural economic
infrastructure.
We also notice the attention of Indian National Congress towards
Technical Education and Industrial Progress at its IIIrd Annual session in 1887
the Congress resolved:
‘That having regard to the poverty of the people it is
desirable that the government be moved to elaborate a
system of technical education to encourage indigenous
manufactures by a more strict observance of the orders
already existing in regard to utilizing such manufactures
for the state purposes and to employ more extensively than
at present, and talents of the people of the country’.21
Jawahar Rozgar Yojna and Jawahar Gram Samridhi Yojna utilized their
funds in creating schools buildings health infrastructure etc.
21 Resolution at the third Annual Session of INC held at Madras, 1887 (28, 29, 30th
Dec.), p.65.

171
Rural Health Programme:-
The provision of adequate medical and health services for the rural
people is not easy, but at the same time, it is very urgent. Medical care is no
doubt fundamental for health, but an adequate family income, proper food,
housing and clothing are also essential for health. Since rural prosperity
depends on agriculture, a well ordered farming economy is of prime necessity
to the assurance of adequate income for most of the rural population. In rural
areas specially health is adversely affected by unsatisfactory, insanitary and
overcrowded dwellings, and since the occupation of people living in such
dwellings goes with poverty, their effects are often aggravated by defective
diet, malnutrition and so on.
The frequency of illness in such areas in greater than those of adverse
characteristics, thus we notice marked increase in the incidence of pneumonia
and Tuberculosis and other respiratory disease. So it is essential that we should
analyse the factors affecting rural health i.e. housing, sanitation and water
supply, nutrition, sickness etc.
Housing:
As Buchanan’s survey of early 19th Century - shows that village houses
were ill ventilated; furthermore Leaky roofs, absence of flouring, ill repaired
houses, smoke and damp, form a favorable environment for respiratory illness.
The purpose of village planning is primarily to utilize the land to the best
172
advantage of the community by making suitable provision for all its needs. The
Community Project authorities have outlined the following features for village
planning, on the assumption that the average village has a population of 500
distributed in about 100 families.
(i) Two surface wells, tube wells or tanks for drinking water.
(ii) Adequate facilities for drainage.
(iii) One third of the area of the village should be kept reserved for housing.
(iv) Road system so developed as to link with the main road.
(v) School for primary education.
Water Supply and Sanitation: The surveys have also disclosed the fact
that the areas where water supply and waste disposal have been properly
attended to, cholera, typhoid, and dysentery have almost disappeared but most
villages did not have pure water so malaria was found responsible for nearly
65% of illness in rural areas.
It is therefore essential that following steps may be taken to eradicate
poverty and to implement health policies and proper sanitary measures in the
rural sectors.
The Government of India, Ministry of Health have prepared s scheme
for safe water supply and sanitation in the rural areas which will include.
(i) Construction of protected wells and other types of water supply, and making sanitary improvements in the existing wells,
(ii) Provision of Public Health Engineering consultant services.

173
(iii) Procurement and distribution of major equipment and certain other materials for the village water supply.
(iv) Helping the States with the necessary educational material.
Measures for controlling communicable diseases:
Health services for certain important communicable disease,
should be provided primarily in rural sectors. As recommended by Bhore
Committee, protective vaccinations and other preventive measures as
segregation and disinfection should be adopted.22
The Nutrition Advisory Committee established by IRFA recommends:
‘The first step in planning nutritional problems is to
estimate the average consumption of the various foods by
the population, preferably on a per capita basis. The rough
data about food intake so obtained should be checked by
family diet surveys. The state of nutrition of the population
should be investigated by the Medical and Public Health
workers’.23
Public awareness is essential because most of people are quite unaware
of the facilities provided by the government and they go to the private
hospitals. However, lack of staff and medical aids in government hospitals is
also evident.
22 Report of the health Survey and Development Committee 1945 Vol.-II,
Recommendations, op.cit., , pp.137-142. 23 Ibid., p.71.
174
‘Only 20% of Indians are covered by Public health sector of government, and the rest take resource of Private sector, which is quite expensive’.24
Public should be well aware of the nutritious value of food items and
average intake of calories for their bodies. M.M.Martin during his survey found
that the people of Bihar and Patna did not take nutritious food. Out of 52000
families in Bihar only1-64 families used to take oil in their foods and only 16-
64 families used to take milk. It suggests that most of the people were taking
under nutritious food, so they were easily subjected to diseases.
Even today people are not quite aware towards their diet. Report on
Nutritional Intake in India provides us information about daily per capita intake
of calorie, protein & Fat, by the people living in urban areas and those living in
rural areas.25 The people living in the rural areas are very much indifferent
towards in their health. Ignorance and illiteracy has been the strongest reason
for this indifferent because they are unaware of the caloric values of the food.
Even after the independence the government has not taken the initiative of
opening the governmental hospitals in remote areas. People have to rush
towards the cities for treatment but poor people hardly go due to lack of
money.
24 Guru Swami, M and Abraham, R.J., ‘Redefine poverty: A new poverty line for
New India’, in Economic & Political weekly, June 24, 2006 p.2537-38, Vol. XLI, No.25.
25 Government of India (2001): NSS Report No.471: Nutritional Intake in India, 1999-2000 National Sample Survey Organization, has prepared the following table for per person caloric intake.

175
Table-7.2: Percentage of expenditure by Indian household and per caipita intake of caloric, protein and fat per day by the average
Indian.26
Sectors % exp. on food
% exp. on cereals
Per capita Per day calorie (Keal)
Per capita Per day protein (0.0gram))
Per capita Per day fat (0.0 gram)
1 2 3 4 5 6
Rural 55.0 18.0 2047 57.0 35.5
Urban 42.5 10.1 2020 57.0 47.5
Proper vaccination programme should be run in rural areas. There
should be provision of at least one hospital within 2 kilometers radius
everywhere.
The Bhore Committee has also suggested the following measures
improve the general living conditions of people.
1. Physical Health Education
2. Health Service for Mothers and Children
3. Health Service for School Children
4. Occupational and Industrial Health Services
26 Report on Nutritional Intake in India 2004-2005, NSS, 61st Round, July 2004-June
2005, Report No.513 (61/1.0/6), National Sample Survey Organization, Ministry of Statistics and Programme Implementation, Government of India, May, 2007.

176
Poverty and Malnutrition:
Malnutrition is particularly high among poor house-holds where the
mothers have poor nutritional levels, less education, and poor access to
antenatal care The following table gives the quantities of the various food stuffs
for a well balanced diet, the usual diet of the villager, and the percentage of
people consuming below the standard level as found in a recent survey by the
Nutrition Section of the Indian Council of Medical Research.27
Table-7.3: Table showing well balanced diet, diet of the villager and the Percentage of people, consuming below the standard level.
Item of food Well balanced per day
Villagers usual diet per day
Percentage of people consuming below desired level
Cereals 14 20 41.6
Pulse 3 1 73.3
Leafy vegetables 4 2 75.8
Non-leafy vegetables 6 2 75.1
Fat 2 0.5 76.5
Milk 10 2 67.2
Meat 4 - 59.7
Sugar & jiggery 2 - 64.4
. 27 Cited in Praphulla C. Dutta, ‘Rural Health and Medical Care in India’, Published
by – Army Educational Stores Ambala, 1955.

177
As has been observed, the lowest incidence of child malnutrition is not in the
richest but in the middle income states with progressive social policy. So it
should be emphasized that social and food security policies, which improve
incomes of the poor as well as access of women to education and health care,
would reduce both poverty and malnutrition.
IV
Initiative of Improving Health Status of Females:
The status of female education in British India was very regretting. The
Census reports show the number of educated female was very less almost
negligible in comparison of males. It has been the greatest factor responsible
for social evils and health problems among the females. In poor families while
all the members suffer, it is women, particularly widows and girls members
who suffer the most. Chronic energy deficiency is generally higher among
females in most of the States of India. Mothers have poor nutritional level and
so children do not attain their full growth potential and productivity level
becomes slow.
As regards infant mortality there is no question that the death rate in the
first month is in a large measure due to improper management at the hands of
‘dais’ with an increase of trained nurses we could reasonably count on a lower
mortality. It is only by education that we can hope to cope with this evil and it

178
should be the duty of educational department to see that every potential mother
knows how to rear a child.
The three main agencies of education, in British India were the
Government Christian Missionaries and Social reformers, all of whose efforts
were directed largely in the same direction their early efforts in the 20th
Century were made mainly within the traditional frame work of Indian society.
However in the later years several measures were introduced which made
education more modern and functionally relevant for women.28
In the contemporary world it has been realized that women have a
significant role in the development society. So issues relating to female
education motherhood and Child survival needs to be understood as an integral
component of total development.
The importance of nutrition education of mothers was realized and
nutrition of the pre-school child combined with nutrition education of mother
was therefore been given priority on the nutrition programmes during the 4th
five year plan. Pandit Nehru also laid stress to it by saying:
‘The building up of a nation depends on building men and
women and the process of building men and women
depends very considerably on what is done to children. It is
therefore of high importance that we pay attention on the
28 Azra Asghar Ali, Emergence of Feminism Along Indian Muslim Women-1920-
1947.op.cit p.52.
179
well being and growth of children the basic habits formed in
the early years and the way their minds have been
conditioned then, will play an important part when they
grow up …, therefore a great deal of attention should be
paid to them.’29
Promotion of Indigenous system of Medicine:-
Indigenous medicine, religious practices and social customs are
inseparably intermingled in our daily life, especially in the villages. Of course
research in Ayurvedic, Unani and other drugs must be encouraged.
While the broad policy objectives articulated in the planning documents
have been quite appropriate, the corresponding development programmes have
not been very effective in achieving the objectives. In brief review of the
policies and programmes for the development of urban and rural areas both
presented in this chapter shows that the policy objectives need to be clearly
defined. The strategies to achieve the objectives should be more approachable.
However, the success of this effort will largely depend on what action
programmes are developed and how they are implemented.
29 Quoted from National Health Seminar ‘On the role of the Voluntary agencies in
the implementation of Public Health Medical Care and Family Planning Programmers, Deco., 29-31, 1965, by Dr. R. Karnad- Nutrition in the Fourth Five Year Plan, p.47.







