
Multisystemic Therapy 04/00
Multisystemic Therapy (MST)
For additional information seewww.mstservices.com

Multisystemic Therapy 04/00
Primary Goals of MST Reduce youth criminal activity Reduce other types of antisocial
behavior such as drug abuse and sexual offending
Achieve these outcomes at cost savings by decreasing rates of incarceration and out-of-home placements

Multisystemic Therapy 04/00
MST Research and Dissemination Family Services Research Center (FSRC)
Research Center at the Medical University of South Carolina (MUSC), Dr. Scott Henggeler, Director
MST Services MUSC affiliated organization offering assistance in MST
program development and training through licensing agreements with the MUSC and the FSRC
MST Institute Independent non-profit organization providing quality
control expertise, data, and tools to all interested parties

Multisystemic Therapy 04/00
MST “Champions” & Advocates OJJDP - Office of Juvenile Justice and
Delinquency Prevention Washington State Institute of Public Policy
MST: most cost effective approach to reducing crime
“Blueprints for Violence Prevention” MST selected as one of the 10 “Blueprint”
programs by Delbert Elliott, Center for the Study and Prevention of Violence, University of Colorado
Multisystemic Therapy 04/00
MST Research and Development
Theoretical underpinnings Research findings on delinquent
behavior MST research findings

Multisystemic Therapy 04/00
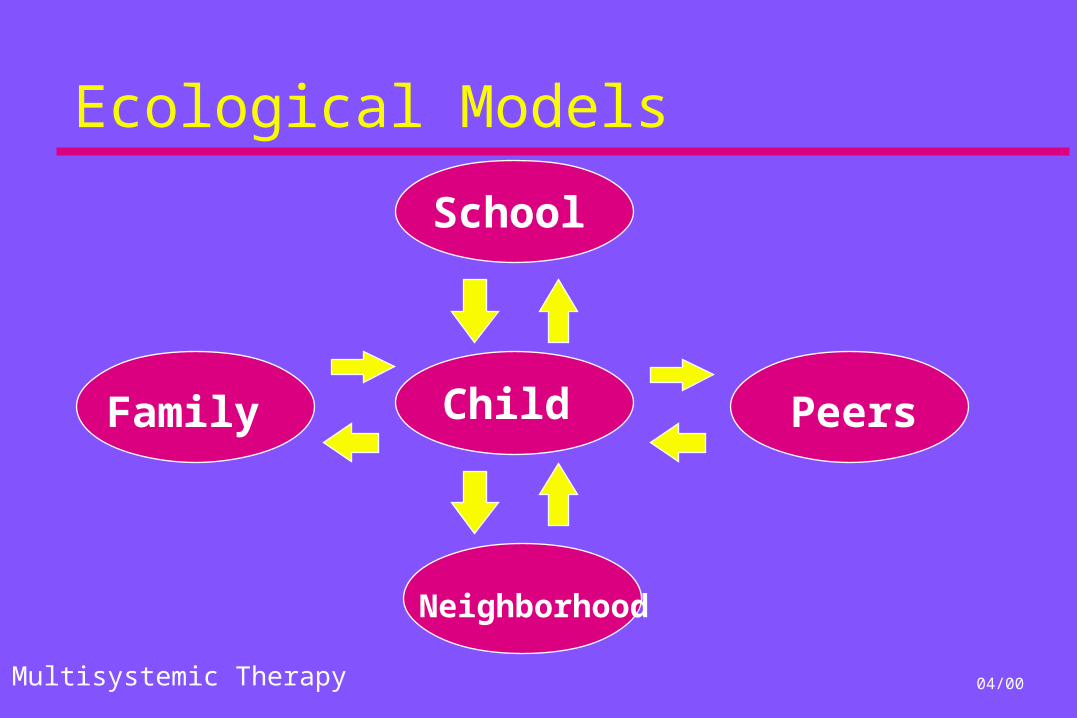
MST Theoretical Assumptions
Children and adolescents are embedded in multiple systems that have direct and indirect influences on their behavior.
Influences are reciprocal and bi-directional
Based on Bronfenbrenner, Haley , and Minuchin
Multisystemic Therapy 04/00
Ecological Models
Child
Neighborhood
Family Peers
School

Multisystemic Therapy 04/00
Ecological Models
Child
Family
Peers
School
Neighborhood
Treatment Providers

Multisystemic Therapy 04/00
Causal Models of Delinquency & Drug Use
Condensed Longitudinal Model
Family
School
DelinquentPeers
DelinquentBehavior
Prior DelinquentBehavior
Low Parental MonitoringLow AffectionHigh Conflict
Low School InvolvementPoor Academic Performance
Elliott, Huizinga & Ageton (1985)
-
-
+
+
Multisystemic Therapy 04/00
Needs of Violent & Chronic Juvenile Offenders and Their Multiproblem Families
Improve parental discipline practices Increase family affection Decrease association with deviant peers Increase association with prosocial peers Improve school/vocational performance Engage in positive recreational activities Improve family-community relations Empower family to solve future difficulties

Multisystemic Therapy 04/00
The Missouri Delinquency ProjectCharles M. Borduin, (PI), University of
MissouriBarton J. Mann, University of Illinois - Chicago
Lynn T. Cone, University of MissouriScott W. Henggeler, Medical University of South
CarolinaBethany R. Fucci, University of MissouriDavid M. Blaske, University of Missouri
Robert A. Williams, University of Missouri

Multisystemic Therapy 04/00
Participants: 200 Offenders and Their Families
Averaged 4.2 previous arrests 64% had been incarcerated previously
for at least 4 weeks Average age = 14.8 years 67% male, 33% female 30% African-American, 70% Caucasian 47% lived with only one parental figure

Multisystemic Therapy 04/00
Service/Treatment Options
Multisystemic Therapy 77 completers 15 dropouts
Individual Therapy 63 completers 21 dropouts
Usual probation services for refusers 24 refusers
Multisystemic Therapy 04/00
Service Delivery vs. Treatment
Service Delivery Models
Family Preservation
Inpatient Outpatient Residential
Treatment Foster Care
Treatment Models
Multisystemic Therapy
Cognitive Therapy Family Therapy Psychodynamic
Therapy Behavior Therapy

Multisystemic Therapy 04/00
Delivery of Multisystemic Therapy Treatment Site In the field (home, school,
neighborhood and community)
Treatment Total behavioral health care
Treatment Duration 3 to 5 months in most cases
Case Management Function Service provider rather than brokerof services
Provider Single therapist (as part of &supported by generalist team)
Clinical Staff: Client Families 1:4-6 (avg. 15 families/ yr/ therapist)
Staff Availability 24 hr/ 7day/ wk team availability
Treatment Outcome Responsibility of staff & agency
Expectations of Outcome Immediate, maximum effort byfamily & staff to attain goals

Multisystemic Therapy 04/00
MST Case Example
15 year old minority youth Referral to MST for truancy,
aggressive behavior at home and school, multiple shopliftings, and drug abuse
Lives with mother, stepfather, and three younger siblings

Multisystemic Therapy 04/00
MST Treatment Principles
Nine principles of MST intervention design and implementation
Treatment fidelity and adherence is measured with relation to these nine principles

Multisystemic Therapy 04/00
Principles of MST
1. Finding the FitThe primary purpose of assessment is to understand the “fit” between the identified problems and their broader systemic context.
2. Positive & Strength FocusedTherapeutic contacts should emphasize the positive and should use systemic strengths as levers for change.

Multisystemic Therapy 04/00
Principles of MST
3. Increasing ResponsibilityInterventions should be designed to promote responsibility and decrease irresponsible behavior among family members.
4. Present-focused, Action-oriented & Well-definedInterventions should be present-focused and action-oriented, targeting specific and well-defined problems.

Multisystemic Therapy 04/00
Principles of MST
5. Targeting SequencesInterventions should target sequences of behavior within and between multiple systems that maintain identified problems.
6. Developmentally AppropriateInterventions should be developmentally appropriate and fit the developmental needs of the youth.
Multisystemic Therapy 04/00
Principles of MST
7. Continuous EffortInterventions should be designed to require daily or weekly effort by family members.
8. Evaluation and AccountabilityInterventions efficacy is evaluated continuously from multiple perspectives, with providers assuming accountability for overcoming barriers to successful outcomes.

Multisystemic Therapy 04/00
Principles of MST
9. GeneralizationInterventions should be designed to promote treatment generalization and long-term maintenance of therapeutic change by empowering care givers to address family members’ needs across multiple systemic contexts.

Multisystemic Therapy 04/00
Instrumental Outcomes at Post-treatment
Increasing family cohesion and adaptability
Increasing family supportiveness Decreasing family hostility Decreasing parental symptomatology Decreasing behavior problems in youth
Multisystemic Therapy was significantly more effective at:
Multisystemic Therapy 04/00
Ultimate Outcomes at Four-Year Follow-Up
Preventing violent offending Preventing other criminal offending Preventing drug-related offending Decreasing seriousness of committed
crimes
Multisystemic Therapy was significantly more effective at:
Multisystemic Therapy 04/00
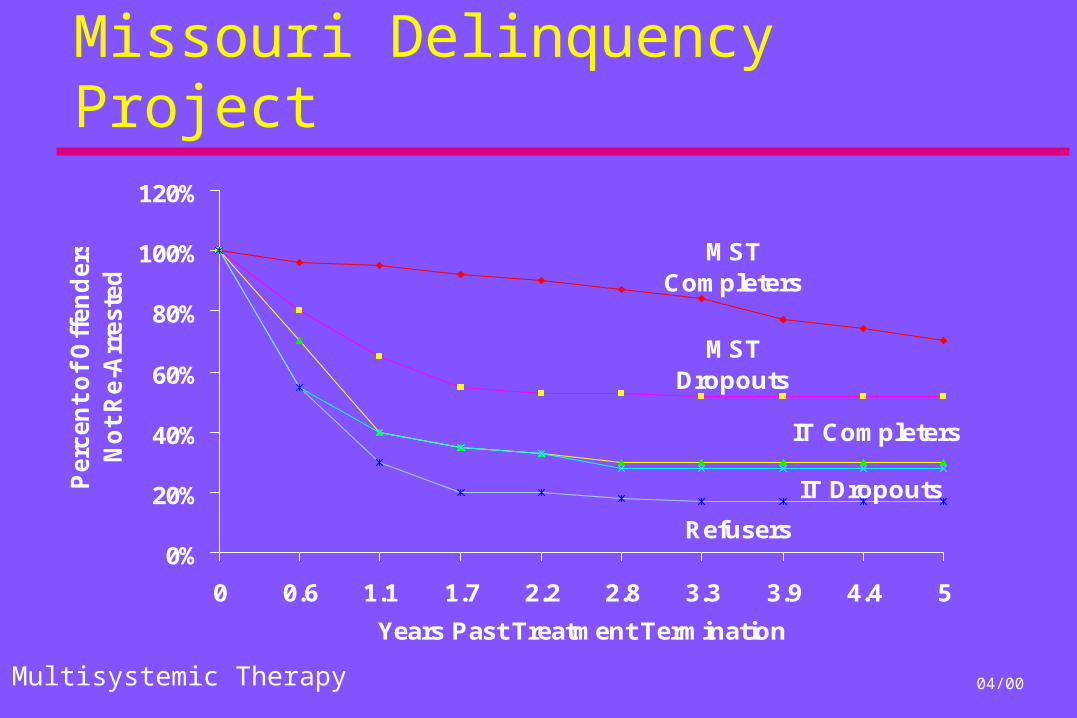
Missouri Delinquency Project
MSTCompleters
MSTDropouts
IT Completers
IT Dropouts
Refusers0%
20%
40%
60%
80%
100%
120%
0 0.6 1.1 1.7 2.2 2.8 3.3 3.9 4.4 5
Years Past Treatment Termination
Perc
en
t o
f O
ffen
ders
No
t R
e-A
rreste
d

Multisystemic Therapy 04/00
The Role of Treatment Fidelity
Standard Training for MST clinical staff
5-Day on-site orientation to MSTWeekly MST consultations:
viewed as the core of the training program -- true on-the-job training
Quarterly on-site booster training
Multisystemic Therapy 04/00
The Role of Treatment Fidelity
Examined the effects of MST in the absence of ongoing weekly MST consultation.
Adherence measure: 26 item questionnaire completed by the youth’s caregiver/parent.
Results: adherence to the MST treatment model varied greatly without weekly MST consultation.
Client outcomes: where treatment adherence was high, outcomes were substantially better.
Multisystemic Therapy 04/00
The Role of Treatment Fidelity
MST treatment adherence predicted:
decreased criminal activity decreased incarceration decreased adolescent emotional
distress increased parental emotional distress

Multisystemic Therapy 04/00
The Role of Treatment Fidelity
Implications of research: High adherence is essential for obtaining
outcomes with difficult clinical populations Traditional training and supervisory protocols are
not sufficient for obtaining high adherence To obtain the strongest possible outcomes, MST
programs should “institutionalize” adherence monitoring and on-going training for staff

Multisystemic Therapy 04/00
Bridging the Gap: University to Community
University-based research projects often show promising results which can not be replicated by community-based programs
MST has successfully made this transition Positive university-based research Positive community-based research Focusing on the implementation of effective
community-based MST programs

Multisystemic Therapy 04/00
Community-based Dissemination Efforts
Program Replications California Connecticut Colorado Delaware* Florida Ireland (No.) Kansas Louisiana Manchester (UK)
Maryland Michigan* Minnesota Missouri New York* Nebraska North Carolina Ohio*
* Clinical Trials
Oregon Pennsylvania* South Carolina* Tennessee* Texas* Washington Washington D.C. Ontario, Canada* Norway*
Multisystemic Therapy 04/00
Critical Elements of Implementation
Continuous Focus on Outcomes Fidelity to the Treatment Model Accessibility of Treatment
What influences these critical elements? Interagency collaboration Organizational support of the program Operational practices and policies

Multisystemic Therapy 04/00
Influences of Other System Stakeholders
Funding structure in place Ability of MST therapist to take the
“lead” in clinical decision making Key stakeholders usually include:
Juvenile Justice, Family Court, Mental Health, Social Welfare, School systems, parent groups
Clearly defined target population, program goals, and referral process

Multisystemic Therapy 04/00
Influences within the Provider Organization
Clear understanding of MST at all levels Commitment to implement MST fully Target MST compatible populations Willingness to modify policies and
dedicate resources to achieve outcomes Commitment to training and supervision Policies (e.g. flex-time, transportation) Resources (e.g. pay, cellular phones)
Multisystemic Therapy 04/00
Influences within the Clinical Context/Team
Clinical supervisor: committed, credible authority Distinct and dedicated MST staff Low caseloads (4-6 families per clinician) Weekly group supervision per MST protocol Weekly MST consultation for clinical team Adequate on-call coverage system MST training for all staff who can influence treatment Outcome-based discharge criteria Therapists: strengths and barriers

Multisystemic Therapy 04/00
Why is MST Successful? Treatment targets known causes of
delinquency: family relations, peer relations, school performance, community factors
Treatment is family driven and occurs in the youths’ natural environment
Providers are accountable for outcomes Therapists are well trained and supported Significant energies are devoted to developing
positive interagency relations







