
PASSIVE LEG RAISING: An indicator of fluid responsiveness in sepsis
Dr. Soumar Dutta MD (PG), Dr. V.P Chandrasekharan, M.D (A&E), Dip (A&E), HODDepartment of Emergency and Critical Care Medicine
Vinayaka Missions Hospital, Salem

• The clinical determination of the intravascular volume can be extremely difficult in critically ill patients, specially those in sepsis.
• Early aggressive resuscitation of critically ill sepsis patients may limit and/or reverse tissue hypoxia, progression to organ failure, and improve outcome.
Introduction

End point resuscitation
• Central venous pressure 8-12 mm Hg• Mean arterial pressure (MAP) ≥ 65 mm Hg• Urine output ≥ 0.5 ml/kg/hr.• Central venous (Superior vena cava) or mixed venous
oxygen saturation 70 % or 65% respectively
End point resuscitation

Aim
To assess whether passive leg raising can help in predicting fluid responsiveness in patients with sepsis and acute circulatory failure.

Methodology
• Study design: Prospective, analytical study conducted in the
emergency room and intensive care units of a multispecialty teaching University in Salem.
• Study period:July 2012 to August 2013

Methodology
• Study group: The study population were subjected to following limitations:
Inclusion criterias:All cases of sepsis • Age > 18 years• Circulatory failure
Exclusion criterias:• Arrhythmias• Pelvic/lower limb fracture• Parturient• Amputation of the lower limbs• Clinical or radiological evidence of mediastinal mass • Pneumothorax/hydrothorax

Methodology
• Data collection: Study measurements were taken in four stages. 30
ml/kgHemodynamic indices:
• Stroke volume (SV) using 2D echocardiography

MethodologyStroke volume assessment using 2D ECHO
Stroke volume = LVOT area x Quantity of blood across LVOT
Parasternal long axis view
LVOTDiameter
LVOT = Left Ventricular Outflow TractVTI = Velocity Time Integral
π x (diameter)2
Stroke Volume = ------------------------------ x LVOT VTI 4

MethodologyStroke volume assessment using 2D ECHO
π x (diameter)2
Stroke Volume : ------------------------- x LVOT VTI 4
Apical 5 chamber view

Methodology
Septic shock
Fluid bolus by treating physician
Stroke volume assessment with and without PLR
Treating physician who give bolus is blinded to ECHO findings

Haemodynamic changes in passive leg raising
Blood shifts toward the intrathoracic compartment
45°
Methodology

Frank-starling principle
Stroke volume
Ventricular preload
normal heart
failing heart
Preload-dependence
Preload-independence

Terminologies
Those who had ≥15% increase
in SV is considered as
predicted response
Those who had <15% increase
in SV is considered as predicted no
response
Those who had any increase in blood pressure considered as
responsive
Those who had no increase in blood pressure considered as
non responsive

Results
A total of 116 patients were evaluated out of whom 73 were fluid responders.
Responders
Non-responders
43 (37%)
73 (63%)
n = 116
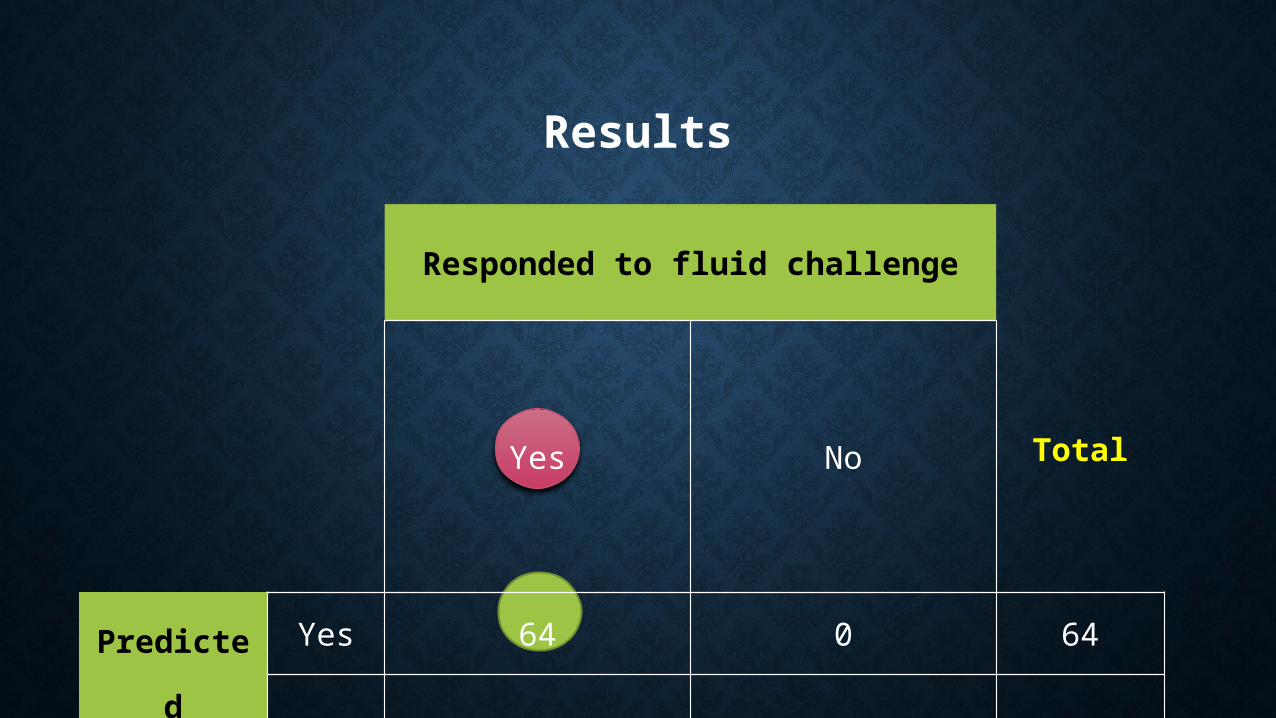
Results
Responded to fluid challenge
TotalYes No
Predicted
Response
Yes 64 0 64
No 9 43 52
Total 73 43 116

Series1
0
10
20
30
40
50
60
70
BEFORE
Stroke Volume(∆SV) among fluid responders before and after PLR
Results
n=73
Before Volume Expansion

Series1
0
10
20
30
40
50
60
70
80
Before After
After volume expansion
Results
VE (30ml/kg) :Stroke volume before and after PLR
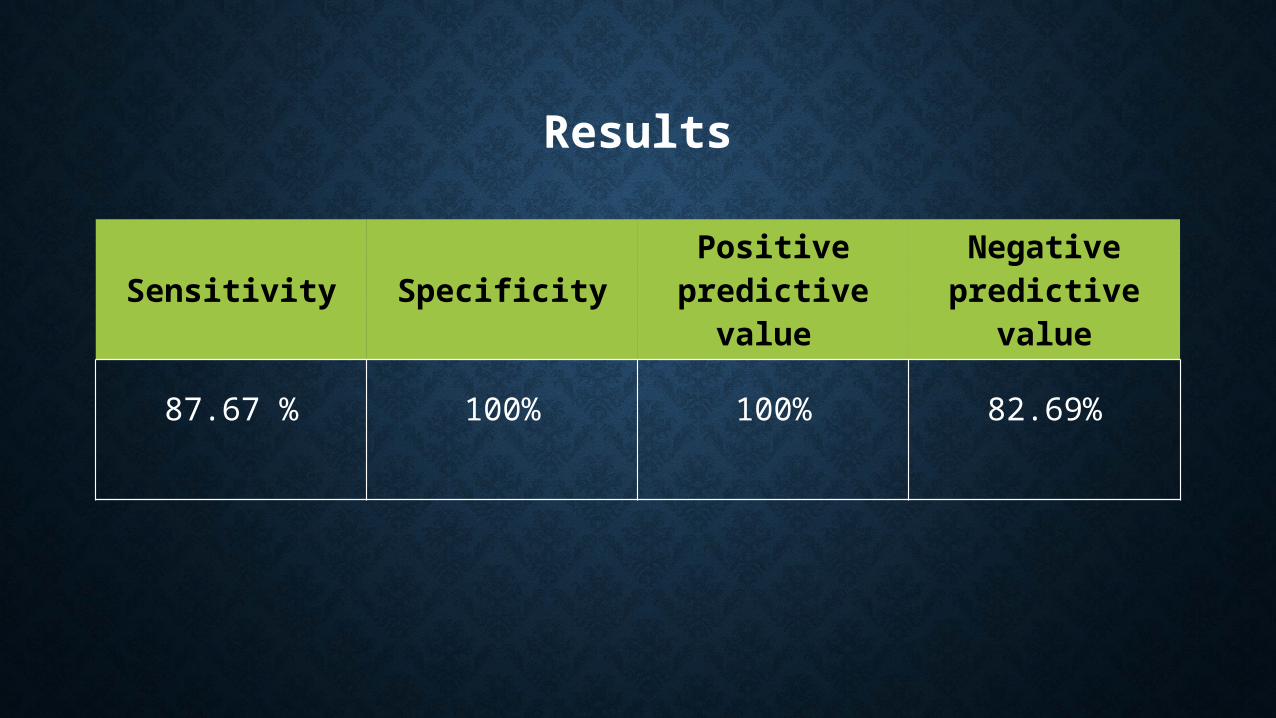
Results
Sensitivity SpecificityPositive
predictive value
Negative predictive
value
87.67 % 100% 100% 82.69%

Conclusion
• A simple, non-invasive bedside test for volume responsiveness which challenges patient’s own “Frank-Starling curve”• Brief and completely reversible “self volume challenge” . • Reduces the use of vasopressors and overzealous fluid
administration.• Can be repeated over in the same patient.

Thank you







