
Safaa Soliman Ahmed Lecturer of Maternal and Newborn Health Nursing
Faculty of Nursing – Beni-Suef university

A New Call for the Prevention of Primary Cesarean Delivery

Introduction Worldwide rise in cesarean section (CS) rate during the last three decades, has been the cause of alarm and needs an in depth study. CS is one of the most common major surgical procedure in private sector health care services. The CS epidemic is a reason for immediate concern and deserves serious international attention

Balancing risks and benefitsCs can be lifesaving for the fetus, the mother , or both in certain cases
For placenta previa or uterine rupture:
Cs is firmly established as safest route of delivery .

For low risk pregnancy cs has greater risk of maternal morbidity and mortality than VD
Risk of sever maternal morbidities:
hge that requires hysterectomy or transfusion,
Uterine rupture
hospital wound disruption Anesthetic complication :shock .cardiac arrest, acute renal failure , assisted ventilation
Venous thromboembolism
Major infection in wound or hematoma compared with VD
Long term risks associated with csPlacental abnormalitiesPlacenta previa , in future pregnancies increases with each sub sequent CS ,from 1%with 1 prior Cs to 3% with 3 prior CS.
After 3 CS , the risk of placenta privea will be complicated by placenta accreta is nearly 40%

Neonatal complications
Neonatal intensive care unit
admission
Perinatal death .
The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine identify many ways to safely reduce the chance of cesarean birth. They focus on preventing “primary” or initial cesareans in pregnant women who have never had a cesarean
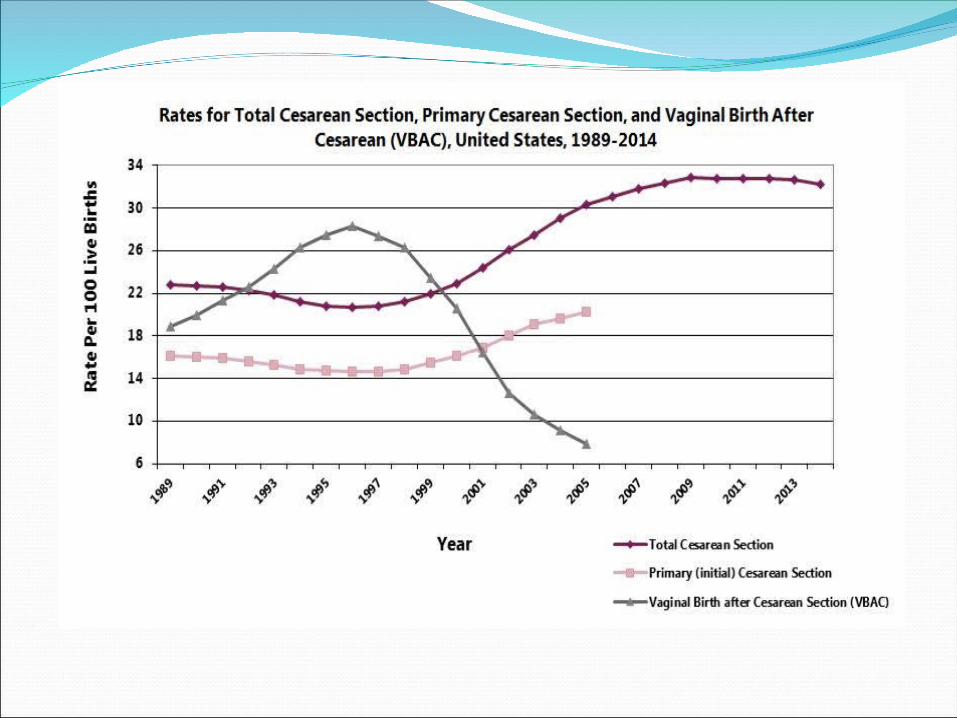
In 2011, one in three women who gave birth in the United States did so by cesarean delivery
However, the rapid increase in cesarean birth rates . from 1996 to 2011 without clear evidence of concomitant decreases in maternal or neonatal morbidity or mortality raises significant concern that cesarean delivery is overused
Therefore, it is important for health care providers to understand the short-term and long-term tradeoffs between cesarean and vaginal delivery, as well as the safe and appropriate opportunities to prevent overuse of cesarean delivery, particularly primary cesarean delivery.
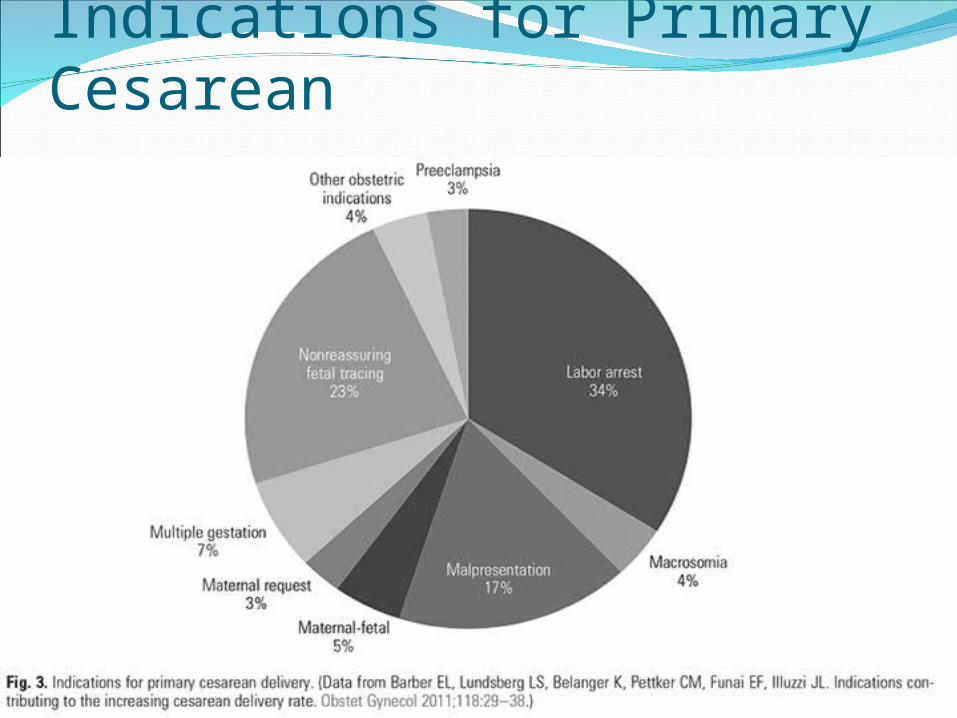
Indications for Primary Cesarean
Definition of Arrest of Laborin the First StageSpontaneous labor: More than or equal to 6 cm dilation with membrane rupture and one of the following:
4 hours or more of adequate contractions (eg, more than 200 Montevideo units)
6 hours or more of inadequate contractions and no cervical change
Safe reduction of the rate of primary cesarean deliveries (2014)some intrapartum care practices promote vaginal birth,
Continuous one-to-one support and midwifery management are associated with lower cesarean section rates.
. Strategies that can be implemented in the current social and cultural setting of obstetrics today are recommended.

Maternal request
Public :Health awareness ,education, media involvement
Patient :
1- Benefits and risks of cs compared with
vaginal birth should be discussed and
recorded.
2- A fear of childbirth :counseling (cognitive,
behavioral therapy for reduced fear of pain
in labour and shorter labour
Clinician Has the right to decline a request for CS in the absence of an identifiable reason
The women decision should be respected and she should be offered referral for second opinion
Continuous labor support, such as labor doula care, reduces risk of cesarean.
Cesarean is not appropriate even for most babies that are estimated to be large near the end of pregnancy (estimates are often wrong, and many large babies are born vaginally).

If a baby is breech (buttocks- or feet-first) at about 36 weeks of pregnancy, hands-tobelly movements to turn babies head-first (“external cephalic version”) should be offered.
Women with twins and the first twin head-first should be encouraged to plan a vaginal birth.

Women who are counseled about avoiding excess pregnancy weight gain may be able to avoid a cesarean.
Women who have had herpes simplex virus. should plan a vaginal birth if the virus is inactive at labor.

Other ways to lower the chance of having a cesarean
Research suggests that : Having a care provider or group and giving birth in a setting with relatively low cesarean rates
Women and care providers working together to delay hospital admission until labor is well under way
Using “intermittent auscultation” – periodic listening with various devices – to monitor fetal heart patterns rather than continuous electronic fetal monitoring during labor
Staying upright and moving around in labor before the pushing phase, which is especially possible without or before the use of epidural pain relief








