
MINDFULNESS TRAINING FOR ADOLESCENTS WITH ADHD AND THEIR FAMILIES: A TIME-SERIES EVALUATION
by
Carly Shecter
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Department of Human Development and Applied Psychology Ontario Institute for Studies in Education
University of Toronto
© Copyright by Carly Shecter 2013

ii
MINDFULNESS TRAINING FOR ADOLESCENTS WITH ADHD AND THEIR
FAMILIES: A TIME-SERIES EVALUATION
Doctor of Philosophy, 2013
Carly Shecter
Department of Human Development and Applied Psychology
University of Toronto
Abstract
The present study involved an extension and evaluation of a mindfulness-based training
program for families of adolescents with Attention-Deficit/Hyperactivity Disorder
(ADHD). MYmind: Mindfulness training for Youth with ADHD and their parents
(Bogels et al., 2008) is an eight-week manualized treatment incorporating elements of
mindfulness meditation, ADHD psychoeducation and cognitive behavioural therapy.
MYmind focuses on helping families cultivate mindfulness through training in formal
meditation practices and integrating this skill into the context of everyday life as a means
of managing ADHD symptoms, stress, family relations and difficult emotions. A North
American sample of 13 parents and 9 adolescents (ages 13-18) participated in MYmind;
during the intervention, parents and adolescents attended separate groups that ran
simultaneously. Using a time-series multiple baseline design, constructs of stress, distress
from family conflict, ADHD symptomatology and meditation practice were measured via
short questionnaires emailed daily to both parents and adolescents throughout baseline,
treatment and six months of follow-up. For multiple baseline purposes, intervention was
introduced in a time-lagged fashion. Results from parent and adolescent reports indicated

iii
reductions in parent and adolescent stress, parent and adolescent distress due to family
conflict, and increased frequency and duration of meditation practice. Parent reports
suggested a decrease in their adolescents’ inattention, hyperactivity and impulsivity
symptoms after participating in MYmind, a reduction that was not confirmed by
adolescent reports. Most treatment gains were maintained up to six-months following
treatment completion. Meditation practice was significantly correlated with reduced stress
levels for both groups. Both parents and adolescents reported high satisfaction with the
MYmind program overall. Mindfulness training appears to hold considerable potential for
improving the multiple difficulties experienced by adolescents with ADHD and their
parents.

iv
Acknowledgements
I am indebted to a number of people who were instrumental in assisting me with the
completion of my dissertation. Firstly, I would like to express my sincere gratitude to my
thesis advisor, Dr. Joe Ducharme, for his guidance and encouragement throughout my
graduate education. Joe provided my first passionate introduction to mindfulness; he was
both a teacher and mentor through this process. A tremendous thank you also goes to Dr.
Judy Wiener, who has played such a large role in this project from brainstorming to
completion. Judy has continuously provided me with support and counsel since my first
year at OISE. I would like to express appreciation to my committee member, Dr. Jack
Miller for his valuable feedback. A thank you also goes to Dr. Susan Bogels for allowing
me the opportunity to contribute to the growth of her innovative program.
This research would not have been possible without the attention to detail,
organization and kindness of our lab manager, Ashley Brunsek. I would also like to offer
a thank you to Jill Haydicky for her collaboration, continual support and friendship
throughout the last 6 years. She has been my partner in crime on this project and I cannot
wait to see what endeavors we take on next.
To my parents, for their unwavering support and belief in me throughout graduate
school. Thank you for teaching me the value of determination, hard work and patience.
You told me I could accomplish anything I put my mind to, and I did.
Lastly, I would like to express my appreciation to the families who participated in
the MYmind program. They illustrated the true power of attention and acceptance through
their cultivation of mindfulness in their relationships and daily life. I can only hope that I
have impacted their lives and understanding of themselves as they have done for me.

v
Table of Contents
Abstract ............................................................................................................................... ii
Acknowledgements............................................................................................................ iv
Table of Contents……………………………………………………………………………………………….. v
List of Tables ..................................................................................................................... ix
List of Figures ..................................................................................................................... x
List of Appendices ............................................................................................................. xi
Chapter 1: Introduction ....................................................................................................... 1
1.1 ADHD Symptomatology .......................................................................................... 1
1.2 ADHD Treatments .................................................................................................... 5
1.3 Parent-Child Conflict in Families with ADHD ........................................................ 8
1.4 Treatments for Parent-Child Conflict ..................................................................... 11
1.5 Parenting Stress....................................................................................................... 13
1.6 Treatments for Parenting Stress .............................................................................. 16
1.7 Mindfulness ............................................................................................................ 17
1.7.1 Acceptance-based approaches…………………………………………………………..17
1.7.2 Mindfulness and mindfulness-based interventions………………………………..18
1.7.3 Mindfulness meditation……………………………………………………………………20
1.7.4 Mindful parenting and mindfulness for parent-child interactions……………22
1.7.5 Mindfulness as a treatment for ADHD symptoms……………………………….25
1.7.5.1 Nonclinical samples……………………………………………………………..25
1.7.5.2 ADHD samples……………………………………………………………………27
1.8 Summary ................................................................................................................. 27

vi
1.9 Background and Rationale of Present Investigation............................................... 28
1.10 Objectives ............................................................................................................. 31
Chapter 2: Method ............................................................................................................ 33
2.1 Participants.............................................................................................................. 33
2.1.1 Recruitment …………………………………………………………………..……………….33
2.1.2 Inclusion/exclusion criteria…………………………………………………………… 33
2.1.3 Demographic and diagnostic information………………………………............... 35
2.2 MYmind Program Description ............................................................................... 37
2.2.1 MYmind: Mindfulness training for Youth with ADHD and their parents..37
2.2.2 General overview of program……………………………………………......................38
2.2.3 Adolescent sessions ………………………………………………………………………..40
2.2.4 Parent sessions ………………………………………………………………………………42
2.3 Procedure ................................................................................................................ 46
2.4 Measures Used to Describe and Define the Sample ............................................... 47
2.4.1 Demographics questionnaire…………………………………………………………….. 47
2.4.2 Conners’ Parent Rating Scale-3rd edition…………………………………………….. 48
2.4.3 Wechsler Abbreviated Scale of Intelligence (WASI)……………………………. 48
2.5 Outcome Measures.................................................................................................. 49
2.5.1 Daily Symptoms Questionnaire (DSQ)……………………………………………… 49
2.5.2 Consumer-Satisfaction Questionnaire (CSQ)……………………………………… 50
2.6 Research Design...................................................................................................... 51
2.7 Data Analysis .......................................................................................................... 53
2.7.1 Time-series analysis………………………………………………………………………… 53

vii
2.7.2 Generalized estimating equations (GEE)……………………………………………. 53
Chapter 3: Results ............................................................................................................. 55
3.1 Participant Stress..................................................................................................... 56
3.1.1 Parent self-report of stress………………………………………………………………... 56
3.1.2 Adolescent self-report of stress ………………………………………………………… 61
3.2 Participant Distress due to Family Conflict ............................................................ 64
3.2.1 Parent self-report of distress due to conflict with adolescent………………… 64
3.2.2 Adolescent self-report of distress due to conflict with parent………………. 68
3.3 Adolescent Inattention ............................................................................................ 71
3.3.1 Parent report of inattention in adolescents………………………………………….. 71
3.3.2 Adolescent self-report of inattention………………………………………………….. 76
3.4 Adolescent Hyperactivity....................................................................................... 79
3.4.1 Parent report of hyperactivity in adolescents………………………………………. 79
3.4.2 Adolescent self-report of hyperactivity…………………………………................ 84
3.5 Adolescent Impulsivity. .......................................................................................... 87
3.5.1 Parent report of impulsivity in adolescents…………………………………………. 87
3.5.2 Adolescent self-report of impulsivity………………………………………………… 91
3.6 Meditation Practice ................................................................................................. 94
3.6.1 Parent self-report of meditation practice…………………………………………….. 94
3.6.2 Adolescent self-report of meditation practice……………………………………… 98
3.7 Relationship Between Stress and Meditation Practice.......................................... 101
3.8 Consumer Satisfaction .......................................................................................... 103
Chapter 4: Discussion ..................................................................................................... 106

viii
4.1 Reported Stress Outcomes .................................................................................... 108
4.1.1 Parent stress………………………………………………………………………………….. 108
4.1.2 Adolescent stress……………………………………………………………………………. 109
4.2 Reported Distress due to Family Conflict Outcomes ........................................... 110
4.2.1 Parent distress due to parent-adolescent conflict………………………………… 111
4.2.2 Adolescent distress due to parent-adolescent conflict ………………………….113
4.3 Reported ADHD Symptomatology Outcomes in Adolescents............................. 114
4.3.1 Parent report of ADHD symptoms in adolescents………………………………. 114
4.3.2 Adolescent self-report of ADHD symptoms………………………………………. 116
4.4 Reported Meditation Outcomes ............................................................................ 117
4.4.1 Parent meditation practice……………………………………………………………….. 117
4.4.2 Adolescent meditation practice ……………………………………………………….. 118
4.4.3 Relationship between meditation and stress………………………………………. 119
4.5 Limitations and Research Implications................................................................. 119
4.6 Clinical Implications and Conclusions ................................................................. 124
References....................................................................................................................... 128
Appendices……………………………………………………………………………………………………...152

ix
List of Tables
Table 1. Demographic and Diagnostic Characteristics of Participantsand Non‐completers……...…………………………………..……………………………….... 36 Table 2. Brief Overview of the Content of Adolescent and Parent Sessions……….. 44 Table 3. GEE Analyses: Examining the Relationship Between Stress and Meditation Practice While Controlling for Adolescent/Parent Status and Phase…………………………………………………………………………………………... 103 Table 4. Adolescent and Parent Satisfaction with the MYmind Program………….. 105
Table G1. GEE Analyses: Examining the Relationship Between Stress and Meditation Practice While Controlling for Adolescent/Parent Status and Phase……….……….……….……….……….……….……….……….………….Appendix G Table G2. GEE Analyses: Examining the Relationship Between Stress and Meditation Practice, Main Effects Only……….……….………....……Appendix G

x
List of Figures
Figure 1. Multiple Baseline Design for Groups A, B, C and D across Baseline, Treatment and Follow-up………………………..........................................................52 Figure 2. Parent Report of Stress Levels Across Baseline, Treatment and 6-month Follow-up…………………...............................................................................................58 Figure 3. Adolescent Report of Stress Levels Across Baseline, Treatment and 6- month Follow-up…………………….............................................................................62 Figure 4. Parent Report of Distress due to Conflict with their Adolescents across Baseline, Treatment and 6-month Follow-up………………………………..........65 Figure 5. Adolescent Report of Distress due to Conflict with their Parents across Baseline, Treatment and 6-month Follow-up……………………………………...69 Figure 6. Parent Report of Adolescent’s Inattention across Baseline, Treatment and 6-month Follow-up……………………........................................................................73 Figure 7. Adolescent Report of Inattention across Baseline, Treatment and 6-month Follow-up…………………...............................................................................................77 Figure 8. Parent Report of Adolescent’s Hyperactivity across Baseline, Treatment and 6-month Follow-up………………….....................................................................81 Figure 9. Adolescent Report of Hyperactivity across Baseline, Treatment and 6- month Follow-up…………………………………....................................................…...85 Figure 10. Parent Report of Adolescent’s Impulsivity across Baseline, Treatment and 6-month Follow-up………………………………………………………………………....88 Figure 11. Adolescent Report of Impulsivity across Baseline, Treatment and 6-month Follow-up…………………...............................................................................................92 Figure 12. Parent Report of Meditation Practice across Baseline, Treatment and 6- month Follow-up………………….................................................................................95 Figure 13. Adolescent Report of Meditation Practice across Baseline, Treatment and 6-month Follow-up………………….............................................................................99

xi
List of Appendices
Appendix A. Information Letter…………………............................................................................152
Appendix B. Consent Form………………….....................................................................................154
Appendix C. Demographics Questionnaire…………………........................................................155
Appendix D. Daily Symptom Questionnaire (Parent and Adolescent versions)……….. 159
Appendix E. Instructions for Completing the Parent and Adolescent Questionnaires. 161
Appendix F. Consumer Satisfaction Questionnaire (Parent and Adolescent versions) 167
Appendix G. Supplementary GEE Analyses…………………......................................................173
1
Chapter 1: Introduction
The present study is an investigation of a mindfulness-based treatment for
adolescents with ADHD and their parents. This intervention was designed to target the
conflict and high stress levels commonly found in these families, as well as the ADHD
symptoms of the adolescents. In this chapter, I will provide a context for the current
difficulties faced by families with an adolescent with ADHD and consider the relevance
of mindfulness for treating these difficulties. First, the symptoms, underlying
mechanisms, and interventions currently available for ADHD will be reviewed. This will
be followed by a discussion of the high rates of conflict in families of adolescents with
ADHD and a consideration of the high stress levels associated with parenting these youth.
Subsequently, I will review empirically supported treatments used to target family
conflict and stress, and consider the potential for mindfulness as an alternative to the
currently available interventions. Empirical studies supporting mindfulness as a treatment
for conflict, stress and ADHD will be presented as a rationale for the present
investigation.
1.1 ADHD Symptomatology
ADHD is a neurobiologically-based disorder characterized by symptoms of
inattention, impulsivity and hyperactivity, which cause impairment in multiple settings
and are atypical for the person’s level of development. Estimates indicate that ADHD
affects 5–10% of school-aged children (Polanczyk & Jensen, 2008; Polanczyk, de Lima,
Horta, Biederman, & Rohde, 2007), and more than 5% of adolescents (Polanczyk et al.,
2007). Compared to other youth, those with ADHD have difficulty with arousal,
2
motivation, planning and pursuing goal-directed behaviours, and adapting their behaviour
in response to the changing demands of different situations (Mercugliano, Power, &
Blum, 1999; Nigg & Casey, 2005).
Various potential underlying mechanisms have been proposed to explain the
behavioural symptoms and functional difficulties involved in ADHD. ADHD has been
associated with neurological deficits and structural and functional brain alterations,
resulting in impaired executive functions, including working memory, attention
regulation and inhibition (Bush, Valera, & Seidman, 2005; Seidman, 2006; Desman,
Petermann, & Hampel, 2008; Ma et al., 2012; Wåhlstedt, Thorell, & Bohlin, 2008). In a
meta-analytic review of 83 studies examining executive functioning in samples with
ADHD, Willcutt, Doyle, Nigg, Faraone, and Pennington (2005) concluded that
compromised executive functioning should be considered a leading cause of the
impairments associated with ADHD.
Barkley’s (1997) model suggests that the primary deficit in ADHD is the specific
executive function of behavioural inhibition. The inability to inhibit responses is
associated with increased emotional reactivity, trouble dealing with frustration/anger, and
increased difficulty self-regulating one’s emotions (Friedman et al., 2003; Nigg, 2001).
Multiple studies have demonstrated that the brain regions producing the inhibition
function are underactive in ADHD participants, causing them to struggle during tasks that
require an inhibitory response and leading to core ADHD symptoms of inattention and/or
impulsiveness (Mulligan et al., 2011; Smith et al. 2006; Tamm, Menon, Ringel, & Reiss,
2004). Furthermore, children with ADHD appear to have abnormal parasympathetic
mechanisms involved in emotion regulation, resulting in difficulty with regulating affect

3
and suppressing emotional expression (Musser et al., 2011).
Walcott and Landau (2004) investigated cognitive disinhibition and emotion
regulation in a sample of 49 boys aged 6-11 with and without ADHD. Cognitive
disinhibition was measured via Stop Signal Reaction Time (i.e., a measure of how much
time is needed to successfully inhibit a motor response). Emotion regulation was
examined with a puzzle task in which two pieces were missing and children were
required to respond faster than a confederate. In addition, half of the children were asked
to mask their frustration from the confederate competitor. Results showed that boys with
ADHD exhibited less effective emotion regulation than boys without ADHD,
demonstrated by more negative responses and immobilized behaviour. They also had
more difficulty regulating their emotional expression when instructed.
In samples of preschoolers, both Schoemaker, Bunte, Wiebe, Espy, Deković, and
Matthys (2012), and Thorell and Wahlstedt (2006) found that children with ADHD
showed significant inhibition and working memory deficits, even after controlling for IQ
(i.e., in the Schoemaker study). Both research teams also demonstrated that although
ADHD is commonly comorbid with Oppositional Defiant Disorder (ODD), poor
executive functioning in preschoolers appeared to be mainly associated with symptoms of
ADHD, whereas the relation to symptoms of ODD can be attributed to the great overlap
between the disorders. These executive function impairments seen in preschoolers and
children with ADHD appear to persist into adolescence. Martel, Nikolas, and Nigg
(2011) compared adolescents diagnosed with ADHD to a control group across a
multistage diagnostic assessment. Results revealed that after controlling for age, IQ,
comorbid disorders and gender, adolescents with ADHD performed significantly worse

4
than the controls on executive function measures. Similar to prior research (Barkley,
2003), Martel et al. concluded that children and adolescents exhibit a similar pattern of
executive functioning deficits suggesting similar clinical impairments across
development.
As a result of the aforementioned executive functioning and regulation difficulties,
adolescents with ADHD often encounter challenges in many life situations. For example,
in comparison to adolescents without ADHD, those with ADHD are at increased risk for
significant academic impairment, including lower grade point averages (GPA), lower
levels of class placement, school failure and dropout (Ek, Westerlund, Holmberg, &
Fernell, 2011; Rogers, Hwang, Toplak, Weiss & Tannock, 2011). Furthermore,
adolescents with ADHD complete significantly less class assignments and are
significantly less likely to achieve their potential (Ek et al., 2011; Kent et al., 2011).
These youth also struggle in relationships as adolescents with ADHD have significantly
fewer close friendships and greater peer rejection compared to non-ADHD peers
(Bagwell, Molina, Pelham, & Hoza, 2001). Adolescents with ADHD are also at an
increased risk to become involved in deviant peer groups, and because they are more
vulnerable to negative social influences of that group, are more likely to use illegal
substances (Marshal, Molina, & Pelham, 2003). In addition to substance use, adolescents
with ADHD are also more likely to engage in reckless driving (Thompson, Molino,
Pelham & Gnangy, 2007), risky sexual behaviour (Flory et al., 2006) and criminal
activities (Fletcher & Wolfe, 2009).
As demonstrated by the above research, youth with ADHD are unable to
modulate their emotions and control their behaviour according to the requirements of the

5
situation, whether these are demands placed on them by parents at home, teachers at
school or peers within social contexts (Barkley, 1990). Many of these adolescents
experience a progressive decline in their self-concept and academic performance, despite
normal intelligence (Dupaul et al., 2004; Frazier, Youngstrom, Glutting, & Watkins,
2007; Hinshaw, Owens, Sami, & Fargeon, 2006; Kawabata, Tseng, & Gau, 2012;
Mannuuzza & Klein, 2000). Due to impaired ability to interpret and control their
emotions and behaviours, youth with ADHD often manage stressful situations with
avoidance and aggression (Hampel, Manhal, Roos, & Desman, 2008). Consequently, they
may begin to believe that academic, social, and familial problems are beyond their
control (Erk, 2000), resulting in additional emotional and behavioural difficulties, such as
social or academic withdrawal, anger, and low self-esteem.
1.2 ADHD Treatments
Based on the results of many randomized clinical trials, the most effective form of
treatment for ADHD is currently medication (Biederman & Farone, 2005; Connor, 2005;
Hechtman & Greenfield, 2003). However, multiple negative side-effects of
pharmacological intervention have been reported, including reduced growth, delayed
sleep onset, reduced appetite, abdominal pain, weight loss, tics, jitteriness, and headaches
(Lerner & Wigal, 2007; MTA Cooperative Group, 2004a; Schachter, Pham, King,
Langford, & Moher, 2001; Wolraich, McGuinn, & Doffing, 2007). Given these potential
side effects, many parents prefer their children to participate in psychosocial treatment
approaches, such as group therapy, social skills training, behaviour management, parent
education, and school-based interventions (Farmer, Compton, Burns, & Robertson, 2002;

6
Pelham, Wheeler, & Chronis, 1998).
Notwithstanding this preference, psychosocial interventions have not yet been
demonstrated to produce effects comparable to medication. For example, when a
methylphenidate (MPH) plus multimodal psychosocial treatment, including parent
training, social skills training and academic remediation was compared to a MPH alone
group, assessments from multiple sources yielded no evidence of additional efficacy for
the combined intervention over the MPH alone (Abikoff et al., 2004). Moreover, all
participants in the multimodal group deteriorated when medication was replaced with a
placebo. Another multi-site study conducted by the MTA Cooperative Group (2004a)
found similar results; the multimodal combination of MPH and behaviour therapy was
not significantly more effective than medication alone. Furthermore, MPH alone and
MPH combined with behaviour therapy were superior to behaviour therapy alone or
community care alone (treatment as usual) during an observational follow-up period of
24 months (MTA Group, 2004b). However, a subsequent follow-up analysis, extending
over 36 months, revealed an increased incidence of symptoms in the combined treatment
group (Swanson et al., 2008).
Although the MTA Cooperative Group concluded that treatments involving
medication were more effective than the conditions that did not, there are further
considerations. For example, there were some large differences in the medication doses
across treatment groups. Specifically, at the 14-month follow-up, the average daily dose
for participants in the combined group was 31.2 mg while the average daily dose for the
MPH alone group was 37.7 mg (MTA Cooperative Group, 1999a). Another concern in
comparing the behavioural treatment and combined conditions with MPH alone is that

7
intensive behavioural treatments were faded by study termination, whereas medication
continued (Pelham, 1999). Because of this disproportionate treatment activity, it is
possible that the comparison of the behaviour therapy and combined conditions to the
MPH alone at the 14-month follow-up point may have been biased in favour of the MPH
alone group. Therefore, the extent to which medication alone is superior to combined or
psychosocial treatments alone has not been categorically determined.
School-based studies have also investigated the single, comparative and combined
effects of pharmacological and behavioural treatments with children with ADHD
(Pelham et al., 2005). For example, Fabiano et al. (2007) examined different levels of
behaviour modification alone (no BMOD, low or high intensity BMOD), different doses
of MPH alone (placebo, 0.15, 0.30 and 0.60 mg) and the treatments combined in an
analogue classroom with 48 ADHD children. Results revealed that a low level of BMOD
in combination with medication was typically as effective in improving classroom
behaviour, productivity and teacher rated ADHD symptoms as a high level of BMOD
with medication. The 0.15 mg dose of MPH was just as effective as the 0.30 mg dose
when combined with a low level of BMOD and these were both more effective than
either of these doses alone, however, a 0.60 mg dose of MPH alone was just as effective
as the combined treatments. Moreover, these treatments took place in an analogue
classroom as part of a summer treatment program; this setting did not approximate the
workload or enrolment numbers of a typical classroom. Also, given the lack of follow-up
data in this study, there was no consideration of maintenance of effects.
Given the negative side-effects of ADHD medication, a lack of evidence for long-
term effects (Goldman, Genel, Bezman, & Slanetz, 1998; Vitiello, 2001), and decreased

8
compliance to medication regimens in adolescence (Atzori, Usala, Carucci, Danjou, &
Zuddas, 2009; Jensen et al., 2007), an alternative approach to treating ADHD is needed.
Moreover, a treatment with the potential to alleviate the difficulties associated with
ADHD (e.g., inattention, behaviour inhibition, emotion regulation, etc.) would be
particularly beneficial for adolescents with this disorder, considering the level of
challenge they experience in a variety of contexts, in a range of important skills areas,
and in their interactions with important others (e.g., parents, teachers, peers).
1.3 Parent-Child Conflict in Families with ADHD
Many significant life changes occur during the developmental transition that takes
place when children enter adolescence. The initiation of secondary school coincides with
numerous shifts in physical, social and cognitive functioning (Steinberg, 2001).
Managing the personal, academic and social pressures that parallel these life changes is
difficult, not just for adolescents, but also for their parents. For example, the attempts of
adolescents to explore their identity and gain autonomy may clash with their parents’
ideas and willingness to allow independence (Jackson, Bijstra, Oostra, & Bosma, 1998;
Spring, Rosen, & Matheson, 2002). This discord may lead to emotional arousal and
conflict between parents and adolescents, which can trigger negative patterns of
interaction (Granic, Dishion, & Hollenstein, 2003).
Although some parent-adolescent conflict is developmentally appropriate, high
levels of conflict are associated with poorer psychological adjustment in adolescents and
parents (Shek, 1998; Dekovic, 1999). For example, a longitudinal study (Shek, 1998)
found that parent-adolescent conflict was associated with more psychiatric symptoms,

9
lower self-esteem, and a lack of sense of purpose in adolescents one year later.
According to Robin (1981), parent-adolescent conflict is frequently a consequence of
deficits in interpersonal and problem-solving skills in both parties, as well as parents’ and
adolescents’ distorted or irrational beliefs about their own or one another’s behaviour.
This combination of deficits may result in discordant parent-adolescent interactional
patterns, especially when adolescents have difficulties with inhibitory processing and
emotional regulation, as is found in youth with ADHD (Wolraich et. al., 2005).
Although adolescence is typically a time of increased parent-child conflict (Laursen,
Coy, & Collins, 1998), families with an adolescent with ADHD demonstrate especially
high levels of discord (Babinski et al., 2011; Barkley, Anastopoulos, Guevremont, &
Fletcher, 1992; Lange et al., 2005; Pressman et al. 2006). In two independent studies
(Fletcher, Fischel, Barkley, & Smallish, 1996; Wymbs & Pelham, 2010), adolescents
with ADHD and behaviour problems, and their parents, exhibited higher levels of
conflict-related behaviour, such as defensiveness, insults, negative affect and commands
during discussions than adolescents and parents in a control group. These families report
arguing about more issues, feeling more anger, and using more negative communication
than families without an adolescent with ADHD (Edwards, Barkley, Laneri, Fletcher, &
Metevia, 2001).
Schroeder and Kelley (2009) investigated the relationship between ADHD
symptoms (executive functioning difficulties) and family conflict among 134 parents of
children with and without ADHD. Parents of children with ADHD reported higher levels
of family conflict and less organization in the home. Relational difficulties may be further
exacerbated by symptoms of ODD or Conduct Disorder that are found in up to 75% of
10
adolescents with ADHD (Wolraich et. al., 2005). Biederman, Mick, Faraone, and
Burback (2001) conducted a four-year longitudinal study of 140 children with ADHD,
who were divided into those with persistent or remitting/desistent Conduct Disorder.
Findings indicated that children with persisting conduct problems had greater levels of
family conflict and less family cohesion at baseline. Moreover, child-reported problems
with parents at baseline significantly predicted continual conduct problems in
adolescence.
The aversive interactions between parents and their adolescents with ADHD appear
to be reciprocal in nature (Burke, Pardini, & Loeber, 2008; Hinshaw, 2000). According to
Mash and Johnston (1990), “both parents and children are victims as well as architects of
conflicted relationships” (p. 314). It may be more difficult to parent youth with ADHD
(especially when they demonstrate increased oppositional behaviours), but studies show
that parenting attitudes and practices, whether hostile or warm, impact the behaviours of
their children with ADHD (Anderson, Hinshaw & Simmel, 1994). For example, Hinshaw
et al. (1997) found that the strongest predictor of prosocial skills among boys with
ADHD was the degree to which their mothers exhibited an authoritative (warm, limit
setting, encouraging autonomy) parenting style. However, parents of children with
ADHD have been shown to use more negative and fewer positive parenting practices
than parents of children without ADHD (Gerdes, Hoza, & Pelham, 2003; Johnston, 1996).
When interacting with their children, parents of children with ADHD are less
responsive and more over-reactive (Barkley, Fischer, Edelbrock, & Smallish, 1991;
DuPaul, McGoey, Eckert, & Vanbrakle, 2001; Ellis & Niggs, 2009). They often avoid
dealing with difficult situations altogether (Goldstein et al., 2007) and show less parental

11
support than parents of typical children (Khamis, 2006). In families that include children
with ADHD and externalizing problems, there are higher levels of parental conflict,
negative parenting practices and poorer social support (Kaiser, McBurnett, & Pheiffer,
2011; McLaughlin & Harrison, 2006). Many parents of children with ADHD have
ADHD symptoms themselves, and consequently may lack the skills necessary to resolve
conflict (Mokrova, OBrien, Calkins, & Keane, 2010).
1.4 Treatments for Parent-Child Conflict
The increased recognition of the parent-child conflict that is associated with ADHD
and the added obstacles to resolution, such as child behaviour problems, has led to the
development of programs targeting these issues in families with ADHD (Gerdes, Haack,
& Schneider, 2012; Mikami, Jack, Emeh, & Stephens, 2010; van den Hoofdakker et al.,
2007; for a review see Zwi, Jones, Thorgaard, York, & Dennis, 2011). Although a wide
range of treatments have been developed and evaluated for children with ADHD and
their parents, only a few such studies have been conducted with adolescents with ADHD
(Smith, Waschbusch, Willoughby, & Evans, 2000). In fact, a review of the literature
determined that more review papers than empirical papers have been published on the
topic of treatments for adolescents with ADHD (Smith et al., 2000). The scarcity of
research may be due to the lack of engagement and adherence in these youths, as well as
a belief of stigma associated with ADHD and it’s treatment (Gulliver, Griffiths, &
Christensen, 2010). For example, in a mixed method study assessing perceptions of
ADHD interventions, Bussing et al. (2012) found that adolescents were significantly less
willing than adult participants to consider either medication or psychosocial treatments

12
for their ADHD and related challenges.
Unfortunately, the few studies that have investigated treatment programs for
adolescents with ADHD and their parents have not demonstrated substantial effects
across all areas of concern. For example, Barkley et al. (1992) compared three family
therapy programs for their effectiveness in resolving conflict among families with ADHD
adolescents. The first program was Problem-Solving and Communication Training
(PS/CT), a cognitive-behavioural based multi-step problem-solving and communication
building approach. The second was Family Structural Therapy (FST), which involves
helping families to identify and alter maladaptive family systems or interaction processes.
The third program comprised parent training in behavioural techniques (BMT), such as
the use of positive parental attention, point systems or token reinforcement, brief periods
of grounding for unacceptable behaviour, and instruction to parents on how to anticipate
impending problem situations. These three therapies were also compared to a wait-list
control condition.
Families in the three treatment groups demonstrated reductions in communication
difficulties, conflict, and internalizing/externalizing symptoms. However, despite
statistically significant improvements at the group level, only 5% to 30% of these
families demonstrated significant within-family change or improved on an index of
clinical significance (i.e., movement to a subclinical range of impaired functioning).
Barkley et al. (1992) concluded that, "Such sobering statistics indicate that most ADHD
adolescents (70% to 95%) . . . show no clinically significant change in their number of
family conflicts or the anger frequency/intensity of these conflicts, with 80% to 95%
remaining deviant after treatment" (p. 460).
13
Barkley et al. (2001) conducted a follow-up study comparing the effects of parental
BMT to PS/CT on families with comorbid ADHD/ODD. The authors sought to improve
previous results by doubling the number of treatment sessions from 9 to 18 sessions.
Findings resembled those reported in the authors’ initial study, showing statistical
significance at the group level, but only minimal change at the individual level of
analysis. Moreover, a greater drop-out rate was found for the PS/CT group, possibly due
to the higher levels of adolescent involvement required in PS/CT.
Although many behavioural and parent training programs are effective for children
with ADHD (for a review, see Zwi et al., 2011), ADHD in adolescence is associated with
greater impairment across multiple domains of functioning, including parent-adolescent
interactions (Wolraich et al., 2005). Based on the aforementioned studies and a lack of
evidence-based treatments for families of adolescents with ADHD, there appear to be
significant limitations to current treatment approaches for these adolescents and their
parents; alternative intervention components or treatment approaches are required.
1.5 Parenting Stress
In addition to parenting styles/practices, parenting stress is also a contributor and
byproduct of parent-adolescent conflicts (Theule et al., 2013). Parenting stress is the
result of parents perceiving their children’s problem behaviour as exceeding the resources
they have available to manage it (McCleary, 2002). Consequently, if parents judge their
child’s ADHD-related difficulties as beyond their control, they will likely respond with
frustration and distress (Bromley Little, 1998).
Parenting stress is significantly higher in parents of children (Reader, Stewart, &

14
Johnson, 2009), and adolescents with ADHD (Biondic, 2011) and stress ratings are
related to higher levels of conflict in the home (Theule et al., 2013). A high degree of
child inattention, hyperactivity and impulsivity places numerous demands on parents, and
increases the probability that they will manage their child’s behaviours inconsistently,
with over-reactive discipline, or avoidance of interactions with their child. The combined
effects of the child’s ADHD and such parenting practices produce the essential conditions
for the development of child oppositional behaviour problems and a difficult family
environment (Johnston & Mash, 2001; Seipp & Johnston, 2005).
Harrison and Sofronoff (2002) investigated the effect of child behaviours on
parental levels of stress by interviewing a sample of 105 mothers of children with ADHD.
They found that the strongest individual predictors of psychological distress were child
behavioural disturbance and lack of perceived parental control over child behaviours.
Parents of children with externalizing disorders, such as ADHD, view themselves as
having less parenting knowledge, less parental competence, and less social support
(Morgan, Robinson and Aldridge, 2002). ADHD is further associated with an
environment of parental discord, perceived parenting incompetence, and negative parent-
child relationships and childrearing beliefs (Johnston & Mash, 2001).
Johnston and Jassey (2007) provide a review of multiple longitudinal studies that
support a transactional model of parent-child interactions, whereby children’s ADHD
symptoms present parents with numerous challenges to parenting, which in turn
contribute to the development of child oppositional behaviour problems and parenting
stress. This reciprocal pattern between parenting stress, parenting practices and the
behaviour problems of ADHD children is prevalent across cultures. For instance, Anjum
15
and Malik (2010) asked 60 Pakistani mothers of children with ADHD to complete
questionnaires regarding their own and their child’s current functioning. Results indicated
a strong significant positive correlation between child disruptive behaviours, maternal
stress and parent disciplinary practices. Maternal stress and child behavioural difficulties
emerged as strong predictors of the use of harsh and more physical discipline. Likewise, a
stepwise regression analysis showed that mother's stress, harsh parenting and over-
involvement/over-protection were strong predictors of child behaviour problems. Such
research highlights the role parenting plays in the development and maintenance of child
disruptive behaviours and the impact child behaviour problems have on parents’ stress
levels and disciplinary practices.
Although an abundance of research suggests that parenting stress in parents of
children with ADHD stems primarily from the child’s ADHD-related behaviour problems,
parental factors also play a significant role. In a study of 150 mothers of children with
ADHD, McLaughlin and Harrison (2006) found that a lower sense of parental
competence was directly associated with less effective parenting practices and high stress,
beyond the effects of child age, having an only child, number or severity of ADHD
behaviours in their child, and parental social isolation. Theule, Wiener, Rogers, and
Marton (2011) investigated the specific parent and contextual factors underlying
parenting stress among parents of children with ADHD, after controlling for the effects of
child factors (e.g., ADHD, gender, age). Findings revealed that parent ADHD
symptomatology was the strongest predictor of parental stress, and social support was
inversely related. Biondic (2011) is the only study to date that has examined parenting
stress among parents of adolescents with ADHD. Results suggest that in addition to the

16
adolescents’ externalizing behaviour, maternal inattention difficulties mediated the
relationship between adolescent ADHD and parenting stress. These results are not
surprising considering the extensive evidence of elevated rates of ADHD in parents of
children with ADHD (Chronis et al., 2003).
1.6 Treatments for Parenting Stress
Although a range of psychosocial, psychoeducational and behaviour management
programs are considered evidence-based treatments for ADHD due to their effects on
ADHD symptoms and problem behaviour, few studies have focused on the impact of
these parent training approaches on parent outcomes (Fabiano et al., 2009; Hoza, Kaiser,
& Hurt, 2008; Pelham & Fabiano, 2008). Pisterman et al. (1992) investigated a program
adapted from a parent-training behavioural intervention with 91 parents of preschoolers
with ADHD. The 12-week parent program predominantly focused on providing parents
with psychoeducation on ADHD and behavioural strategies (e.g., reinforcement, time-out,
shaping) to improve child compliance and on-task behaviour. Compared to a waitlist
control group, parents who participated in the program reported improvements in the
Parent Domain and Sense of Competence subscale of the Parenting Stress Index (PSI)
following treatment and three months later. However, no significant reductions were
found in the Child Domain of the PSI. These results suggest that the parent training
helped parents feel more competent and become more effective with managing the stress
associated with being a parent, but not with the stress resulting from problems with their
child. Anastopoulos, Shelton, Du Paul, and Guevremont (1993)’s research extended
Pisterman et al.’s study to parents of school-age children with ADHD. Using Barkley’s

17
(1990) parent training model, they found significant improvements in parenting stress,
self-esteem and parental perceptions of their children’s ADHD symptoms compared to
wait-list controls.
More recently, Gerdes, Haack, and Schneider (2012) evaluated a parent-training
program with 20 parents of children with ADHD. The researchers found significant
reductions of parenting stress for mothers across most domains (dysfunctional parent–
child interactions, difficult child, and total parenting stress); however, no significant
results emerged when investigating paternal parenting stress. Similarly, a nine-week
parent stress management program with 63 mothers and fathers of children with ADHD
found significant improvements in parent-domain parenting stress and parenting style for
mothers, but not for fathers (Treacy, Tripp, & Baird, 2005). Furthermore, the perceived
locus of control, child-domain parenting stress, parent-child relationship quality, mood,
and perception of child externalizing behaviour of parents did not improve from pre- to
post-treatment.
Results from past research provide mixed results for the efficacy of parent-training
programs for treating the high stress levels of parents of children with ADHD. Moreover,
the effects of parent-training on parenting stress in parents of adolescents with ADHD
have not yet been examined. Given the added stressors of parenting an adolescent,
especially with ADHD, treatments targeting stress in this population are required.
1.7 Mindfulness
1.7.1. Acceptance-based approaches. Given the apparent limitations of PSM
programs, PS/CT and BMT, Greco and Eifert (2004) recommended using acceptance

18
strategies in the context of family therapy. As an alternative to the change- and control-
oriented strategies promoted in BMT and PS/CT, acceptance-based approaches
emphasize an empathic understanding of the experiences of others and a nonjudgmental
acceptance when addressing these experiences. Hayes (1994) states that acceptance
entails “experiencing events fully and without defense, as they are” (p. 30), and indicates
that scientist-practitioners may have overstressed the significance of changing unpleasant
symptoms, without recognizing the value of acceptance. In acceptance-based methods
there is little focus on controlling or altering the content of thoughts, but instead on
shifting how people relate to their thoughts (Segal, Teasdale, & Williams, 2004). While
decreasing the use of strategies aimed at avoiding negative thoughts, emotions, and body
sensations, clients are encouraged to be “experientially open” to whatever is happening in
the present moment (Hayes, Strosahl, & Wilson, 1999). Acceptance-based approaches
include many interventions rooted in the practice of mindfulness, such as Mindfulness-
Based Cognitive Therapy (MBCT), Mindfulness-Based Stress Reduction (MBSR) and
Acceptance and Commitment Therapy (ACT).
1.7.2 Mindfulness and mindfulness-based interventions. Mindfulness is the non-
evaluative, present-centered awareness that results from the deliberate focusing and
refocusing of attention on sensations, thoughts and feelings as they arise moment-by-
moment (Williams, Teasdale, Segal, & Kabat-Zinn, 2007). Mindfulness stems from
Eastern Buddhist traditions and philosophy, and, as part of this tradition, is practiced to
alleviate suffering and to gain insight into the nature of reality (Silananda, 1990). The
Buddhist practice of mindfulness is rooted in compassion, detachment and understanding
(Hanh, 1975). Buddhists have practiced mindfulness for over 2,500 years to free
19
themselves from attachments and cognitions and lead them to enlightenment and personal
awakening (Silananda, 1990).
Drawn from an integration of Buddhist teachings with current Western psychology
and knowledge, mindfulness-based interventions are used to enhance psychological and
physical well-being through the processes of decentering, acceptance, exposure, and self-
regulation (Baer, 2003; Bishop et. al., 2004). Mindfulness comprises five main facets: (a)
detached observation of and attention to one’s internal experiences; (b) a nonjudgmental
attitude; (c) the ability to participate in activities with complete awareness; (d)
recognition, description and labeling of one’s experiences; and (e) nonreactivity to
internal experiences (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006). Objectively
attending to inner experiences allows one to monitor thoughts and feelings without
judgment or self-criticism. Adopting an attitude of acceptance and openness to
experience allows previously suppressed thoughts to enter the field of awareness. Greater
awareness, recognition and regulation of cognitive processes reduce the tendency to react
on ‘autopilot’ and fall into habitual patterns of responding to stressors (Baer, 2003).
A growing body of evidence supports the use of mindfulness as a treatment for a
variety of health and mental health conditions. In a meta-analytic review by Hofmann,
Sawyer, Witt, and Oh (2010), the authors reported that mindfulness-based programs are
moderately effective treatments for adults with anxiety and depression. In her empirical
review of mindfulness interventions, Baer (2003) noted the same moderate effect sizes
for pain and stress in adults. MBCT, MBSR and other mindfulness-based interventions
have been developed and/or adapted for the treatment of a variety of psychiatric disorders
and medical diseases. For example, mindfulness-based interventions have been

20
demonstrated effective for clients with eating disorders (Baer, Fischer, & Huss, 2006),
substance abuse (Bowen et al., 2006), chronic pain (Kabat Zinn, 1990), depression (Segal,
Williams, & Teasdale, 2002), anxiety (Evans et al., 2008), insomnia (Ong, Shapiro, &
Manber, 2008), attention-deficit hyperactivity disorder (Zylowska et al. 2008),
fibromyalgia (Grossman et al., 2007), HIV (Creswell, Myers, Cole & Irwin, 2009),
cancer (Witek-Janusek et al. 2008) and heart disease (Sullivan et al. 2009).
1.7.3 Mindfulness meditation. Mindfulness meditation involves the cultivation of
a nonjudgmental sustained awareness to an object of attention (e.g., an emotion, the
breath, a physical feeling, an image, or an external object) (Kabat-Zinn, 1990). In
describing meditation with the breath, Hanh (1975) states that when the mind is
overwhelmed, the breath is used as an anchor to bring the mind back to the present
moment. Meditating cultivates a mindfulness that allows an individual to observe and
accept the presence of every thought and feeling that is experienced (Hanh). Continuous
meditation practice fosters greater awareness of internal experiences and increased self-
regulation of attention, which leads to enhanced affect tolerance, emotional awareness,
reduced avoidance, and additional attentional resources when extended to everyday life
(Keune & Forintos, 2010). Given the value of practicing meditation, researchers have
asserted meditation as necessary for the development of mindfulness skills (Kabat-Zinn,
1990) and investigated its independent contribution to the effects demonstrated by
mindfulness-based interventions.
Most mindfulness-based interventions prescribe daily meditation practice at home
as an essential component of treatment. For example, in MBSR programs, participants
are given CDs with instructions to guide their formal meditations, and are recommended

21
to practice everyday for 45 min (Kabat-Zinn, 1990). Other manualized programs,
including MBCT and ACT, encourage regular at-home meditation for at least 15 - 40 min
each day (Hayes & Smith, 2005; Segal et al., 2002).
Although meditation home practice is strongly recommended in many mindfulness
programs, only a few studies have evaluated the relationship between home practice and
treatment outcomes. In a study of 90 cancer patients, Speca, Carlson, Goodey and Angen
(2000) investigated how home meditation practice further contributed to the changes seen
after a MBSR program. Findings showed that more home practice predicted reductions in
stress levels and mood disturbance. Using a sample of adults with a diverse range of
problems (e.g., illness-related stress, chronic pain, anxiety, etc.), Carmody and Baer
(2008) found that time spent meditating during a MBSR course was significantly related
to positive changes in mindfulness, and the reduction of many psychological and medical
symptoms, including well-being and stress. Moreover, results revealed that increases in
mindfulness mediated the relationship between formal meditation practice and improved
psychological functioning, suggesting that meditation practice may lead to increases in
mindfulness, which in turn leads to improvements in mental health outcomes and
perceived stress.
Similarly, a randomized clinical trial assessing MBSR for adolescent psychiatric
outpatients showed that frequency of sitting meditation practice and average duration of
each session correlated with significant reductions in psychological symptoms, including
depression and anxiety (Biegel, Brown, Shapiro, & Scubert, 2009). It should be noted
that a few studies investigating meditation practice found no relationship between
practice time and stress levels (Astin, 1997; Davidson et al, 2003). These findings may

22
not be as relevant to the current discussion, however, given that they were conducted with
nonclinical samples and baseline stress levels were not at clinical levels.
1.7.4 Mindful parenting and mindfulness for parent-child interactions. In
addition to a range of clinical disorders, the applications of mindfulness have also been
explored in the context of parenting. Coined mindful parenting (Kabat-Zinn & Kabat-
Zinn, 1997), this emerging field has attempted to bring a more accepting and empathic
approach to raising children (Dumas, 2005). Mindful parenting involves bringing
moment-to-moment awareness to the parent–child relationship (Duncan, Coatsworth, &
Greenberg, 2009). Goldstein (2012) described mindful parenting as the process of
recognizing how parents’ own upbringings affect how they parent their children, and
being present and attuned to their children’s inner worlds. Duncan et al. (2009)’s model
of mindful parenting suggests that parents who can remain aware and accepting of their
child’s needs through mindfulness practices can create a family context that allows for
more enduring satisfaction and enjoyment in the parent–child relationship.
Kabat-Zinn and Kabat-Zinn (1997) consider empathy, acceptance, and sovereignty
to be the foundations of mindful parenting. Because responding empathically and
nonjudgmentally to the behavioural and emotional needs of youth with disabilities
requires increased levels of attention, cognitive flexibility, and self regulation from
parents, these capacities may be important foci for intervention (Dumas, 2005). Through
mindful parenting programs, parents are helped to recognize their beliefs and
expectations about parenting and determine which types of parent-child interactions lead
to conflict in their relationship. They become more aware of how they can change these
interactions by changing their response to them, and select ways that foster and uphold a

23
positive connection with their children (Dumas, 2005; Goldstein, 2012).
Research suggests that nurturing mindfulness in the everyday context of parenting
could greatly enhance the effectiveness of parent training interventions (Dumas, 2005).
Numerous mindfulness programs for parents and families have emerged over the last two
decades, and findings are promising (for a review, see Cohen & Semple, 2010). Studies
indicate that mindfulness training for parents reduces parenting stress (Blackledge &
Hayes, 2006), enhances parenting practices (van der Oord, Bögels, & Peijnenburg, 2012)
and improves child compliance (Singh et. al., 2010).
To evaluate the added value of mindfulness training, Coatsworth, Duncan,
Greenberg and Nix (2010) adapted an evidence-based parenting program by integrating it
with mindfulness activities. Using a randomized trial design, three conditions were
included: the original parenting intervention, the mindfulness-adapted parenting
intervention and a delayed intervention control group. Compared to the original parenting
intervention, the mindful parenting program showed similar increases on measures of
child management practices, but greater improvements on measures of mindful parenting,
positive and negative affective child behaviour and the parent-youth relationship.
Mediation analyses revealed that the mindful parenting program enhanced mindful
parenting, which in turn led to changes in child management practices and parent–youth
relationships. These findings suggest that mindful parenting may contribute additive
effects to current empirically validated parenting programs. Similarly, Duncan et al.
(2009) amalgamated a seven-week adolescent drug prevention program with components
of mindful parenting. Reports from a parent focus group subsequent to treatment
completion suggested that mindful parenting enhanced awareness of how moods affect
24
their reactions towards their adolescents, and reduced reactivity in family situations.
Benn, Akiva, Arel, and Roeser (2012) conducted a randomized, wait-list
controlled clinical study to investigate the effectiveness of an intensive 5-week
mindfulness program for parents and educators of children with disabilities. Self-report
data from parents in the treatment group revealed significant positive changes in stress,
anxiety, mindfulness (e.g., greater awareness of internal and external experiences, less
judgmental), self-compassion, relational concern (i.e., empathic concern and forgiveness)
and personal growth at post-treatment and 2-month follow-up in comparison to the wait-
list control group. Similar to earlier described studies, Benn et al. (2012) found that
mindfulness-related effects at treatment completion mediated the caregivers’ changes in
stress and anxiety at follow-up.
Using small samples of parents and children with developmental disabilities, Singh
and colleagues (Singh et al., 2004; Singh et al. 2006; Singh et al., 2007) investigated how
an 8- or 12-week mindful parenting program affected parent and child variables.
Observational data in these multiple baseline across subjects design studies indicated that
the mindful parent training led to reduced children’s aggression, non-compliance, self-
injurious behaviour and improved positive mother-child interactions. Moreover, mothers
reported increased parent satisfaction with their parenting skills and interactions with
their children. The authors emphasized that reductions in child problem behaviours
involved covariant change as a result of improvements in mindful parenting; these
responses were not directly targeted in treatment.
In another multiple-baseline design study by Singh et al. (2010), two mothers of
children with ADHD participated in a 12-week mindfulness parent training and results
25
showed enhanced child compliance. Moreover, subsequent mindfulness training for their
children lead to even higher compliance levels and more positive interactions; these
improvements were maintained during a six month follow-up.
1.7.5 Mindfulness as a treatment for ADHD symptoms. Little research has been
conducted involving the specific application of mindfulness to the treatment of ADHD
symptoms (Smalley et al., 2009). However, the rationale for using mindfulness practices
to help manage ADHD-related problems is rooted in evidence demonstrating that through
mindfulness, individuals learn to control arousal levels with breathing and meditation
exercises, and inhibit automatic responses by gaining awareness of their emotional,
cognitive and physiological experiences (Zylowska et al., 2008). Moreover, given that
mindfulness involves development of greater self-regulation and awareness (Bishop et al.,
2004), it may have potential for improvement of poor behavioural inhibition that is at the
core of ADHD deficits (Barkley, 1997). That is, by learning to intentionally monitor
thought processes and affect through mindfulness intervention, a person may be able to
reduce problematic and habitual patterns of response (Williams et al., 2007), such as
impulsive behaviours. Continued self-awareness may allow an individual to identify such
automatic ADHD-related patterns before they arise, and consider alternative ways to
respond. The repetitive act of directing one’s attention to a single, neutral stimulus (e.g.,
breath) through meditation may also help the individual to disengage from particularly
heightened emotional states. Therefore, individuals practicing mindfulness may become
less impulsive and emotionally reactive, and learn to exercise better self-regulation and
manage their ADHD symptoms more effectively (Zylowska et al., 2008).
1.7.5.1 Nonclinical samples. Research involving nonclinical samples of adults has

26
demonstrated improvements in many of the symptoms with which individuals with
ADHD struggle. For example, mindfulness meditation has resulted in improvements in
attention-related behavioural responses (Jha et al., 2007; Semple, 2010), self-regulation
(Tang et al., 2007), positive affect (Jha, Stanley, Kiyonaga, Wong, & Gelfand, 2010) and
improved information-processing (Van Vugt, & Jha, 2011). In a recent study (Van den
Hurk et al., 2010), the authors found that adults with years of meditation experience
showed better ability to focus attention and enhanced inhibition of automatic responses
compared to non-meditators.
Mindfulness studies involving nonclinical samples of children have also revealed
potential benefits of mindfulness training for youth with ADHD. For example, in a
randomized control study of 64 children, Flook et al. (2010) investigated the efficacy of a
school-based mindfulness program using both parent and teacher reports. Results
indicated that only those children who began the study with poor executive function had
gains in behavioural regulation, meta-cognition, and overall global executive control.
Also using a school-based mindfulness intervention, Napoli, Krech and Holley (2005)
conducted a randomized controlled trial with 194 typically developing first, second and
third grade students. Results from three attention tasks and teacher reports showed
significant increases in attention and social skills, and decreases in test anxiety and
ADHD-related classroom behaviours following intervention.
Salzman and Goldin (2010) examined the impact of a joint parent-child
mindfulness program on 24 families. Compared to a waitlist control group, the families
who received treatment showed significantly greater attention skills (i.e., alertness,
switching, cognitive control) and reduced emotional reactivity in response to threatening

27
situations. Results indicated improved metacogntive functioning, specifically, self-
judgment and self-compassion in both parents and children. However, only parents
reported a significant decrease in anxiety and depression.
1.7.5.2 ADHD samples. In the last few years, mindfulness-based interventions have
been developed and evaluated to determine their efficacy with ADHD samples. For
example, Zylowska et al. (2008) conducted a pilot study of an eight-week mindfulness
program for adults and adolescents with ADHD, called Mindful Awareness Practices
(MAPs). Pre-post changes included significant improvements in self-reported ADHD
symptoms and performance on neurocognitive tasks assessing attention and cognitive
inhibition. Haydicky, Wiener, Badali, Milligan, and Ducharme (2012) evaluated a
mindfulness-based martial arts intervention for learning disabled adolescents with and
without ADHD. The authors found that, compared to a waitlist control group, youth with
co-occurring ADHD improved on parent-rated externalizing behaviour, oppositional
defiant problems, and conduct problems. Boys with elevated hyperactive/impulsive
symptoms improved on parent-rated social problems and monitoring skills.
1.8 Summary
Adolescents with ADHD experience a range of difficulties due to cognitive deficits
in executive functioning, including working memory, attention regulation and inhibition
(Bush, Valera, & Seidman, 2005). At present, the most common treatments for ADHD
include psychostimulant medication and psychosocial treatments (Abikoff et al., 2004).
Although medication is significantly more effective than psychosocial treatments (MTA
Group, 2004a), there is continued interest in non-pharmacological interventions due to

28
the negative side effects and poor long-term compliance associated with ADHD
medications (Atzori et al., 2009; Wolraich et al., 2007). Moreover, the ADHD difficulties
of adolescents place numerous demands on their parents, increasing parent stress levels
and their use of overreactive parenting practices, that in turn lead to parent-adolescent
conflict and increased adolescent behaviour problems (Seipp & Johnston, 2005).
Although current treatments do not appear to address the range of concerns experienced
by families with ADHD (Barkley et al., 2001), there may be some potential for
mindfulness-based interventions to fill this gap. Given that such approaches have the
potential to improve both parent (e.g., stress, parenting practices) and adolescent (e.g.,
attention, self-regulation, oppositionality) related variables, mindfulness strategies may
serve as an effective alternative treatment or component of intervention.
1.9 Background and Rationale of Present Investigation
Given the need for further examination of the effects of mindfulness on parent-
adolescent conflict, parent stress, as well as ADHD symptoms, the present study is an
extension and examination of a mindfulness-based program for adolescents with attention
difficulties and their parents. The program is named MYmind: Mindfulness training for
Youth with ADHD and their parents, and it was originally developed and tested by
researchers in Amsterdam (Bogels, Hoogstad, van Dun, Schutter, & Restifo, 2008).
MYmind, based on the empirically validated MBCT (Segal, Williams, & Teasdale, 2002),
is an 8-week manualized program designed to reduce ADHD symptomatology. With a
sample of 14 adolescents suffering from a range of externalizing disorders, and their
parents, Bogels et al. found that the MYmind program improved internalizing and

29
externalizing complaints, attention problems, happiness, mindful awareness, self-control,
and attunement to others, as indicated by self- and parent-report measures.
More recently, Bogels and her colleagues conducted two replication pilot studies
with children aged 8-12 with ADHD and their parents (van der Oord et al., 2012), and
adolescents aged 11-15 with ADHD and their parents (van de Weijer-Bergsma, Formsma,
de Bruin, & Bogels, 2011). Van der Oord et al. demonstrated that MYmind significantly
decreased ADHD symptoms in parents and their children, as well as parental stress and
overreactivity (based on parent reports). However, teacher ratings showed non-significant
effects. In van de Weijer-Bergsma et al. (2011), no significant changes were found across
mother and tutor reports, but fathers reported reductions in their own stress and their
adolescents’ inattention, internalizing and externalizing symptoms. Adolescents also
reported improvements in their attention and externalizing symptoms at 8-week follow-
up and demonstrated improved performance on neurocognitive computerized tasks.
However, most of these changes were not maintained at four months follow-up.
Given the preliminary evidence for MYmind as a treatment for ADHD children and
youth with behavioural difficulties and their parents, our goal was to adapt the
intervention for further investigation in a North-American culture. Moreover, considering
the mixed results when the sample comprised adolescents with ADHD, there is need for
future investigation with this group.
The present study was designed to further examine the impact of MYmind on
adolescents with ADHD and their parents. Rather than relying on pre-post questionnaires
that provide little information on the process of change seen in mindfulness programs,
time-series measurement via a daily emailed questionnaire was used to monitor the
30
ongoing reported levels of participant behaviours. The long-term effects of MYmind
were measured through continued use of emailed questionnaire over six months of
follow-up.
The current study included a Canadian sample to determine the effectiveness of the
intervention in a North American culture and was designed to evaluate changes in the
parent-adolescent relationship and family conflict. Additionally, we investigated changes
in symptoms associated with ADHD and parenting stress, as was done in previous studies
(Bogels et al., 2008; van de Weijer-Bergsma et al., 2011; van der Oord et al., 2012).
Mindfulness and acceptance-based procedures can help individuals bring automatic,
mindless behaviour into awareness to decrease maladaptive interactions (Sawyer, Cohen
& Miller, 2009). With the MYmind intervention, we hoped to teach families to identify
and alter interactions that result in relational disconnections, such as emotional
withdrawal or projected anger. We expected that through MYmind, adolescents with
ADHD and their parents could learn empathic understanding and nonjudgmental
acceptance, as well as perspective-taking and the ability to moderate behaviours focused
on changing or controlling the other’s behaviours (Greco & Eifert, 2004), thereby
rendering parent-adolescent interactions less distressing.
Through a detached, compassionate awareness of cognitions, individuals practicing
mindfulness can learn to accept their internal experiences without becoming angry or
upset by them. As a result of such enhanced emotion regulation and psychological
flexibility, mindfulness can significantly reduce stress (Kabat-Zinn, 1990), which is
heightened in parents of adolescents with ADHD (Johnston & Mash, 2001). Participants
in the MYmind program were expected to experience lower stress levels as a result of

31
exercising more adaptive coping strategies, and avoiding the potentially detrimental
influence of contextual-, and family-related stress appraisals.
Because mindfulness improves self-regulation of attention and emotion (Teasdale,
Segal, & Williams, 1995), a skill often lacking in adolescents with ADHD (Barkley,
1997), it may be an ideal treatment for this population. By cultivating a greater sense of
self-awareness, individuals practicing mindfulness can identify their impulses, distracters
and purposeless motor behaviours prior to acting on them, thereby subverting their need
to engage in inattentive, hyperactive and impulsive behaviours. Since past studies
investigating MYmind have found mostly positive results regarding its efficacy in
reducing ADHD symptoms, we hoped to replicate these findings in the present study.
Finally, given the emphasis placed on meditation in mindfulness treatments (Kabat-
Zinn, 1990), we investigated the change in meditation practice of participants throughout
the course of treatment and follow-up. Given the daily home practice prescribed each
week in treatment, and the guided meditation CD provided to each family to support their
home practice, we expected that the duration of meditation practice would increase.
Considering past research suggesting a relationship between meditation and stress
reduction (e.g., Carmody & Baer, 2008), we also hypothesized that an analysis of
participants’ reports would reveal that meditation practice predicted stress levels.
1.10 Objectives
The present empirical investigation examined the following research objectives:
1) To evaluate the efficacy of the MYmind program with a Canadian sample of
adolescents with ADHD and their parents by investigating the process of change in their
32
daily responses to an emailed questionnaire from baseline to treatment.
2) To examine the efficacy of the MYmind program in improving parent-adolescent
relationship quality. Changes and trends in the participants’ daily reports of their distress
associated with parent-adolescent conflict will be visually analyzed in time series graphs
of data over baseline, treatment and follow-up.
3) To examine the efficacy of the MYmind program in improving adolescent ADHD
symptomatology. Changes and trends in the parent and adolescent daily reports of
adolescent inattentive, hyperactive and impulsive symptoms will be visually analyzed in
time series graphs of data over baseline, treatment and follow-up.
4) To examine the efficacy of the MYmind program in improving parent and adolescent
stress levels. The change and trend in parent and adolescent daily reports about their level
of stress will be visually analyzed in time series graphs of data over baseline, treatment
and follow-up.
5) To examine the efficacy of the MYmind program in improving duration of parent and
adolescent mindfulness practice. The change and trend in parent and adolescent daily
reports of the length of time they spent meditating will be visually analyzed in time series
graphs of data over baseline, treatment and follow-up.
6) To examine whether the duration of home-based meditation was associated with parent

33
and adolescent stress levels. Parametric statistics will be used to analyze the correlation
between meditation practice and stress ratings.
Chapter 2: Method
2.1 Participants
2.1.1 Recruitment. Participants were recruited from a database of youth who were
previously involved in research through the ADHD lab at the Ontario Institute of Studies
in Education. All participants who agreed to involvement in future research were
contacted by undergraduate volunteers and asked if they would be interested in receiving
information about the present study. Additionally, participants were recruited via flyers
posted in nearby community centers and schools, and online sites related to ADHD.
2.1.2 Inclusion/exclusion criteria. To be included in the treatment program,
adolescents were required to be between the ages of 13 – 18 years of age, to have a
previous diagnosis of ADHD from a physician or mental health practitioner, and to have
at least one parent willing to participate. Given that ADHD symptoms often change with
maturation (Gustafsson, Holmström, Besjakov, & Karlsson, 2010), and many of the
potential participants may have been diagnosed at a young age, a confirmation of ADHD
symptomatology was required. Therefore, the Conners 3 - Parent version was used as a
screening tool to assess current ADHD symptomatology, as indicated by at least one
clinically significant score (T ≥ 70) on the DSM-IV Inattentive or DSM-IV
Hyperactive/Impulsive scales (Conners, 2008). Undergraduate student volunteers
administered this questionnaire and a demographic questionnaire to the parents of the
adolescents over the phone prior to enrollment in the treatment program. This diagnostic

34
screening and intake was used to determine eligibility for the program.
Adolescents with severe mental health problems (i.e., Pervasive Developmental
Disorders, Psychotic Disorders) and those with an IQ score of 80 or less were excluded
from treatment due to the possibility that these deficits could affect their ability to fully
participate in the MYmind program. The Vocabulary and Matrix Reasoning subtests of
the Wechsler Abbreviated Scale of Intelligence (WASI) were administered to obtain an
estimate of adolescents’ cognitive abilities.
Additional criteria were devised according to a secondary analysis of participation
throughout intervention. Participants were excluded if (a) they attended less than 6
sessions and did not make-up the missed sessions (b) did not respond to the daily emailed
questionnaires for more than 10 days consecutively throughout treatment, and (c) did not
participate in home meditation practice for at least 5-10 min per day for at least 1-2 days
per week, as indicated by the meditation practice item on the daily emailed questionnaires.
Insufficient meditation practice was included as an exclusion criteria because of
the strong positive relationship between frequency of meditation practice and specific
health outcomes (e.g., emotional well-being, mood, stress) (Biegel et al., 2009; Carmody
& Baer, 2008; Keune, & Forintos, 2010; Speca et al., 2000). Best practices of MBCT
suggest daily meditation of at least 30-45 min (Segal et al., 2002). However, mindfulness
research involving youth with ADHD is still emerging and many current studies do not
report a required length or duration of home practice (e.g., Singh et al., 2010). Given that
some studies suggest that short meditations practiced once or twice a week result in
positive changes in youth with mental health difficulties (Britton et al., 2010), we
included participants who meditated for at least 5-10 min per day for at least 1-2 days per

35
week.
Based on the above criteria, 11 (32%) of 34 participants enrolled (19 parents, 15
adolescents), were excluded from the study and considered treatment non-completers. Of
the 11 non-completers, three (2 adolescents, 1 parent) did not attend at least six sessions
(27%), five (3 adolescents, 2 parents) did not respond to the daily emailed questionnaire
for more than 10 consecutive days (46%), resulting in insufficient data, and three (1
adolescent, 2 parents) did not participate in home meditation practice for at least 5-10
min per day for at least 1-2 days per week (27%). Completers and non-completers did not
differ with respect to any of the measured demographic variables (see Table 1).
2.1.3 Demographic and diagnostic information. Twenty-two participants were
included in the study, including nine adolescents (4 girls, 5 boys) and 13 parents (10
mothers, 3 fathers). As shown in Table 1, eight of the nine adolescents had a history of at
least one comorbid condition, according to parent report before intervention. Although
parent ADHD was not assessed, and no other data related to a history of mental health
was collected for parents, four of the parents reported having a previous diagnosis of
ADHD. Six of the families previously participated in family therapy and five of the
families previously participated in behavioural treatment for the behaviour of the
adolescent. Seven of the adolescents were taking psychostimulant medication for ADHD
symptoms and three were taking other medications at the onset of treatment. Participants
were asked to continue treatment as usual throughout their participation in MYmind.

36
Table 1
Demographic and Diagnostic Characteristics of Participants and Noncompleters
Participants Noncompleters
Adolescent Parent Adolescent Parent
(n = 9) (n = 13) (n = 6) (n = 5)
Characteristic n % n % n % n %
Male 5 56 3 23 5 83 1 20
Female 4 44 10 77 1 17 4 80
ADHD Diagnosis 9 100 4 31 6 100 1 20
Comorbid Diagnosis
Learning
Disability
5 56 5 83
Depression 2 22 1 17
Anxiety Disorder 2 22 1 17
Tic Disorder 1 11 0 0
Use of
psychostimulant
medication
7 78 4 67
Use of other
medication
3 33 1 17
Past participation in
therapy
Family therapy 6 67 6 46 5 83 4 80
Behavioural 5 56 5 38 4 67 3 60

37
therapy
Marital Status
Married 10 77 5 100
Single 1 8
Divorced/separated 2 15
Education level
Some college or
university
1 8
College diploma 3 23 3 60
Undergraduate
university degree
5 38 1 20
Postgraduate
degree
4 31 1 20
English spoken at
home
7 78 11 85 5 83 4 80
M SD M SD M SD M SD
Age (years) 16.11 1.62 48.82 3.82 14.5 1.64 50.2 6.57
2.2 MYmind Program Description
2.2.1 MYmind: Mindfulness training for Youth with ADHD and their
parents. MYmind, based on the empirically validated MBCT program developed by
Segal et al. (2002), is an eight week manualized group treatment program for adolescents
with ADHD and their parents. The purpose of MYmind is to foster mindfulness through
training in formal meditation practices, and to integrate this awareness and attitude into
the context of daily life as a means of coping with ADHD symptoms, stress, family
38
relations and difficult emotions. It was originally developed and piloted in the
Netherlands (Bogels et al., 2008). For the purposes of the current study, the manual and
participant handouts were translated from Dutch into English, with review by the original
authors for accuracy. The Canadian version of the manual was modified to reflect the
current cultural and linguistic trends of a major North American urban centre. For
example, videos of European celebrities were replaced with videos featuring North
American celebrities. Content was also added to ensure that the manual remained
consistent with the goals of the current study and appropriate for the population under
investigation. For example, psycho-education about the history, meaning and applications
of mindfulness was added because many participants were novices to mindfulness.
Reflection sheets, which asked participants to think about their experiences in MYmind,
were incorporated into the 4th and 8th sessions to gauge treatment impact, enhance
motivation for change, increase adherence, and maintain therapeutic rapport.
2.2.2 General overview of program. Families were invited to attend an intake
interview with a facilitator to discuss motivation, commitment, and individualized goals
for the program. Families were also asked to identify barriers that could interfere with
their participation in the program (e.g., transportation). The purpose of the interview was
to assess readiness and suitability for the program, establish therapeutic rapport, and
enhance engagement in the therapeutic process. Families who were deemed to be a good
fit for the intervention were enrolled in the next available group.
Parents and adolescents attended parallel groups. For both groups, each 1.5 hour
session consisted of activities and discussions related to major themes, and included
elements of mindfulness/yoga, CBT, and psycho-education. The core mindfulness

39
concepts emphasized throughout the program were awareness, non-judging, acceptance,
letting go, beginner’s mind, and presence in the moment. Mindfulness exercises included
the body scan, 3-min breathing space, sitting meditation, and mindfulness in everyday
activities, such as eating. These exercises were modified to ensure compatibility with the
needs of the participants. For example, adolescents began with very brief meditations
(e.g., 5 min), and gradually increased the length of meditation each week. The groups
discussed the application of mindfulness practices to their everyday struggles (e.g.,
breathing space before a test or during an argument). The CBT component of the
program consisted of identifying thoughts, feelings and sensations; exploring the ways in
which thoughts and feelings influence actions; recognizing cognitive distortions; and
noticing automatic thoughts and patterns of behaviour. In keeping with the philosophy of
mindfulness, emphasis was placed on awareness and acceptance of internal and external
experiences. Psycho-education about mindfulness, attention, and ADHD was delivered in
the initial sessions through videos, didactic presentations and discussions, and reviewed
in subsequent sessions as needed.
Home exercises were a required component of the program. Each family was
given a CD with guided meditations to support their home practice. Parents and
adolescents received workbooks containing summaries of key concepts, assignments, and
space to record their experiences during the week. Participants received daily text
messages reminding them to practice mindfulness at home. To increase levels of
engagement and reduce the risk of dropout, adolescents earned points for participation in
mindfulness exercises in session and at home. These points were exchanged for rewards
from parents (e.g., computer time) and from facilitators (e.g., movie passes). A joint

40
parent-adolescent booster session was held approximately six weeks after the completion
of MYmind. The purpose of the booster session was to review progress toward goals,
trouble-shoot with families who were having difficulty maintaining their mindfulness
practice, and provide individualized feedback about improvements to each family.
Groups were facilitated by doctoral students with Masters degrees in clinical child
psychology who had therapeutic experience with children and families. Both facilitators
were Caucasian, female, and in their mid-twenties. Facilitators attended a 12-week
mindfulness course for mental health professionals and practiced mindfulness meditation
regularly. Supervision was provided in-vivo during sessions and in weekly debriefing
meetings with two registered clinical child psychologists. One facilitator ran all four
parent groups and the other facilitator ran all four adolescent groups to ensure treatment
consistency and to control for therapist effects. Facilitators followed the manual closely
to ensure treatment fidelity.
2.2.3 Adolescent sessions. Adolescent groups consisted of 3-5 participants and 1-
2 facilitators. Adolescent sessions were conducted in a quiet, low-stimulus room
furnished with chairs, yoga mats, cushions, an easel with chart paper, and a projector. In
order to provide consistency and predictability, sessions followed a standard format and
activities were outlined on an agenda. The agenda was displayed in a prominent place
and reviewed at the beginning of each session. The agenda delineated the theme of the
session, the main activities, and the points associated with participation in the activities.
Each session began with a guided sitting meditation. Adolescents were
encouraged to use chairs for meditation because chairs support correct posture (i.e.
prevent slouching) and promote generalization to other settings (e.g., similar to sitting in

41
a desk chair, at the kitchen table, or on the bus). In the final few sessions, adolescents
were introduced to zafu cushions as an alternative option. Sessions began with short (5
min), highly structured meditations in which the facilitator provided frequent guidance
and reminders to return their attention to their breath. The length of the meditation
gradually increased and the level of scaffolding gradually decreased each week. By the
final session, adolescents were expected to meditate for 15 min with only minimal
guidance from the facilitator. Sitting meditations were followed by group discussion
about thoughts, feelings, and sensations that arose during the exercise. These discussions
were included to foster curiosity, openness, and nonjudgmental acceptance of moment-to-
moment experiences. Following a brief review of the concepts covered the previous week,
the facilitator introduced the main theme of the session.
Content was delivered via teaching, group discussions, videos, images, poetry,
mindful activities, games, and role-play. The content of the first four sessions focused on
awareness and acceptance of self in relation to ADHD. Major topics of discussion
included the symptoms of ADHD, positive attributes associated with ADHD, challenges
faced by teens with ADHD (e.g., anxiety, depression, peer relations, learning problems),
the impact of ADHD on daily functioning, and the applications of mindfulness for
ADHD (e.g., improving focus, reducing impulsivity). The aim of the latter four sessions
was to cultivate mindful relationships. Adolescents learned to identify their automatic
reactions and make mindful choices, use mindfulness techniques to regulate their
emotions during conflicts, listen with full attention, respond to others with empathy, and
refrain from judging themselves or others. For an overview of major themes and activities,
see Table 2.

42
Adolescents also participated in 10 min of mindful yoga each week. They were
guided to focus attention on their breath and the sensation of their muscles stretching and
contracting with each pose. Yoga was done near the end of each session to help the
adolescents calm their breath, bodies and minds and ease the transition from the
therapeutic space to the outside world. Each session ended with a discussion about home
practice assignments and points.
2.2.4 Parent sessions. Parent groups included 3-7 participants and 1 facilitator.
Parent sessions were held in a quiet room with a large table and chairs in the center, zafu
cushions placed in a circle towards the back, an easel with chart paper towards the side,
and a projector screen at the front. Posters stating relevant quotes were posted on the
walls at the start of almost every session to reflect that session’s theme. Each session
began with parents seated on zafu cushions for a meditation that gradually increased in
duration each week. In the first session, the facilitator guided parents through a 5-min
structured sitting meditation. Facilitator supervision was gradually faded over the course
of the program. By the final session, parents were meditating independently with no
guidance for 30 – 40 min.
All sessions ended with a shorter (e.g., 5 -10 min) meditation, which differed
from the sitting meditation. These different meditation practices (e.g., a body scan,
breathing space, metta meditation or a mountain meditation), were introduced, discussed
and then practiced. The range of exercises provided the parents with a variety of options
to practice their breathing and awareness at home. Parents were encouraged to practice
the exercises that were most applicable to their lifestyle, level of experience, and practical
constraints (e.g., physical limitations). All meditations were followed by a group

43
discussion in which parents were given the opportunity to explore their experiences with
curiosity and acceptance. The facilitator encouraged the parents to discuss any obstacles
they may have experienced (e.g., recurring distractions), or thoughts, emotions and
sensations that surfaced during the meditation.
The content of the sessions focused on the participants’ role as parents and the
specific challenges they face in raising an adolescent with ADHD. Therefore, in addition
to formal meditations and mindfulness exercises, activities and discussions addressed the
application of mindfulness to their relationship with their adolescent. For example,
parents were taught to observe themselves and their adolescent with acceptance and
compassion. They learned to attend to the attributions and expectations they make about
themselves and their adolescent that allowed them to bring an open, nonjudgmental
stance to their parenting interactions. They were encouraged to become more aware of
their stressful triggers and to preemptively make conscious choices about how to respond,
rather than reacting automatically. Many activities focused on specific skills, including
communication, problem-solving, empathic understanding and self-compassion. For a
summary of the main themes and exercises, see Table 2.
In session, each topic was typically first discussed by the facilitator through
didactic teaching, videos, or powerpoint presentations. Parents were then asked to engage
in a group discussion, role-play, or reflection on a poem or quote. This structure was used
to facilitate both didactic and experiential learning, in addition to providing parents with a
forum to share personal experiences and ask questions. All sessions concluded with a
discussion of that week’s home practice assignments and handouts.

44
Table 2
Brief Overview of the Content of Adolescent and Parent Sessions
Adolescent Sessions
Theme Activities
1. Attention Welcome, sitting meditation, psychoeducation about ADHD,
group contract, review points system, mindful eating activity
2. At Home in Your
Body
Sitting meditation, psychoeducation about mindfulness, body
scan, yoga with emphasis on body
3. Breath Sitting meditation, breath for daily activities, 3-minute
breathing space, yoga with emphasis on breath
4. Distraction and The
Wandering Mind
Bubble meditation, fixation exercise (stationary point vs.
moving object), attention to detail game, meditation with
sounds, yoga, half-way reflection
5. Thoughts are Not
Facts/ Doing Homework
Mindfully
Movie theatre meditation; moods, thoughts and alternative
viewpoints exercise; detective thinking to challenge automatic
thoughts; impulse control activity with candy bar; applying
mindfulness skills to homework; yoga
6. Automatic Reactions Sitting meditation, automatic pilot (expressway vs. pathway),
role-play, yoga, breathing space with coping and choices
7. Mindful
Communication
Sitting meditation with stressful event and empathy; thoughts,
feelings and sensations related to automatic pilot; being
present in communication; mindful listening role play; yoga
8. On Your Own Sitting meditation, adolescent-led mindfulness exercises,

45
reflection activity, action plan for continuing mindful practice,
Metta meditation
Parent Sessions
Theme Activities
1. Awareness Welcome and introductions, sitting meditation, rationale of
training, raisin exercise, introduction to mindfulness,
explanation of homework assignments and adolescents’
reward system
2. At Home in Your
Body
Sitting meditation with emphasis on body, discussion of
obstacles to home practice, psychoeducation about ADHD,
psychoeducation about mindfulness and its connection to
parenting, body scan
3. Breath Sitting meditation with emphasis on the breath, pleasant
events calendar and triangle of awareness, poem and
awareness activity, introduction to 3-minute breathing space
4. Responding with
Awareness
Sitting meditation, unpleasant events calendar,
psychoeducation about stress and automatic responding,
responding with awareness activity, 3-minute breathing space,
half-way reflection
5. Automatic Reactions
and Patterns
Sitting meditation, psychoeducation and discussion about
automatic behaviour patterns/parenting practices, sitting
meditation with stressful event and empathy
6. Communication and Sitting meditation, role-play on communication with child,
46
Empathy mindful listening activity, breathing space with coping and
choices
7. Acceptance and
Boundaries
Sitting meditation, perception poem and reflection, breathing
space with feeling boundaries, changing vs. accepting action
plan, mountain meditation
8. On Your Own Sitting meditation, written inquiry, presentation of symbol or
experience, reflection activity, action plan for continuing
mindful practice, Metta meditation, discussion of booster
session
2.3 Procedure
The intervention was delivered to 16 families across four groups of 3-5 families.
The groups were capped at five families to ensure that all participants were able to
participate fully in the exercises and discussions. The treatment was carried out in two
waves over a period of seven months, with the first two groups running from April to
June 2011 and the second two groups from June to August 2011.
Prior to enrollment in MYmind, adolescents and their parents attended individual
interviews lead by the group facilitators. The goals, expectations and potential risks and
benefits of the MYmind program were explained in detail. The individual interviews with
families and group facilitators were also used to ensure that MYmind was a good fit for
each families’ needs, and to enhance participants’ motivation by setting personal goals.
Following these meetings, participants were given a package containing an information

47
letter (see Appendix A), consent form (see Appendix B), and standardized questionnaires
that were included for a separate study. Youth who did not have a previous cognitive
assessment confirming an IQ above 80 were administered the WASI in a separate room
by one of the group facilitators. Approximately one month after these initial meetings,
participants started the MYmind program, which ran for eight consecutive weeks. Six
weeks following the last session of MYmind, participants were offered an additional
booster session.
All participants were required to complete the DSQ individually, which was
emailed to them each day at a specified time. A few adolescents did not have an email
account that they checked regularly and thus, either had the questionnaires sent to their
parents’ email address for them to complete, or were given paper questionnaires that they
submitted each week. In addition to the emails, participants received a daily text-message
reminding them to meditate and to check their email for the purpose of questionnaire
completion. The participants were asked to complete the questionnaires every evening
during baseline and treatment phases and then for one week every month for six months
following the completion of treatment (Follow-up). On the final day of treatment, the
participants were asked to complete a Consumer’s Satisfaction Questionnaire to evaluate
the acceptability of the MYmind program.
2.4 Measures Used to Describe and Define the Sample
2.4.1 Demographics Questionnaire. Undergraduate volunteers administered the
demographic questionnaire to parents over the phone prior to their enrollment in the
treatment program (see Appendix C). The demographics questionnaire contained

48
questions concerning the adolescent’s health history, adolescent use of medication, past
participation in psychotherapy, parental education and employment status, and family
composition.
2.4.2 Conners’ Parent Rating Scale—Third Edition. The Conners’ Parent Rating
Scale -Third Edition (Conners, 2008; Conners 3-P) was administered to parents over the
phone by graduate or undergraduate student volunteers to confirm continuation of ADHD
symptoms in adolescents prior to enrollment in treatment. The Conners 3-P is a norm-
referenced questionnaire used to evaluate inattention, hyperactivity and impulsivity, as
well as executive functioning, learning problems, aggression, peer relations, and family
relations. Parents were asked to rate their adolescent on a 4-point scale from 0 (Not at
all/Seldom, Never) to 3 (Very Much True/Very Often, Very Frequent). The two DSM-IV
ADHD subscales on the Conners 3-P (DSM-IV Inattention, DSM-IV
Hyperactivity/Impulsivity) demonstrate high internal consistency (.93, .92) and adequate
to high test-retest reliability (.84, .89).
2.4.3 Wechsler Abbreviated Scale of Intelligence (WASI). The WASI (Wechsler,
1999) is a standardized abbreviated intelligence test, which provides an estimate of
general cognitive ability. For those adolescents who did not have a recent assessment of
their cognitive abilities, the WASI was administered to them to confirm an IQ of at least
80. The Vocabulary and Matrix Reasoning subtests were administered by one of the
facilitators prior to enrollment in treatment. The WASI has high internal consistency (.93)
and test-retest reliability (ranging from .88 to .93) across the two IQ scales.

49
2.5 Outcome Measures
2.5.1 Daily Symptoms Questionnaire (DSQ). The Daily Symptom Questionnaire
(DSQ) was developed by the primary investigator and her supervisor (see Appendix D).
In designing the DSQ, we had two main objectives: (1) to develop an objective measure
of a wide range of mental health issues relevant to families with ADHD, (2) to make sure
the questionnaire was short and straightforward, so that respondents could complete the
measure everyday via email. The parent and adolescent versions of the DSQ measured
the same constructs.
Because we hypothesized that participation in the MYmind program would
improve the participants’ stress levels and family conflict, two major concerns in families
with ADHD, we included one item evaluating participants’ stress levels and one
evaluating parent-adolescent conflict. We also hypothesized that participation in the
MYmind program would reduce adolescents’ ADHD symptomatology. Therefore, we
included three ADHD symptom items, one to assess inattention, one for hyperactivity and
one for impulsivity. Both parents and adolescents were asked to evaluate the adolescents’
ADHD symptomatology since research indicates that adolescents’ reports of their own
symptoms markedly differ from parent reports about their adolescents (Rasmussen et al.,
2002).
Another item asked how much time participants spent with their parent/adolescent,
providing a potential means of determining whether lack of stress or conflict was due to a
lack of interaction. Lastly, one item queried the duration of home-based meditation
practice to investigate whether more meditation leads to greater treatment effects.
Overall, this 7-item questionnaire was developed to investigate whether participation in

50
the MYmind program would result in less stress, less parent-adolescent conflict, reduced
levels of ADHD symptomatology and greater meditation practice.
The 7-item DSQ incorporated a 5-point likert scale format that was easy for
participants to complete in a short period of time. Participants were asked to respond to
each item by typing an X beside the rating that best describes their feelings and
behaviours that day. The 5-point scale ranged from 1 (Not at all, Not very, Almost none)
to 5 (A lot, Very well, More than __ time). Participants were also sent an instruction
sheet that provided an operational definition of each level of each construct (see
Appendix E), to help participants assess their behaviours/emotions and differentiate
between different levels of a construct. For example, “a little” stress was defined as
feeling fairly calm, and only mildly bothered by events that day.
2.5.2 Consumer-Satisfaction Questionnaire (CSQ). The Consumer-Satisfaction
Questionnaire (CSQ) assessed parent and adolescent satisfaction with intervention efforts
as a measure of social validation of study results (Wolf, 1978). The CSQ was developed
by the primary investigator and modeled after a similar measure used for other treatments
in previous studies (Ducharme & Drain, 2004; Ducharme, Atkinson, & Poulton, 2001)
(See appendix F). The CSQ includes 15 items divided into three sections. The first
section consists of nine 5-point likert scale items and two open-ended questions asking
participants about their experience in the MYmind program. The second section includes
three items for rating group facilitators on a 5-point likert scale. The third section
comprised one open-ended question asking participants to share any general comments
about the MYmind experience. Both adolescent and parent participants were asked to
complete the CSQ on the final day of treatment.
51
2.6 Research Design
The multiple Daily Symptom Questionnaire (DSQ) responses from each
participant throughout the course of baseline, treatment and follow-up provided a source
of time-series measurement that could be used as part of a multiple baseline design.
Baseline DSQ measurement began simultaneously for the first two groups; at a later time,
baseline DSQ measurement for the second two groups was also initiated simultaneously.
For multiple baseline purposes, intervention was introduced in a time-lagged fashion.
Group A had two weeks of baseline, Group B had three weeks of baseline, Group C had
four weeks of baseline, and Group D had five weeks of baseline (See Figure 1). Thus,
Group B served as a form of waitlist control for Group A, and Group D provided a form
of waitlist control for Group C. Moreover, the longer time lags for Groups C and D
contributed an additional component to the research design, providing a more rigorous
control for length of time engaged in pre-treatment measurement.
With this multiple baseline format, experimental control is demonstrated if levels
of responding remain unchanged until the independent variable is introduced, regardless
of the varied lengths of baseline phases (Hartman & Hall, 1976). In the present study,
DSQ measurement of the first group was expected to change with the introduction of the
MYmind program, while the behaviour of untreated groups was expected to remain
stable until the subsequent introduction of the intervention.
In this design, baseline measures of specific behaviours of individual participants,
such as the duration of parents’ and adolescents’ meditation practice, or their overall
stress levels, were compared to the same measures following introduction of the
intervention, and during post-intervention follow-up, to determine the extent of treatment

52
effects. One of the advantages of multiple baseline time-series measurement is that it
enables the researchers to observe the process of change in the pattern of treatment results
over a period of time, while ruling out the confounding influence of chance fluctuations
in behaviour, historical events, and maturation effects (Myers & Hansen, 2006).

53
2.7 Data Analysis
2.7.1.Time-series analysis. Based on the daily-submitted DSQ, the number
response to each item was entered into a database to measure the related construct (e.g.,
general stress) over baseline, treatment and follow-up for each participant. Response
means for each participant were calculated across baseline, the first four weeks of
treatment, the last four weeks of treatment and follow-up to compare the mean difference
of each construct from baseline to follow-up. As is appropriate for time-series designs,
data points and mean lines were analyzed through visual analysis of graphic displays of
the daily response data (Hersen & Barlow, 1976). The graphs were examined to evaluate
the magnitude of change, rate of change, and diversity of responses from baseline to
follow-up. To assess the magnitude of change, the changes in level (i.e., shift or
discontinuity in practices) across phases were examined. The rate of change was
evaluated through inspection of changes in trend (i.e., systematic increase or decrease)
and latency of the change (i.e., the temporal proximity of the change to the introduction
of treatment) (Kazdin, 2001). The variability of data was investigated by examining the
degree to which behaviour fluctuated across and within phases (Horner et al., 2005). In
keeping with the multiple-baseline across groups design, visual analysis also entailed
comparison of baseline levels of one group of participants to the concurrent post-
treatment levels of participants for whom treatment had already occurred, as a form of
time-series wait-list control group comparison (Kazdin, 2001).
2.7.2. Generalized estimating equations (GEE). Considering the relatively small
sample size of the present investigation, the dependent nature of the data, and the lack of
assumptions about the distribution of the behaviours of interest in the general population,
54
most parametric statistical analyses could not be used in the current analyses. However,
generalized linear modeling supports non-normal distributions for dependent variables,
and generalized estimating equations (GEE) extends general linear models further by
involving dependent data for repeated measures, logistic regression and various other
models for time series or correlated data (Ballinger, 2004; McCullagh & Nelder, 1989).
For general linear models, data must meet the assumption of normality, independence and
homogeneity of variance, but the GEE method accounts for the correlation of responses
within response variables and is flexible enough for use in analyzing response variables
that are not normally distributed. Therefore, these are parametric approaches, which have
unique assumptions regarding the distribution of the reported data (Neal & Simons,
2007). GEEs are used to estimate the parameters of a generalized linear model with a
possible unknown correlation between outcomes. When faced with longitudinal data that
consists of repeated measures that may be correlated within a subject, researchers must
consider the correlation within responses when estimating regression parameters.
Otherwise, they can make incorrect inferences about the regression coefficients and
inefficient or biased estimates of the regression coefficients (Diggle et al., 2003) that
could lead to false conclusions regarding their research questions. Thus, the GEE
procedure allows for a better model fit over analyses based on ordinary least squares
(OLS), such as analysis of variance (ANOVA) and multiple regression (Ballinger, 2004).
To fulfill objective #6 (i.e., ‘to examine whether the meditation component of the
MYmind program had an independent relationship with participants’ stress-related
outcomes’), a GEE analysis was conducted. Considering past research has suggested a
potential correlation between stress reductions and at-home meditation practice among

55
other populations (e.g., Carmody & Baer, 2008; Speca et al., 2000), the current study
aimed to investigate whether meditation practice would positively impact the stress levels
of parents and youth with ADHD. No past research has suggested a relationship between
meditation practice and any of the other constructs being investigated in the present study,
so only stress levels were further analyzed.
The GEE analysis was conducted with a gamma distribution and a log link. The
construct-specific participant stress-related indicators were transformed to reflect a
positively skewed gamma distribution. The gamma distribution was chosen because the
aforementioned dependent variables are ordinal, positively skewed and the gamma
distribution represented the best fit to the distribution of the dependent variable, stress. A
log link was chosen because it applies to positive numbers and ensures a positive mean
(Ruppert, Wand & Carroll, 2003). Generalized estimating equations were the selected
method of analysis because participants’ responses were correlated over time. Given the
time-series nature of the data, phase (baseline, treatment and follow-up) was included as
a variable in the model, in addition to the parent or adolescent status of the participant, to
determine whether either of these variables affected stress levels. The impact of
adolescent/parent status and phase was assessed by adding the interaction terms in the
analysis.
Chapter 3: Results
To investigate the effects of MYmind on parents and their adolescents with ADHD,
we examined both trends in the time series data and mean levels for each phase of
intervention: baseline, the first four weeks of treatment, the last four weeks of treatment,

56
and follow-up. For a data series in which there was a substantial positive change in level
from baseline to treatment that continued in follow-up, the series was considered a
treatment improvement with maintenance. When the data series showed substantial
positive change from baseline to treatment that did not continue in follow-up, the series
was deemed a treatment improvement without maintenance. For a data series that showed
no substantial change in treatment, but a positive change from baseline to follow-up, the
series was considered a late treatment improvement. Finally, a data series that indicated
no substantial change from baseline to treatment or from baseline to follow-up was
deemed as representing no improvement.
To distinguish the extent of treatment improvements, differential levels of
improvement magnitude were established. If the mean demonstrated a positive change
from baseline to treatment/follow-up of 0.5 to 0.9 (10 – 19%), it was classified as a small
improvement. If the mean showed a positive change of 1.0 – 1.9 (20 – 39%), it was
classified as a medium improvement. If the mean demonstrated a positive change of 2.0
or greater (40% or more), it was classified as a large improvement. For a series to be
considered a treatment improvement, visual analysis of time-series data trends had to
corroborate the changes in mean levels.
3.1 Participant Stress
3.1.1 Parent self-report of stress. Visual analysis of data trends and mean levels in
Figure 2 suggests that participation in MYmind had a reductive effect on parent reported
levels of stress for the majority of parents. Although data for stress ratings remained
somewhat variable at the onset of treatment, 11 of 13 parents (85%) showed notable
57
improvements in the last half of treatment and/or across follow-up. Regarding magnitude
of change, six parents reported medium treatment improvements (P1, P2, P3, P6, P12,
P13), five parents reported small treatment improvements (P4, P5, P7, P9, P11) and two
parents reported no improvements (P10, P13). Of the eleven parents who reported at least
some positive change, seven of them reported treatment improvements that were
maintained in follow-up (P1, P2, P3, P4, P7, P12, P14), three of them reported a late
treatment improvement (P5, P6, P11), and one of them reported improvements that were
not maintained in follow-up (P9). As a further demonstration of the stable patterns of low
stress levels after intervention, no parents reported the two highest levels of stress, “A lot”
or “Quite a bit”, in follow-up.

58
Note. Mean lines highlighted in blue.

59
Note. Mean lines highlighted in blue.

60
Note. Mean lines highlighted in blue.
61
3.1.2 Adolescent self-report of stress. Visual analysis of data trends and mean
levels in Figure 3 reveals that participating in MYmind had a reductive effect on stress
levels for adolescent participants. Eight of the nine adolescents (A1, A2, A3, A4, A5, A6,
A7, A8) showed small decreases by the end of treatment and/or in follow-up, and one
adolescent reported no improvement (A9). Of the eight adolescents reporting reduced
stress, one of them reported treatment improvements that were maintained in follow-up
(A3), four of them reported late treatment improvements (A1, A2, A4, A5), and three of
them reported improvements that were no longer present in follow-up (A6, A7, A8).
As indicated by visual analysis and mean levels, most adolescents reported high
and variable levels of stress throughout baseline and at the start of treatment. However, a
downward trend throughout treatment can be seen in Figure 3, suggesting somewhat
lower levels of stress near the completion of this phase or in follow-up. For instance, the
majority of adolescents’ stress ratings decreased by one level so that those reporting
“Quite a bit” of stress at the start of treatment were mainly reporting “Some” stress by the
end, and those reporting “Some” stress at the onset were reporting “A little” stress or
“Almost none” by the final sessions. However, stress ratings increased for A4, A5, A7
and A8 in follow-up, when school resumed in September (indicated on the graph by
vertical dotted lines).
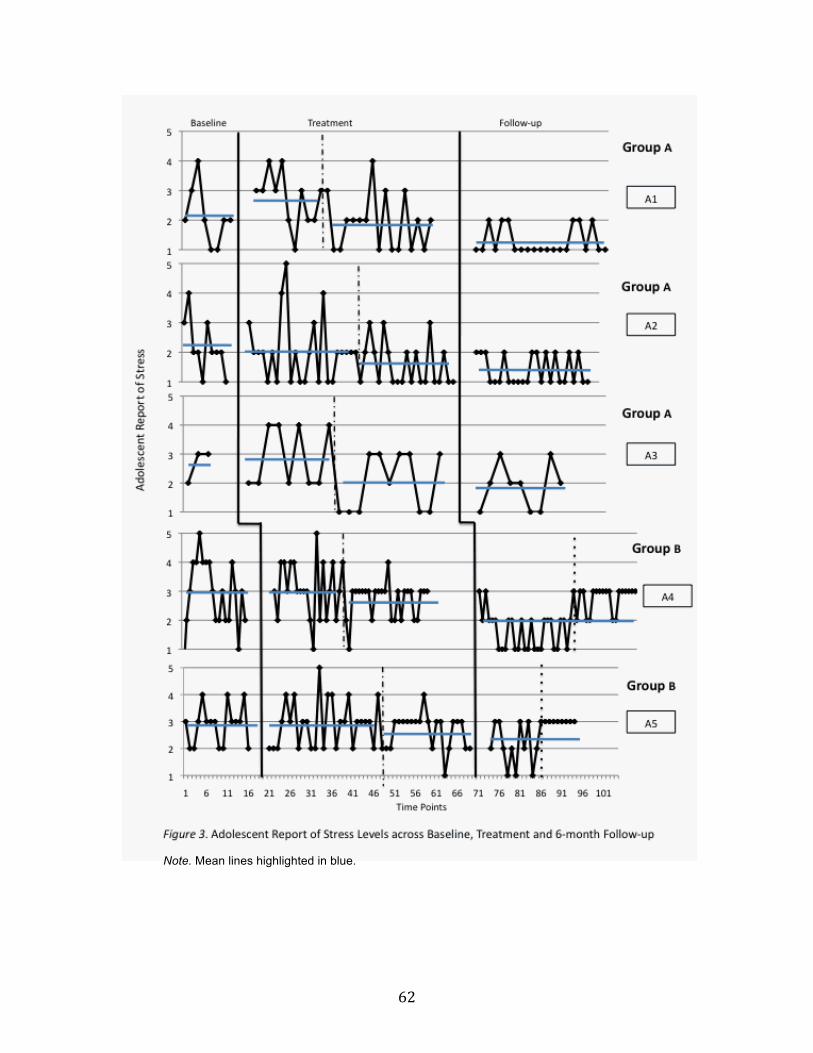
62
Note. Mean lines highlighted in blue.

63
Note. Mean lines highlighted in blue.

64
3.2 Participant Distress due to Family Conflict
3.2.1 Parent self-report of distress due to conflict with adolescent. Given that
one parent completed two of these items each day because of her two adolescent
participants, 14 rather than 13 parent reports are included in the analysis of parent distress
due to family conflict. Visual analysis of data trends and mean levels in Figure 4
indicates that completion of MYmind had a positive effect on the parents’ self-reported
distress from conflicts with their adolescents. For 10 of the 14 parents (71%), there was a
downward trend in reports of distress from family conflict during treatment, with a much
lower level of variability by the end of this phase and in follow-up. Six parents reported
medium improvements (P2, P3, P4, P11, P12, P14), four parents reported small
improvements (P1, P5, P6, P13) and four parents reported no improvements (P7, P8, P9,
P10). All four of the parents demonstrating no treatment effects reported baseline levels
predominantly in the “Almost none” or “A little” distress range with baseline means
below 1.9, providing little potential for improvement. Thus, 10 of the 10 parents (100%)
with real potential for change reported reduced levels of distress from conflict.
Visual analysis of Figure 4 shows that more than half of the parents (57%) reported
distress ratings that were higher at the onset of treatment than in baseline. Despite these
increased distress ratings, seven of the 10 parents who indicated some distress reduction
reported treatment improvements that were maintained in follow-up (P2, P3, P4, P6, P11,
P12, P14), and the other three parents reported late treatment improvements (P1, P5, P13).
These follow-up data suggest that the further treatment progressed, the less distressing
conflicts with their adolescents became. In fact, no parent reported that they were
experiencing “A lot” or “Quite a bit” of distress due to family conflict throughout six
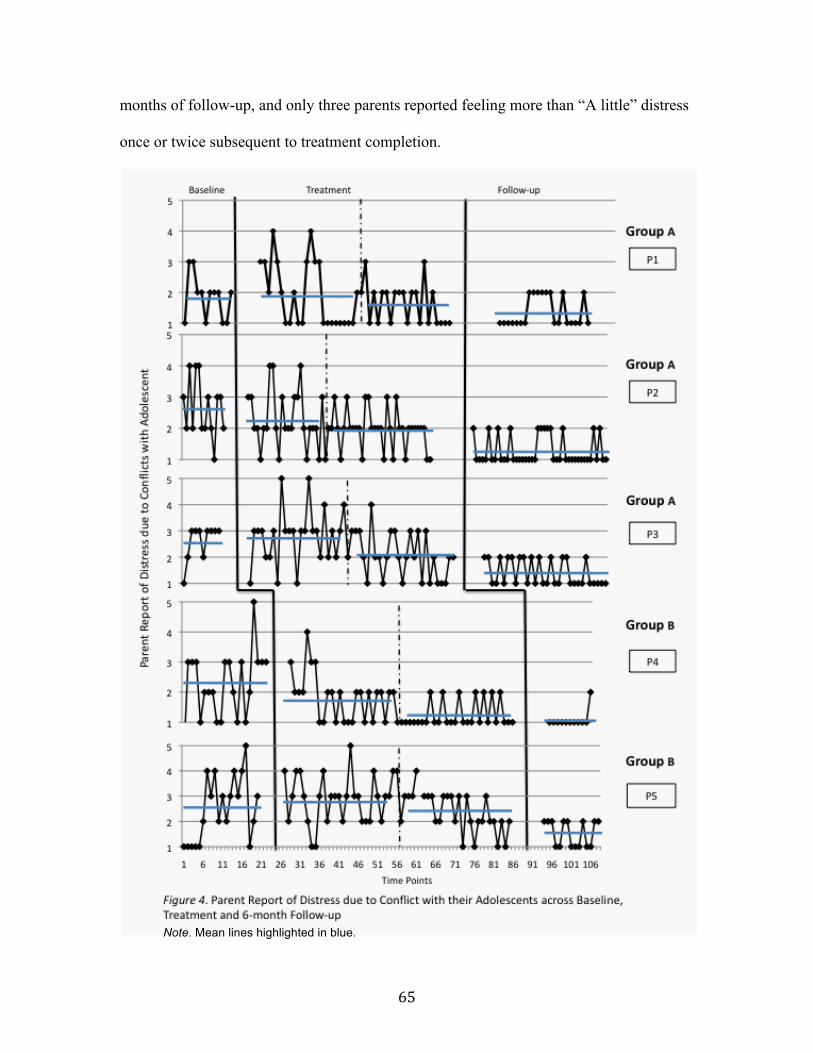
65
months of follow-up, and only three parents reported feeling more than “A little” distress
once or twice subsequent to treatment completion.
Note. Mean lines highlighted in blue.

66
Note. Mean lines highlighted in blue.
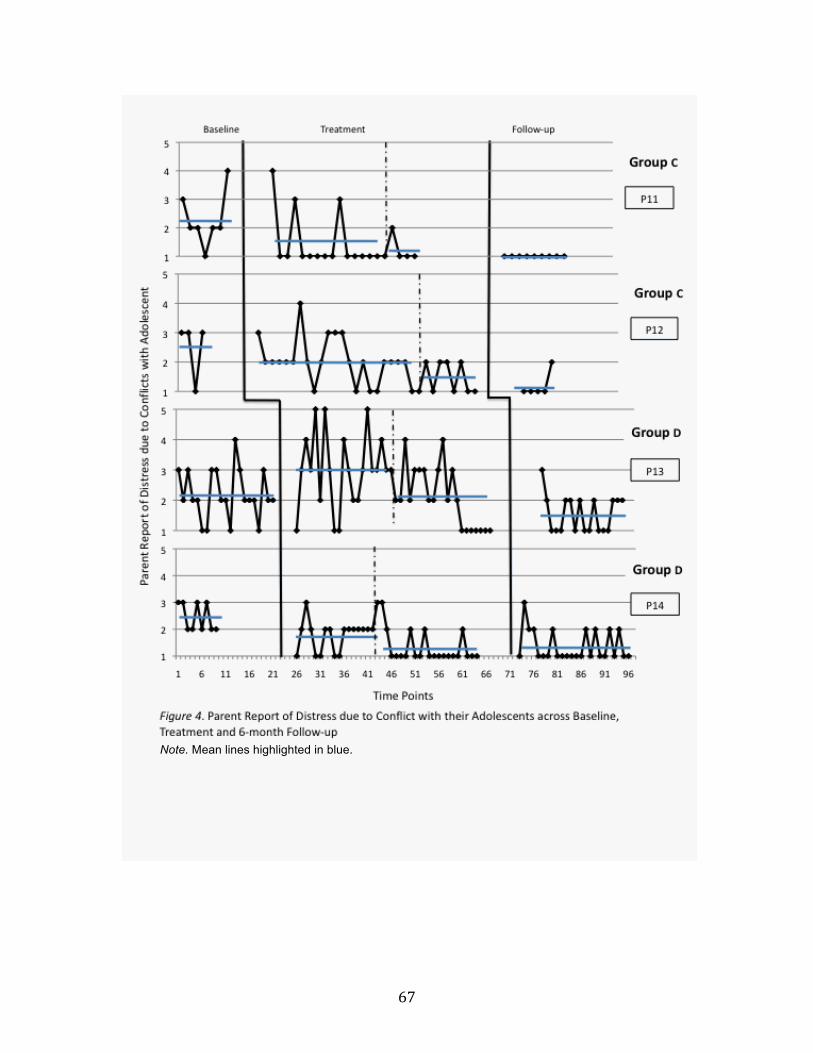
67
Note. Mean lines highlighted in blue.

68
3.2.2 Adolescent self-report of distress due to conflict with parent. Visual
analysis of data trends and mean levels in Figure 5 shows that participation in MYmind
had a positive impact on adolescent-reported distress due to conflict with their parents,
with seven of nine adolescents (78%) showing improvements. Three adolescents reported
medium improvements (A6, A8, A9), four adolescents reported small improvements (A1,
A2, A3, A4) and two adolescents reported no improvements (A5, A7). Treatment data
were generally characterized by a downward trend with lower, more stable levels of
distress as treatment progressed and no adolescents reporting high levels of conflict-
related distress (e.g., “A lot” or “Quite a bit”) during the second half of treatment or
follow-up. Of the seven adolescents reporting a reduction in distress, four of them
reported treatment improvements that were maintained in follow-up (A2, A4, A8, A9),
and the other three adolescents reported late treatment improvements (A1, A3, A6).
Similar to parent distress ratings, adolescents’ distress data in follow-up suggest that the
treatment effects maintained or improved with time.
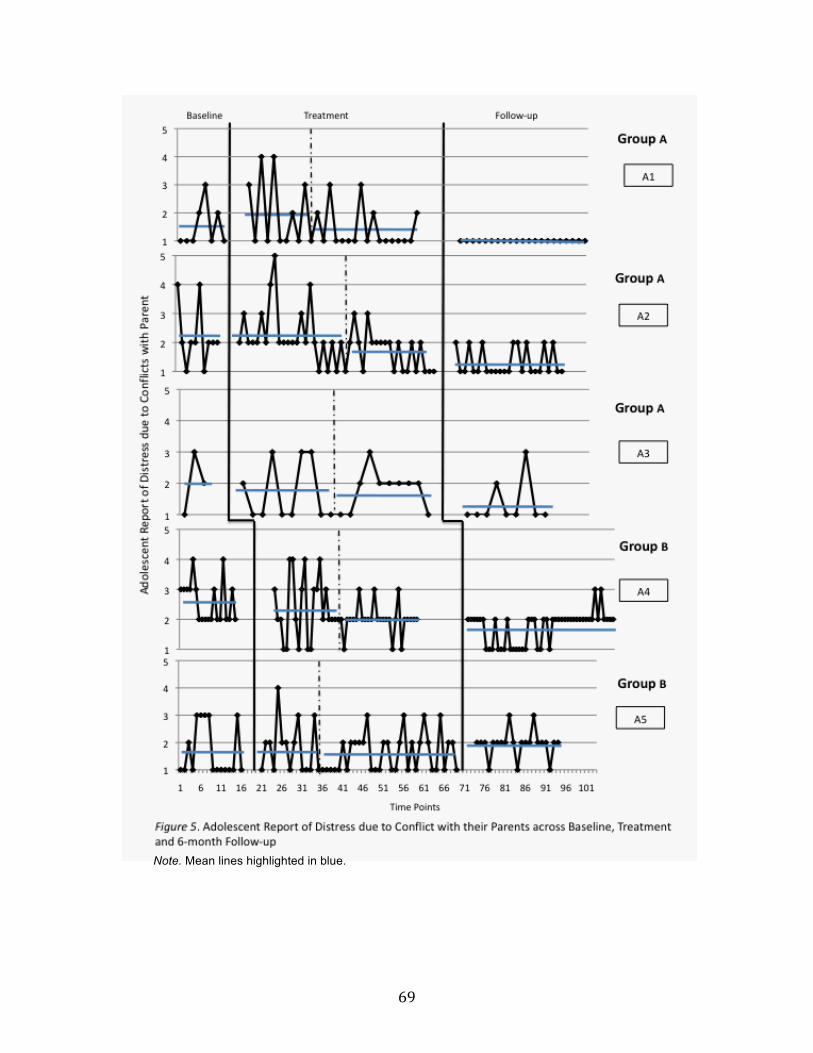
69
Note. Mean lines highlighted in blue.

70
Note. Mean lines highlighted in blue.

71
3.3 Adolescent Inattention
3.3.1 Parent report of inattention in adolescents. Given that one parent
completed two of these items each day because of her two adolescent participants, 14
instead of 13 parent reports are included in the analysis of adolescent inattention. Visual
analysis of data trends and mean levels in Figure 6 demonstrates that participating in
MYmind had a reductive effect on a subsample of adolescents’ inattention levels,
according to parent reports. Nine of 14 parents (64%) reported that their adolescents
experienced less difficulty paying attention subsequent to completing MYmind. However,
some of these downward trends were difficult to discern and characterized by a high
degree of variability.
Of the nine parents who reported a notable decrease in their adolescents’
inattention, one parent indicated a large improvement (P12), two reported medium
improvements (P4, P11), and six indicated small improvements (P1, P2, P3, P5, P6, P14).
Five parents reported no changes across phases (P7, P8, P9, P10, P13). However, given
the nearly flat baselines of P9 and P10, there was no potential for their ratings to improve.
Thus, of the 12 parents whose data had the potential for improvement, nine parents (75%)
reported positive changes in their adolescents’ inattention symptoms.
Analysis of trends and mean levels suggest that of the nine parents who reported a
reduction in adolescent inattention, four of them reported treatment improvements that
were maintained in follow-up (P4, P11, P12, P14), four of them reported a late treatment
improvement (P1, P2, P3, P5), and one of them reported improvements that were not
maintained in follow-up (P6). Most parents reported many more low ratings during the
latter half of treatment and follow-up with less variability compared to baseline and

72
initial weeks of treatment. P6 showed a unique pattern of results with reports of lower
levels of adolescent inattention at the end of treatment and start of follow-up compared to
baseline and the start of treatment; however, these ratings increased again in the latter
half of follow-up.
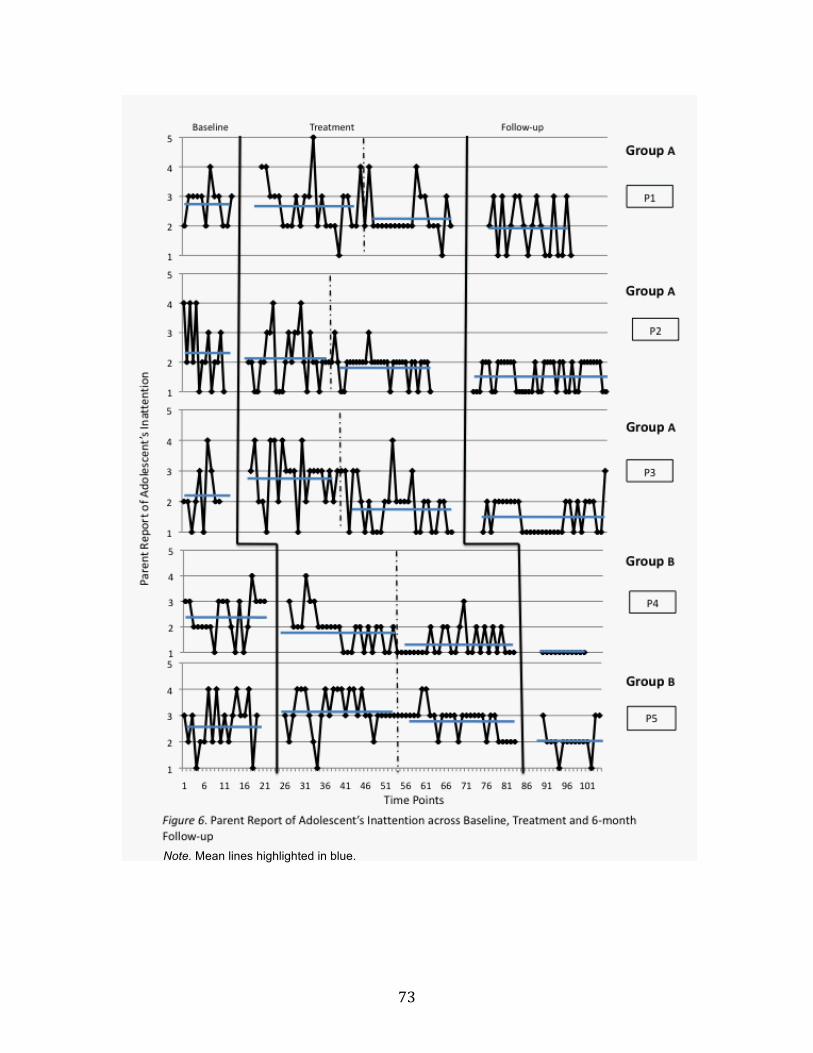
73
Note. Mean lines highlighted in blue.

74
Note. Mean lines highlighted in blue.
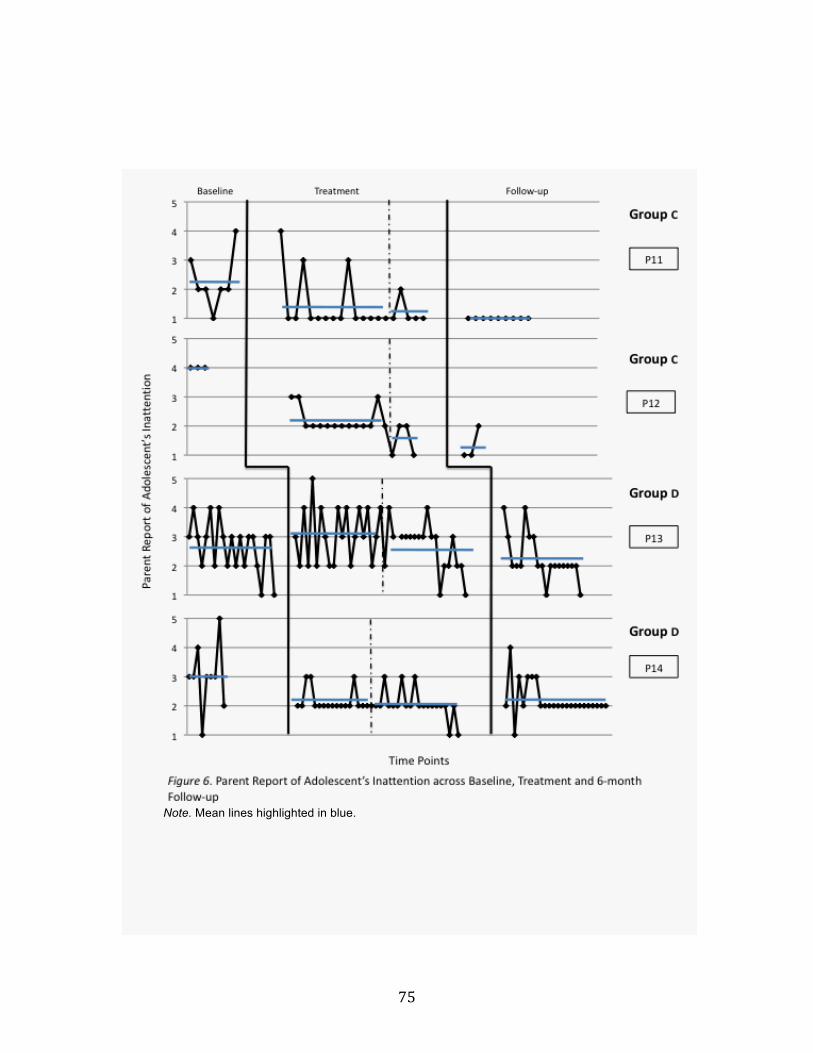
75
Note. Mean lines highlighted in blue.

76
3.3.2 Adolescent self-report of inattention. Visual analysis of data trends and
mean levels in Figure 7 suggests that participating in MYmind positively affected a
subsample of adolescents’ self-reported inattention levels, with only four adolescents
indicating reductions (44%). Similar to parent ratings, adolescent data were characterized
by a high degree of variability within and between participants. In contrast to parent
ratings, however, more than half of the adolescents (5) showed no downward trends in
their reports of inattention symptoms from baseline to treatment (A1, A3, A5, A6, A7), as
evidenced by the large number of overlapping data points across phases. Of the four
adolescents who reported positive change, three adolescents reported small improvements
(A2, A4, A8), and one adolescent reported a medium improvement (A9).
Two of these four adolescents reported treatment improvements that were
maintained in follow-up (A2, A9), one adolescent reported a late treatment improvement
(A4), and one adolescent reported an improvement in treatment that was not maintained
(A8). Although data from A4 and A8 reveal reduced inattention levels after participating
in MYmind, A8’s ratings increased at the start of follow-up and remained high
throughout, whereas A4’s data was low at the start of follow-up, but increased in the last
couple of months. These late peaks in data suggest that both adolescents struggled to
maintain the effects of treatment.

77
Note. Mean lines highlighted in blue.
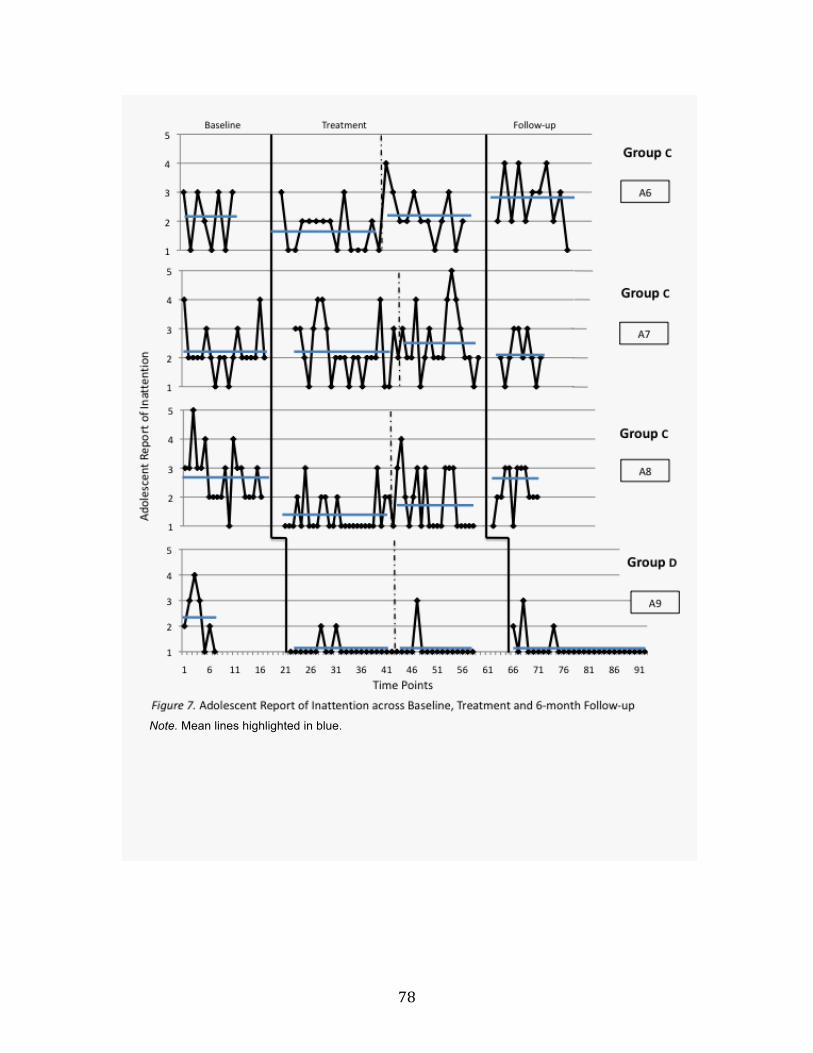
78
Note. Mean lines highlighted in blue.

79
3.4 Adolescent Hyperactivity
3.4.1 Parent report of hyperactivity in adolescents. Given that one parent
completed two of these items each day because of her two adolescent participants, 14
instead of 13 parent reports are included in the analysis of adolescent hyperactivity.
Visual analysis of data trends and mean levels in Figure 8 suggests that completing the
MYmind treatment had a reductive effect on most of the adolescents’ hyperactivity
symptoms, according to parent reports. Specifically, 10 of 14 parents (71%) reported
decreased levels of their adolescents’ hyperactivity by follow-up. One parent reported a
large improvement following treatment (P12), three parents indicated medium
improvements (P4, P11, P14), six parents reported small improvements (P1, P2, P3, P5,
P6, P8), and four parents reported that their adolescents’ hyperactivity symptoms did not
improve (P7, P9, P10, P13). Similar to their inattention ratings, P9 and P10 rated their
adolescent as “Not very” hyperactive throughout most of baseline and, thus, showed no
potential for positive change. Of the 12 parents whose adolescents had potential for
improvement, 10 parents (83%) reported a decrease in hyperactivity.
Six of these 10 parents reported treatment improvements that were maintained in
follow-up (P2, P3, P4, P11, P12, P14), three reported a late treatment improvement (P1,
P5, P6), and one reported improvements that were not maintained in follow-up (P6).
Although data by mid-treatment and/or follow-up showed less variability at generally low
frequencies for most parents, two of the parents’ reports were characterized by more
inconsistency. For example, P6’s data revealed a downward trend in treatment until the
final few weeks, where ratings increased. However, despite this peak in data at the end of
treatment, the mean level of data in the second half of treatment was still considerably

80
lower in comparison to baseline levels. P14 reported an increase in adolescent
hyperactivity at the start of follow-up in comparison to treatment, but these levels
decreased and stabilized for the latter half of follow-up.

81
Note. Mean lines highlighted in blue.

82
Note. Mean lines highlighted in blue.

83
Note. Mean lines highlighted in blue.

84
3.4.2 Adolescent self-report of hyperactivity. Visual analysis of data trends and
mean levels in Figure 9 suggests that completing MYmind positively affected only a
subsample of adolescents’ self-reported hyperactivity symptoms. Out of nine adolescents,
four (44%) reported reduced hyperactivity levels from participating in MYmind. Two
reported medium improvements (A4, A8), and another two indicated small improvements
(A2, A9). Five adolescents reported no change in hyperactivity symptoms (A1, A3, A5,
A6, A7). Data for these latter five adolescents are characterized by a high degree of
variability and somewhat high frequencies across phases.
Of the four adolescents who revealed downward trends in hyperactivity, two of
them reported treatment improvements that were maintained in follow-up (A2, A9), one
adolescent indicated a late treatment improvement (A4), and one adolescent reported a
positive change in treatment that was not maintained in follow-up (A8). Similar to her
reports of inattention, however, A4’s pattern of responses for hyperactivity exhibited a
high level of variability. For example, her follow-up data are, on average, much lower
than her baseline and treatment data, but the upward trend in mid-follow-up suggests that
she struggled to maintain the reduction in hyperactivity symptoms.
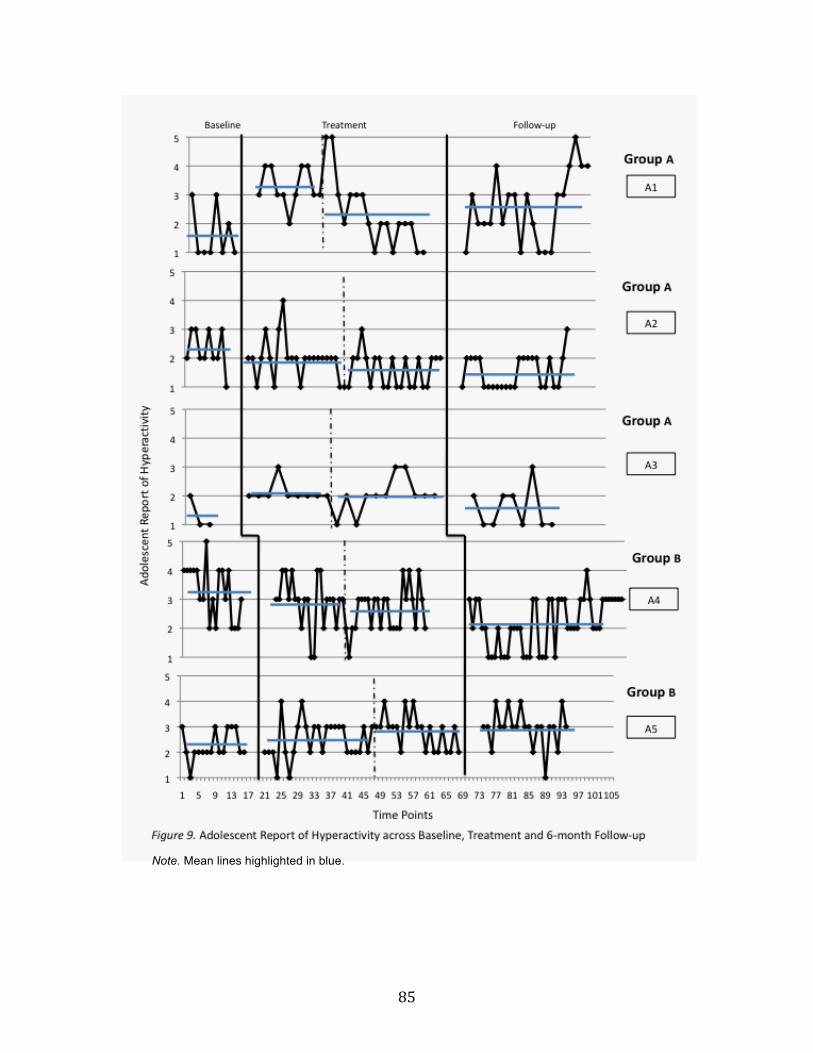
85
Note. Mean lines highlighted in blue.

86
Note. Mean lines highlighted in blue.

87
3.5 Adolescent Impulsivity.
3.5.1 Parent report of impulsivity in adolescents. Given that one parent
completed two of these items each day because of her two adolescent participants, 14
instead of 13 parent reports are included in the analysis of adolescent impulsivity.
Visual analysis of data trends and mean levels in Figure 10 denotes that participation in
the MYmind treatment had a positive impact on parent-reported adolescent impulsivity,
according to nine of the 14 parents (64%). Of these parents, one indicated a large
treatment improvement (P12), two reported medium treatment improvements (P4, P11),
and six indicated small treatment improvements (P1, P2, P3, P5, P6, P14). Five parents
reported that their adolescents’ impulsivity symptoms did not improve at all (P7, P8, P9,
P10, P13). Comparable to inattention and hyperactivity reports, the baseline ratings of P9
and P10 were predominantly in the “Not very” range and therefore, showed no potential
for improvement. Thus, of the 12 parents whose adolescents did have potential to
improve, nine parents (75%) reported reduced levels of impulsivity in their adolescents.
Analysis of participant profiles suggest that of the nine parents who reported a
decrease in adolescent impulsivity, six parents reported treatment improvements that
were maintained in follow-up (P2, P4, P6, P11, P12, P14), and three parents reported a
late treatment improvement (P1, P3, P5). In follow-up, all nine of these parents reported
consistently lower levels of adolescent impulsivity compared to baseline and the start of
treatment.

88
Note. Mean lines highlighted in blue.

89
Note. Mean lines highlighted in blue.

90
Note. Mean lines highlighted in blue.

91
3.5.2 Adolescent self-report of impulsivity. Visual analysis of data trends and
mean levels in Figure 11 illustrates that participating in MYmind had a minimal impact
on adolescents’ self-reported impulsivity symptoms. Of the nine adolescents who
completed MYmind, only three reported reductions in impulsivity levels (33%) and all
three of these showed only small treatment improvements (A3, A4, A8). Data from the
other six adolescents suggested no improvements (A1, A2, A5, A6, A7, A9).
Of the three adolescents who reported reductions in impulsivity, two of them
reported late treatment improvements (A3, A4), and one adolescent reported a positive
change in treatment that was not maintained in follow-up (A8). Similar to her
hyperactivity ratings, data of A4 is much lower in follow-up than in baseline and
treatment, however, there is an upward data trend in mid-follow-up.

92
Note. Mean lines highlighted in blue.

93
Note. Mean lines highlighted in blue.

94
3.6 Meditation Practice
3.6.1 Parent self-report of meditation practice. Visual analysis of data trends
and mean levels in Figure 12 suggests that participation in the MYmind treatment had a
prominent effect on parent-reported meditation practice. Patterns from 12 of 13 (92%)
parents revealed substantial increases in meditation practice in treatment compared to
baseline. However, a few parents had difficulty maintaining regular meditation practice
in follow-up.
Although P1, P6, P11 and P12 reported practicing some meditation before
MYmind was initiated, their baseline practice was inconsistent and/or for short durations,
with the exception of P12. By mid treatment, almost all parents reported increases in both
frequency and duration of meditation practice. Of the 13 parent participants, five parents
indicated large increases (P1, P4, P7, P10, P13), six parents reported medium increases
(P2, P3, P5, P9, P12, P14), one parent revealed a small increase (P6), and one parent
reported that their meditation practice decreased after MYmind (P11). The majority of
parents reported meditating almost every day, and some days for 20 minutes or more by
the end of treatment.
Further analysis revealed that of the 12 parents who reported increased meditation
practice, 10 parents reported increases that were maintained in follow-up (P1, P2, P3, P4,
P5, P7, P8, P9, P12, P13, P14), and two parents reported an increase that was not
maintained in follow-up (P6, P10). Some parents’ meditation practice persisted at the
start of follow-up, but tapered off after a few months (P5, P9, P14). Nonetheless, for the
majority of parents, meditation practice continued after treatment completion, albeit in
some cases for shorter durations.

95
Note. Mean lines highlighted in blue.
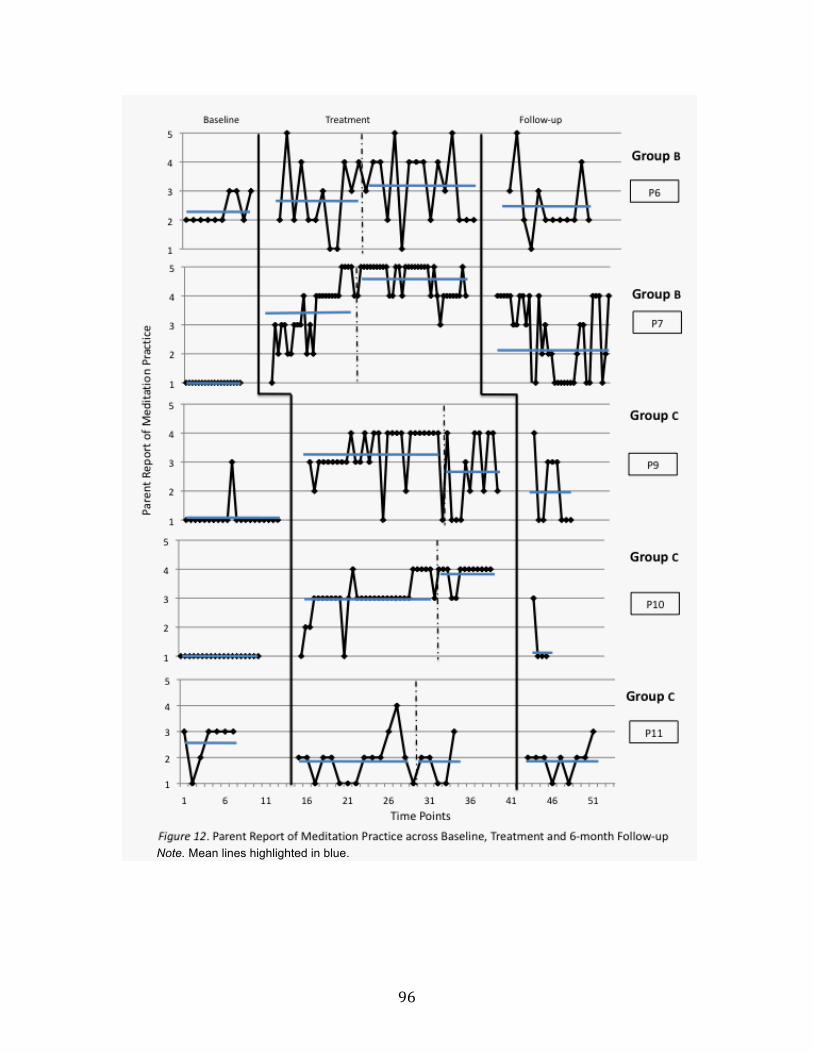
96
Note. Mean lines highlighted in blue.

97
Note. Mean lines highlighted in blue.

98
3.6.2 Adolescent self-report of meditation practice. Visual analysis of data
trends in Figure 13 indicates that participating in the MYmind treatment had a positive
impact on adolescent-reported meditation practice. In comparison to baseline, eight of the
nine adolescents (89%) reported considerable increases in their meditation practice by
treatment completion. One adolescent reported a large increase in meditation practice
(A9), six adolescents indicated medium increases (A1, A2, A3, A4, A5, A6), one
adolescent reported a small increase (A7) and one adolescent reported no increases (A8).
By the end of treatment, almost all adolescents were reporting more days meditating than
not meditating, and A2, A3, A4, A5 and A6 reported practicing meditation every day
consistently for at least two weeks.
Of the eight adolescents who reported improved meditation practice, six of them
reported treatment increases that were maintained in follow-up (A1, A2, A4, A5, A7, A9),
and two adolescents reported an increase in treatment that was not maintained in follow-
up (A3, A6). Although most adolescents’ follow-up meditation practice was more
variable and irregular than in treatment, levels were still higher than in baseline for
almost all adolescents.

99
Note. Mean lines highlighted in blue.

100
Note. Mean lines highlighted in blue.
101
3.7 Relationship Between Stress and Meditation Practice
Although visual analysis of meditation trends indicated that meditation practice
increased over treatment and follow-up for the majority of participants, a statistical
analysis of meditation practice was conducted on these data so that we could
subsequently correlate meditation practice with stress levels.
To statistically explore whether the amount of meditation practice significantly
varied across the three phases, GEE analysis with meditation practice as the dependent
variable and phase as a factor predictor variable was conducted. Results from GEE
analyses are interpreted similarly to results from ordinary least squares regression
(multiple linear regression). However, Wald χ2 tests are used instead of t and F tests, and
a measure of association (i.e., R2) is not available. Gamma distribution and a log link
function were selected for this analysis and the results indicated a significant difference
in the amount of meditation practice among the three phases, Wald χ2 (2)=103.72, p < .05.
Pairwise comparisons indicate that the average amount of meditation practice in Phase 1
(Baseline) is significantly smaller than in Phase 2 (Treatment) (MD = -1.43, SE = 0.16)
and in Phase 3 (Follow-up) (MD = -1.38, SE = 0.18). The amount of meditation practice
in Phases 2 and 3 are not significantly different. These results suggest that participants
continued their meditation practice six months after completing treatment.
A subsequent analysis examining predictors of participant stress was conducted
using the GEE procedure, with a gamma distribution and a log function. To fully explore
the relationship between meditation practice and stress, all possible interactions and
factors were included in the model. Specifically, to investigate whether adolescents or
parents benefited more from the meditation practice, interaction terms between group

102
status and other covariates were added to the model. Given that the data collected in the
current study was time-dependent (i.e., participants responded differently based on the
amount of time spent in treatment), within subject responses are likely to be correlated. A
failure to incorporate within-subject correlations into the analytic model leads to incorrect
coefficients and standard errors (Ballinger, 2004). Thus, time was included as a covariate
in the model. Additionally, phase was included in the model in order to determine
whether the relationship between meditation practice and stress varied according to phase
in the program (i.e., baseline, treatment, follow-up). Using backwards elimination, the
least significant interaction term was dropped and the model re-estimated, a procedure,
which continued until no more interaction terms could be eliminated.
Early results revealed no significant interaction effects across all variables, and no
main effects for adolescent/parent status, or phase (see Table G1 in Appendix G). These
findings indicated that the relationship between stress and meditation practice did not
differ between adolescents and parents, and therefore adolescent/parent status was
excluded as a covariate from further analysis. In the subsequent model, no significant
interactions or main effects were found for phase, suggesting that the effects of
meditation practice on stress levels did not vary across phases of treatment (see Table G2
in Appendix G). Results of the final model demonstrated a significant main effect for
meditation practice (Exp(B) = .96, p < .01), whereby 1 point in meditation practice on the
likert scale decreases stress by 4% (see Table 5). In general, findings from the GEE
analysis suggest that the more participants meditated the less stress they experienced and
this significant relationship did not vary across time, participant status or phase.

103
Note. OR = odds ratio. *p < .01, **p < .001. a Compared to Follow-up.
3.8 Consumer Satisfaction
Based on responses to items on the CSQ, both parents and adolescents reported
high levels of treatment satisfaction. Means and standard deviations for each item are
presented in Table 4. The mean satisfaction score across all areas of satisfaction was 4.39
(out of 5) for adolescents and 4.33 (out of 5) for parents. Overall, group leaders were
viewed highly by both groups of participants. Data suggests that participants felt group
leaders listened to and understood their concerns, and implemented the program
effectively. The lowest mean ratings by parents were for the question: ‘To what degree
has the MYmind program helped to improve your adolescent’s ADHD symptoms
overall?’ The lowest mean ratings by adolescents were for the item: ‘To what extent has
the MYmind program met your needs?‘ Under the “General Comments” section, 10 of 13
Table 3
GEE Analyses: Examining the Relationship Between Stress and Meditation
Practice, Main Effects Only.
Type of Predictor B SE Wald χ2 OR
Intercept .78 .07 126.01** 2.17
Baselinea .24 .05 19.61** 1.27
Treatmenta .23 .04 43.32** 1.26
Meditation Practice -.04 .02 8.17* .96
Time -.00 .00 1.86 .99

104
parents and seven of nine adolescents reported an improved relationship with their family
and/or an overall reduction in stress within the home. Seven parents also reported greater
awareness of themselves and their children, while eight of nine adolescents reported that
the effects generalized to their academic, artistic or athletic performance.

105
Table 4
Adolescent and Parent Satisfaction with the MYmind Program
Adolescents Parents
(n = 9) (n = 13)
Item M SD M SD
Participants’ satisfaction with help received 4.44 0.53 4.69 0.48
The extent MYMIND improved participants' ability to
deal with problems
4.33 0.71 4.31 0.75
Appropriateness of MYmind for treating participants’
ADHD symptoms and family conflict
4.67 0.50 4.77 0.44
The extent that MYmind met participant's needs 3.89 0.33 4.08 0.64
The extent the participants would recommend
MYmind to others
4.33 0.50 4.69 0.48
Participants' confidence in ability to manage future
conflicts
4.22 0.44 4.04 0.52
Amount of change experienced by participants across
areas of difficulty due to participation in MYmind
Adolescents’ ADHD symptoms 4.11 0.60 3.46 0.66
Participants’ ability to manage stress 4.44 0.53 4.08 0.64
Parent-adolescent relationship 4.33 0.50 4.19 0.75
Other personal problems 4.22 0.67 4.00 0.58

106
Chapter 4: Discussion
The present research involved an evaluation of a mindfulness-based training
program for adolescents with ADHD, and their parents. There is growing evidence
supporting mindfulness-based interventions as effective for a wide range of physical and
mental health disorders in a range of populations (e.g., Baer, 2003). The current study
contributed to the existing body of research by demonstrating the value of mindfulness
for families struggling with increased conflict and stress due to the additional challenges
experienced by youth with ADHD and their parents. Results from this multiple baseline
evaluation indicated that participating in the MYmind program were associated with
specific improvements for both parents and adolescents. Visual analyses of parent- and
adolescent-reported data revealed reductions in parent and adolescent stress, parent and
adolescent distress due to family conflict, and greater meditation practice. Most parents
reported a decrease in their adolescents’ inattention, hyperactivity and impulsivity
Parents ratings of MYmind for their adolescents 4.39 0.51
Parent ratings of themselves as parents after MYmind 4.08 0.49
Group Leader Abilities
Listening to participants’ concerns 4.67 0.50 4.69 0.48
Understanding participants’ concerns 4.67 0.50 4.69 0.48
Understanding adolescents’ concerns (according to
parent)
4.72 0.47
Implementing the MYmind program 4.78 0.44 4.85 0.37
Overall Mean 4.39 0.26 4.33 0.40
107
symptoms after participating in MYmind, however, results were less consistent across
adolescent responses. The majority of adolescents indicated no improvements in their
ADHD symptomology in treatment and follow-up compared to baseline. However, both
groups reported high satisfaction with the MYmind program overall.
Compared to behavioural and psychosocial programs, which have predominantly
not been found highly effective for youth with ADHD and their families (MTA
Cooperative Group, 2004a), the present study provides empirical support for mindfulness
as a promising treatment for this population. Mindfulness is a self-regulatory skill
involving observation of one’s own thoughts and feelings without judgment (Brown &
Ryan, 2003), and appears to help adolescents with ADHD who have deficits with
executive functioning (Oberle, Schonert-Reichl Lawlor, & Thomson, 2012). For example,
due to difficulties with modulating emotions and inhibiting behaviours in these
adolescents (Nigg, 2001), behavioural programs rooted in token economies and
reinforcement may not adequately address such neurological deficits. However,
cultivating mindful attention may be associated with improved executive functioning
because it requires an individual to regulate the focus of attention while inhibiting the
urge to act on thoughts and feelings that naturally arise in consciousness (Bishop et al.,
2004). Thus, adolescents become more attuned to their emotions and cognitions, allowing
them to disengage from impulsive reactions and adopt a more adaptive response to
managing their stress, interactions and inattention (Brown & Ryan, 2003). Likewise,
although most behavioural parent training approaches teach parents to modify their
reactions to the aberrant behaviour of their ADHD children through reinforcement and
problem-solving techniques (e.g., Abikoff et al., 2004), they do not improve parent
108
awareness of their automatic responses to emotional triggers or help them gain insight
and empathy about the behaviour of their adolescent offspring. Thus, due to these unique
mechanisms of action, mindfulness may have the potential as a more effective treatment
for addressing the difficulties of adolescents with ADHD and their parents than more
commonly prescribed behavioral and psychosocial interventions.
4.1 Reported Stress Outcomes
To evaluate the efficacy of participating in MYmind on parent and adolescent
stress levels, all participants were asked to rate their daily experiences of stress over
baseline, treatment and follow-up. Visual analyses of data trends and means suggest that
compared to baseline, stress levels for 85% of parents and 89% of adolescents were
greatly reduced by treatment completion. These low levels of stress remained fairly stable
across follow-up for the majority of both groups, although some adolescents’ ratings
peaked when school began in September.
4.1.1 Parent stress. Most parents reported fairly high and inconsistent levels of
stress in baseline, which is not surprising given past research suggesting a relationship
between stress and parenting youth with ADHD (Biondic, 2011; Theule et al., 2013).
Compared to baseline, parent reports of stress were notably lower by the end of MYmind
and in follow-up, which is similar to past findings on the effects of mindfulness-based
parenting programs with children (e.g., Benn et al., 2012). However, the present findings
extend the results of these studies by demonstrating these effects with parents of
adolescents, who may be associated with even more stressors than children (Shek, 1998).
It appears that, as parents in the present research practiced mindfulness, they (1)
became more aware and reflective of their automatic responses to common emotional

109
triggers before they arose, and (2) learned how to disengage and calm down more quickly
from difficult interactions, allowing them to more effectively cope with their stress (e.g.,
Duncan et al., 2009; Singh et al., 2010). For example, in MYmind parents were taught
that physiological stress reactivity can have physical signs (e.g., an increasingly rapid
heart rate), and if they attempt to observe those signs, they can use meditative practices to
alleviate their heightened emotions before responding (Benn et al., 2012).
Of the 11 parents who reported improvements in their stress levels, 10 indicated
that they were able to continue to effectively cope with their stress six months after
MYmind ended. Considering many stress management programs for parents of youth
with ADHD are ineffective in reducing child-related parenting stress, especially long-
term (e.g., Treacy et al., 2005), the maintenance of stress-related treatment effects in the
present study is encouraging. Considering that parenting stress is associated with high
attrition rates and poor use of strategies following treatment (Friars & Mellow, 2007;
Kazdin, Mazurick, & Bass, 1993), the low levels of stress likely contributed to parents’
efforts to fully participate in treatment and to continually practice mindfulness strategies
over time (Lanier et al., 2011).
4.1.2 Adolescent stress. Similar to parent stress reports in baseline, adolescent
stress ratings were fairly high and variable. Given the academic and social deficits
associated with ADHD adolescents, high stress reports were anticipated (Frazier et al.,
2007; Kawabata et al., 2012). In comparison to baseline, eight of the nine adolescents
reported experiencing less stress by the end of treatment and/or in follow-up. The present
findings are the first to identify the potential value of using mindfulness to reduce stress
in adolescents with ADHD. Mindfulness may be particularly appropriate for these

110
adolescents with poor emotion regulation because it cultivates a more adaptive appraisal
of the cognitions and emotions that trigger stress, allowing adolescents to make use of
more effective coping methods (Zylowska et al., 2008).
Unlike the consistent downward trend observed in parent stress ratings, some
adolescents reported an increase in stress levels during follow-up when school resumed in
September (at the start of follow-up for Groups 3 and 4; halfway through follow-up for
Groups 1 and 2). Although the MYmind curriculum included strategies intended to help
adolescents with school-related challenges as a result of their ADHD (e.g., how to focus
their attention, how to manage their workload, etc.), the simultaneous increase in stress
across adolescents in September suggests that MYmind may not have been sufficiently
effective in preparing them for the transition back to school. Considering that social
support plays an important role in helping adolescents cope with stress (Licitra-Kleckler
& Waas, 1993), such assistance may have been sufficient in the home as a result of parent
participation in MYmind. However, with no teacher involvement in the program, school
supports may have been inadequate to assist adolescents in effective management of
associated stressors.
4.2 Reported Distress due to Family Conflict Outcomes
Due to the lack of research in this area, we examined the impact of MYmind on
parent-adolescent interactions. All participants were asked to rate their level of distress as
a result of conflicts or interactions with their parent/adolescent everyday over baseline,
treatment and follow-up. Visual analysis of data and means indicated that there was a
downward trend in reports of distress from family conflict in 100% of parent reports

111
(among those with real potential for change) and 78% of adolescent reports after
treatment completion and/or in follow-up. These reduced distress ratings in follow-up,
suggest that mindfulness may be an effective treatment for targeting parent-adolescent
interactions.
4.2.1 Parent distress due to parent-adolescent conflict. Distress ratings in
baseline were not as high as one might expect considering the high levels of conflict
experienced by families of youth with ADHD (e.g., Babinski et al., 2011). In fact,
baseline levels of distress from four parents were so low (below a distress mean level of
1.9) that they had almost no potential to improve. In contrast to past research, these
parents may indeed feel that their interactions with their youth are not distressing. One
alternative hypothesis for these low reported levels of distress is that parents of
adolescents with ADHD may use an avoidance coping strategy (e.g., Goldstein et al.,
2007), and thus, avoid interactions with their adolescents rather than making an effort to
deal with their problem behaviour. Alternatively, since many of the MYmind parents
reported experiencing ADHD symptoms themselves, including disorganization, they may
have higher thresholds for disorganization in their adolescents, are poorer at monitoring
adolescent behaviour and are less consistent disciplinarians (Weinstein, Apfel, &
Weinstein 1998; Murray & Johnston, 2006).
In comparison to baseline, more than half of the parents’ reports of distress
increased during the initial weeks of treatment. Considering the weekly attendance and
regular home practice required to participate in MYmind, the additional responsibility
and commitment expected of adolescents may have provided further issues about which
parents and adolescents argued. For example, anecdotal comments from some MYmind
112
parents at the onset of treatment suggested that they struggled to persuade their
adolescents to attend the sessions, as well as to meditate at home. The majority of parents
were very motivated to seek help for their adolescents in MYmind, which may have
conflicted with adolescent disinterest in full participation (e.g., Bussing et al., 2012).
This upward trend in early treatment may also be due to parents’ enhanced
awareness of their emotions and thoughts during conflicts as a result of participating in
MYmind. For example, in MYmind sessions 2 and 3, parents were asked to keep a log of
their unpleasant events, pleasant events, and stressful situations with their youth as part of
home practice. Parents likely became more alert to difficult situations early in treatment
and more attuned to the distress they experienced as a result of them. In fact, the elevated
distress may be perceived as a treatment effect because enhanced ability to self-monitor
thoughts and emotions is a large part of mindfulness practice (Kabat-Zinn, 1990).
In the second half of treatment and/or follow-up, parents’ reports of distress due
to family conflict were considerably lower compared to baseline and the onset of
treatment, suggesting that intervention had a reductive effect on family conflict. Given
the correlation between high parenting stress and over-reactive parent disciplinary
practices (Theule et al., 2013), these lower conflict-related distress levels were likely
affected by parents’ reduced stress, and visa versa. For example, less stress may have
enhanced parents’ ability to adopt a more patient, empathic parenting style, which in turn
led to improved parent-adolescent relationships, reduced conflict and stress. Moreover,
MYmind also likely increased parents’ tolerance of negative emotions and enhanced their
ability to let go of the expectations and attributions that were often the root of conflicts
(Duncan et al., 2009). The enduring effects of MYmind in follow-up suggest that parents

113
were able to maintain their positive parent-adolescent interactions long-term, and
continued to respond to disputes with empathy, compassion and acceptance.
4.2.2 Adolescent distress due to parent-adolescent conflict. Compared to
baseline levels that were characterized by variability, adolescent conflict-related distress
showed a downward trend during intervention with lower, more stable levels by
treatment completion and/or follow-up. These reduced levels of conflict-related distress
after MYmind may have been due to adolescents’ greater self-awareness and regulation
of emotions following mindfulness practices (Tang et al., 2007). As a result of MYmind,
adolescents with ADHD may have become more effective at empathically resolving
conflict rather than impulsively reacting to social stressors related to interactions with
parents.
Adolescents’ reduced levels of conflict-related distress were also likely affected
by their parents’ reduced distress levels, as well as reports of lower stress levels by both
parties. By cultivating mindfulness, both parents and adolescents may have become more
self-aware and better able to disengage from the cognitive and emotional events that
fueled impulsive reactions (Dumas, 2005). Through alleviation of the distress associated
with their interactions, parents and adolescents may have had more positive experiences
with one another, facilitating an improved relationship (Johnston & Jassey, 2007).
Moreover, parents’ modeling of mindful emotion regulation is directly related to
children’s emotion regulation (Valients, Lemer-Chafabt, & Reiser, 2007); when parents
in the present study demonstrated mindful behaviour in their interactions, they may have
promoted similar mindful responding in the adolescents.

114
4.3 Reported ADHD Symptomatology Outcomes in Adolescents
Adolescents and parents were asked to rate the adolescents’ experience of
inattention, hyperactivity and impulsivity everyday over baseline, treatment and follow-
up. Because similar patterns were observed across data for these three symptoms, they
will be discussed together. Visual analysis of trends and means revealed that
approximately 60-70% of parents reported a reduction in adolescent ADHD symptoms
after treatment, whereas only 30-40% of adolescents reported improvements. These
mixed results make it difficult to draw firm conclusions about the potential efficacy of
MYmind for ameliorating these behavioral challenges.
4.3.1 Parent report of ADHD symptoms in adolescents. Although variable, most
parent ratings of adolescent ADHD symptoms in baseline were not as consistently high
as expected. These low parent reports may reflect the age-dependent decline in primary
ADHD symptomology that children experience as they enter adolescence (Biederman,
Mick, & Faraone, 2000; Langberg et al., 2008). Moreover, the majority of adolescents
(78%) were on medication before and during treatment, which may have been effective in
moderating ADHD-related behaviours.
These low parent reports may also be associated with an avoidant coping style,
resulting in minimal interaction with their adolescent. If parents infrequently interact with
their adolescents, they are unlikely to observe their ADHD symptoms on a daily basis.
Moreover, parents in the current study anecdotally noted in treatment sessions that they
did not know until that point in time that certain problems (e.g., excessive talking,
jumping from subjects in a conversation, poor memory, etc.) were attributed to ADHD;
this lack of knowledge about ADHD symptomatology may have led to under-reporting of
115
such ADHD behaviours on the DSQ in baseline. Further, the DSQ included one general
question each for adolescent inattention, hyperactivity, and impulsivity, which may not
have been as valid as measures that ask parents about each symptom through multiple
more specific items. Thus, parents may have under-reported their adolescents’ ADHD
because all behaviours related to each symptom were not clearly addressed in the DSQ
questions.
Treatment data revealed that 60-70% of parents reported that their adolescents’
ADHD symptoms decreased after participating in MYmind and these effects were
maintained in follow-up. Three previous studies investigating the MYmind program
found significant reductions in parent-rated inattention and externalizing symptoms in
children and adolescents with ADHD and/or behaviour disorders (Bogels et al., 2010; van
de Weijer-Bergsma et al., 2011; van der Oord et al., 2012), however, their results were
mixed. For example, only fathers reported improvements in van de Weijer-Bergsma et al.
(2011), not mothers, and teacher reports in van der Oord et al. (2012) and van de Weijer-
Bergsma et al. (2011) indicated no improvement.
Of note, P9 and P10 reported almost exclusively that their adolescent exhibited no
ADHD-related behaviour from baseline to follow-up. These parents were husband and
wife, and similar to the low levels of symptomatology that appeared in their DSQ ratings,
their comments in treatment also revealed minimal stress or tribulation at home. However,
in later MYmind sessions both parents disclosed experiencing stress and family discord,
suggesting an initial desire to present favorably to the group that decreased once they felt
more comfortable in their group interactions. Despite increased comfort, both parents

116
continued to report no problems in follow-up. Given the likely bias present in their
responses across phases, it is difficult to draw any conclusions from their data.
4.3.2 Adolescent self-report of ADHD symptoms. Most adolescents felt that
MYmind did not effectively address their ADHD-related difficulties, as only about one
third reported reduced inattention, hyperactivity and impulsivity symptoms after
participating in MYmind. These stable reports of ADHD symptoms across phases are in
contrast to the reduced adolescent ratings of stress and family conflict. It appeared that
adolescents were more effective at applying mindfulness skills to their relationships than
to their executive functioning and impulsive behaviour. Moreover, due to their ADHD
many adolescent participants struggled to remain still during meditations/yoga and to
concentrate during discussions, making it more difficult for them to fully participate and
benefit from the mindfulness activities.
These results are consistent with the increase in self-reported externalizing
symptoms for adolescents with comorbid ADHD and LD following an intervention that
involved mindfulness combined with martial arts training (Haydicky et al., 2012). These
researchers suggested that the increase in symptoms may have been due to the enhanced
awareness and self-monitoring skills that adolescents gained from participating in the
mindfulness program. Similarly, the adolescents with ADHD in the study by van de
Weijer-Bergsma et al. (2011), reported no positive changes in ADHD symptoms after
completion of MYmind.
The above studies also found a discrepancy between parent and adolescent reports of
the adolescents’ ADHD symptomatology. Research suggests that parents are more valid
reporters of adolescents’ ADHD symptoms than self-report data (Hoza et al., 2004).
117
However, poor parent–adolescent agreement may not suggest unreliable or invalid
reporting, but rather differences between parent and adolescent perceptions of ADHD-
related symptoms (Rasmussen et al., 2002). Parents likely rate their adolescents’
symptoms based on readily observed behavioural patterns (i.e., externalizing behaviours),
whereas adolescents’ ratings are rooted in their internalized experiences, of which parents
may be less aware (Vance et al., 2002). A qualitative study suggested that adolescents
with ADHD perceived some of their difficulties as something ‘wrong with their mind’
that made them different from their peers (Kendall, Hatton, Beckett, & Leo, 2003).
Therefore, while parents in the present study may have reported improvements in their
adolescents’ hyperactive behaviours, adolescents may have continued to feel different
and to experience trouble thinking.
4.4 Reported Meditation Outcomes
To evaluate whether participating in MYmind improved meditation practice,
participants were asked to rate their time spent meditating across baseline, treatment and
follow-up. Visual analyses of treatment data suggest that compared to baseline,
approximately 90% of participants reported meditating more frequently and for longer
durations. In follow-up, the duration of meditation decreased for some parents and
adolescents. GEE analyses revealed that meditation practice was significantly correlated
with reduced stress levels for both groups.
4.4.1 Parent meditation practice. Most parents had no previous experience with
meditation prior to treatment and the few who did meditated inconsistently and mostly
for short durations. All parents except one reported significant improvements in their
118
meditation practice over the course of treatment. By mid treatment, most parents were
meditating almost every day, and some days for 20 min or longer.
These results were anticipated given the emphasis placed on meditation in
treatment and the gradually increasing durations of meditation recommended in weekly
home practice. In support of this recommendation, parents were provided with a range of
meditations to practice at home, given a CD containing guided meditations, prompted as
a group to brainstorm strategies to overcome barriers to their meditation practice, and
sent daily text messages reminding them to meditate.
After treatment was completed, some parents reported less frequent and shorter
meditation sessions. This finding is not surprising given that they were no longer
receiving the supports provided in treatment. However, the majority of parents were still
meditating more days than not over six months of follow-up, suggesting long-term
treatment effects. At the booster session six weeks after treatment, parents conveyed that
finding ways to embed meditation practice into their busy daily schedules was the largest
obstacle to continued meditation practice.
4.4.2 Adolescent meditation practice. Almost all adolescents reported no
meditation practice during baseline; the two who indicated that they meditated did so
infrequently and for short durations. Over treatment, all adolescents but one reported
improved meditation practice with increases in both frequency and duration. Given that
youth with ADHD often have difficulty remaining still and concentrating for long periods
of time, these positive results are promising. Similar to the parents, adolescents were
given CDs with guided meditations, sent daily text message reminders and were
encouraged to practice for a longer duration of time each week between sessions.

119
Additionally, the use of meditation among athletes and actors was also discussed with the
adolescents to increase their motivation to practice for all areas of their life. Therefore,
such improvements in meditation practice may also be due to the enhanced performances
in other activities that adolescents associated with their meditation practice. Specifically,
adolescents reported meditating before hockey, skateboarding or playing an instrument,
which indirectly improved their subsequent performance.
In follow-up, less than half of the adolescents reported meditating as frequently
and as long as they did during treatment. Nonetheless, almost all adolescents reported
improvements in meditation practice compared to baseline.
4.4.3 Relationship between meditation and stress. In the present study, we
sought to determine whether participants’ meditation practice predicted their stress levels.
Results indicated that longer durations of meditation practice were significantly
correlated with reductions in the stress experienced by adolescents and parents. These
findings extend previous studies demonstrating the impact of meditation on stress and
wellbeing (Baer et al., 2006; Speca et al., 2000). For example, a randomized clinical trial
of MBSR conducted with adolescent psychiatric outpatients demonstrated that meditation
practice was significantly correlated with reductions in a range of psychological
symptoms, including anxiety and depression (Biegel et al., 2009). The present study
contributes to emerging research emphasizing the importance of meditation practice in
mindfulness-based programs.
4.5 Limitations and Research Implications
There are several limitations to the present study that suggest implications for

120
future research. First, this investigation involved a sample of only thirteen parents and
nine adolescents. Given that the symptoms associated with ADHD vary significantly
across youth (Nigg & Casey, 2005), the present sample size may have limited
generalizability of the findings to the broader population of adolescents with ADHD and
their families. However, it is important to note that, although the sample was too small to
do a rigorous group comparison study, the current design allowed for a thorough
evaluation of MYmind on individual participants. In fact, this sample size is considered
large for time-series investigations, and provided the opportunity for examining the
process, long-term outcomes, and experiential effects of the MYmind program.
The sample size presented an additional limitation related to the fact that only two-
thirds of participants qualified as research and treatment “completers”, raising the
possibility of selection bias. Participants who met inclusion criteria regarding treatment
attendance, meditation practice and consistent DSQ completion may have differed in
significant ways from those who did not meet criteria, and therefore were not included in
the research.
Another concern with the current study involves the simultaneous conduction of
parent and adolescent treatment groups, making it difficult to determine the relative
contribution of each to the improvements demonstrated by participants. In fact, Singh et
al. (2010) conducted a study with families of children with ADHD and examined the
effects of parent mindfulness training alone and combined with child mindfulness
training. They found that providing mindfulness training to the children added
substantially to the improvements obtained through parent mindfulness training.
Although preliminary, the Singh et al. (2010) study suggested that intervention for both

121
parent and child is important for optimal treatment effects. Further research examining
the effects of independent treatment for parents and adolescents would help to determine
the relative contribution of each to the improvements achieved.
A fourth drawback of the present study was that no data regarding parent ADHD
symptomatology was collected. Given that many parents of children with ADHD have
similar diagnostic features, assessing parent ADHD symptomatology prior to the onset of
treatment and measuring the effect of MYmind on their symptoms throughout treatment
would have provided additional information on the effects of mindfulness. Future
research should include measures to collect diagnostic parent information, and evaluate
parent outcomes to investigate whether mindfulness interventions successfully target
ADHD in parents.
Fifth, the present study did not evaluate whether the treatment effects enhanced
relationships with untreated family members (i.e., no data was collected regarding
participant relationships with non-participant family members). Such data would provide
information on whether mindfulness training can positively affect interactions with
individuals who have not had similar training opportunities. In particular, given the
increased conflict found in sibling relationships of children with ADHD (Mikami &
Pfiffner, 2008), future studies should investigate whether the improved interactions
associated with MYmind generalized to the adolescents’ sibling relationships.
Sixth, meditation in the current study was measured via participant self-reports of
duration and frequency of meditation practices. However, time spent meditating and past
experience with meditation are inadequate alternatives for true competency with
meditation; it is the quality of meditation practice, not quantity, that produces improved

122
health-related outcomes (Caspi & Burleson, 2005). Other measurement methods, such as
physiological measures (including heart rate variability or skin conductance), may be the
most effective means of determining whether someone is meditating in a present and
mindful manner that is likely to produce positive change (Caspi & Burleson).
Seventh, for the current study, we developed the Daily Symptom Questionnaire
(DSQ) to collect data on participants. Given the absence of an assessment instrument that
suited our purposes, the DSQ provided the information we sought for evaluating our
specific hypotheses regarding MYmind. However, no data on the psychometric properties
of the DSQ were collected. Data on the validity and reliability of the DSQ would have
helped ensure the accuracy of the results obtained and should be collected in future
studies.
Eighth, parents and adolescents were asked to rate inattention, hyperactivity, and
impulsivity globally with one question per behavioural area. In contrast to most rating
scales that include ratings of several more specific behaviours using multiple items, we
relied on the measurement of the overall construct (e.g., inattention) to represent all
related behaviours (e.g., difficulty concentrating). Although the three general items used
allowed us to obtain daily ratings of each overall category of behaviors, they did not
address the diversity of specific behaviours that adolescents struggle with, potentially
reducing the validity of our measurement system. Although some research suggests that
single-item self-report measures of clinical symptom severity (e.g., depression) and
psychosocial functioning are significantly correlated with the total scores and individual
item scores of longer measures (e.g., Zimmerman et al., 2006), no such data exists for
measures of ADHD.
123
A final limitation of the current research involved the reliance on self-report data
for evaluating the effectiveness of the intervention. Although most time-series designs
include repeated live observations over time as the primary source of evaluative data (e.g.,
Ducharme & Drain, 2004), observations were not feasible in this study given the nature
of the sample and the constructs being considered. Self-report questionnaires are
generally deemed less reliable than observational data. Cassady (2001) discusses
numerous potential sources of bias that can be caused by self-report data, including a
selective memory, perception of time (confusing when an event actually occurred),
exaggeration, and misattribution (attributing positive events to an internal cause and
negative events to an external force). Self-report data may be even more of a concern
with ADHD adolescents who tend to overestimate their abilities and underestimate the
severity of their problems (Wiener et al., 2012). In addition, the desire to be seen as
socially acceptable may have biased self-report data with some participants in the current
study. For example, P9 and P10 almost exclusively reported that their adolescent
demonstrated no ADHD-related behaviour from baseline to follow-up. Due to possible
bias in their self-reports that was revealed anecdotally, it was difficult to draw
conclusions from their data.
One of the strongest arguments against using self-report data is that administering
questionnaires before and after (but not during) the intervention, as in pre-post designs,
requires participants to rely on their memory, thus reducing the accuracy of their reports
(Margetts, Vorster & Venterm, 2003). Research has shown that participants respond more
accurately to questions about their behaviour the shorter the elapsed time between the
report and the behaviour under consideration (Judd, Smith & Kidder, 1991; Whippie &

124
Richey, 1997). Thus, notwithstanding the use of self-report data in the present study, the
daily time-series measurement precluded participant reliance on memory that frequently
biases retrospective self-report data in pre-post designs. Moreover, pre-post designs
require participants to report at only one point in time after treatment, which is likely not
representative of their overall functioning across time (Lambert, Doucette & Bickamn,
2001). For example, a self-report can significantly vary depending on many variables
(e.g., time or day it is given, participant’s current mood, etc.), and thus a single report
may not be a valid outcome measure of general functioning after treatment. However,
multiple self-reports, such as in the current study, will provide a more comprehensive
picture of a participant’s behaviour over time without the potential influence of
extraneous variables (Lambert et al.).
4.6 Clinical Implications and Conclusions
Results from the current study demonstrate that mindfulness is an effective
approach for reducing stress and enhancing parent-adolescent interactions for adolescents
with ADHD and their parents. No studies to date have investigated the impact of
mindfulness on parent-adolescent interactions in families of youth with ADHD.
Moreover, similar to past studies (Bogels et al., 2010; Haydicky et al., 2012; van de
Weijer-Bergsma et al., 2011; van der Oord et al., 2012), the current investigation
demonstrated that mindfulness may have some potential for treating ADHD symptoms in
youth. However, results from adolescent reports were less encouraging than parent
reports. Previous research has highlighted the discrepancy frequently found between
parent and child/adolescent reports where youth self-report more symptoms than parents

125
(Grills & Ollendick, 2002; Van Roy, Groholt, Heyerdah, & Clench-Aas, 2010).
It is important to note that the majority of adolescents were also taking medication
while participating in the MYmind program. The discouraging reports from adolescents
may suggest that MYmind did not provide many additional improvements to their daily
ADHD symptoms beyond the effects of their medication. This explanation is particularly
relevant given the low reported rates of ADHD in baseline and evidence from past studies
indicating that medication is currently the most effective form of treatment for managing
ADHD symptoms (Biederman & Farone, 2005). However, although medication may also
have positive effects on the stress levels and negative parenting practices of parents
raising youth with ADHD (Wells et al., 2000), it does not provide parents or adolescents
with the skills, coping strategies or awareness required to change their automatic patterns
long-term. Moreover, youth are more likely to discontinue medication or use it
inconsistently during adolescence (Atzori et al., 2009). Consequently, mindfulness may
be an important and necessary adjunct treatment to medication for managing the range of
difficulties experienced by adolescents with ADHD and their parents.
In the current study, we asked participants to report on their experiences and
symptoms for six months following completion of MYmind. These follow-up data
provided evidence that the positive effects observed during treatment were maintained or
improved after treatment ended. Unlike many psychosocial interventions for ADHD that
result in inadequate maintenance of treatment effects (Abikoff, 2009), the results of the
current study suggest that mindfulness may produce specific long-term positive outcomes.
During each MYmind session, participants discussed potential solutions to the
obstacles they experienced during home practice, and a booster session was provided six
126
weeks after treatment. These supports likely contributed to the participants’ ability to
uphold their mindfulness practice after the weekly MYmind sessions finished. Moreover,
questionnaires were emailed throughout follow-up as a cue for reflection on daily
experiences. By reviewing events at the end of each day, participants may have
developed a habit of self-monitoring, a practice that enhances awareness of internal
experiences (Williams et al., 2007). Daily self-reflection may have allowed participants
to observe their automatic tendencies, facilitating their ability to respond differently to
stressful situations well after intervention was completed.
Notwithstanding the multiple enduring effects observed in the present study, many
adolescents reported elevated stress levels when school resumed in September. It appears
that the intervention did not adequately prepare adolescents for managing the added
stressors associated with beginning a new school year, a finding that is congruent with
previous MYmind studies (van de Weijer-Bergsma et al., 2011; van der Oord et al., 2012)
in which teachers reported no improvements following treatment. In the future, MYmind
should include activities focusing on the school-related stressors (e.g., starting a new
school, workload demands, exam time, etc.) and directly apply mindfulness practices to
the achievement-related self-regulation required of students (Mendelson et al., 2010).
The use of time-series self-report measurement to assess the effects of MYmind on
parent and adolescent behaviours was a unique feature of the present research. These
daily self-reports allowed us to observe changes across key constructs over time.
Mindfulness involves a gradual process of change through the development of greater
awareness and acceptance that is not captured with a pre-post design. Criticisms of
currently available pre-post measures of mindfulness suggest that self-assessment at one

127
time point does not grasp the full range of experiences associated with practicing
mindfulness (Grossman, 2008). As a result, it may be beneficial to shift our focus from
examining only discrete outcomes of mindfulness to the overall process across key areas
of well-being.
In summary, the long-term efficacy of MYmind for parent-adolescent conflict and
stress in families with ADHD will hopefully fill the need for treatments targeting the
additional difficulties experienced by this population. Moreover, the use of time-series
measurement provided a novel approach to measuring the effects of mindfulness
programs in a more efficient and comprehensive way. The present research adds to the
burgeoning field of mindfulness by demonstrating its associated positive effects with
adolescents with ADHD and their parents. Given the breadth of populations and
presenting problems for which mindfulness has been found effective, mindfulness-based
approaches have been established as the third wave of behavioural and cognitive
therapies, providing an alternative to the goal-oriented, behaviour-modification and
symptom-change focus of early behaviourism (Hayes, 2004). This clinical focus on
acceptance and awareness of difficult conditions that is the foundation of mindfulness
may be the ideal antidote for managing the rapidly changing times that are adding so
many new challenges to the lives of patients and their healthcare providers.

128
References
Abikoff, H. (2009). ADHD psychosocial treatments: Generalization reconsidered. Journal of Attention Disorders, 13(3), 207-210. doi: 10.1177/1087054709333385 Abikoff, H., Hechtman, L., Klein, R. G., Weiss, G., Fleiss, K., Etcovitch, J., . . .Pollack, S. (2004). Symptomatic improvement in children with ADHD treated with long-term methylphenidate and multimodal psychosocial treatment. Journal of the American Academy of Child & Adolescent Psychiatry, 43(7), 802-811. doi:10.1097/01.chi.0000128791.10014.a Anastopoulos, A. D., Shelton, T. L., DuPaul, G. J., & Guevremont, D. C. (1993). Parent training for attention-deficit hyperactivity disorder: Its impact on parent functioning. Journal of Abnormal Child Psychology, 21(5), 581-596. doi: http://dx.doi.org/10.1007/BF00916320 Anderson, C. A., Hinshaw, S. P., & Simmel, C. (1994). Mother-child interactions in ADHD and comparison boys: Relationships with overt and covert externalizing behavior. Journal of Abnormal Child Psychology, 22(2), 247-265. doi:10.1007/BF0216790 Anjum, N., & Malik, F. (2010). Parenting practices in mothers of children with ADHD: Role of stress and behavioral problems in children. Pakistan Journal of Social and Clinical Psychology, 8(1), 18-38. Retrieved from http://search.proquest.com/docview/915044703?accountid=14771 Astin, J. A. (1997). Stress reduction through mindfulness meditation: Effects on psychological symptomatology, sense of control, and spiritual experiences. Psychotherapy and Psychosomatics, 66(2), 97-106. doi:10.1159/000289116 Atzori, P., Usala, T., Carucci, S., Danjou, F., & Zuddas, A. (2009). Predictive factors for persistent use and compliance of immediate-release methylphenidate: A 36- month naturalistic study. Journal of Child and Adolescent Psychopharmacology, 19(6), 673-681. doi:10.1089/cap.2008.0146 Babinski, D. E., Pelham, W. E., Molina, B. S. G., Gnagy, E. M., Waschbusch, D. A., Yu, J., . . . Karch, K. M. (2011). Late adolescent and young adult outcomes of girls diagnosed with ADHD in childhood: An exploratory investigation. Journal of Attention Disorders, 15(3), 204-214. doi:10.1177/1087054710361586 Baer, R. A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science and Practice, 10(2), 125-143. Retrieved from http://search.proquest.com/docview/236411305?accountid=14771 Baer, R. A., Fischer, S., & Huss, D. B. (2006). Mindfulness and acceptance in the treatment of disordered eating. Journal of Rational-Emotive & Cognitive-Behavior

129
Therapy, 23(4), 281-299. doi: 10.1007/s10942-005-0015-9 Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self- report assessment methods to explore facets of mindfulness. Assessment, 13(1), 27- 45. doi: 10.1177/1073191105283504 Ballinger, G. A. (2004). Using generalized estimating equations for longitudinal data analysis. Organizational Research Methods, 7(2), 127-150. doi: 10.1177/1094428104263672 Banks, T., Ninowski, J. E., Mash, E. J., & Semple, D. L. (2008). Parenting behavior and cognitions in a community sample of mothers with and without symptoms of Attention-deficit/Hyperactivity Disorder. Journal of Child and Family Studies, 17, 28–43. doi:10.1007/s10826-007-9139-0 Barkley, R. A. (1990). Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford Press. Barkley, R. A. (1997). Attention-deficit/hyperactivity disorder, self-regulation, and time: Toward a more comprehensive theory. Journal of Developmental and Behavioral Pediatrics, 18(4), 271-279. Retrieved from http://search.proquest.com/docview/65244633?accountid=14771 Barkley, R. A. (2003). Issues in the diagnosis of attention-deficit/hyperactivity disorder in children. Brain & Development, 25(2), 77-83. doi: 10.1016/S0387- 7604(02)00152-3 Barkley, R. A., Anastopoulos, A. D., Guevremont, D. C., & Fletcher, K. E. (1992). Adolescents with attention deficit hyperactivity disorder: Mother−adolescent interactions, family beliefs and conflicts, and maternal psychopathology. Journal of Abnormal Child Psychology, 20(3), 263-288. Retrieved from http://search.proquest.com/docview/64997088?accountid=14771 Barkley, R. A., Edwards, G., Laneri, M., Fletcher, K., & Metevia, L. (2001). The efficacy of problem-solving communication training alone, behavior management training alone, and their combination for parent–adolescent conflict in teenagers with ADHD and ODD. Journal of Consulting and Clinical Psychology, 69(6), 926- 941. doi: 10.1037/0022-006X.69.6.926 Barkley, R. A. R., Fischer, M. M., Edelbrock, C. C., & Smallish, L. L. (1991). The adolescent outcome of hyperactive children diagnosed by research criteria--III. mother-child interactions, family conflicts and maternal psychopathology. Journal of Child Psychology and Psychiatry, 32(2), 233-255. Retrieved from http://search.proquest.com/docview/80566383?accountid=14771

130
Benn, R., Akiva, T., Arel, S., & Roeser, R. W. (2012). Mindfulness training effects for parents and educators of children with special needs. Developmental Psychology, doi:10.1037/a0027537 Biederman, J., Ball, S. W., Monuteaux, M. C., Mick, E., Spencer, T. J., McCreary, M., . . . Faraone, S. V. (2008). New insights into the comorbidity between ADHD and major depression in adolescent and young adult females. Journal of the American Academy of Child & Adolescent Psychiatry, 47(4), 426-434. doi:10.1097/CHI.0b013e31816429d3 Biederman, J. & Faraone, S. V. (2005). Attention-deficit hyperactivity disorder. Lancet, 366(9481), 237–248. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16023516 Biederman, J., Faraone, S. V., & Monuteaux, M. C. (2002). Impact of exposure to parental attention-deficit hyperactivity disorder on clinical features and dysfunction in the offspring. Psychological Medicine, 32(5), 817-827. doi: 10.1017/S0033291702005652 Biederman, J., Mick, E., Faraone, S. V., & Burback, M. (2001). Patterns of remission and symptom decline in conduct disorder: A four-year prospective study of an ADHD sample. Journal of the American Academy of Child and Adolescent Psychiatry, 40(3), 290-298. doi: 10.1097/00004583-200103000-00008 Biegel, G. M., Brown, K. W., Shapiro, S. L., & Schubert, C. M. (2009). Mindfulness- based stress reduction for the treatment of adolescent psychiatric outpatients: A randomized clinical trial. Journal of Consulting and Clinical Psychology, 77(5), 855– 866. doi:10.1037/a0016241 Biondic, D. (2011). Parenting Stress of Parents of Adolescents with Attention- deficit/Hyperactivity Disorder (Masters Thesis, University of Toronto). Retrieved from http://hdl.handle.net/1807/30075 Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., et al. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230-241. doi: 10.1093/clipsy.bph077 Blackledge, J. T. & Hayes, S. C. (2006). Using acceptance and commitment training in support of parents of children diagnosed with autism. Child & Family Behavior Therapy, 28(1), 1-18. Retrieved from http://search.proquest.com/docview/64567373?accountid=14771 Bogels, S., Hoogstad, B., van Dun, L., de Schutter, S., & Restifo, K. (2008). Mindfulness
training for adolescents with externalizing disorders and their parents. Behavioural and Cognitive Psychotherapy, 36(2), 193-209. Retrieved from http://search.proquest.com/docview/62022826?accountid=14771

131
Bowen, S., Witkiewitz, K., Dillworth, T. M., Chawla, N., Simpson, T. L., Ostafin, B. D., . . . Marlatt, G. A. (2006). Mindfulness meditation and substance use in an incarcerated population. Psychology of Addictive Behaviors, 20(3), 343-347. doi: 10.1037/0893-164X.20.3.343 Braaten, E. B., & Rosén, L. A. (2000). Self-regulation of affect in attention deficit- hyperactivity disorder (ADHD) and non-ADHD boys: Differences in empathic responding. Journal of Consulting and Clinical Psychology, 68(2), 313-321. doi: 10.1037/0022-006X.68.2.313 Britton, W. B., Bootzin, R. R., Cousins, J. C., Hasler, B. P., Peck, T. T., & Shapiro, S. L. (2010). The contribution of mindfulness practice to a multicomponent behavioral sleep intervention following substance abuse treatment in adolescents: A treatment-development study. Substance Abuse, 31(2), 86-97. Retrieved from http://search.proquest.com/docview/733531243?accountid=14771 Bromley Little, H. J. (1998). Parenting stress among parents of children with attention- deficit/hyperactivity disorder: The role of control and responsibility attributions. (Doctoral Dissertation). Retrieved from ProQuest Dissertations and Theses. (Order No. NQ30590). Brown, K. W., Ryan, R. M., & Creswell, J. D. (2007). Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18(4), 211-237. doi: 10.1080/10478400701598298 Burke, J. D., Pardini, D. A., & Loeber, R. (2008). Reciprocal relationships between parenting behavior and disruptive psychopathology from childhood through adolescence. Journal of Abnormal Child Psychology, 36(5), 679-692. doi:10.1007/s10802-008-9219-7 Bush, G., Valera, E. M., & Seidman, L. J. (2005). Functional neuroimaging of attention- deficit/hyperactivity disorder: A review and suggested future directions. Biological Psychiatry, 57(11), 1273-1278. doi:10.1016/j.biopsych.2005.01.034 Bussing, R., Koro-Ljungberg, M., Noguchi, K., Mason, D., Mayerson, G., & Garvan, C. W. (2012). Willingness to use ADHD treatments: A mixed methods study of perceptions by adolescents, parents, health professionals and teachers. Social Science & Medicine, 74(1), 92-100. doi:10.1016/j.socscimed.2011.10.009 Carmody, J. J., & Baer, R. A. R. A. (2008). Relationships between mindfulness practice
and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine, 31(1), 23-33. Retrieved from http://search.proquest.com/docview/70473124?accountid=14771

132
Caspi, O., & Burleson, K. O. (2005). Methodological challenges in meditation research. Advances in Mind-Body Medicine, 21(1), 4-11. Retrieved from http://search.proquest.com/docview/620798849?accountid=1477
Cassady, J. C. (2001). Self-reported gpa and sat: a methodological note. Practical Assessment, Research & Evaluation, 7(12). Retrieved July 3, 2012 from http://PAREonline.net/getvn.asp?v=7&n=12 Chronis, A. M., Lahey, B. B., Pelham, W. E., Kipp, H. L., Baumann, B. L., & Lee, S. S.
(2003). Psychopathology and substance abuse in parents of young children with attention-Deficit/Hyperactivity disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 42(12), 1424-1432. doi: 10.1097/00004583-200312000-00009
Chronis-Tuscano, A., Raggi, V.L., Clarke, T.L., Rooney , M.E. , Diaz, Y., & Pian, J.
(2008). Associations between maternal attention-deficit/hyperactivity disorder symptoms & parenting. Journal of Abnormal Child Psychology, 36(8), 1237-1250. doi: 10.1007/s10802-008-9246-4
Coatsworth, J. D, Duncan, L. G., Greenberg, M. T., & Nix, R. L. (2010). Changing parent’s mindfulness, child management skills and relationship quality with their youth: Results from a randomized pilot intervention trial. Journal of Child and Family Studies, 19(2), 203-217. doi: 10.1007/s10826-009-9304-8 Cohen, J. A. S., & Semple, R. J. (2010). Mindful parenting: A call for research. Journal of Child and Family Studies, 19(2), 145-151. doi:10.1007/s10826-009-9285-7 Conners, C. K. (2008). Conners-3rd Edition. Toronto, ON: Multi-Health Systems Inc. Connor, D. F. (2005). Psychostimulants in attention deficit hyperactivity disorder. In D., Gozal, D. L., Molfese (Eds.), Attention deficit hyperactivity disorder: from genes to patients (pp. 487–527). New Jersey: Humana Press. Creswell, J. D., Myers, H. F., Cole, S. W., & Irwin, M. R. (2009). Mindfulness meditation training effects on CD4+ T lymphocytes in HIV-1 infected adults: A small randomized controlled trial. Brain, Behavior, and Immunity, 23(2), 184-188. doi:10.1016/j.bbi.2008.07.004 Crundwell, R. M. A. (2005). An initial investigation of the impact of self-regulation and emotionality on behavior problems in children with ADHD. Canadian Journal of School Psychology, 20(1-2), 62-74. doi: 10.1177/0829573506295458 Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D., Santorelli, S. F., . . . Sheridan, J. F. (2003). Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic Medicine, 65(4), 564-570. doi:10.1097/01.PSY.0000077505.67574.E3

133
Dekovic, M. (1999). Parent-adolescent conflict: Possible determinants and consequences. International Journal of Behavioral Development, 23(4), 977-1000. doi: 10.1080/016502599383630 Desman, C., Petermann, F., & Hampel, P. (2008). Deficit in response inhibition in children with attention deficit/hyperactivity disorder (ADHD): Impact of motivation? Child Neuropsychology, 14(6), 483-503. doi: 10.1080/09297040701625831 Diggle, P. J., Heagerty, P. J., Liang, K., Zeger, S. L., & Rigby, A. S. (2003). Analysis of longitudinal data. Journal of the Royal Statistical Society, 52(2), 239-240. Retrieved from http://search.proquest.com/docview/38487308?accountid=1477 Douglas, V. I., & Parry, P. A. (1994). Effects of reward and nonreward on frustration and attention in attention deficit disorder. Journal of Abnormal Child Psychology, 22(3), 281-302. doi: 10.1007/BF02168075 Ducharme, J. M., Atkinson, L., & Poulton, L. (2001). Errorless complicance training with physically abusive mothers: A single-case approach. Child Abuse & Neglect, 25(6), 855-868. doi: 10.1016/S0145-2134(01)00243-5 Ducharme, J. M., & Drain, T. L. (2004). Errorless academic compliance training: Improving generalized cooperation with parental requests in children with autism. Journal of the American Academy of Child and Adolescent Psychiatry, 43(2), 163- 163. Retrieved from http://search.proquest.com/docview/62121244?accountid=14771 Dumas, J. E. (2005). Mindfulness-based parent training: Strategies to lessen the grip of automaticity in families with disruptive children. Journal of Clinical Child and Adolescent Psychology, 34(4), 779-791. doi: 10.1207/s15374424jccp3404_20 Duncan, L. G., Coatsworth, J. D., & Greenberg, M. T. (2009). A model of mindful parenting: Implications for parent–child relationships and prevention research. Clinical Child and Family Psychology Review, 12(3), 255–270. doi: 10.1007/s10567-009-0046-3 DuPaul, G. J., McGoey, K. E., Eckert, T. L., & Vanbrakle, J. (2001). Preschool children with attention-deficit/hyperactivity disorder: Impairments in behavioral, social, and school functioning. Journal of the American Academy of Child and Adolescent Psychiatry, 40, 508–515. doi:10.1097/00004583-200105000-00 DuPaul, G. J., Volpe, R. J., Jitendra, J., Lutz, G., Lorah, K. S., & Gruber, R. (2004). Elementary school students with ADHD: Predictors of academic achievement. Journal of School Psychology , 42, 285–301. doi: 10.1016/j.jsp.2004.05.001
134
Edwards, G. G., Barkley, R. A. R., Laneri, M. M., Fletcher, K. K., & Metevia, L. L. (2001). Parent-adolescent conflict in teenagers with ADHD and ODD. Journal of Abnormal Child Psychology, 29(6), 557-572. Retrieved from http://search.proquest.com/docview/72337718?accountid=14771 Eisenberg, N., Zhou, Q., Spinrad, T. L., Valiente, C., Fabes, R. A., & Liew, J. (2005). Relations among positive parenting, children's effortful control, and externalizing problems: A three-wave longitudinal study. Child Development, 76(5), 1055-1071. Retrieved from http://search.proquest.com/docview/57082098?accountid=14771 Ek, U., Westerlund, J., Holmberg, K., & Fernell, E. (2011). Academic performance of adolescents with ADHD and other behavioural and learning problems—A population‐based longitudinal study. Acta Paediatrica, 100(3), 402-406. doi:http://dx.doi.org/10.1111/j.1651-2227.2010.02048.x Ellis, B., & Nigg, J. (2009). Parenting practices and attention-deficit/hyperactivity disorder: New findings suggest partial specificity of effects. Journal of the American Academy of Child & Adolescent Psychiatry, 48(2), 146-154. doi:10.1097/CHI.0b013e31819176d0 Erk, R. R. (2000). Five frameworks for increasing understanding and effective treatment of attention-deficit/hyperactivity disorder: Predominately inattentive type. Journal of Counseling & Development, 78(4), 389-399. doi: 10.1002/j.1556- 6676.2000.tb01922. Evans, S., Ferrando, S., Findler, M., Stowell, C., Smart, C., & Haglin, D. (2008). Mindfulness-based cognitive therapy for generalized anxiety disorder. Journal of Anxiety Disorders, 22(4), 716-721. doi: 10.1016/j.janxdis.2007.07.005 Fabiano, G.A., Chacko, A., Pelham, W.E., Robb, J.A., Walker, K.S., Wienke, A.L., Arnold, F., Flammer, L., Keenan, J.K., Visweswaraiah, H., Shulman, S., Herbst, L., & Pirvics, L. (2009). A comparison of behavioral parent training programs for fathers of children with attention-deficit/hyperactivity disorder. Behavior Therapy, 40(2), 190-204. doi: 10.1016/j.beth.2008.05.002 Farmer, E. M. Z., Compton, S. N., Burns, B. J. & Robertson, E. (2002). Review of the evidence base for treatment of childhood psychopathology: externalizing disorders. Journal of Consulting and Clinical Psychology, 70(6), 1267-1302. doi: 10.1037//0022-006X.70.6.1267 Fletcher, K. E., Fischer, M., Barkley, R. A., & Smallish, L. (1996). A sequential analysis of the mother–adolescent interactions of ADHD, ADHD/ODD, and normal teenagers during neutral and conflict discussions. Journal of Abnormal Child Psychology, 24(3), 271-297. doi: 10.1007/BF01441632 Fletcher, J., & Wolfe, B. (2009). Long-term consequences of childhood ADHD on

135
criminal activities. Journal of Mental Health Policy and Economics, 12(3), 119- 138. Retrieved from http://search.proquest.com/docview/754032729?accountid=14771 Flook, L., Smalley, S. L., Kitil, M. J., Galla, B. M., Kaiser-Greenland, S., Locke, J., . . . Kasari, C. (2010). Effects of mindful awareness practices on executive functions in elementary school children. Journal of Applied School Psychology, 26(1), 70- 95. doi: 10.1080/15377900903379125 Flory, K., Molina, B. S. G., Pelham, W. E., Gnagy, E., & Smith, B. (2006). Childhood ADHD predicts risky sexual behavior in young adulthood. Journal of Clinical Child and Adolescent Psychology, 35(4), 571-577. doi: http://dx.doi.org/10.1207/s15374424jccp3504_8 Frazier, T. W., Youngstrom, E. A., Glutting, J. J., & Watkins, M. W. (2007). ADHD and achievement: Meta-analysis of the child, adolescent, and adult literature and a concomitant study with college students. Journal of Learning Disabilities, 40(1), 49–65. Retrieved from http://search.proquest.com.myaccess.library.utoronto.ca/psycinfo/docview/19422 3011/fulltextPDF/13867DA6D414EF9299C/1?accountid=14771 Friars, P. M., & Mellor, D. J. (2007). Drop out from behavioral management training programs for ADHD: A prospective study. Journal of Child and Family Studies, 16, 427–441. doi:10.1007/s10826-006-9096-z Friedman, S. R., Rapport, L. J., Lumley, M., Tzelepis, A., VanVoorhis, A., Stettner, L., . . . Kakaati, L. (2003). Aspects of social and emotional competence in adult attention-deficit/hyperactivity disorder. Neuropsychology, 17(1), 50-58. doi: 10.1037/0894-4105.17.1.50 Gerdes, A. C., Haack, L. M., & Schneider, B. W. (2012). Parental functioning in families of children with ADHD: Evidence for behavioral parent training and importance of clinically meaningful change. Journal of Attention Disorders, 16(2), 147-156. doi:10.1177/1087054710381482 Gerdes, A. C., Hoza, B., & Pelham, W. E. (2003). Attention-deficit/hyperactivity disordered boys' relationships with their mothers and fathers: Child, mother, and father perceptions. Development and Psychopathology, 15(2), 363-382. doi: 10.1017/S0954579403000208 Goldman, L. S., Genel, M., Bezman, R. J., & Slanetz, P. J. (1998). Diagnosis and treatment of attention-deficit/hyperactivity disorder in children and adolescents. JAMA: Journal of the American Medical Association, 279(14), 1100-1107. doi: 10.1001/jama.279.14.1100 Goldstein, E. (2012). Mindful Parenting: The Buck Stops Here. Psych Central. Retrieved

136
on August 14, 2012, from http://blogs.psychcentral.com/mindfulness/2012/04/mindful-parenting-the-buck- stops-here/ Goldstein, L. H., Harvey, E. A., Friedman-Weieneth, J., Pierce, C., Tellert, A., & Sippel, J. C. (2007). Examining subtypes of behavior problems among 3-year-old children, part II: Investigating differences in parent psychopathology, couple conflict, and other family stressors. Journal of Abnormal Child Psychology, 35(1), 111-123. doi:10.1007/s10802-006-9088-x Granic, I., Dishion, T. J., & Hollenstein, T. (2003). The family ecology of adolescence: A dynamic systems perspective on normative development. In G. R. Adams & M. D. Berzonsky (Eds.), Blackwell handbook of adolescence (pp. 60 –91). Malden, MA: Blackwell. Greco, L.A. & Eifert, G. H. (2004). Treating parent-adolescent conflict: Is acceptance the missing link for an integrative family therapy? Cognitive and Behavioral Practice, 11(3), 305-314. doi: 10.1016/S1077-7229(04)80045-2 Grills, A.E. & Ollendick, T. H. (2002). Issues in parent-child agreement: the case of structured diagnostic interviews. Clinical Child and Family Psychology Review, 5(1), 57-83. Retrieved from: http://resolver.scholarsportal.info.myaccess.library.utoronto.ca/resolve/10964037 v05i0001/57_iipatcosdi Grossman, P. (2008). On measuring mindfulness in psychosomatic and psychological research. Journal of Psychosomatic Research, 64(4), 405-408. doi: http://dx.doi.org/10.1016/j.jpsychores.2008.02.001 Grossman, P., Tiefenthaler-Gilmer, U., Raysz, A., & Kesper, U. (2007). Mindfulness training as an intervention for fibromyalgia: Evidence of postintervention and 3- year follow-up benefits in weil-being. Psychotherapy and Psychosomatics, 76(4), 226-233. doi: 10.1159/000101501
Gulliver, A., Griffiths, K. M., & Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry 10, 113. doi:10.1186/1471-244X-10-113 Gustafsson, P., Holmström, E., Besjakov, J., & Karlsson, M. K. (2010). ADHD
symptoms and maturity - a follow up study in school children. Acta paediatrica, 99(10), 1536–1539. doi: 10.1111/j.1651-2227.2010.01851.x
Hanh, T. N. (1975). The miracle of mindfulness: An introduction to the practice of
meditation. Boston, Masschusets: Beacon Press.

137
Hampel, P., Manhal, S., Roos, T., & Desman, C. (2008). Interpersonal coping among boys with ADHD. Journal of Attention Disorders, 11(4), 427-436. doi:10.1177/1087054707299337 Harrison, C., & Sofronoff, K. (2002). ADHD and parental psychological distress: Role of demographics, child behavioral characteristics, and parental cognitions. Journal of the American Academy of Child & Adolescent Psychiatry, 41(6), 703-711. doi: 10.1097/00004583-200206000-00010 Hartman, D. P, & Hall, R. V. (1976). The changing criterion design. Journal of Applied Behaviour Analysis, 9(4), 527–532. doi: 10.1901/jaba.1976.9-527 Harty, S. C., Miller, C. J., Newcorn, J. H., & Halperin, J. M. (2009). Adolescents with childhood ADHD and comorbid disruptive behavior disorders: aggression, anger, and hostility. Child Psychiatry and Human Development, 40(1), 85-97. doi: 10.1007/s10578-008-0110-0 Haydicky, J., Wiener, J., Badali, P., Milligan, K., & Ducharme, J. M. (2012). Evaluation of a mindfulness-based intervention for adolescents with learning disabilities and co-occurring ADHD and anxiety. Mindfulness, 3(2), 151-164. doi:10.1007/s12671- 012-0089-2 Hayes, S. C. (1994). Content, context, and the types of psychological acceptance. In S. C. Hayes, N. S. Jacobson, V. M. Follette, & M. J. Dougher (Eds.), Acceptance and change: Content and context in psychotherapy (pp. 13-32). Reno, NV: Context Press. Hayes, S. C., & Smith, S. (2005). Get out of your mind and into your life: The new Acceptance and Commitment Therapy. Oakland, CA: New Harbinger. Hayes, S. C., Strosahl, K. D., & Wilson, K. G. (1999). Acceptance and commitment therapy: An experiential approach to behavior change. New York: Guilford Press, New York, NY. Hechtman, L. & Greenfield, B. (2003). Long-term use of stimulants in children with attention deficit hyperactivity disorder: safety, efficacy, and long-term outcome. Pediatric Drugs, 5(12), 787-794. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/14658920 Hersen, M. & Barlow, D. H. (1976). Single case experimental designs: Strategies for studying behavior change. Pergamon Press: New York. Hinshaw, S. P., March, J. S., Abikoff, H., Arnold, L. E., Cantwell, D. P., Conners, C. K., . . . Wigal, T. (1997). Comprehensive assessment of childhood attention-deficit hyperactivity disorder in the context of a multisite, multimodal clinical trial. Journal of Attention Disorders, 1(4), 217-234. doi:

138
10.1177/108705479700100403 Hinshaw, S. P. , Owens , E. B. , Sami , N. , & Fargeon , S. (2006). Prospective follow-up of girls with attention-deficit/hyperactivity disorder into adolescence: Evidence for continuing cross-domain impairment . Journal of Consulting and Clinical Psychology, 74(3), 489–499. doi: 10.1037/0022-006X.74.3.489
Hinshaw, S. P., Owens, E. B., Wells, K. C., Kraemer, H. C., Abikoff, H. B., Arnold, L. E., . . . Wigal, T. (2000). Family processes and treatment outcome in the MTA: Negative/ineffective parenting practices in relation to multimodal treatment. Journal of Abnormal Child Psychology, 28(6), 555-568. doi: 10.1023/A:1005183115230 Hofmann, S. G., Sawyer, A. T., Witt, A. A., & Oh, D. (2010). The effect of mindfulness- based therapy on anxiety and depression: A meta-analytic review. Journal of Consulting and Clinical Psychology, 78(2), 169-183. doi: http://dx.doi.org/10.1037/a0018555 Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., Wolery, M. (2005). The use of single subject research to identify evidence-based practice in special education. Exceptional Children, 71(2), 165–179. Hoza, B., Kaiser, N., & Hurt, E. (2008). In Steele R. G., Elkin T. D. and Roberts M. C. (Eds.), Evidence-based treatments for attention-deficit/hyperactivity disorder (ADHD). New York, NY, US: Springer Science + Business Media, New York, NY. doi: 10.1007/978-0-387-73691-4_12 Jackson, S., Bijstra, J., Oostra, L., & Bosma, H. (1998). Adolescents' perceptions of communication with parents relative to specific aspects of relationships with parents and personal development. Journal of Adolescence, 21(3), 305-322. doi: 10.1006/jado.1998.0155 Jensen, P. S., Arnold, L. E., Swanson, J. M., Vitiello, B., Abikoff, H. B., Greenhill, L. L., . . . Hur, K. (2007). 3-year follow-up of the NIMH MTA study. Journal of the American Academy of Child & Adolescent Psychiatry, 46(8), 989-1002. doi: 10.1097/CHI.0b013e3180686d48 Jha, A.P., Krompinger, J., & Baime, M.J. (2007). Mindfulness training modifies subsystems of attention. Cognitive Affective and Behavioral Neuroscience, 7(2), 109-119. doi: 10.3758/CABN.7.2.109 Jha, A.P., Stanley, E.A., Kiyonaga, A., Wong, L., & Gelfand, L. (2010). Examining the protective effects of mindfulness training on working memory and affective experience. Emotion, 10(1), 54–64. doi: 10.1037/a0018438 Johnston, C. (1996). Parent characteristics and parent–child interactions in families of nonproblem children and ADHD children with higher and lower levels of

139
oppositional-defiant behavior. Journal of Abnormal Child Psychology, 24(1), 85- 104. doi: 10.1007/BF01448375
Johnston, C., & Mash, E. J. (2001). Families of children with Attention-Deficit/ Hyperactivity Disorder: Review and recommendations for future research. Clinical Child and Family Psychology Review, 4(3), 183-207. Retrieved from http://resolver.scholarsportal.info.myaccess.library.utoronto.ca/resolve/10964037/ v04i0003/183_focwadrarffr Johnston, C., & Jassy, J. S. (2007). Attention-deficit/hyperactivity disorder and oppositional/conduct problems: Links to parent-child interactions. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 16(2), 74-79. Retrieved from http://search.proquest.com/docview/621798824?accountid=14771 Judd, C.M., Smith, E.R. & Kidder, L.H. (1991) Research Methods in Social Relations, 6th edn. Holt, Rinehart and Winston, Inc.: Chicago. Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain and illness. New York: Delacorte. Kabat-Zinn, J. & Kabat-Zinn, M. (1997). Everyday blessings: The inner work of mindful parenting. New York: Hyperion. Kaiser, N. M., McBurnett, K., & Pfiffner, L. J. (2011). Child ADHD severity and positive and negative parenting as predictors of child social functioning: Evaluation of three theoretical models. Journal of Attention Disorders, 15(3), 193-203. doi:10.1177/1087054709356171 Kawabata, Y., Tseng, W., & Gau, S. S. (2012). Symptoms of attention- deficit/hyperactivity disorder and social and school adjustment: The moderating roles of age and parenting. Journal of Abnormal Child Psychology, 40(2), 177- 188. doi:10.1007/s10802-011-9556-9 Kazdin, A. E. (2001). Progression of therapy research and clinical application of treatment require better understanding of the change process. Clinical Psychology: Science and Practice, 8(2), 143-151. doi: 10.1093/clipsy/8.2.143 Kazdin, A. E., Mazurick, J. L., & Bass, D. (1993). Risk for attrition in treatment of antisocial children and families. Journal of Clinical Child Psychology, 22(1), 2- 16. doi:10.1207/s15374424jccp2201_1 Kent, K. M., Pelham, W. E., Molina, B. S. G., Sibley, M. H., Waschbusch, D. A., Yu, J., . . . Karch, K. M. (2011). The academic experience of male high school students with ADHD. Journal of Abnormal Child Psychology, 39(3), 451-462. doi:http://dx.doi.org/10.1007/s10802-010-9472-4

140
Kessler, R. C., Green, J. G., Adler, L. A., Barkley, R. A., Chatterji, S., Faraone, S. V., . . . Van Brunt, D. L. (2010). Structure and diagnosis of adult attention- deficit/hyperactivity disorder: Analysis of expanded symptom criteria from the adult ADHD clinical diagnostic scale. Archives of General Psychiatry, 67(11), 1168-1178. doi:10.1001/archgenpsychiatry.2010.146 Keune, P. M., & Forintos, D. (2010). Mindfulness meditation: A preliminary study on meditation practice during everyday life activities and its association with well- being. Psihologijske Teme, 19(2), 373-386. Retrieved from http://search.proquest.com/docview/906331401?accountid=14771 Khamis, V. (2006). Family environment and parenting as predictors of Attention-Deficit and Hyperactivity among Palestinian children. Journal of Social Service Research, 32(4), 99-116. doi: 10.1300/J079v32n04_06 Lambert, E. W., Doucette, A., & Bickman, L. (2001). Measuring mental health outcomes with pre-post designs. The Journal of Behavioral Health Services & Research, 28(3), 273-86. Retrieved from http://search.proquest.com/docview/205217780?accountid=14771 Langberg, J. M., Epstein, J. N., Altaye, M., Molina, B. S. G., Arnold, L. E., & Vitiello, B. (2008). The transition to middle school is associated with changes in the developmental trajectory of ADHD symptomatology in young adolescents with ADHD. Journal of Clinical Child and Adolescent Psychology, 37(3), 651-663. doi:10.1080/15374410802148095 Lange, G., Sheerin, D., Carr, A., Dooley, B., Barton, V., Marshall, D., . . . Doyle, M. (2005). Family factors associated with attention deficit hyperactivity disorder and emotional disorders in children. Journal of Family Therapy, 27(1), 76-96. doi: 10.1111/j.1467-6427.2005.00300.x Lanier, P., Kohl, P. L., Benz, J., Swinger, D., Moussette, P., & Drake, B. (2011). Parent– child interaction therapy in a community setting: Examining outcomes, attrition, and treatment setting. Research on Social Work Practice, 21(6), 689-698. doi: 10.1177/1049731511406551 Laursen, B., Coy, K. C., & Collins, W. A. (1998). Reconsidering changes in parent–child conflict across adolescence: A meta-analysis. Child Development, 69(3), 817-832. doi: 10.2307/1132206 Lerner, M., & Wigal, T. (2008). Long-term safety of stimulant medications used to treat children with ADHD. Journal of Psychosocial Nursing and Mental Health Services, 46(8), 39-48. doi:10.3928/02793695-20080801-06 Licitra-Kleckler, D., & Waas, G. A. (1993). Perceived social support among high-stress

141
adolescents: The role of peers and family. Journal of Adolescent Research, 8(4), 381-402. doi: 10.1177/074355489384003 Ma, J., Lei, D., Jin, X., Du, X., Jiang, F., Li, F., . . . Shen, X. (2012). Compensatory brain activation in children with attention deficit/hyperactivity disorder during a simplified Go/No-go task. Journal of Neural Transmission, 119(5), 613-619. doi: 10.1007/s00702-011-0744-0 Mannuzza, S., & Klein, R. G. (2000). Long-term prognosis in attention-deficit/ hyperactivity disorder. Child and Adolescent Psychiatric Clinics of North America, 9(3), 711-726. Retrieved from http://search.proquest.com/docview/619449353?accountid=14771 Margetts, B., Vorster, H., & Venter, C. (2003). Evidence-based nutrition: the impact of information and selection bias on the interpretation of individual studies. South African Journal of Clinical Nutrition, 16(3), 78-87. Retrieved from: http://www.sajcn.co.za/index.php/SAJCN/article/view/38/34 Marshal, M. P., Molina, B. S. G., & Pelham, W. E. (2003). Childhood ADHD and adolescent substance use: An examination of deviant peer group affiliation as a risk factor. Psychology of Addictive Behaviors, 17(4), 293-302. doi: http://dx.doi.org/10.1037/0893-164X.17.4.293 Martel, M., Nikolas, M., & Nigg, J. T. (2007). Executive function in adolescents with ADHD. Journal of the American Academy of Child & Adolescent Psychiatry, 46(11), 1437-1444. doi:10.1097/chi.0b013e31814cf953 Mash, E. J., & Johnston, C. (1990). Determinants of parenting stress: Illustrations from families of hyperactive children and families of physically abused children. Journal of Clinical Child Psychology, 19(4), 313-328. doi: 10.1207/s15374424jccp1904_3 McCleary, L. (2002). Parenting adolescents with attention deficit hyperactivity disorder: Analysis of the literature for social work practice. Health & Social Work, 27(4), 285- 292. doi: 10.1093/hsw/27.4.285 McCullagh, P. & Nelder, J. A. (1989). Generalized linear models. Chapman and Hall: London. McLaughlin, D. P., & Harrison, C. A. (2006). Parenting practices of mothers of children with ADHD: The role of maternal and child factors. Child and Adolescent Mental Health, 11(2), 82-88. doi: 10.1111/j.1475-3588.2005.00382.x Mendelson, T., Greenberg, M. T., Dariotis, J. K., Gould, L. F., Rhoades, B. L., & Leaf, P. J. (2010). Feasibility and preliminary outcomes of a school-based mindfulness intervention for urban youth. Journal of Abnormal Child Psychology, 38(7), 985- 994. doi: http://dx.doi.org/10.1007/s10802-010-9418-x

142
Mercugliano, M., Power, T. J., & Blum, N. J. (1999). The clinician's practical guide to attention-deficit/hyperactivity disorder. Baltimore: Brookes Publishing. Mikami, A. Y., Jack, A., Emeh, C. C., & Stephens, H. F. (2010). Parental influence on children with attention-deficit/hyperactivity disorder: I. relationships between parent behaviors and child peer status. Journal of Abnormal Child Psychology, 38(6), 721- 736. doi: 10.1007/s10802-010-9393-2 Mikami, A. Y., & Pfiffner, L. J. (2008). Sibling relationships among children with ADHD. Journal of Attention Disorders, 11(4), 482-492. doi: http://dx.doi.org/10.1177/1087054706295670 Mokrova, I., OBrien, M., Calkins, S., & Keane, S. (2010). Parental ADHD symptomology and ineffective parenting: The connecting link of home chaos. Parenting: Science and Practice, 10(2), 119-135. doi:10.1080/15295190903212844 Morgan, J., Robinson, D., & Aldridge, J. (2002). Parenting stress and externalizing child behavior. Child and Family Social Work, 7(3), 219–225. doi: 10.1046/j.13652206.2002.00242.x MTA Cooperative Group (1999). A 14-Month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. Archives of General Psychiatry, 56(12), 1073-1086. Retrieved from http://search.proquest.com/docview/207995571?accountid=14771
MTA Cooperative Group (2004a). National institute of mental health multimodal treatment study of ADHD follow-up: Changes in effectiveness and growth after the end of treatment. Pediatrics, 113(4), 762-769. Retrieved from http://search.proquest.com/docview/228368237?accountid=14771 MTA Cooperative Group (2004b). National institute of mental health multimodal treatment study of ADHD follow-up: 24-month outcomes of treatment strategies for attention-Deficit/Hyperactivity disorder. Pediatrics, 113(4), 754-761. Retrieved from http://search.proquest.com/docview/228411530?accountid=14771 Mulligan, R. C., Knopik, V. S., Sweet, L. H., Fischer, M., Seidenberg, M., & Rao, S. M. (2011). Neural correlates of inhibitory control in adult attention deficit/ hyperactivity disorder: Evidence from the Milwaukee longitudinal sample. Psychiatry Research: Neuroimaging, 194(2), 119-129. doi: 10.1016/j.pscychresns.2011.02.003 Murray, C., & Johnston, C. (2006). Parenting in mothers with and without attention- deficit/ hyperactivity disorder. Journal of Abnormal Psychology, 115(1), 52-61. doi: 10.1037/0021-843X.115.1.52

143
Musser, E. D., Backs, R. W., Schmitt, C. F., Ablow, J. C., Measelle, J. R., & Nigg, J. T. (2011). Emotion regulation via the autonomic nervous system in children with attention-deficit/hyperactivity disorder (ADHD). Journal of Abnormal Child
Psychology, 39(6), 841-852. doi:10.1007/s10802-011-9499-1 Myers, A., & Hansen, C. (2006). Experimental psychology, 6th ed. Belmont, CA, US: Thomson Wadsworth, Belmont, CA. Retrieved from http://search.proquest.com/docview/620893133?accountid=14771 Napoli, M., Krech, P. R., & Holley, L. C. (2005). Mindfulness training for elementary school students: The attention academy. Journal of Applied School Psychology, 21(1), 99-125. doi: 10.1300/J370v21n01_05 Neal, D. J., & Simons, J. S. (2007). Inference in regression models of heavily skewed alcohol use data: A comparison of ordinary least squares, generalized linear models, and bootstrap resampling. Psychology of Addictive Behaviors, 21(4), 441- 452. doi: 10.1037/0893-164X.21.4.441 Nigg, J. T. (2001). Is ADHD a disinhibitory disorder? Psychological Bulletin, 127(5), 571-598. doi: 10.1037/0033-2909.127.5.571 Nigg, J. T., & Casey, B. J. (2005). An integrative theory of attention-deficit/hyperactivity disorder based on the cognitive and affective neurosciences. Development and Psychopathology, 17(3), 785-806. doi: 10.1017/S0954579405050376 Oberle, E., Schonert-Reichl, K., Lawloe, M., & Thomson, K. (2012). Mindfulness and inhibitory control in early adolescence. The Journal of Early Adolescence, 32(4), 565-588. doi: 10.1177/0272431611403741 Ong, J. C., Shapiro, S. L., & Manber, R. (2008). Combining mindfulness meditation with cognitive-behavior therapy for insomnia: A treatment-development study. Behavior Therapy, 39(2), 171-182. doi: 10.1016/j.beth.2007.07.002 Pelham, W. E. (1999). The NIMH multimodal treatment study for attention-deficit hyperactivity disorder: Just say yes to drugs alone? The Canadian Journal of Psychiatry / La Revue Canadienne De Psychiatrie, 44(10), 981-990. Retrieved from http://search.proquest.com/docview/619438388?accountid=14771 Pelham, W. E., & Fabiano, G. A. (2008). Evidence-based psychosocial treatments for attention-deficit/hyperactivity disorder. Journal of Clinical Child and Adolescent Psychology, 37(1), 184–214. doi: 10.1080/15374410701818681 Pelham, W. E., Wheeler, T., & Chronis, A. (1998). Empirically supported psychosocial treatments for attention deficit hyperactivity disorder. Journal of Clinical Child Psychology, 27(2), 190-205. doi: 10.1207/s15374424jccp2702_6

144
Pisterman, S., Firestone, P., McGrath, P., Goodman, J. T., Webster, I., Mallory, R., & Coffin, B. (1992). The effects of parent training on parenting stress and sense of competence. Canadian Journal of Behavioural Science, 24(1), 41-58. doi: http://dx.doi.org/10.1037/h0078699 Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: A systematic review and metaregression analysis. American Journal of Psychiatry, 164, 942–948. doi: 10.1176/appi.ajp.164.6.942 Polanczyk, G., & Jensen, P. (2008). Epidemiologic considerations in attention deficit hyperactivity disorder: A review and update. Child and Adolescent Psychiatry Clinics of North America, 17, 245–260. doi: 10.1016/j.chc.2007.11.006 Pressman, L. J., Loo, S. K., Carpenter, E. M., Asarnow, J. R., Lynn, D., McCracken, J. T., . . . Smalley, S. L. (2006). Relationship of family environment and parental psychiatric diagnosis to impairment in ADHD. Journal of the American Academy of Child & Adolescent Psychiatry, 45(3), 346-354. doi:10.1097/01.chi.0000192248.61271.c8 Rasmussen, E. R., Todd, R. D., Neuman, R. J., Heath, A. C., Reich, W., & Rohde, L. A. (2002). Comparison of male adolescent- report of attention-deficit /hyperactivity disorder (ADHD) symptoms across two cultures using latent class and principal components analysis. Journal of Child Psychology and Psychiatry, 43(6), 797–805. Retrieved from http://search.proquest.com/docview/64724677?accountid=14771 Reader, S. K., Stewart, L. M. & Johnson, J. H. (2009). Assessing ADHD-related family stressors with the Disruptive Behavior Stress Inventory (DBSI): A replication and extension. Journal of Clinical Psychology in Medical Settings, 16, 148–160. doi: 10.1007/s10880-008-9140-9 Robin, A. L. (1981). A controlled evaluation of problem-solving communication training with parent adolescent conflict. Behavior Therapy, 12(5), 593-609. doi: 10.1016/S0005-7894(81)80132-3 Rogers, M., Hwang, H., Toplak, M., Weiss, M., & Tannock, R. (2011). Inattention, working memory, and academic achievement in adolescents referred for attention deficit/hyperactivity disorder (ADHD). Child Neuropsychology, 17(5), 444-458. doi:http://dx.doi.org/10.1080/09297049.2010.544648 Ruppert, D., Wand, M. P., & Carroll, R. J. (2003). Semiparametric Regression. Cambridge University Press: New York. Saltzman, A., & Goldin, P. (2010). Mindfulness Based Stress Reduction for school-age children. In S. C. Hayes and L. A. Greco (eds.), Acceptance and mindfulness interventions for children, adolescents, and families. Context Press/New Harbinger

145
Publications, Oakland, California. Sawyer Cohen, J., & Miller, L. J. (2009). Interpersonal mindfulness training for well- being: A pilot study with psychology graduate students. Teachers College Record, 111(12), 2760-2774. Retrieved from http://search.proquest.com/docview/857125501?accountid=14771 Schachter, H. M. H., Pham, B. B., King, J. J., Langford, S. S., & Moher, D. D. (2001). How efficacious and safe is short-acting methylphenidate for the treatment of attention-deficit disorder in children and adolescents? A meta-analysis. CMAJ: Canadian Medical Association Journal, 165(11), 1475-1488. Retrieved from http://search.proquest.com/docview/72337901?accountid=14771 Schoemaker, K., Bunte, T., Wiebe, S. A., Espy, K. A., Deković, M., & Matthys, W. (2012). Executive function deficits in preschool children with ADHD and DBD. Journal of Child Psychology and Psychiatry, 53(2), 111-119. doi:10.1111/j.1469- 7610.2011.02468.x Schroeder, V. M., & Kelley, M. L. (2009). Associations between family environment, parenting practices, and executive functioning of children with and without ADHD. Journal of Child and Family Studies, 18(2), 227-235. doi:10.1007/s10826- 008-9223-0 Segal, Z. V., Teasdale, J. D., & Williams, J. M. G. (2004). Mindfulness-based cognitive
therapy. In S. C. Hayes, V. M. Follette, & M. M. Linehan (Eds.), Mindfulness and Acceptance: Expanding the Cognitive-Behavioral Tradition (pp. 45-65). New York: The Guilford Press.
Segal, Z., Williams, J. M., & Teasdale, J. D. (2002). Mindfulness-based cognitive therapy for depression: A new approach to preventing relapse. New York, NY: The Guilford Press. Seidman, L. J. (2006). Neuropsychological functioning in people with ADHD across the lifespan. Clinical Psychology Review, 26(4), 466-485. Retrieved from http://search.proquest.com/docview/68642689?accountid=14771 Seipp, C. M., & Johnston, C. (2005). Mother-son interactions in families of boys with attention-deficit/hyperactivity disorder with and without oppositional behavior. Journal of Abnormal Child Psychology, 33(1), 87-98. Retrieved from http://search.proquest.com/docview/64587387?accountid=14771 Semple, R. J. (2010). Does mindfulness meditation enhance attention? A randomized controlled trial. Mindfulness, 1(2), 121-130. doi:10.1007/s12671-010-0017-2. Shek, D. T. L. (1998). A longitudinal study of the relations between parent-adolescent conflict and adolescent psychological well-being. The Journal of Genetic

146
Psychology, 159(1), 53-67. Retrieved from http://search.proquest.com/docview/65182849?accountid=14771 Silananda, U. (1990). The four foundations of mindfulness. Boston: Wisdom Publications Singh, N. N., Lancioni, G. E., Winton, A. S. W., Fisher, B. C., Wahler, R. G., McAleavey, K., . . . Sabaawi, M. (2006). Mindful parenting decreases aggression, noncompliance, and self-injury in children with autism. Journal of Emotional and Behavioral Disorders, 14(3), 169-177. Retrieved from http://search.proquest.com/docview/62016404?accountid=14771 Singh, N. N., Lancioni, G. E., Winton, A. S. W., Singh, J., Curtis, W. J., Wahler, R. G., & Mcaleavey, K. M. (2007). Mindful parenting decreases aggression and increases social behavior in children with developmental disabilities. Behavior Modification, 31(6), 749-771. Retrieved from http://search.proquest.com/docview/62080366?accountid=1477 Singh, N. N., Lancioni, G. E., Winton, A. S. W., Wahler, R. G., Singh, J., & Sage, M. (2004). Mindful caregiving increases happiness among individuals with profound multiple disabilities. Research in Developmental Disabilities, 25(2), 207-218. doi: 10.1016/j.ridd.2003.05.001 Singh, N. N., Singh, A.N., Lancioni, G.E., Singh, J., Winton, A.S.W., & Adkins, A.D. (2010). Mindfulness training for parents and their children with ADHD increases the children’s compliance. Journal of Child and Family Studies, 19, 157-166. doi:10.1007/s10826-009-9272-z
Smalley, S. L., Loo, S. K., Hale, T. S., Shrestha, A., McGough, J., Flook, L., & Reise, S. (2009). Mindfulness and attention deficit hyperactivity disorder. Journal of Clinical Psychology, 65(10), 1087-1098. doi: http://dx.doi.org/10.1002/jclp.20618
Smith, A. B., Taylor, E., Brammer, M., Toone, B., & Rubia, K. (2006). Task-specific hypoactivation in prefrontal and temporoparietal brain regions during motor inhibition and task switching in medication-naive children and adolescents with attention deficit hyperactivity disorder. The American Journal of Psychiatry, 163(6), 1044-1051. doi: 10.1176/appi.ajp.163.6.1044
Smith, B. H., Waschbusch, D. A., Willoughby, M. T., & Evans, S. (2000). The efficacy, safety, and practicality of treatments for adolescents with attention- Deficit/Hyperactivity disorder (ADHD). Clinical Child and Family Psychology Review, 3(4), 243-67. doi: 10.1023/A:1026477121224 Sonuga-Barke, E., Daley, D., & Thompson, M. (2002). Does maternal ADHD reduce the effectiveness of parent training for preschool children's ADHD? Journal of the American Academy of Child & Adolescent Psychiatry, 41(6), 696-702. doi: 10.1097/00004583-200206000-00009

147
Speca, M., Carlson, L. E., Goodey, E., & Angen, M. (2000). A randomized, wait-list controlled clinical trial: The effect of a mindfulness meditation-based stress reduction program on mood and symptoms of stress in cancer outpatients. Psychosomatic Medicine, 62(5), 613-622. Retrieved from http://search.proquest.com/docview/619450579?accountid=14771
Spoth, R., & Redmond, C. (2000). Research on family engagement in preventive interventions: Toward improved use of scientific findings in primary prevention practice. The Journal of Primary Prevention, 21(2), 267-284. doi: 10.1023/A:1007039421026 Spring, B., Rosen, K. H., & Matheson, J. L. (2002). How parents experience a transition to adolescence: A qualitative study. Journal of Child and Family Studies, 11(4), 411-425. Retrieved from http://search.proquest.com/docview/57801925?accountid=14771 Steinberg, L. (2001). We know some things: Parent-adolescent relationships in retrospect and prospect. Journal of Research on Adolescence, 11(1), 1-19. Retrieved from http://search.proquest.com/docview/61424678?accountid=14771 Sullivan, M. J., Wood, L., Terry, J., Brantley, J., Charles, A., McGee, V., et al. (2009). The Support, Education and Research in Chronic Heart Failure Study: a mindfulness-based psychoeducational intervention improves depression and clinical symptoms in patients with chronic heart failure. American Heart Journal, 157(1), 84–90. doi:10.1016/j.ahj.2008.08.033 Swanson, J., Arnold, L. E., Kraemer, H., Hechtman, L., Molina, B., Hinshaw, S., . . . Wigal, T. (2008). Evidence, interpretation, and qualification from multiple reports of long-term outcomes in the multimodal treatment study of children with ADHD (MTA): Part I: Executive summary. Journal of Attention Disorders, 12(1), 4-14. doi: 10.1177/1087054708319345 Tamm, L., Menon, V., Ringel, J., & Reiss, A. L. (2004). Event-related fMRI evidence of frontotemporal involvement in aberrant response inhibition and task switching in attention-deficit/hlyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry, 43(11), 1430-1440. doi: 10.1097/01.chi.0000140452.51205.8d Tang, Y., Ma, Y., Wang, J., Fan, Y., Feng, S., Lu, Q., . . . Posner, M. I. (2007). Short- term meditation training improves attention and self-regulation. PNAS Proceedings of the National Academy of Sciences of the United States of America, 104(43), 17152-17156. Retrieved from http://search.proquest.com/docview/621925156?accountid=14771 Tannock, R. (2000). Attention-deficit/hyperactivity disorder with anxiety disorders. In T.

148
E. Brown (Ed.), Attention-deficit disorders and comorbidities in children, adolescents, and adults (pp. 125−170). Washington, DC: American Psychiatric Press. Teasdale, J. D., Segal, Z., & Williams, J. M. (1995). How does cognitive therapy prevent depressive relapse and why should attentional control (mindfulness) training help? Behaviour Research and Therapy, 33(1), 25-39. doi: http://dx.doi.org/10.1016/0005-7967(94)E0011-7 Theule, J., Wiener, J., Rogers, M. A., & Marton, I. (2011). Predicting parenting stress in families of children with ADHD: Parent and contextual factors. Journal of Child and Family Studies, 20(5), 640-647. doi: 10.1007/s10826-010-9439-7 Theule, J., Wiener, J., Jenkins, J., & Tannock, R. (2013). Parenting stress in families of
children with ADHD: A meta-analysis. Journal of Emotional and Behavioral Disorders, 21(1), 3-17. doi: 10.1177/1063426610387433 Thompson, A. L., Molina, B. S. G., Pelham, W., & Gnagy, E. M. (2007). Risky driving in adolescents and young adults with childhood ADHD. Journal of Pediatric Psychology, 32(7), 745-759. doi: http://dx.doi.org/10.1093/jpepsy/jsm002 Thorell, L. B., & Wåhlstedt, C. (2006). Executive functioning deficits in relation to symptoms of ADHD and/or ODD in preschool children. Infant and Child Development, 15(5), 503-518. doi: 10.1002/icd.475 Treacy, L., Tripp, G., & Baird, A. (2005). Parent stress management training for Attention-Deficit/Hyperactivity disorder. Behavior Therapy, 36(3), 223-233. doi: 10.1016/S0005-7894(05)80071-1 Valiente, C., Lemery-Chalfant, K., Swanson, J., & Reiser, M. (2008). Prediction of children's academic competence from their effortful control, relationships, and classroom participation. Journal of Educational Psychology, 100(1), 67-77. doi: http://dx.doi.org/10.1037/0022-0663.100.1.67 van de Weijer-Bergsma, E., Formsma, A. R., de Bruin, E.I., & Bogels, S. M. (2011). The effectiveness of mindfulness training on behavioral problems and attentional functioning in adolescents with ADHD. Journal of Child and Family Studies, doi: 10.1007/s10826-011-9531-7 van den Hoofdakker, B. J., van der Veen-Mulders, L., Sytema, S., Emmelkamp, P. M. G., Minderaa, R. B., & Nauta, M. H. (2007). Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: A randomized controlled study. Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1263- 1263. Retrieved from http://search.proquest.com/docview/62058090?accountid=14771

149
van den Hurk, P. A., Giommi, F., Gielen, S. C., Speckens, A. E., & Barendregt, H. P. (2010). Greater efficiency in attentional processing related to mindfulness meditation. Quarterly Journal of Experimental Psychology, 63(6), 1168-1180. doi:10.1080/17470210903249365 van der Oord, S., Bögels, S. M., & Peijnenburg, D. (2012). The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. Journal of Child and Family Studies, 21(1), 139-147. doi:10.1007/s10826-011-9457-0
Van Roy, B., Groholt, B., Heyerdahl, S., & Clench-Aas, J. (2010). Understanding discrepancies in parent-child reporting of emotional and behavioural problems: Effects of relational and socio-demographic factors. BMC Psychiatry, 10(56). doi:10.1186/1471-244X-10-56 van Vugt, M. & Jha, A.P. (2011). Investigating the impact of mindfulness meditation training on working memory: A mathematical modeling approach. Cognitive, Affective, and Behavioral Neuroscience, 11, 344-353. doi: 10.3758/s13415-011- 0048-8 Vitiello, B. (2001). Long-term effects of stimulant medications on the brain: Possible relevance to the treatment of Attention Deficit Hyperactivity Disorder. Journal of Child and Adolescent Psychopharmacology, 11(1), 25-34. doi:10.1089/104454601750143384. Wåhlstedt, C., Thorell, L. B., & Bohlin, G. (2009). Heterogeneity in ADHD: Neuropsychological pathways, comorbidity and symptom domains. Journal of Abnormal Child Psychology, 37(4), 551-564. doi: 10.1007/s10802-008-9286-9 Walcott, C. M., & Landau, S. (2004). The relation between disinhibition and emotion regulation in boys with attention deficit hyperactivity disorder. Journal of Clinical Child and Adolescent Psychology, 33(4), 772-782. Retrieved from http://search.proquest.com/docview/62130721?accountid=14771 Weinberger, D. A., Ford, M. E., Tublin, S. K., & Feldman, S. S. (1990). Preadolescents' social-emotional adjustment and selective attrition in family research. Child Development, 61, 1374-1386. Retrieved from http://search.proquest.com/docview/57883841?accountid=14771 Wechsler, D. (1999). Wechsler Abbreviated Scale of Intelligence (WASI). San Antonio, TX: Harcourt Assessment. Weinstein, C. S., Apfel, R. J., & Weinstein, S. R. (1998). Description of mothers with ADHD with children with ADHD. Psychiatry: Interpersonal and Biological Processes, 61(1), 12-19. Retrieved from http://search.proquest.com/docview/619323605?
150
Whipple, E. E., & Richey, C. A. (1997). Crossing the line from physical discipline to child abuse: How much is too much? Child Abuse & Neglect, 21(5), 431-444. doi: 10.1016/S0145-2134(97)00004-5 Wiener, J., Malone, M., Varma, A., Markel, C., Biondic, D., Tannock, R., & Humphries, T. (2012). Children’s perceptions of their ADHD symptoms: Positive illusions, attributions, and stigma. Canadian Journal of School Psychology, 27(3) 217 –242. doi: 10.1177/0829573512451972 Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). A meta-analytic review of the executive function theory of ADHD. Biological Psychiatry, 57(11), 1336-1346. doi: 10.1016/j.biopsych.2005.02.006 Williams, M., Teasdale, J., Segal, Z., & Kabat-Zinn, J. (2007). The mindful way through depression: Freeing yourself from chronic unhappiness. New York, NY, US: Guilford Press, New York, NY. Retrieved from http://search.proquest.com/docview/621804127?accountid=14771 Witek-Janusek, L., Albuquerque, K., Chroniak, K. R., Chroniak, C., Durazo-Arvizu, R., & Mathews, H. L. (2008). Effect of MBSR on immune function, quality of life, and coping in women newly diagnosed with early stage breast cancer. Brain, Behavior and Immunology, 22(6), 969–981. doi: 10.1016/j.bbi.2008.01.012 Wolf, M. M. (1978). Social validity: The case for subjective measurement or how applied behavior analysis is finding its heart. Journal of Applied Behavior Analysis, 11(2), 203-214. doi: 10.1901/jaba.1978.11-203 Wolraich, M. L., Lambert, E. W., Bickman, L., Simmons, T., Doffing, M. A., & Worley, K. A. (2004). Assessing the impact of parent and teacher agreement on diagnosing attention-deficit hyperactivity disorder. Journal of Developmental and Behavioral Pediatrics, 25(1), 41-47. doi:10.1097/00004703-200402000-00007 Wolraich, M. L., McGuinn, L., & Doffing, M. (2007). Treatment of attention deficit hyperactivity disorder in children and adolescents: Safety considerations. Drug Safety, 30(1), 17-26. Retrieved from http://adisonline.com/drugsafety/Fulltext/2007/30010/Treatment_of_Attention_D eficit_Hyperactivity.3.aspx Wolraich, M. L., Wibbelsman, C. J., Brown, T. E., Evans, S. W., Gotlieb, E. M., Knight, J. R., et al. (2005). Attention-Deficit/Hyperactivity Disorder among adolescents: A review of the diagnosis, treatment, and clinical implications. Pediatrics, 115(6), 1734-1746. doi: 10.1542/peds.2004-195 Wymbs, B. T., & Pelham, W. E. (2010). Child effects on communication between parents of youth with and without attention-deficit/hyperactivity disorder. Journal of

151
Abnormal Psychology, 119(2), 366-375. doi: 10.1037/a0019034 Zimmerman, M., Ruggero, C. J., Chelminski, I., Young, D., Posternak, M. A., Friedman, M., Boerescu, D., & Attiullah, N. (2006). Developing brief scales for use in clinical practice: the reliability and validity of single-item self-report measures of depression symptom severity, psychosocial impairment due to depression, and quality of life. Journal of Clinical Psychiatry, 67 (10), 1536-1541. Zisser, A. R., & Eyberg, S. M. (2012). Maternal ADHD: Parent-child interactions and relations with child disruptive behavior. Child & Family Behavior Therapy, 34(1), 33-52. doi:10.1080/07317107.2012.654450 Zwi, M., Jones, H., Thorgaard, C., York, A., & Dennis, J. A. (2011). Parent training interventions for Attention Deficit Hyperactivity Disorder (ADHD) in children aged 5 to 18 years. Cochrane Database of Systematic Reviews,12, 1-99. doi: 10.1002/14651858.CD003018.pub3 Zylowska, L., Ackerman, D. L., Yang, M. H., Futrell, J. L., Horton, N. L., Hale, T. S., . . . Smalley, S. L. (2008). Mindfulness meditation training in adults and adolescents with ADHD: A feasibility study. Journal of Attention Disorders, 11(6), 737-746. doi:10.1177/1087054707308502

152
Appendix A Information Letter
What is MYmind: Mindfulness training for Youth with ADHD and their parents?
MYmind: Mindfulness training for Youth with ADHD and their parents is an 8-week group intervention for teenagers who have ADHD, and their parents. The goals of the program are to helpteensmanagetheirADHDsymptoms,tohelpteensandparentsreducetheirstress,andtoreduceconflictandimprovethequalityofrelationshipsbetweenadolescentsandtheirparents. The program involves meditation exercises and discussions about problem solving strategies. It has been previously evaluated by researchers in Holland and both parents and teens found it to be very helpful. Research has shown that mindfulness meditation has helped improve ADHD behaviours, such as inattention, impulsivity and oppositionality. Mindfulness also reduces stress and improves quality of life.
What do I have to do?
You will attend 8 weekly sessions, lasting approximately 1.5 hours. The parent and teens group will be running simultaneously, and sometimes come together as one large group. The sessions will take place at OISE, which is located at Bloor and St. George. The sessions are held on Saturday mornings. Both parents are invited to join the program, but at least one parent must commit to attending all 8 sessions. IfyouhavemorethanoneteenagerwithADHDthenbothmaybeeligibletoparticipate.
The research component will involve filling out questionnaires at 4 time points in sessions of approximately 1 hour. You will also receive daily email reminders to practice the mindfulness techniques and problem solving strategies at home. Because we will only be meeting weekly, it will be really important to practice what you’ve learned in sessions at home. Some people will be selected to complete a short questionnaire at this time and submit it via email nightly.
What about our privacy?
Your privacy will be respected. All questionnaire data are considered strictly confidential and will not be shared with anyone outside of the research group at OISE/UT. Any research reports thatresultfromthisstudywillbeinagroupformat,withallidentifyinginformationofparticipantsremoved.Thereareafewinstanceswheretheresearchersarerequiredbylawtobreachconfidentiality.Intheeventthatanadolescentunder16indicatesthatheorsheis(indangerof)beingharmed,weareobligatedtoinformhis/herparentsandtheappropriateprofessionals,and/ormakeareporttoappropriatechildprotectionagencies.Wealsohaveadutytoreportifwe

153
havereasontobelievethatanyparticipant,nomattertheirage,hasintenttocauseseriousharmtohim/herselforothers.
What are the benefits?
In addition to contributing to scientific knowledge about ADHD and mindfulness meditation, there are several benefits that participants will receive from the study.
• Parents and youth participating may get personal benefit in the form of improved self-efficacy, reduction in problem behaviours, reduction in stress, and improved parent-child interactions.
• Dr. Wiener’s research group has created a web site for participants in her studies, communicating the results of the studies and providing links to resources for individuals with ADHD. The website is: http://adhdld.com
• Youth who are in high school will receive Community Service Certificates for the time they spend completing questionnaires in connection with this study (approximately 4-5 hours). Alternatively, youth can receive a small gift as compensation.
Are there any risks?
Other than investment of time, there are no known risks associated with participating in the study. One potential risk is that some people may feel some discomfort when answering questions about their relationships. You will be prepared for this situation during the consent procedure. You may skip any question, request a break, or withdraw from the study at any time without penalty. You are encouraged to speak with the group leaders if they need further support. The meditation practice may become be uncomfortable or boring for some participants, but these issues usually subside with practice.
If you have any further questions, please contact [email protected] or call us at (416) 978-0933

154
Thiswasonofficialletterhead
Appendix B Parent and Adolescent Consent Form
Didyouunderstandtheexplanationofthemindfulnessprogram?□yes □noDoyouwishtoparticipatein8weeklysessions,whichincludesfillingoutquestionnairesatfourdifferenttimes? □yes □noDoyouunderstandthatyouwillreceiveanemailremindereverynight,andyoumaybeselectedtocompleteabriefquestionnaireatthattime?□yes □noDoyouunderstandthatyoumayskipaquestion,requestabreak,orstopparticipatingintheresearchatanytime? □yes □noNameofparticipant:_______________________________________Participant’sdateofbirth:Month:________Day:_______Year:_______Signatureofparticipant:____________________________Date:_____________________________Emailand/orCellPhoneNumber:______________________________________

155
Appendix C Demographics Questionnaire
Parent’s Name:______________________________ Phone Number: ______________________(Home)
______________________(Cell) ______________________ (Work)
Would you (parent) prefer to complete the daily questionnaire via email or facebook? Parent Email:_______________________________ Parent Contact Name on Facebook:___________________________ Adolescent’s Name:_______________________________ Adolescent’s D.O.B.: /___/___/___ Age:________ Grade:_____ dd/mm/yy Home Address: __________________________________________ __________________________________________ __________________________________________ Will one or both parents be participating in the mindfulness program? ONE BOTH Please list the people currently living in your home:
Name Gender (M/F) Age Relationship to Child
Please list any immediate family members (parent, brother/sister) not currently living at home.
Name Gender (M/F) Age Relationship to Child

156
What is your marital status? Single Married Re-married Common Law Separated Divorced Widowed Was your son/daughter diagnosed with ADHD/ADD? YES NO If yes, what subtype of ADHD was your son/daughter diagnosed with (circle one)?
a) Inattentive b) Hyperactive/impulsive c) Combined I & HA/I d) Unsure/don't remember
When was you son/daughter diagnosed? Who diagnosed him/her? Was your son/daughter diagnosed with LD? YES NO When was your son/daughter diagnosed? Who diagnosed him/her?
What is the nature of your son/daughter's LD (eg. Processing speed, fine motor, verbal language, fluency etc.)
Which academic areas are affected by your son/daughter's LD (eg. Language, math)
Does your son/daughter have any diagnoses besides ADHD or LD? YES, Specify:________________________ NO Has your son/daughter had any assessments/psychological evaluations?

157
YES NO If so, what kind of assessment and when were they tested? Is your son or daughter currently taking any medication? YES, Specify:_____________________________ NO If your son or daughter takes medication for ADHD, do they take it on weekends? YES NO Have you and/or your child received any treatment for your child's behavioural issues? (e.g. behaviour management training, parent management training, therapy) YES, Specify type and date received:_____________________________ NO Have you and/or your child received and treatment/intervention for family issues? (e.g. family therapy, couples counseling) YES, Specify type and date received:_____________________________ NO Do any members of the family (immediate or extended) have an ADHD diagnosis? YES (Specify member of family)_____________________ NO Do you suspect that any members of the family (immediate or extended) have undiagnosed ADHD? YES NO If yes, Who? If yes, What makes you think that? Is English your first language? YES NO Is English your son/daughter’s first language? YES NO Is there a language other than English spoken at home? YES NO
If yes, what other language(s) are spoken?_____________________________ Was your child born in Canada? YES NO If not, where was s/he born? _____________________ How long has s/he lived in Canada?____________years

158
Were you born in Canada? YES NO If not, where were you born? ___________________ How long have you lived in Canada?_____________years If applicable, was your spouse/partner born in Canada? YES NO
If not, where was s/he born?_____________________ How long has s/he lived in Canada?_______________years What is the highest level of education that you completed?
1. No schooling 2. Some elementary 3. Completed elementary 4. Some secondary 5. Completed secondary 6. Some college 7. Completed a college program 8. Some university 9. Completed an undergraduate university degree 10. Master’s degree 11. Doctoral degree
If applicable, what is the highest level of education that your partner/spouse completed? 1. No schooling 2. Some elementary 3. Completed elementary 4. Some secondary 5. Completed secondary 6. Some college 7. Completed a college program 8. Some university 9. Completed an undergraduate degree 10. Master’s degree 11. Doctoral degree
What kind of work do you and your spouse/partner (if applicable) do? You: _________________________ Full time Part time Currently unemployed
Spouse/ Full time Partner:_________________________ Part time Currently unemployed

159
Appendix D DailySymptomQuestionnaireParentversion
PleaseplaceanXbesidetheratingthatbestdescribesyourfeelingsandbehavioursandthoseofyourson/daughtertoday.
1.) Howmuchstresswereyoufeelingingeneraltoday?(Almostnone)(ALittle)(Some)(Quiteabit)(Alot)
2.) Howmuchtimedidyouspendwithyourson/daughtertoday?
__(Almostnone)__(lessthan1hour)__(2‐3hours)__(4‐5hours)__(morethan5hours)
3.) Howmuchdistressdidyouexperienceasaresultofinteractions/conflictswithyourson/daughtertoday?
(Almostnone)(ALittle)(Some) (Quiteabit)(Alot)
4.) Howdifficultwasitforyourson/daughtertopayattention(e.g.,troublelistening,focusing)today?
(Notvery)(ALittle)(Somewhat)(Quiteabit)(Alot)
5.) Howrestless(e.g.,troublesittingstill,fidgeting,talkingtoomuch)wasyour
son/daughtertoday?(Notvery)(ALittle)(Somewhat)(Quiteabit)(Alot)
6.) Howimpulsive(e.g.,actingbeforethinking)wasyourson/daughtertoday?(Notvery)(ALittle)(Somewhat)(Quiteabit)(Alot)
7.) Howlongdidyoumeditatetoday?(Notatall)(5min) (10min)(15min)(20
minormore)

160
DailySymptomQuestionnaireAdolescentversionPleaseplaceanXbesidetheratingthatbestdescribesyourfeelingsandbehaviourstoday.
1.) Howmuchstresswereyoufeelingingeneraltoday?(Almostnone)(ALittle)(Some)(Quiteabit)(Alot)
2.) Howmuchtimedidyouspendwithyourparenttoday?
__(Almostnone)__(lessthan1hour)__(2‐3hours)__(4‐5hours)__(morethan5hours)
3.) Howmuchdistressdidyouexperienceasaresultofinteractions/conflictswithyourparenttoday?
(Almostnone)(ALittle)(Some) (Quiteabit)(Alot)
4.) Howdifficultwasitforyoutopayattention(e.g.,troublelistening,focusing)
today?
(Notvery)(ALittle)(Somewhat)(Quiteabit)(Alot)
5.) Howrestless(e.g.,troublesittingstill,fidgeting,talkingtoomuch,justfeelingrestlessinside)wereyoutoday?(Notvery)(ALittle)(Somewhat)(Quiteabit)(Alot)
6.) Howimpulsive(e.g.,actingbeforethinking)wereyoutoday?
(Notvery)(ALittle)(Somewhat)(Quiteabit)(Alot)
7.) Howlongdidyoumeditatetoday?(Notatall)(5min)(10min)(15min)(20min
ormore)

161
Appendix E Instructions for Completing the Parent Questionnaires
Below is a list of explanations of what each rating means in order to help you fill out the daily email questionnaires. Please feel free to print it out and have it as an aid to help you in rating your own and your adolescent's feelings and behaviours. 1. How much stress were you feeling in general today? ___(Almost none) ___(A little) ___(Some) ___(Quite a bit) ___(A lot) “Almost None” means that you were calm and relaxed overall today. “A little” means that you were fairly calm, and only mildly bothered by events today. “Some” means that you were agitated by events today, but it did not greatly disrupt your day. “Quite a bit” means that you were upset and disturbed today and you had a difficult time carrying out your day. “A lot” means you were frantic, panicked and felt out of control today and could not manage to get through the day. 2. How much time did you spend with your son/daughter today?
__(Almost none) __(less than 1 hour) __(2-3 hours) __(4-5 hours ) __(more than 5 hours)
3. How much distress did you experience as a result of interactions/conflicts with your son/daughter today? ___(Almost none) ___(A little) ___(Some) ___(Quite a bit) ___(A lot) “Almost none” means that you had mostly positive feelings during your interactions with your adolescent today. “A little” means that you experienced minimal annoyance or frustration while interacting with your adolescent today, but those feelings did not last very long. “Some” means that you experienced some frustration while interacting with your adolescent today and it may have turned into a mild conflict(s). “Quite a bit” means that you experienced anger and aggravation after getting into a conflict(s) with your adolescent today, and it affected your mood for the rest of the day. “A lot” means that you experienced so much aggravation and fury from interacting with your adolescent you were not able to carry on with your day because the conflict(s) affected you so much. 4. How difficult was it for your son/daughter to pay attention (e.g., trouble listening, focusing) today? ___(Not very) ___(A little) ___(Somewhat) ___(Quite a bit) ___(A lot)

162
“Not Very” means your adolescent was able to concentrate and listen attentively today with almost no difficulty. “A little” means that your adolescent was mostly able to concentrate and listen attentively today, even if support was provided (e.g., reminders, repetitions, prompts). “Somewhat” means that your adolescent needed reminders and instructions to be repeated in order to concentrate and listen to what was being said, although still had some difficulty. “Quite a bit” means that your adolescent had a difficult time concentrating and listening attentively, even if support was provided (e.g., reminders, repetitions, prompts). “A lot” means your adolescent could not listen attentively (e.g., did not hear anything said to him/her) or concentrate (e.g., was very distracted), even if support was provided (e.g., reminders, repetitions, prompts). 5. How restless (e.g., trouble sitting still, fidgeting, talking too much) was your son/daughter today? ___(Not very) ___(A little) ___(Somewhat) ___(Quite a bit) ___(A lot) “Not Very” means your adolescent was able to wait for his/her turn, sit still and speak about one topic at a time today with almost no difficulty. “A little” means that your adolescent was sometimes able to wait for his/her turn, sit still and speak about one topic at a time today, when support was provided (e.g., reminders, prompts). “Somewhat” means that your adolescent had some trouble waiting for his/her turn, sitting still, and staying on one topic before jumping to the next today, and reminders or prompts would only sometimes help. “Quite a bit” means that your adolescent had a difficult time waiting for his/her turn, sitting still and speaking about one topic at a time today, and reminders or prompts would only occasionally help. “A lot” means your adolescent was very impatient, could not wait for his/her turn, could not sit still and demonstrated excessive talking today, even if support was provided (e.g., reminders, prompts). 6. How impulsive (e.g., acting before thinking) was your son/daughter today? ___(Not very) ___(A little) ___(Somewhat) ___(Quite a bit) ___(A lot) “Not Very” means your adolescent was able to take time and think before acting today with almost no difficulty. “A little” means that your adolescent was sometimes able to take time and think before acting today, when support was provided (e.g., reminders, prompts). “Somewhat” means that your adolescent had some trouble taking time to think before acting today, and reminders or prompts would only sometimes help. “Quite a bit” means that your adolescent frequently acted without thinking first today, and reminders or prompts would only occasionally help.. “A lot” means your adolescent was very impulsive and acted spontaneously today

163
without thinking first at all, even if support was provided (e.g., reminders, prompts). 7. How long did you meditate today? ___(Not at all) ___(5 mins) ___(10 mins) ___(15 mins) ___(20 mins or more)

164
Instructions for Completing the Adolescent Questionnaires
Below is a list of explanations of what each rating means in order to help you fill out the daily email questionnaires. Please feel free to print it out and have it as an aid to help you in rating your feelings and behaviours. 1. How much stress were you feeling in general today? ___(Almost none) ___(A little) ___(Some) ___(Quite a bit) ___(A lot) “Almost None” means that you were calm and relaxed overall today. “A little” means that you were fairly calm, and only mildly bothered by events today. “Some” means that you were agitated by events today, but it did not greatly disrupt your day. “Quite a bit” means that you were upset and disturbed today and you had a difficult time carrying out your day. “A lot” means you were frantic, panicked and felt out of control today and could not manage to get through the day. 2. How much time did you spend with your parent today? __(Almost none) __(less than 1 hour) __(2-3 hours) __(4-5 hours ) __(more than 5 hours)
3. How much distress did you experience as a result of interactions/conflicts with your parent today? ___(Almost none) ___(A little) ___(Some) ___(Quite a bit) ___(A lot) “Almost none” means that you had mostly positive feelings during your interactions with your parent today. “A little” means that you experienced minimal annoyance or frustration while interacting with your parent today, but those feelings did not last very long. “Some” means that you experienced some frustration while interacting with your parent today and it may have turned into a mild conflict(s). “Quite a bit” means that you experienced anger and aggravation after getting into a conflict(s) with your parent today, and it affected your mood for the rest of the day. “A lot” means that you experienced so much aggravation and fury from interacting with your parent you were not able to carry on with your day because the conflict(s) affected you so much. 4. How difficult was it for you to pay attention (e.g., trouble listening, focusing) today? ___(Not very) ___(A little) ___(Somewhat) ___(Quite a bit) ___(A lot)

165
“Not Very” means you were able to concentrate and listen attentively today with almost no difficulty. “A little” means that you were mostly able to concentrate and listen attentively today, even if support was provided (e.g., reminders, repetitions, prompts). “Somewhat” means that you needed reminders and instructions to be repeated in order to concentrate and listen to what was being said, although still had some difficulty. “Quite a bit” means that you had a difficult time concentrating and listening attentively, even if support was provided (e.g., reminders, repetitions, prompts). “A lot” means you could not listen attentively (e.g., did not hear anything said to him/her) or concentrate (e.g., was very distracted), even if support was provided (e.g., reminders, repetitions, prompts). 5. How restless (e.g., trouble sitting still, fidgeting, talking too much) were you today? ___(Not very) ___(A little) ___(Somewhat) ___(Quite a bit) ___(A lot) “Not Very” means you were able to wait for your turn, sit still and speak about one topic at a time today with almost no difficulty. “A little” means that you were sometimes able to wait for your turn, sit still and speak about one topic at a time today, when support was provided (e.g., reminders, prompts). “Somewhat” means that you had some trouble waiting for your turn, sitting still, and staying on one topic before jumping to the next today, and reminders or prompts would only sometimes help. “Quite a bit” means that you had a difficult time waiting for your turn, sitting still and speaking about one topic at a time today, and reminders or prompts would only occasionally help. “A lot” means you were very impatient, could not wait for your turn, could not sit still and demonstrated excessive talking today, even if support was provided (e.g., reminders, prompts). 6. How impulsive (e.g., acting before thinking) were you today? ___(Not very) ___(A little) ___(Somewhat) ___(Quite a bit) ___(A lot) “Not Very” means you were able to take time and think before acting today with almost no difficulty. “A little” means that you were sometimes able to take time and think before acting today, if support was provided (e.g., reminders, prompts). “Somewhat” means that you had some trouble taking time to think before acting today, and reminders or prompts would only sometimes help. “Quite a bit” means that you frequently acted without thinking first today, and reminders or prompts would only occasionally help.. “A lot” means you were very impulsive and acted spontaneously today without thinking first at all, even if support was provided (e.g., reminders, prompts).

166
7. How long did you meditate today? ___(Not at all) ___(5 mins) ___(10 mins) ___(15 mins) ___(20 mins or more)

167
Appendix F Parent Consumer Satisfaction Questionnaire
ThefollowingquestionnaireispartofourevaluationoftheMYmindprogramthatyouhavereceived.Itisimportantthatyouanswerashonestlyaspossible.Theinformationobtainedwillhelpustoevaluateandcontinuallyimprovetheprogramweoffer.Yourco‐operationisgreatlyappreciated!Pleasecircletheappropriateresponsethatbestexpresseshowyoufeel.A. THEOVERALLPROGRAM1.Howsatisfiedareyouwiththehelpyoureceived?very dissatisfied neutral satisfied verydissatisfied satisfied2.TowhatdegreehastheMYmindprogramhelpedyoutodealwithyourproblems?Notatall AlittleSomewhatQuiteabit Alot
3. Ifeeltheapproachtotreatingadolescent’sADHDdifficultiesandparent‐
adolescentconflictusingthistypeoftrainingprogramis:
very inappropriate neutral appropriate veryinappropriate appropriate4. TowhatextenthastheMYmindprogrammetyourneeds?none afew some many almostallofmyneeds ofmyneeds ofmyneedsofmyneeds ofmyneeds5. WouldyourecommendtheMYmindprogramtoafriendorrelative?not not neutral recommend stronglyrecommend recommend recommend strongly 6. TowhatdegreehastheMYmindprogramhelpedtoimproveyouradolescent’s
ADHDsymptomsoverall?
NotatallAlittleSomewhatQuiteabitAlot
168
7. TowhatdegreehastheMYmindprogramhelpedtoimproveyourabilityto
manageyourstressoverall?NotatallAlittleSomewhatQuiteabitAlot
8. TowhatdegreehastheMYmindprogramhelpedtoimproveyourrelationship
withyouradolescent(e.g.,howyouresolveconflicts)?NotatallAlittleSomewhatQuiteabitAlot9. Towhatdegreehasthetreatmentprogramhelpedwithothergeneralpersonal
orfamilyproblemsnotdirectlyrelatedtoyouradolescent?NotatallAlittleSomewhatQuiteabitAlotPleasebrieflydescribewhatthoseproblemswere:
10. Howconfidentareyouinyourabilitytomanagefutureconflictswithyour
adolescentusingwhatyouhavelearnedfromthisprogram?notatall notvery neutral confident veryconfident confident confident11. Myoverallfeelingaboutthetreatmentprogramformyadolescentis:very negative neutral positive verynegative positive12. Overall,asaresultofbeinginthisprogram,howwouldyourateyourselfasa
parent?considerably worse the improved greatlyworse same improved13. Pleasewritedownanypartofservicesyoudidnotlike.
B. GROUPLEADER
169
1.Howwelldoyouthinkyourgroupleaderlistenedtoyourconcern(s)?notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐52.Howwelldoyouthinkyourgroupleaderunderstoodyourconcerns?notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐53.Howwelldoyouthinktheadolescentgroupleaderunderstoodyouradolescent’sneeds?notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐54.HowwelldoyouthinkyourgroupleaderimplementedtheMYmindprogram?notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐5C. GENERAL1.Pleasecommentonhowthisinterventionaffectedyouandyourfamily.
THANKYOUVERYMUCH

170
Adolescent Consumer Satisfaction Questionnaire
ThefollowingquestionnaireispartofourevaluationoftheMYmindprogramthatyouhavereceived.Itisimportantthatyouanswerashonestlyaspossible.Theinformationobtainedwillhelpustoevaluateandcontinuallyimprovetheprogramweoffer.Yourco‐operationisgreatlyappreciated!Pleasecircletheappropriateresponsethatbestexpresseshowyoufeel.D. THEOVERALLPROGRAM1.Howsatisfiedareyouwiththehelpyoureceived?very dissatisfied neutral satisfied verydissatisfied satisfied2.TowhatdegreehastheMYmindprogramhelpedyoutodealwithyourproblems?NotatallAlittleSomewhatQuiteabitAlot6. Ifeeltheapproachtotreatingadolescent’sADHDdifficultiesandparent‐
adolescentconflictusingthistypeoftrainingprogramis:very inappropriate neutral appropriate veryinappropriate appropriate7. TowhatextenthastheMYmindprogrammetyourneeds?none afew some many almostallofmyneeds ofmyneedsofmyneeds ofmyneeds ofmy
needs8. WouldyourecommendtheMYmindprogramtoafriendorrelative?not not neutral recommend stronglyrecommend recommend recommend strongly 14. TowhatdegreehastheMYmindprogramhelpedtoimproveyourADHD
symptomsoverall?

171
considerably worse the improved greatlyworse same improved
15. TowhatdegreehastheMYmindprogramhelpedtoimproveyourabilityto
manageyourstressoverall?
NotatallAlittleSomewhatQuiteabitAlot
16. TowhatdegreehastheMYmindprogramhelpedtoimproveyourrelationshipwithyourparent(e.g.,howyougetalong)?
NotatallAlittleSomewhatQuiteabitAlot
17. Towhatdegreehasthetreatmentprogramhelpedwithotherareasofyourlife
(e.g.,sports,school,personalproblems)?NotatallAlittleSomewhatQuiteabitAlotPleasebrieflydescribewhatthoseareaswere:
18. Howconfidentareyouinyourabilitytomanagefutureconflictswithyour
parentusingwhatyouhavelearnedfromthisprogram?notatall notvery neutral confident veryconfident confident confident19. Pleasewritedownanypartofservicesyoudidnotlike.
E. GROUPLEADER1.Howwelldoyouthinkyourgroupleaderlistenedtoyourconcern(s)?notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐52.Howwelldoyouthinkyourgroupleaderunderstoodyourconcerns?

172
notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐53.HowwelldoyouthinkyourgroupleaderimplementedtheMYmindprogram?notatallwell verywell 1‐‐‐‐‐‐‐‐‐2‐‐‐‐‐‐‐‐‐3‐‐‐‐‐‐‐‐‐4‐‐‐‐‐‐‐‐‐5F. GENERAL1.Pleasecommentonhowthisinterventionaffectedyouandyourfamily.
THANKYOUVERYMUCH

173
Appendix G
Supplementary GEE Analyses
Note. * p < .05. a Compared to Adolescent. b Compared to Follow-up. c Compared to Adolescent x Follow-up x Meditation Practice. d Compared to Adolescent x Follow-up x Time. e Compared to Parent x Follow-up. f Compared to Adolescent x Baseline. g Compared to Adolescent x Treatment.
Table G2 GEE Analyses: Examining the Relationship Between Stress and Meditation Practice while Controlling for Phase. Type of Predictor B SE B Wald χ2 Odds Ratio Intercept .77 .12 42.61* 2.16
Baselinea .30 .17 3.33 1.36
Treatmenta .26 .14 3.50 1.30
Meditation Practice -.08 .03 6.10* .93
Time .04 .01 .27 1.00
Baseline x Meditation Practiceb .02 .07 .12 1.02
Treatment x Meditation Practiceb .04 .04 .86 1.04
Table G1 GEE Analyses: Examining the Relationship Between Stress and Meditation Practice While Controlling for Adolescent/Parent Status and Phase
Type of Predictor B SE B Wald χ2
Odds Ratio Intercept .88 .20 19.42* 2.40 Parenta -.12 .24 .25 .89 Baselineb .4 .10 14.61* 1.49 Treatmentb .08 .14 .33 1.08 Meditation Practice -.17 .06 7.00* .85 Time .01 .02 .39 1.01 Parent x Baseline x Meditation Practice x Time .01 .01 2.62 1.01 Parent x Treatment x Meditation Practice x Time .00 .00 .01 1.00 Parent x Follow-up x Meditation Practice x Time .00 .00 .20 1.00 Adolescent x Baseline x Meditation Practice x Time .01 .012 .83 1.01 Adolescent x Treatment Meditation Practice x Time .00 .00 .74 1.00 Adolescent x Follow-up x Meditation Practice x Time -.00 .01 .02 .999 Parent x Baseline x Meditation Practice .13 .09 2.14 1.14 Parent x Treatment x Meditation Practice .10 .07 1.926 1.108 Parent x Follow-up x Meditation Practice .12 .07 2.62 1.12 Adolescent x Baseline x Meditation Practicec -.04 .07 .31 .96 Adolescent x Treatment x Meditation Practicec .14 .04 10.51* 1.15 Parent x Baseline x Time -.03 .02 1.55 .97 Parent x Treatment x Time -.02 .02 .70 .99 Parent x Follow-up x Time -.01 .02 .40 .99 Adolescent x Baseline x Timed -.04 .02 4.09* .97 Adolescent x Treatment x Timed -.02 .01 1.84 .98 Parent x Baselineef -.13 .25 .26 .88 Parent x Treatmenteg .30 .23 1.82 1.35

174
Baseline x Timec -.02 .02 1.99 .98
Treatment x Timec -.01 .01 1.57 .99
Meditation Practice x Time .00 .00 .01 1.00
Baseline x Meditation Practice x Timed .01 .01 1.10 1.01
Treatment x Meditation Practice x Timed -1.23E-05 .00 .00 1.00
Note. * p < .05. a Compared to Follow-up. b Compared to Follow-up x Meditation Practice. c Compared to Follow-up x Time. d Compared to Follow-up x Meditation Practice x Time.







