
PHARMACOVIGILANCE-COLLABORATION WITH WHO (VIGIFLOW) AND DOH (APP)
Mrs P NkambuleDirector: Clinical Evaluations and Trials
SAAPI CONFERENCE 13 – 14 APRIL 2016 CSIR
PRESENTATION TITLE

LAYOUTBackground on PharmacovigilanceContributions made by pharmaceutical industryGlobal trends in PharmacovigilanceCollaboration with WHO‐UMC ()– Vigiflow– E2B Imports– eReportingCollaboration with NDOH (App)– RPV vs PPV

Pharmacovigilance A common understanding?
Pharmacovigilance: the science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other drug‐related problems.
The Importance of Pharmacovigilance: WHO 2002

Pharmacovigilance includestectionSignalsDiagnosis of ADRsSpontaneous Reporting Other surveillance and research methods (cohort, case control, PEM, record linkage studies, registries etc)
sessmentResearch – signal strengthening and signal validationCausality Assessment, severity, extent of the problem, preventabilityRisk factors, biological mechanism, public health impactderstanding Education and training
evention Communication and trainingHealth system changesEducation
Rs and drug‐related problemsADRs (serious and non‐serious, expected and unexpected)Medication errorsSystem failures causing ADRs

A Changing environment in South Africa…Case for a Holistic approach to pharmacovigilance
t South Africans has access to the internet (and all the stuff ’s on it!)Age of “Blockbuster” drugs – aggressive marketing practicesatient: “I’ll tell you what to prescribe for me”ep: “Our new product is safer than the older version”The Mercedes Benz of antihypertensives”e potions and immortality elixirslifestyle drugs”ts and shoots (evolving traditional medicine use)
nterfeit medicines and illegal drugsw Regulatory Authority ‐ SAHPRA

What is Scale of the Problem?

00 000 deaths per year in US due to ADRs – (4th highest cause of mortality in USA) (Lazarou).99 errors per 1,000 medication orders (IOM port)
Medication error or adverse effect in 50% of urgical procedures (Mass Gen Hosp)pprox 6-8% of all SA hospital admissions are ue to adverse reactions (Mehta, Mouton)
– excluding..overdoses, drug abuse-related i d di i !
Few Shockers….

AlgeriaIndia
Turkey
Yemen1997
rogrammatic error
Insulin given to 70 infants instead of DPT vaccine with 21 deaths
TT DTP

macovigilance issues are the motivators for changeADRs are often symptoms of a bigger problem..
halidomide…need for regulation of medicines (Regulation)hylene glycol poisonings ‐ product quality problems (GMP)goxin deaths in France…higher doses usedJohn’s Wort/ kava kava ‐ “natural” “safe”…phytovigilancecase of date‐rape... unfolds a new culture of drug abuse –Rohypnol”.eloxicam ‐ fatal GI haemorrhages in France… advertised as safer n the stomacheaths after immunisation... dangerous storage practice

ontributions made by the Pharmaceutical Industry
Responsible from “conception to resurrection” (and beyond)…
Technological advances in development of safer medicines.
Innovative in‐house signal detection systems and databases.
Growing awareness of safety and increasing resources committed to these activities.
Improved communications and information with regulators, patients and the public.

Global trends in PVMore proactive– Risk management – PEM/CEM, registries, hospital surveillance– Targeted studies More accessible– Online reporting using Apps– Transparent, searchable, national databases– Websites with updated safety informationMore shared– More players involved – NGOs, consumer groups, patient networks, clinical societies, other governmental bodies, veterinary and environmental groups

Pharmacovigilance in South Africa… Where are we?

ICSR management systemUsed for:– Data entry/import– Assessment– Storage– Retrieval (e.g. follow‐ups)– Line listings, statistics– Data exchange ICSR = Individual Case Safety Report

NADEMC /RPV unit at NDOH
UppsalaMonitoring Centre (UMC)CC
ublic
National DRAs and Pharmacovigilance Centres
stry of Health
1. processing
y
UCT/MIC
The world tour of the ADR form

OLLABORATION WTH WHO ‐ UMC (VIGIFLOW)

he Uppsala Monitoring Centre (UMC)
Foundation established 1978
• Agreement Sweden – WHO
• International board
• WHO-HQ providing policy
• WHO Programme• Centre of excellence for
pharmacovigilance

WHO Programme MembersUppsala, Sweden
18

National Pharmacovigilance Centre
VigiBase -WHO international
database of suspected adverse drug reactions
VigiLyze
The flow of ICSRs in the WHO Programme

National PV Centres
Data analysis and feedback
WHO globalICSR database
Vi iB ®
Search & analysis tool VigiLyzeTM
UMC Signal detection
National ICSR databasese.g. VigiFlow®

What is VigiFlow®?
An Individual Case Safety Report (ICSR) management system

Vigiflow ...Developed by Uppsala Monitoring Centre UMC). Compatible with the ICH‐E2B standard for electronic transmission of ICSRs. Web based and accessible over the Internetia an encrypted (https) connection. Different access rights and password control

VigiFlow
Facilitates quality of data entry– Error checks and lexicons– Mandatory fields– Help texts
Integrated terminologies facilitates drug and ADR coding
Easy communication between regional and national centres
Available in four different languages
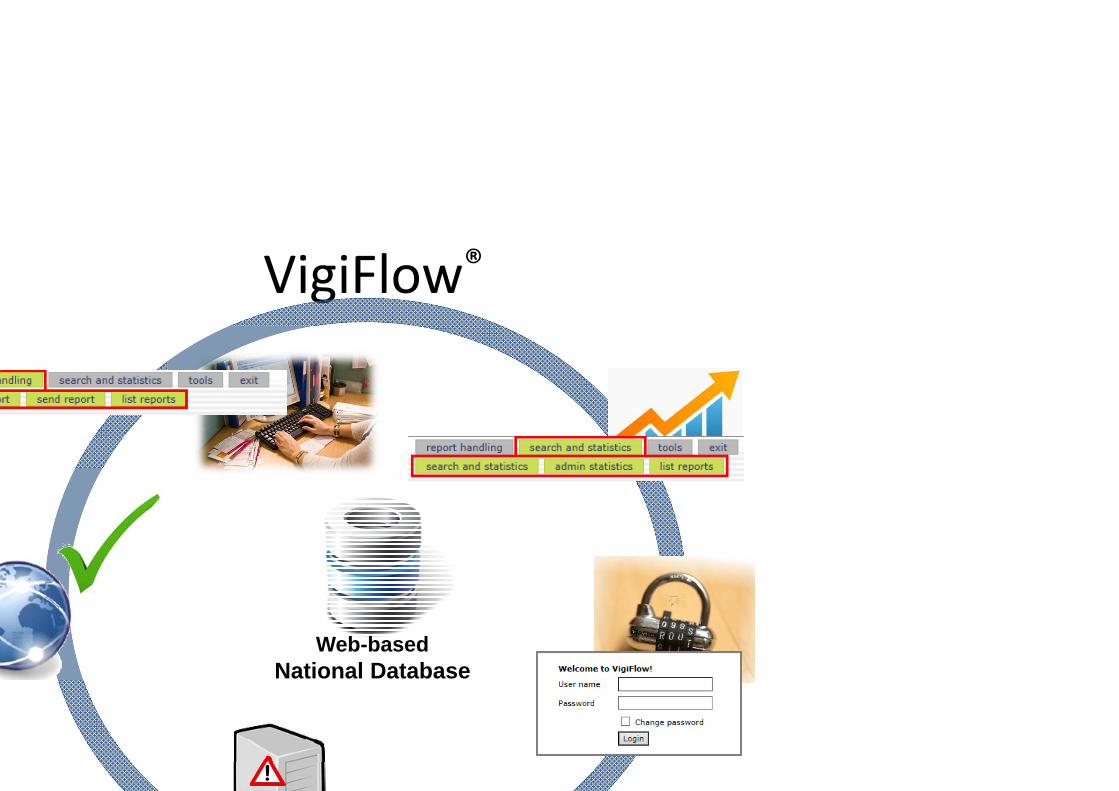
VigiFlow®
Web-basedNational Database

VigiFlow®
Language options
User guide
Top menu
Side menu

Built in qualitySupport (help pop‐ups, user guide)Mandatory fields– Receive date– Age at onset + patient initials– Drug– Reaction + start year of reactionTerminology and dictionary look up toolsData entry overview page and audit trailEncrypted access (https://) via internetTraining available online and in person

VIGIFLOW DATABASE
Mandatory fields ‐minimum information on a spontaneous report for it to be considered complete’ Until all mandatory fields in the report are filled in, it is considered incomplete and cannot be committed to the Search and Statistics database.

Data entry

ICSR databaseSearch, analyze and export national data

Search and Statistics
Committed (finalized) reports are available in the Search and Statistics module• Predefined output types (profiles)
– Line listings– Statistics– Administrative statistics
• Possible to save queries• Export to Excel for further analysis

Electronic ICSR exchange
VigiFlow is fully compatible with the ICH E2B formatCH E2B = international standard for transmission of ICSRs between database systems)

E2B import
Only correct E2B files in xml format can be mported. f the file is incorrect an error message will appear There is also an option to generate report Id(s) during import. The generated report Id(s) will then be included in the acknowledgment file for follow‐up reports report Id of the already

E2B IMPORT
All imported reports get the title "Import: [first reaction], [first drug]“Each imported report needs to be checked before it is committed. To erform the check, the report is opened for editing.

ACKNOWLEDGEMENT

VIGIFLOW E‐REPORTING
e‐Reporting is a newly released module for Vigiflow data management system which allows capturing of ICSRs directly from the source into the Vigiflow database.This could be achieved by creating an open ink on the MCC website. The open link transfers data automatically to Vigiflow database.

eReporting continues...Newly released module for Vigiflow data management system which allows capturing of ICSRs directly from the source into the Vigiflow database
-achieved by creating an open link on the regulator’s website.
-open link transfers data automatically to Vigiflow database.
-Only minor manual data entry
- No delay in receiving the reports
-Available to NCs using VigiFlow

eReporting continues...Translations
Place holder for the “open link”


Advantages of Electronic formatMandatory fields (complete reports)Automatically imported into DatabaseDrop‐down listUse of free –textsAttachment of Photos & reportMore time for coding verification, causalityassessment and signal identification.

COLLABORATION WITH NDOH (APP)

EGULATORY VS PROGRAMMATIC Pharmacovilance
rious roles and functions between the regulatory and programmatic pharmacovigilance

Regulatory Programmatic
Medicine used in the programmeAll medicines
SAFETYMedicines
Patients
Medicine used in the programme does not cause harm
Quality & Efficacy of all medicines
Methods: Methods:
Regulatory/programmatic pharmacovigilance

Regulatory PharmacovigilanceRestriction measures in order to reduce the risk. The measures may include: safety alerts (that get published in scientific journals), press releases (published in the media to alert the public), and Dear Healthcare Professional letters (addressed to healthcare professionals).
Up‐scheduling, labelling restrictions, product recalls (quality)Cancellation of registration

Programmatic Pharmacovigilance
Rationale use of drugs in progammesEvaluate the impact of programmenform guidelinesReeducation/training of staff

NDOH MOBILE APP

How to download the PHC clinical guideline APP



ow to report ADRs using the APPAfter downloading PHC clinical guide,Select the tools tabSelect report Adverse Drug Reaction tabReport the ADR tab has drop down menus and selection criteria where possibleStructured to give balance for sufficient information On successful completion, a copy of the report will be sent to he reporter and NDOH.Currently working on designing a single uniform APP that will be suitable for regulatory, programmatic and sector wide procurement needs nformation will be received by the relevant departments

CONCLUSION
Pharmacovigilance is a shared responsibilityCollaboration is very criticalGlobal trends ICSR databaseApps

Acknowledgements
Dr Joey GouwsProf M BlockmanDr Ushma MehtaMr Mukesh DhedhaThe Uppsala Monitoring Centre (UMC)

Thank You!







