
V. Ferraresi Divisione di Oncologia Medica 1
Il parere dell’esperto
Melanoma

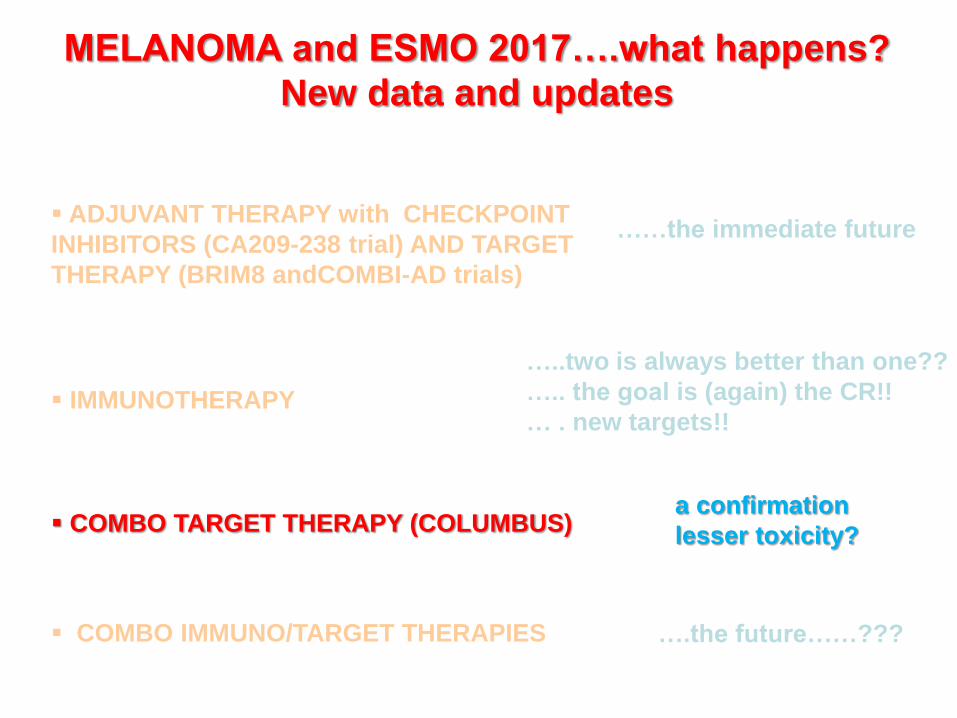
MELANOMA and ESMO 2017….what happens?
New data and updates
COMBO IMMUNO/TARGET THERAPIES
….the future……???
IMMUNOTHERAPY
…..two is always better than one??
….. the goal is (again) the CR!!
…. new targets!!
COMBO TARGET THERAPY (COLUMBUS) a confirmation
lesser toxicity?
ADJUVANT THERAPY with CHECKPOINT
INHIBITORS (CA209-238 trial) AND TARGET
THERAPY (BRIM8 and COMBI-AD trials)
….the immediate future
MELANOMA and ESMO 2017….what happens?
New data and updates
COMBO IMMUNO/TARGET THERAPIES
….the future……???
IMMUNOTHERAPY
…..two is always better than one??
….. the goal is (again) the CR!!
…new targets!!
COMBO TARGET THERAPY (COLUMBUS) a confirmation
lesser toxicity?
ADJUVANT THERAPY with CHECKPOINT
INHIBITORS (CA209-238) AND TARGET
THERAPY (BRIM8, COMBI-AD)
…..the immediate future

ESMO 2017 and MELANOMA
IPI10 vs NIVO3
DABR+TRAM vs placebo
VEM vs placebo

OS data immature
COMBI-AD
CA 209-038
BRAF mutated pts: about 40%
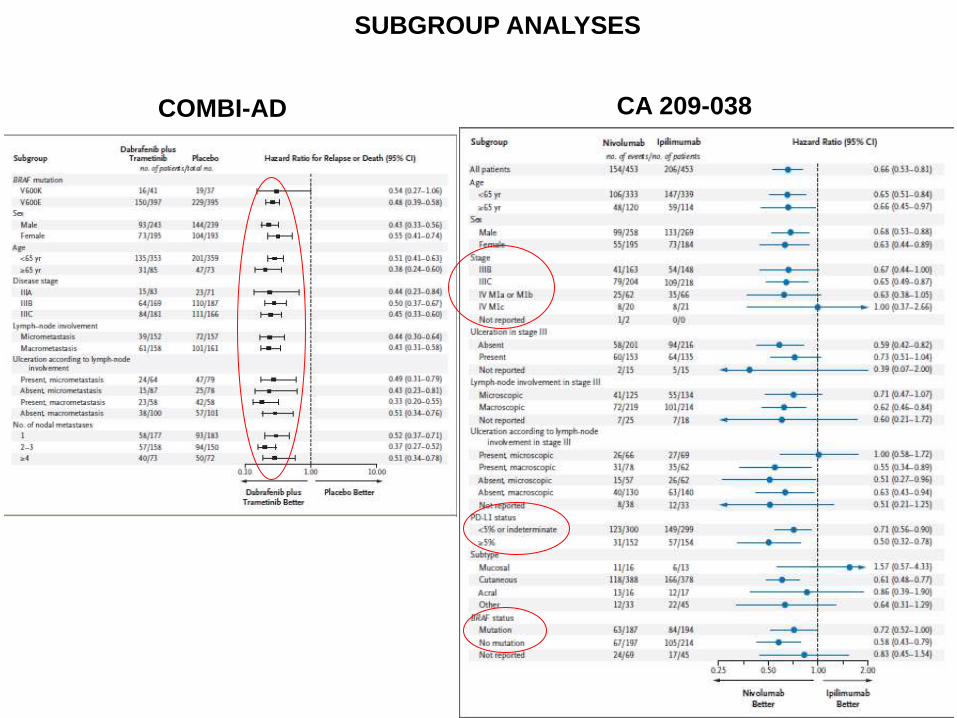
SUBGROUP ANALYSES
COMBI-AD CA 209-038

EORTC 18071
No stratification according to BRAF status
HR= 0.86, CI 0.81-0.91; P < 0.00001
HR = 0.90, CI 0.85-0.97; P = 0.003
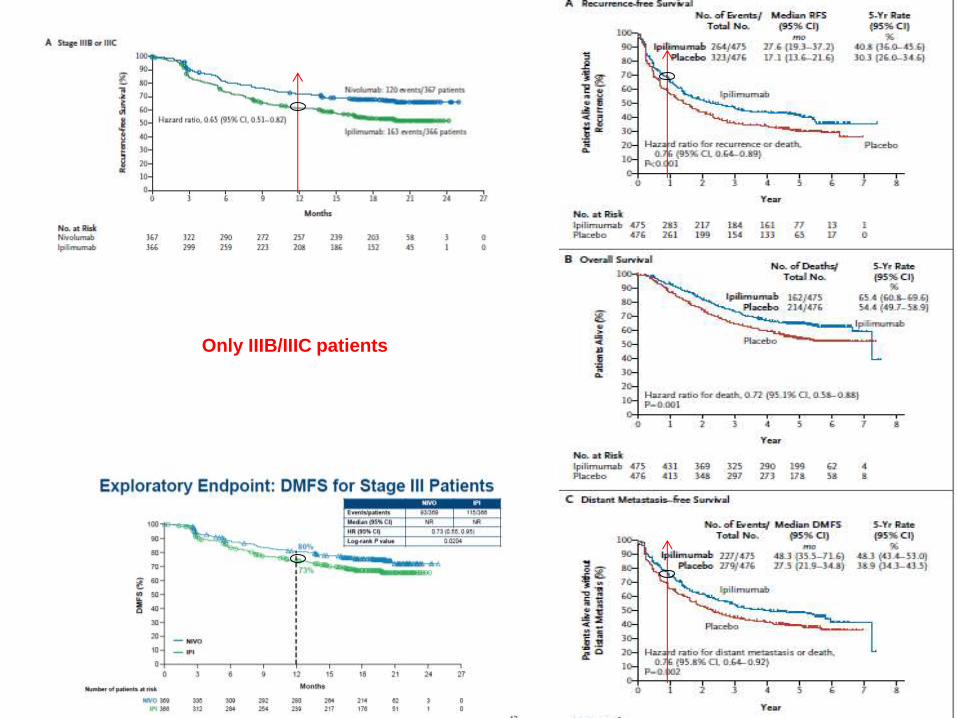
Only IIIB/IIIC patients
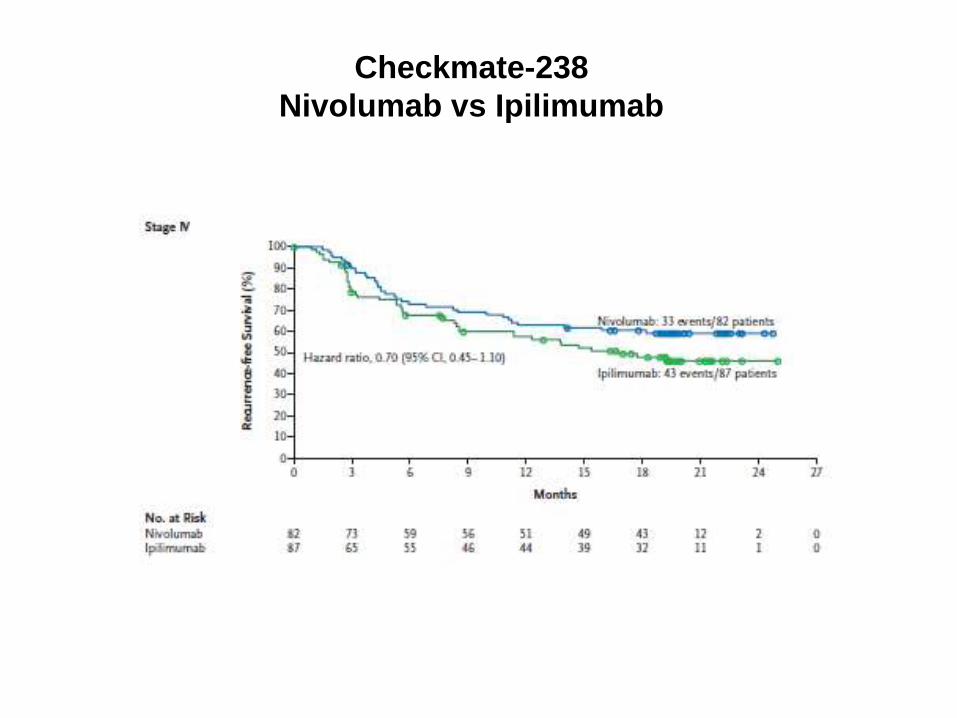
Checkmate-238
Nivolumab vs Ipilimumab
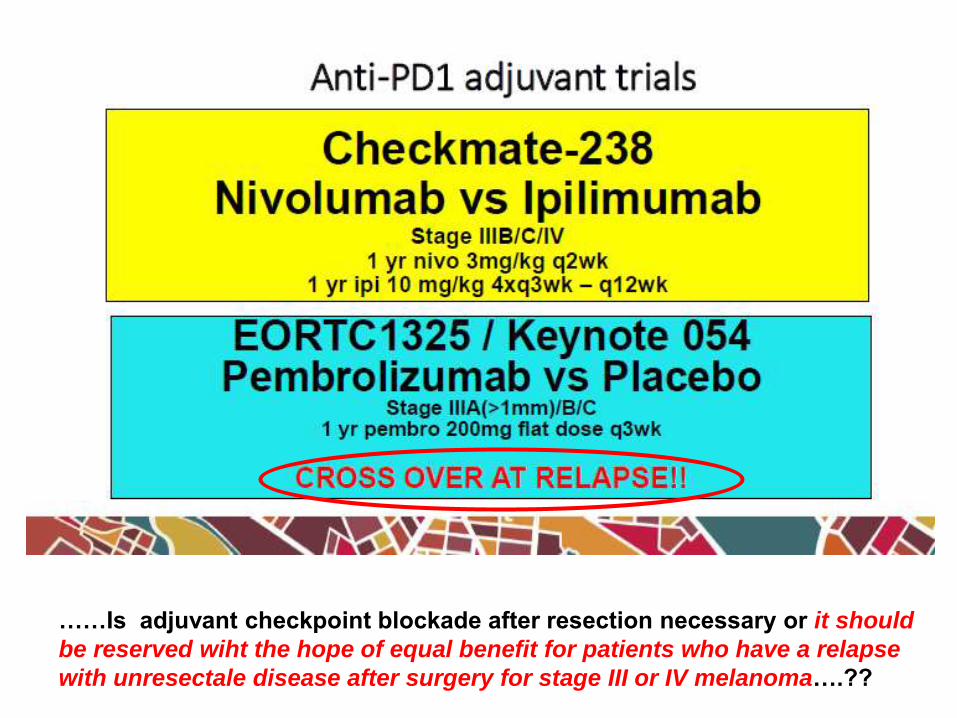
……Is adjuvant checkpoint blockade after resection necessary or it should
be reserved wiht the hope of equal benefit for patients who have a relapse
with unresectale disease after surgery for stage III or IV melanoma….??

An Investigational Immuno-therapy Study of Nivolumab Combined With
Ipilimumab Compared to Nivolumab by Itself After Complete Surgical
Removal of Stage IIIb/c/d or Stage IV Melanoma (NCT 03068455)
CheckMate 915
IPI alone arm eliminated
Recruiting
Italy partecipation pending….

MELANOMA ADJUVANT THERAPY with CHECKPOINT INHIBITORS AND TARGET THERAPY
BRAF inhibitors alone: is there a future…???
BRAFi/MEKi combo (COMBI-AD trial): clear RFS, DMFS and OS benefit
in all stages. The new “standard” for BRAF mutated patients?
anti-PD1: Pending OS data
q2wks NIVO vs q3wks flat PEMBRO
End of adjuvant IPI10mg/kg (FDA approval): more toxic and less active
than NIVO, “light dose” in combo with NIVO in ongoing trials
Differences in population characteristics (stage, BRAF status):
comparisons methodologically not correct
ESMO 2017
Neoadjuvant + adjuvant treatment with combo immuno or combo
target therapy
high % of ORR (80-100%) and pCR (40-50%)
improve locoregional control??
avoid TLND in pts with palpable nodes??

MELANOMA and ESMO 2017….what happens?
New data and updates
COMBO IMMUNO/TARGET THERAPIES
….the future……???
IMMUNOTHERAPY
…..two is always better than one??
….. the goal is (again) the CR!!
…. new targets!!
COMBO TARGET THERAPY (COLUMBUS) a confirmation
lesser toxicity?
ADJUVANT THERAPY with CHECKPOINT
INHIBITORS (CA209-238 trial) AND TARGET
THERAPY (BRIM8 andCOMBI-AD trials)
…..the immediate future
17
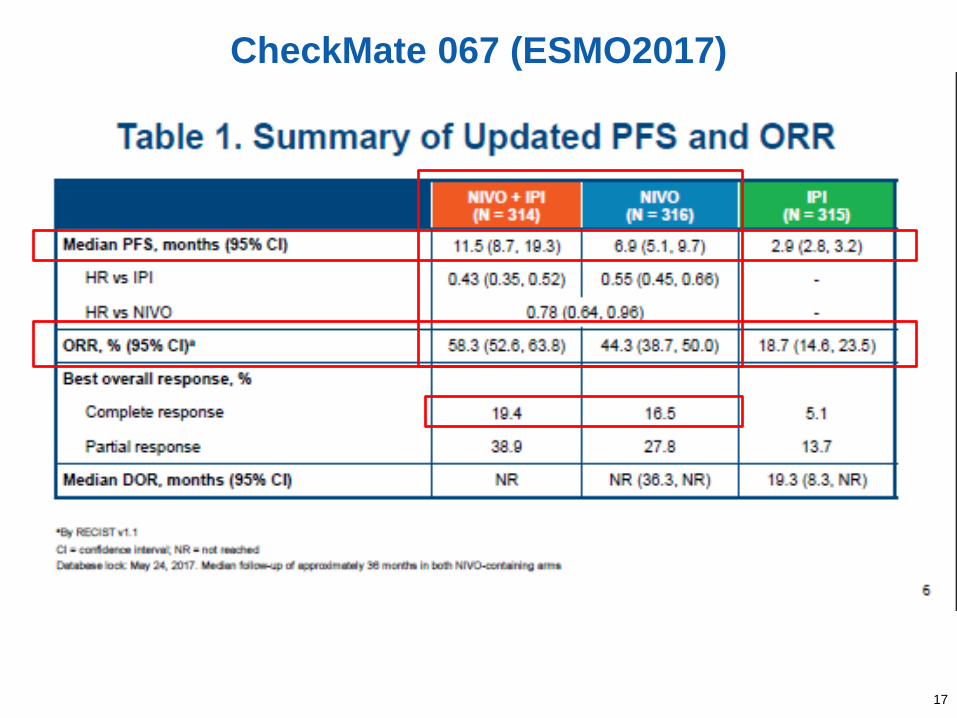
CheckMate 067 (ESMO2017)
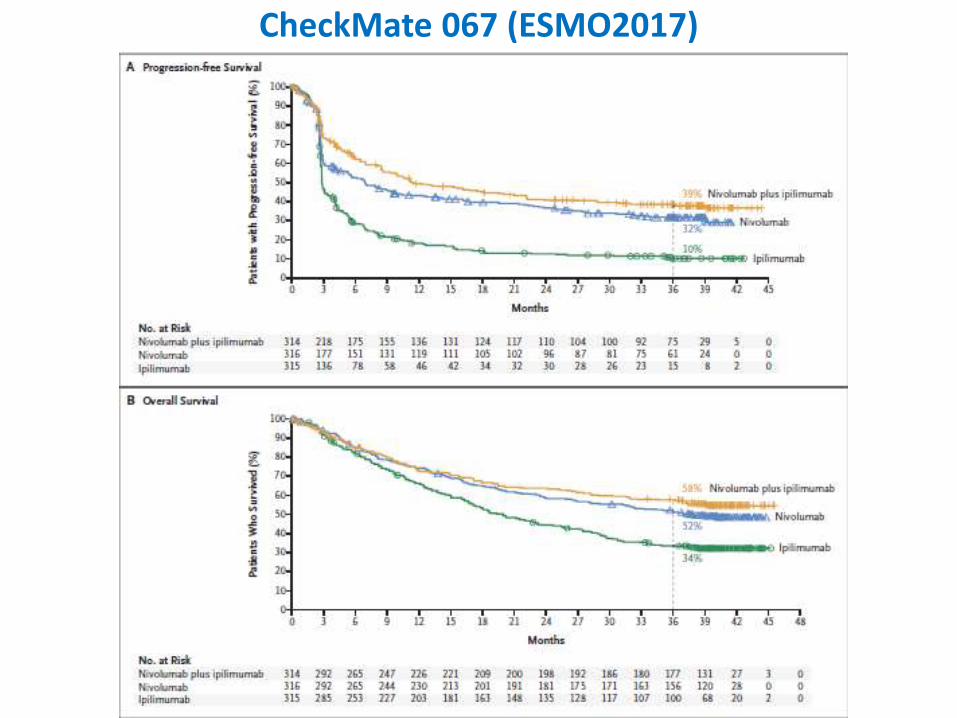
CheckMate 067 (ESMO2017)
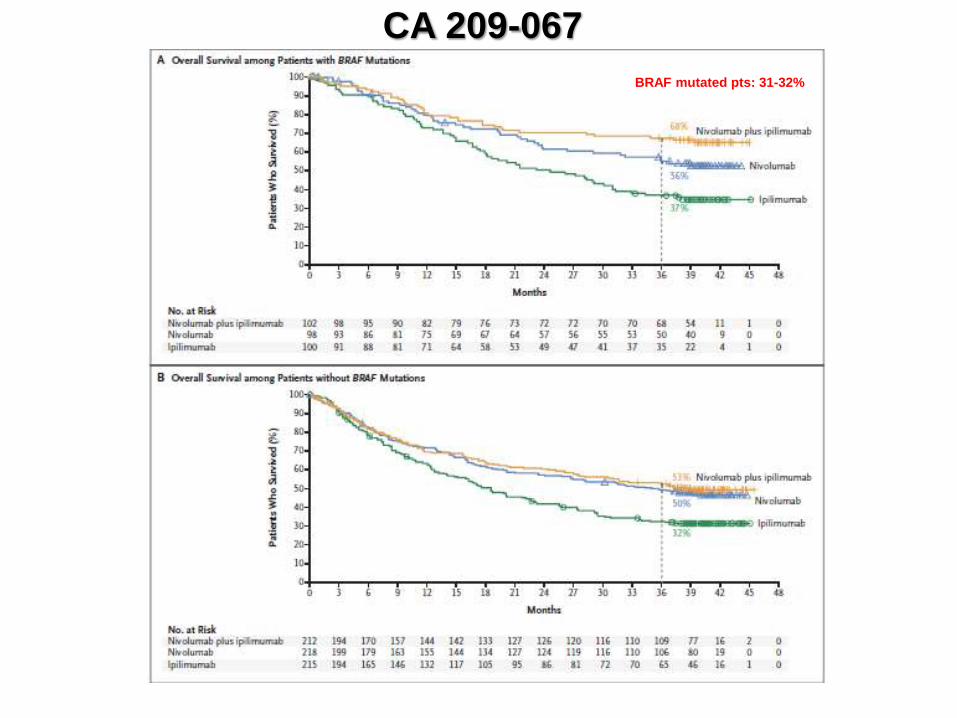
CA 209-067
BRAF mutated pts: 31-32%
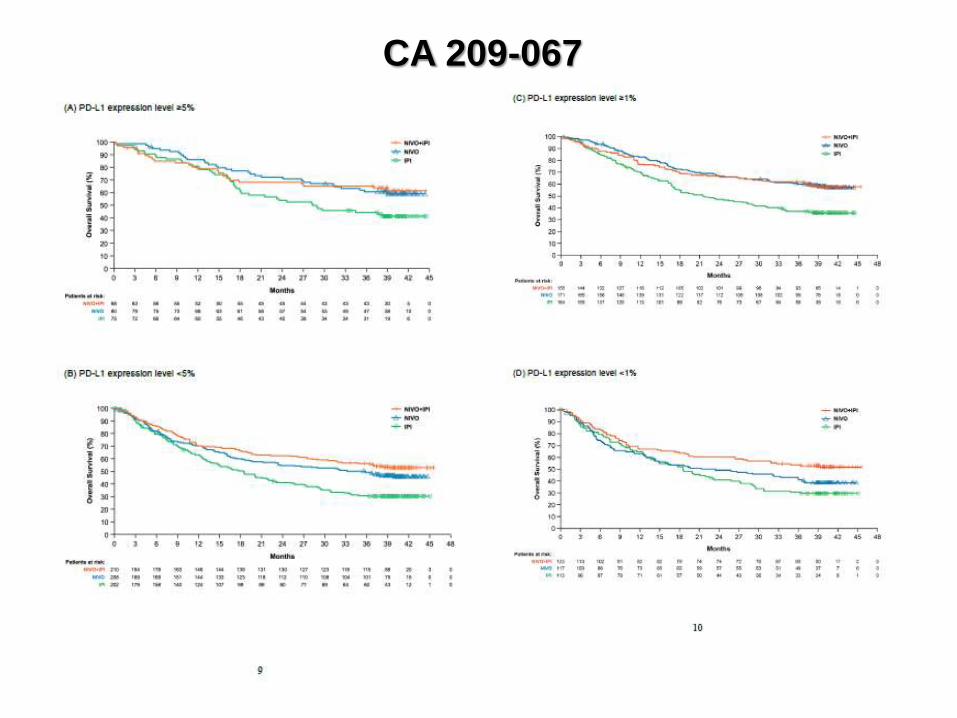
CA 209-067
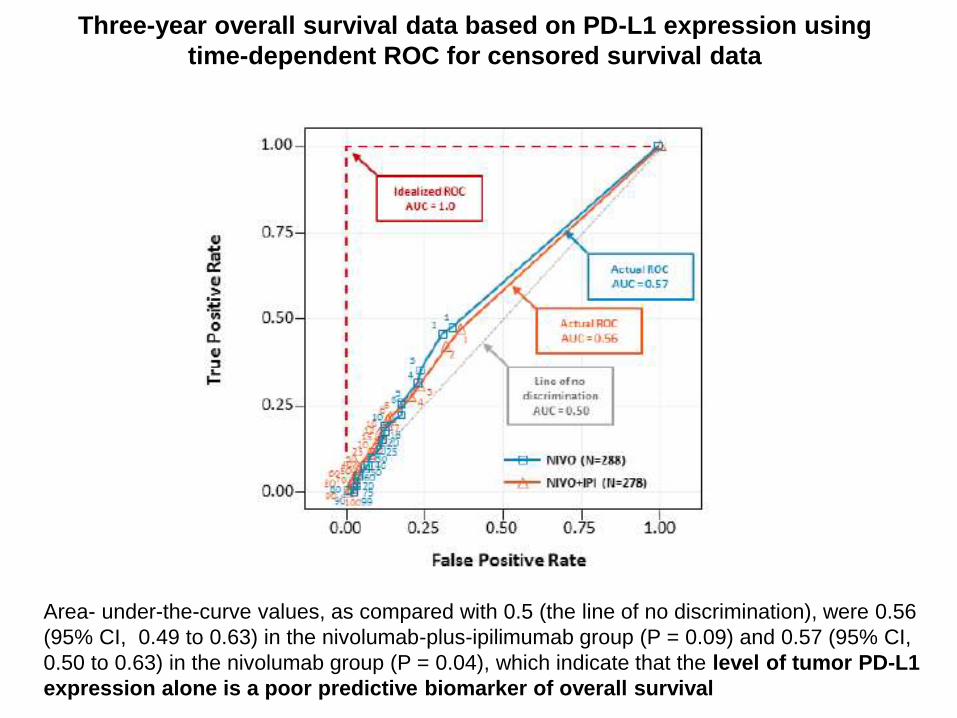
Three-year overall survival data based on PD-L1 expression using
time-dependent ROC for censored survival data
Area- under-the-curve values, as compared with 0.5 (the line of no discrimination), were 0.56
(95% CI, 0.49 to 0.63) in the nivolumab-plus-ipilimumab group (P = 0.09) and 0.57 (95% CI,
0.50 to 0.63) in the nivolumab group (P = 0.04), which indicate that the level of tumor PD-L1
expression alone is a poor predictive biomarker of overall survival
PD-L1: starting point for discussion with patients for combo IPI/NIVO
versus NIVO (if we don’t need the “response” to palliate symptoms
and if you have “favorite” sites of disease……)
BRAF mutation status and combo immunotherapy IPI/NIVO:
we need more data on patients’ characteristics (bias of selection?)
no head-to-head comparison versus combo target therapy
role of subsequent lines of therapy
toxicity as a point for discussion with patients (% G3-4 toxicities)
NIVOLUMAB/IPILIMUMAB combo
What to say……awaiting the regimen?

Classifying Cancers Based onT-cell Infiltration and PD-L1 - Melanoma
Teng MWL, Cancer Research 2015
~40% ~40%
~20% ~1%

Potential Role of LAG-3 in T-Cell Exhaustion and Anti–PD-1 Resistance
34
PD-L1
LAG-3
MHC II Effector
CD4+/CD8+
T cell
Acquired
resistance
Tumor or other
infiltrating cell
+ Antigen
PD-1
PD-1
LAG-3 MHC II
PD-L1
PD-1
+Nivolumab + Nivolumab
+ Relatlimab
+ Nivolumab
+ Relatlimab
I-O therapy naive:
LAG-3 may limit I-O
response
I-O therapy
experienced:
LAG-3 may contribute
to resistance
• LAG-3 regulates a checkpoint pathway that limits the activity of T cells1
• LAG-3 and PD-1 receptors are overexpressed and/or co-expressed on tumor-infiltrating lymphocytes in melanoma2,3
Nivolumab
Relatlimab
(BMS-986016/anti–LAG-3)
I-O, immuno-oncology; MHC II, major histocompatibility complex class II; PD-1, programmed death-1; PD-L1, programmed death ligand 1.
1. Grosso JF et al. J Clin Invest. 2007;117:3383‒3392. 2. Goding SR et al. J Immunol. 2013;190:4899–
4909. 3. Taube JM et al. Clin Cancer Res. 2015;21:3969–3976.

Relatlimab (anti-LAG3) + Nivolumab
35
Mel Prior PD-(L)1a
All
n = 61
LAG-3 ≥ 1%b
n = 33
ORR, n (%)c
95% CI 7 (11.5)d
4.7, 22
6 (18)d
7, 35.5
BOR, n (%)c
CR 1 (1.6) 1 (3.0)
PR 6 (9.8)d 5 (15)d
SD 23 (38) 15 (45)
PD 25 (41) 8 (24)
Clinical progressione 6 (9.8) 4 (12)
DCR (CR + PR + SD), n (%)c
95% CI 30 (49)
36, 62
21 (64)
45, 80
PD1/PD-L1 resistant patients (46% PD as
best response, 77% > 2 prior lines)
LAG-3 expression (≥ 1%) enriched for response
Median duration of response was not reached
(range, 0.1+ to 39+)
All Patientsa
N = 270
Any
Grade
n (%)
Grade 3–
4
n (%)
Any TRAEb 137 (51) 27 (10)
TRAEs in ≥ 5% of patients
Fatigue 30 (11) 0
Pruritus 19 (7.0) 0
Diarrhea 18 (6.7) 3 (1.1)
Arthralgia 17 (6.3) 0
Infusion-related reaction 15 (5.6) 0
Any serious TRAEb 18 (6.7) 12 (4.4)
Serious TRAEs in > 1 patient
Colitis 4 (1.5) 3 (1.1)
Pneumonitis 2 (0.7) 2 (0.7)
Myocarditisc 2 (0.7) 0
Pyrexia 2 (0.7) 0
Any TRAE leading to discontinuationb 11 (4.1) 8 (3.0)
PD-1/PD-L1 resistant/refractory melanoma pts t

37
Pink: PD-L1 ≥ 1% Blue: PD-L1 < 1% Gray: PD-L1 unknown
100
80
60
40
20
0
-20
-40
-60
-100
-80
100
80
60
40
20
0
-20
-40
-60
-100
-80
100
80
60
40
20
0
-20
-40
-60
-100
-80
37
45% with
tumor
reduction
24% with
tumor
reduction
13% with
tumor
reduction
Best
perc
en
t c
han
ge i
n s
um
of
targ
et
lesio
n d
iam
ete
rs f
rom
baselin
ea,b
aSix patients with clinical progression prior to their first scan and 1 with PD due to a new symptomatic brain metastasis prior to getting full
scans were not included. bOne patient with best change from baseline > 30% had a best response of SD.
LAG-3 ≥ 1% n = 29
LAG-3 < 1% n = 17
LAG-3
Unknown n = 8
RELATLIMAB – PD-1/PD-L1 resistant/refractory melanoma pts
Best Change in Target Lesion Size by LAG-3 and PD-L1 Expression
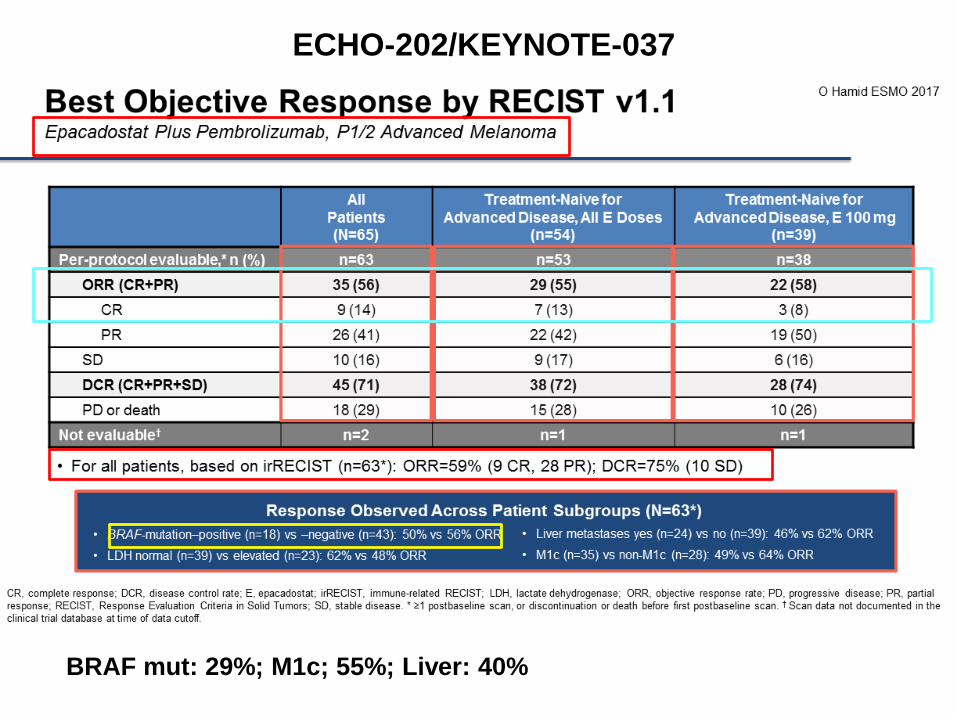
BRAF mut: 29%; M1c; 55%; Liver: 40%
ECHO-202/KEYNOTE-037

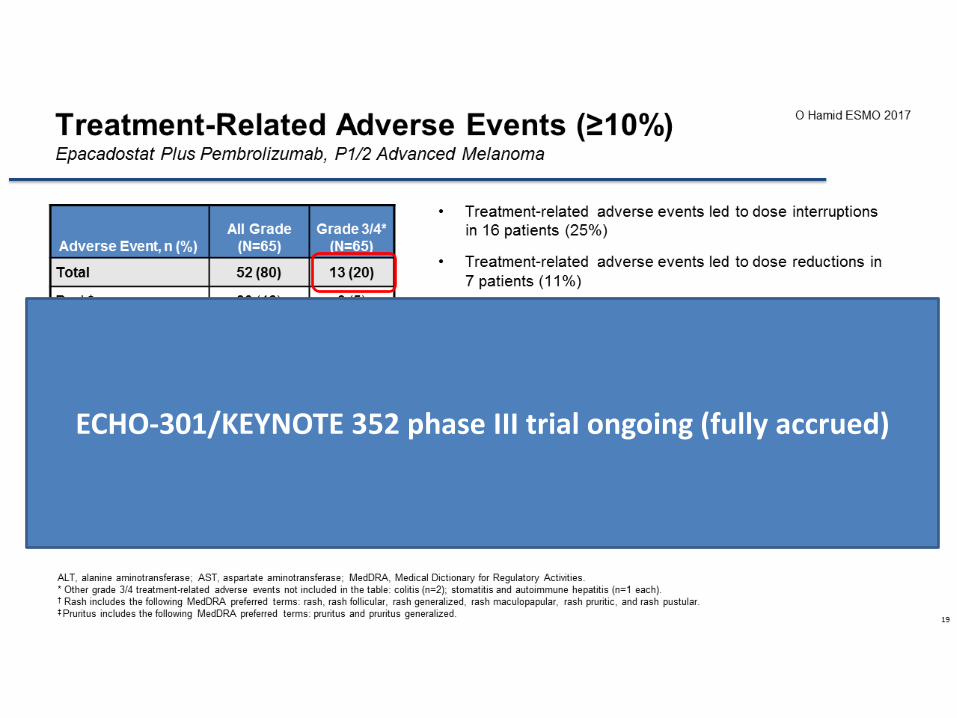
ECHO-301/KEYNOTE 352 phase III trial ongoing (fully accrued)
MELANOMA and ESMO 2017….what happens?
New data and updates
COMBO IMMUNO/TARGET THERAPIES
….the future……???
IMMUNOTHERAPY
…..two is always better than one??
….. the goal is (again) the CR!!
… . new targets!!
COMBO TARGET THERAPY (COLUMBUS) a confirmation
lesser toxicity?
ADJUVANT THERAPY with CHECKPOINT
INHIBITORS (CA209-238 trial) AND TARGET
THERAPY (BRIM8 andCOMBI-AD trials)
……the immediate future


BRAF + MEK Inhibitor Combination Treatment Phase 3 Studies: Adverse Events of Special Interest
COMBI-d1 COMBI-v2 coBRIM3
Study Agent(s) Dabrafenib + Trametinib
Dabrafenib Dabrafenib + Trametinib
Vemurafenib Vemurafenib +
Cobimetinib Vemurafenib
Patients, n (study arm) 209 211 350 349 254 239
AEs of interest, %
CuSCC/KA 2 9 1 18 3 11
Skin papilloma 1 21 2 23 --- ---
Hyperkeratosis 3 32 4 25 10 28
Photosensitivity reaction --- --- 4 22 28 15
Decreased ejection fraction 4 2 8 0 7 3
Hypertension 22 14 26 24 --- ---
Chorioretinopathy < 1 < 1 1 < 1 12 < 1
Hand-foot syndromeb 5 27 4 25 --- ---
Increased ALT 11 5 14 17 24 18
Increased AST 11 3 11 13 22 13
Retinal detachment --- --- --- --- 8 0
QT interval prolongation --- --- --- --- 4 5
COLUMBUS ESM0 2017
- Lower incidence of pyrexia and dermatological toxicity - Higher incidence of hepatic toxicity not confirmed in phase III trial

(1% due to tox)

MELANOMA and ESMO 2017….what happens?
New data and updates
COMBO IMMUNO/TARGET THERAPIES
….the future……???
IMMUNOTHERAPY
…..two is always better than one??
….. the goal is (again) the CR!!
…new targets!!
COMBO TARGET THERAPY (COLUMBUS) a confirmation
lesser toxicity?
ADJUVANT THERAPY with CHECKPOINT
INHIBITORS (CA209-238 trial) AND TARGET
THERAPY (BRIM8 andCOMBI-AD trials)
……the immediate future

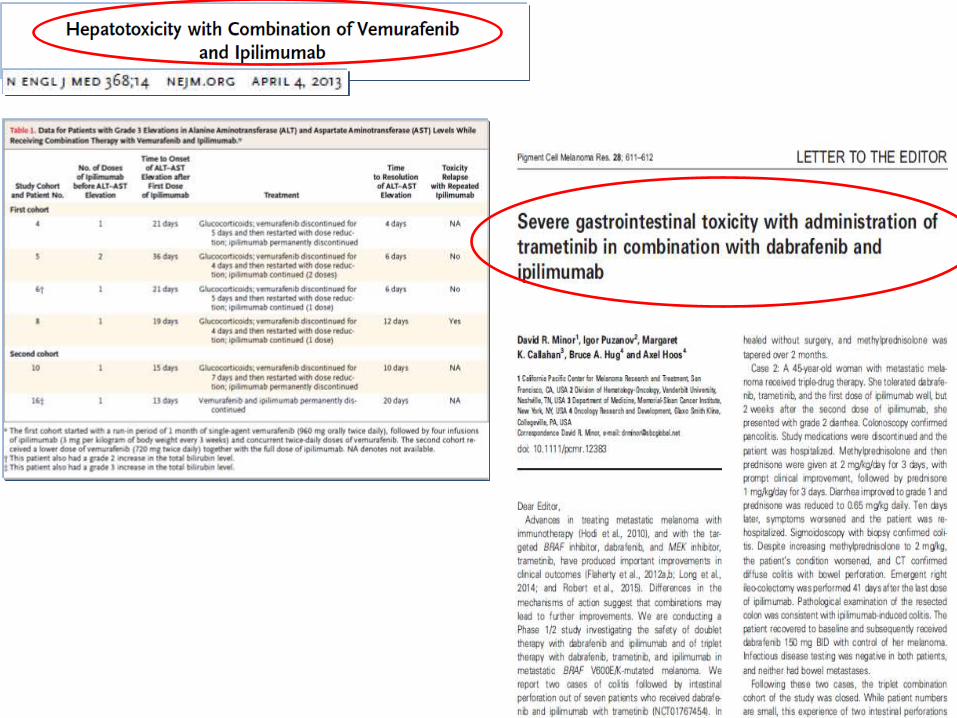
TARGETED THERAPIES AND IMMUNOTHERAPIES
HOW TO USE THESE AGENTS TOGETHER?
SEQUENCES???
after progression?
at predefinite time?
CONCURRENT COMBINATIONS???
METASTATIC MELANOMA
BRAF MUTATED DISEASE

BRAF inhibitors and immune system



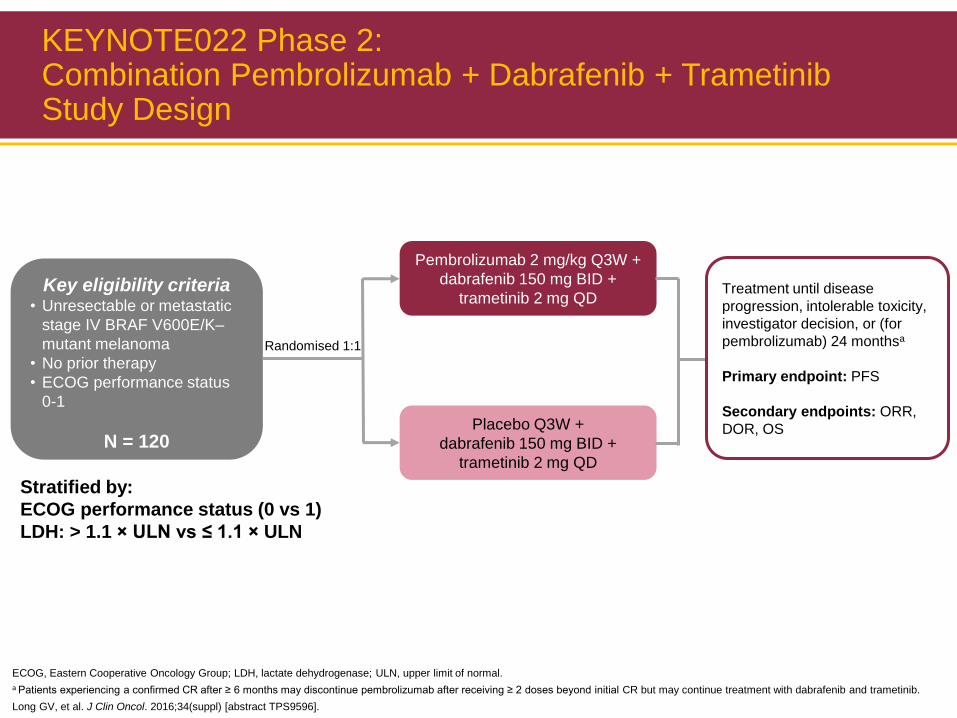
KEYNOTE022 Phase 2: Combination Pembrolizumab + Dabrafenib + Trametinib Study Design
Key eligibility criteria • Unresectable or metastatic
stage IV BRAF V600E/K–
mutant melanoma
• No prior therapy
• ECOG performance status
0-1
N = 120
Randomised 1:1
Pembrolizumab 2 mg/kg Q3W +
dabrafenib 150 mg BID +
trametinib 2 mg QD
Placebo Q3W +
dabrafenib 150 mg BID +
trametinib 2 mg QD
Treatment until disease
progression, intolerable toxicity,
investigator decision, or (for
pembrolizumab) 24 monthsa
Primary endpoint: PFS
Secondary endpoints: ORR,
DOR, OS
Stratified by:
ECOG performance status (0 vs 1)
LDH: > 1.1 × ULN vs ≤ 1.1 × ULN
ECOG, Eastern Cooperative Oncology Group; LDH, lactate dehydrogenase; ULN, upper limit of normal.
a Patients experiencing a confirmed CR after ≥ 6 months may discontinue pembrolizumab after receiving ≥ 2 doses beyond initial CR but may continue treatment with dabrafenib and trametinib.
Long GV, et al. J Clin Oncol. 2016;34(suppl) [abstract TPS9596].
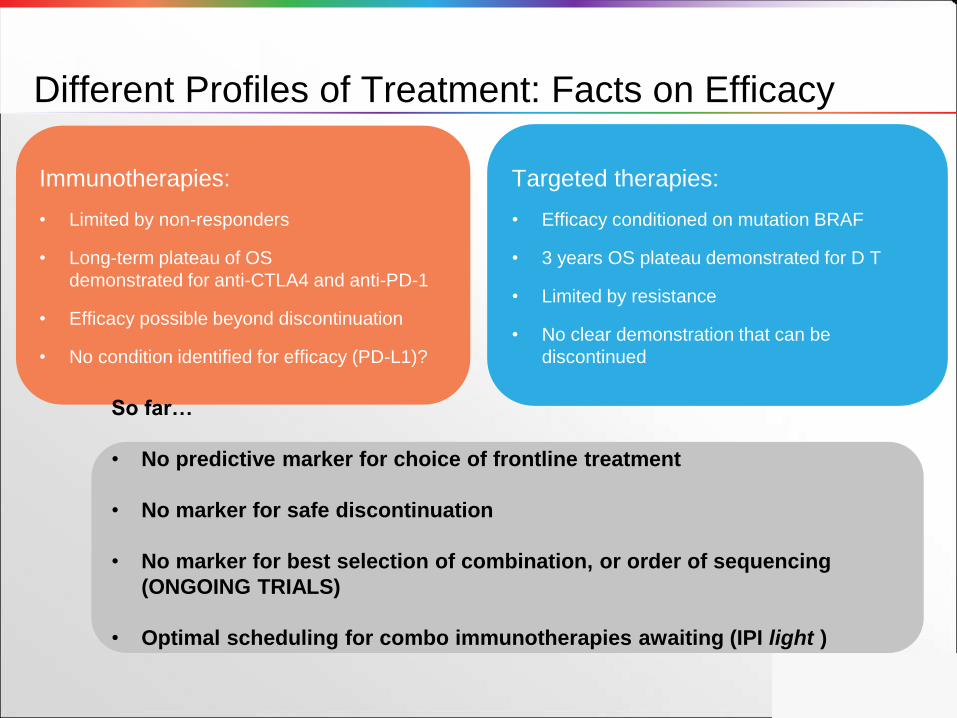
Immunotherapies:
• Limited by non-responders
• Long-term plateau of OS
demonstrated for anti-CTLA4 and anti-PD-1
• Efficacy possible beyond discontinuation
• No condition identified for efficacy (PD-L1)?
Targeted therapies:
• Efficacy conditioned on mutation BRAF
• 3 years OS plateau demonstrated for D T
• Limited by resistance
• No clear demonstration that can be
discontinued
So far…
• No predictive marker for choice of frontline treatment
• No marker for safe discontinuation
• No marker for best selection of combination, or order of sequencing
(ONGOING TRIALS)
• Optimal scheduling for combo immunotherapies awaiting (IPI light )
Different Profiles of Treatment: Facts on Efficacy

Immunotherapies:
• “Natural”: exploit endogenous immune
system to eradicate cancer
• Slow
• Exclude fast progressions
• Long response
Targeted therapies:
• “Artificial”: precision/perzonalized medicine
• Fast
• More active in case of fast progression
• Resistance sooner or later
Different Profiles of Treatment: Perceptions....... Truth is different than perception
• All treatments are less active when the disease is
aggressive and fast (eg, high LDH)
• Anti-PD-1+CTLA4 inhibitors work nearly as fast as
targeted therapies
• Targeted therapies can provide very long survival
• Different profiles of toxicities (…and combo
TT/IT)
• What to do? AWAIT THE RESULTS OF CLINICAL
TRIALS!
• Outside an investigational trial we must still be
guided by patients and disease characteristics

Grazie
Melanoma treatment







