Maternal-fetal biomarkers of
prenatal exposure to ethanol
Simona Pichini
National Observatory on Alcohol, tobacco,
smoking, doping and gambling
Istituto Superiore di Sanità
Rome, Italy

Indirect Maternal biomarkers of gestational ethanol consumption
• -Interview with the mother (the most used,
the most unreliable!)
-Ethanol concentrations in expired air, blood
and urine (very rare)
- Glutamyltransferase (GGT)
-Aspartate aminotransferase (AST)
-Mean corpuscular volume (MCV)
-N-Acetyl-β-Hexosaminidase (Beta-Hex)
-apolipoprotein J
-Total sialic acid
-Hydroxytryptophol 5-(5-HTOL)
-Phosphatidyl Ethanol (PEth)
-Carbohydrate Deficient Transferrin (CDT)
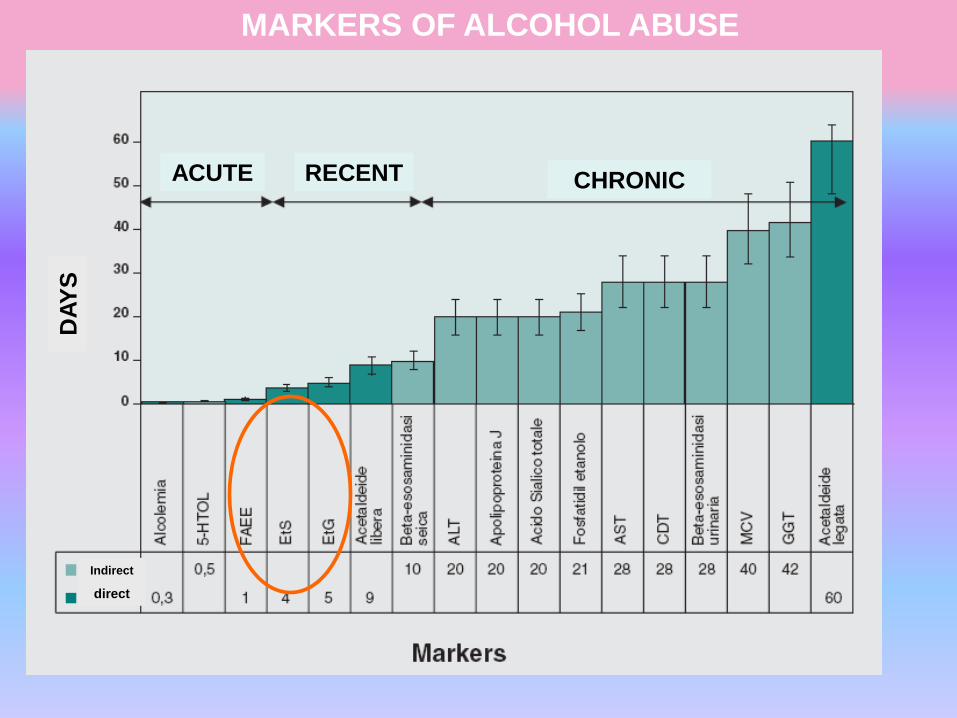
ACUTE RECENT CHRONIC
DA
YS
Indirect
direct
MARKERS OF ALCOHOL ABUSE
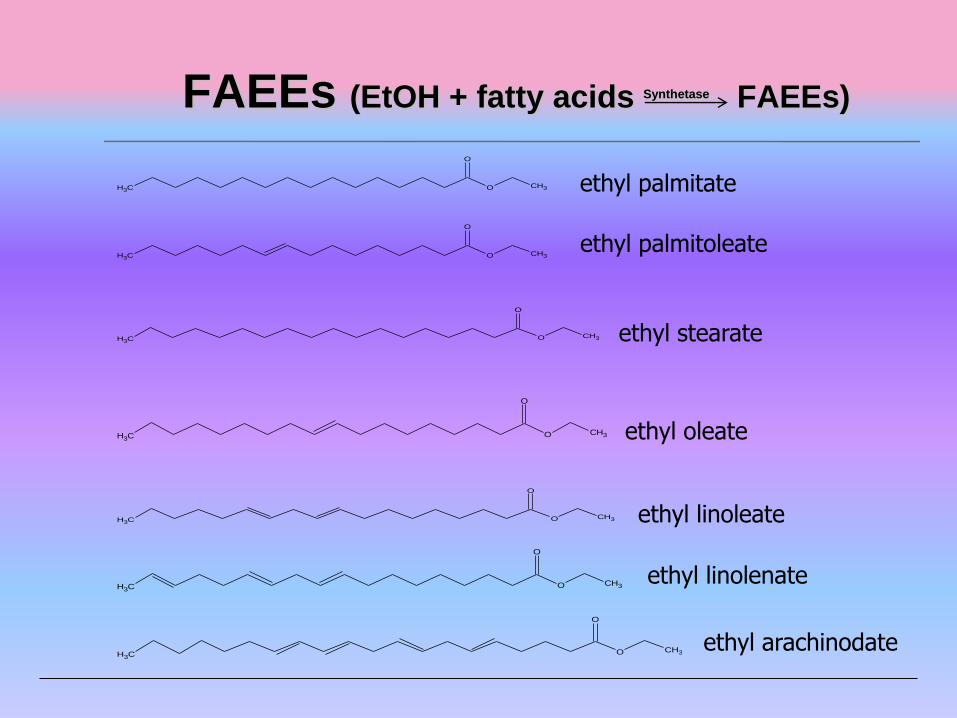
FAEEs (EtOH + fatty acids Synthetase FAEEs)
O
O
CH3CH3
O
O
CH3CH3
O
O
CH3CH3
O
O
CH3CH3
O
O
CH3CH3
O
O
CH3CH3
O
O
CH3CH3
ethyl palmitate
ethyl palmitoleate
ethyl stearate
ethyl oleate
ethyl linoleate
ethyl linolenate
ethyl arachinodate
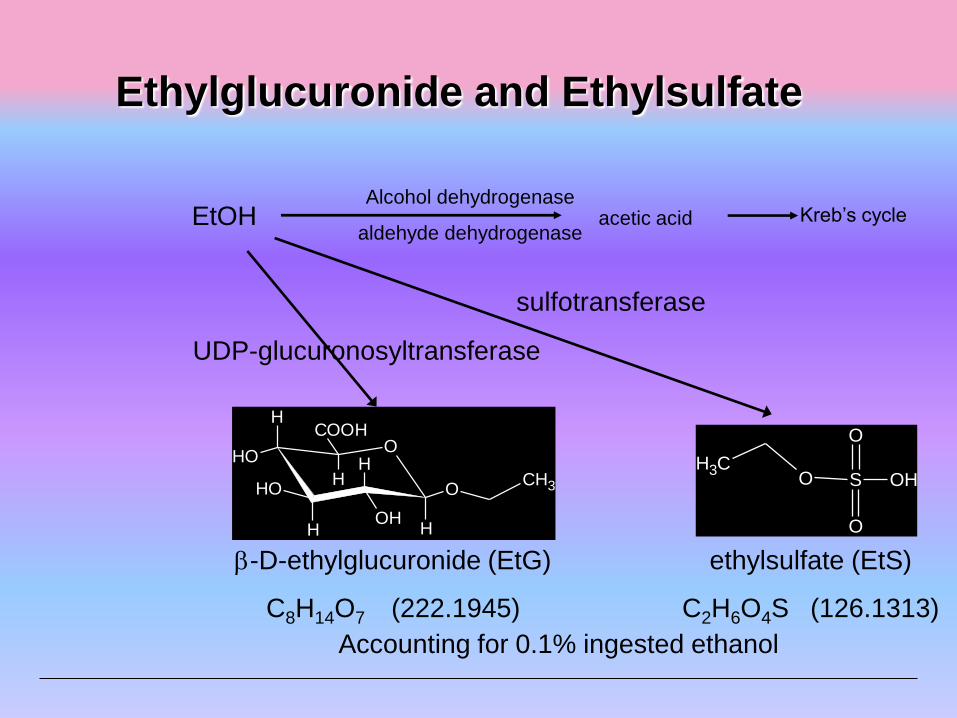
Ethylglucuronide and Ethylsulfate
EtOH
CH3
O
HOH
HH
H
H
OOH
OH
COOH
UDP-glucuronosyltransferase
-D-ethylglucuronide (EtG)
C8H14O7 (222.1945)
S OH
O
O
OCH3
sulfotransferase
ethylsulfate (EtS)
C2H6O4S (126.1313)
Alcohol dehydrogenase
aldehyde dehydrogenase acetic acid Kreb’s cycle
Accounting for 0.1% ingested ethanol
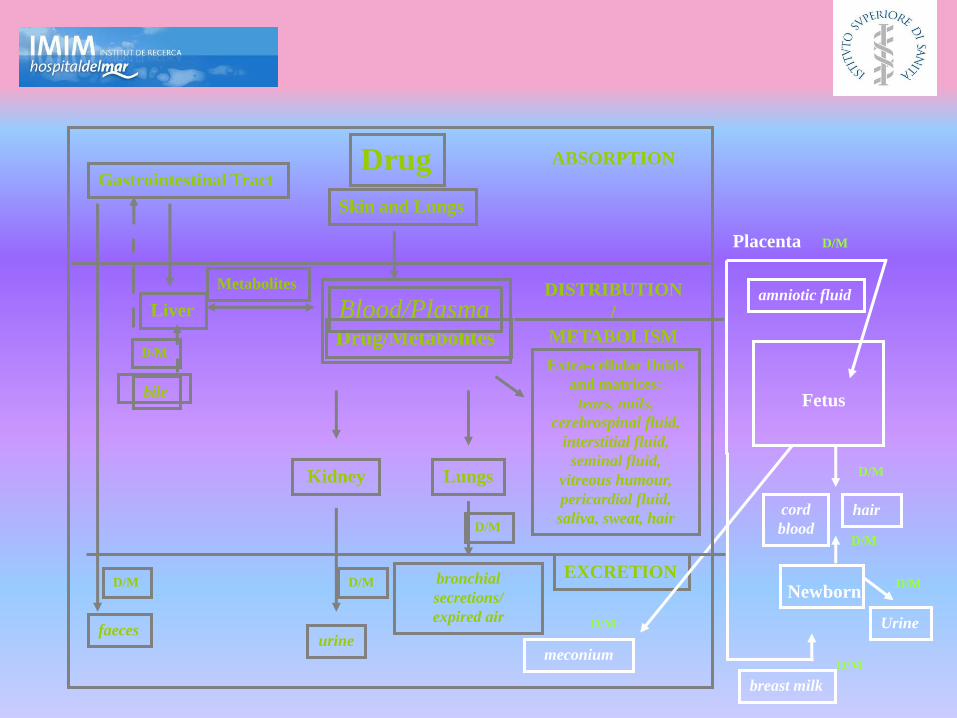
Placenta
Fetus
ABSORPTION
DISTRIBUTION
/
METABOLISM
EXCRETION
cord
blood
meconium
Newborn
breast milk
hair
Drug
Drug/Metabolites
Blood/Plasma
Gastrointestinal Tract
faeces
Skin and Lungs
bronchial
secretions/
expired air
Liver
bile
Lungs
Extra-cellular fluids
and matrices:
tears, nails,
cerebrospinal fluid,
interstitial fluid,
seminal fluid,
vitreous humour,
pericardial fluid,
saliva, sweat, hair
amniotic fluid
Kidney
urine
Metabolites
D/M
D/M D/M
D/M
D/M
D/M
D/M
D/M
D/M Urine
D/M

Direct ethanol metabolites in maternal biological
matrices
• Fatty acid ethyl esters (FAEEs).
• - FAEEs in blood account for acute consumption.
• - FAEEs in hair account for chronic consumption as
a function of hair length and segmental analysis
(performed only in two labs worldwide).
• Ethyl glucuronide (EtG) and Ethyl sulfate (EtS).
• - EtG and EtS in blood account for recent
consumption.
• - EtG and EtS in urine increase the window of
detection to the previous 3-4 days.
• - EtG and EtS in hair account for chronic
consumption as a function of hair length and
segmental analysis

Biological Matrices
related to gestation-
delivery-neonatal
period
Amniotic Fluid
Placenta
Fetal hair
Meconium
Cord blood
Neonatal urine

Ethyl glucuronide and ethyl sulfate in placenta and fetal tissues
by LC-MS/MS: biomarkers of placental ethanol transport
Luca Morini*1, Maria Falcón2, Simona Pichini3, Oscar Garcia-
Algar4, Paolo Danesino1, Angelo Groppi1 and Aurelio Luna2
1Department of Legal Medicine, Forensic and Pharmaco-Toxicological Science, University of Pavia, Italy; 2Deparment of Legal Medicine, Universidad de Murcia, Murcia, Spain; 3Istituto Superiore di Sanità, Rome, Italy; 4Unitat de Recerca Infancia i Entorn (URIE), Institut Municipal d’Investigació Mèdica-Hospital del Mar, Barcelona, Spain.

Real samples
EtG EtS Placenta
ng/g
Fetal Tissues
ng/g
Hair
pg/g
Placenta
ng/g
Fetal Tissues
ng/g
S 1-S5 <LOD <LOD <LOD <LOD <LOD
S6 1305.8 391.0 59.0 125.6 50.7
S7-S16 <LOD <LOD <LOD <LOD <LOD
S17 122.2 33.2 <LOD 9.6 <LOQ
S18-S20 <LOD <LOD N/D <LOD <LOD
S21 <LOD <LOD N/D 28.9 <LOD
S22-S25 <LOD <LOD N/D <LOD <LOD
S26 436.7 234.3 N/D 91.5 60.4
S27-S28 <LOD <LOD N/D <LOD <LOD
S29 <LOD <LOD N/D 175.6 <LOD
S30-S32 <LOD <LOD N/D <LOD <LOD
S33 215.2 79.2 N/D 17.2 15.2
S34-S35 <LOD <LOD N/D <LOD <LOD
SOFT/TIAFT meeting, San Francisco, CA, Sept. 2011

Similarly to amniotic fluid and
placenta, cord blood objectively
assess the acute exposure, which
occurs at the end of the
pregnancy.
Cord blood is obtained during
delivery and thus provides
information on the last days
before it.
Neonatal urine is obtained the first
day(s) of life and can account
for the previous 60-72 hours.

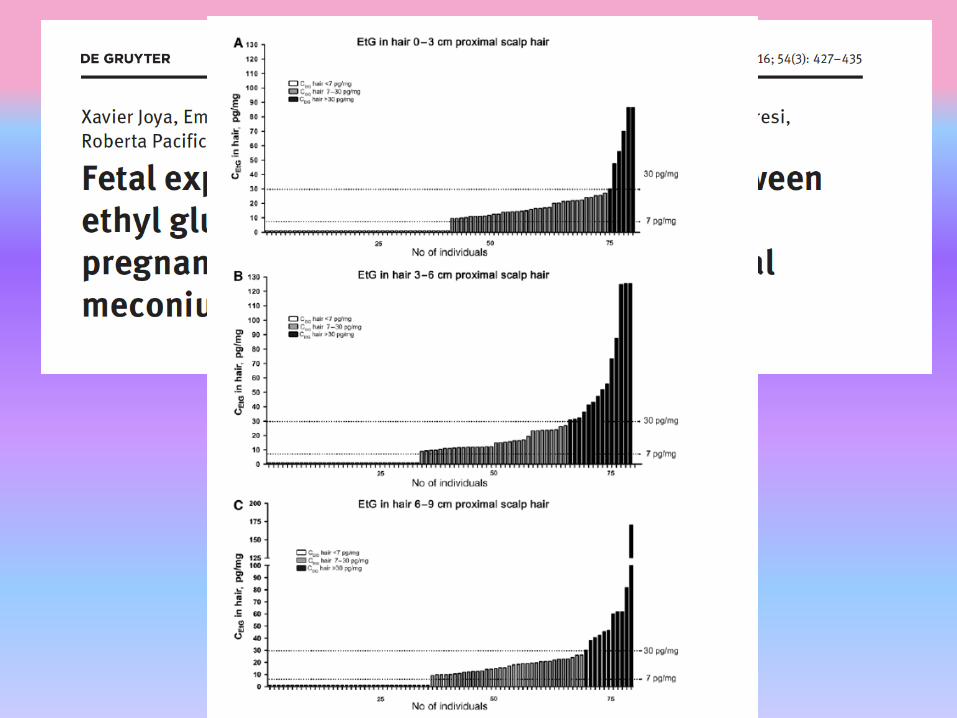
As previously
reported, meconium
and fetal hair
objectively assess a
chronic exposure to
drugs during fetal life,
starting from second
trimester of pregnancy
in case of meconium
whereas hair grows
only during the third
trimester of
pregnancy.
FAEEs in neonatal hair
• Caprara DL, Klein J, Koren G.
Baseline measures of fatty acid etil esters in hair of
neonates born to abstaining or mild social drinking
mothers.
Ther Drug Monit. 2005 Dec;27(6):811-5.
• hair samples of infants born to women with problems of
excessive alcohol consumption should be analyzed to
check the possible difference in the concentrations of
FAEEs
• AN IMPORTANT LIMITATION IS THE AMOUNT OF
NEONATAL HAIR WHICH CAN BE COLLECTED (< 10
mg)
EtG and EtS in neonatal hair?
• All hair samples from newborns tested < LLOQ for HEtG.
Morini L, Marchei E, Vagnarelli F, Garcia Algar O, Groppi A, Mastrobattista L, Pichini S.
Ethyl glucuronide and ethyl sulfate in meconium and hair-potential biomarkers of intrauterine exposure to ethanol.
Forensic Sci Int. 2010 Mar 20;196(1-3):74-7. Epub 2010 Jan 8.
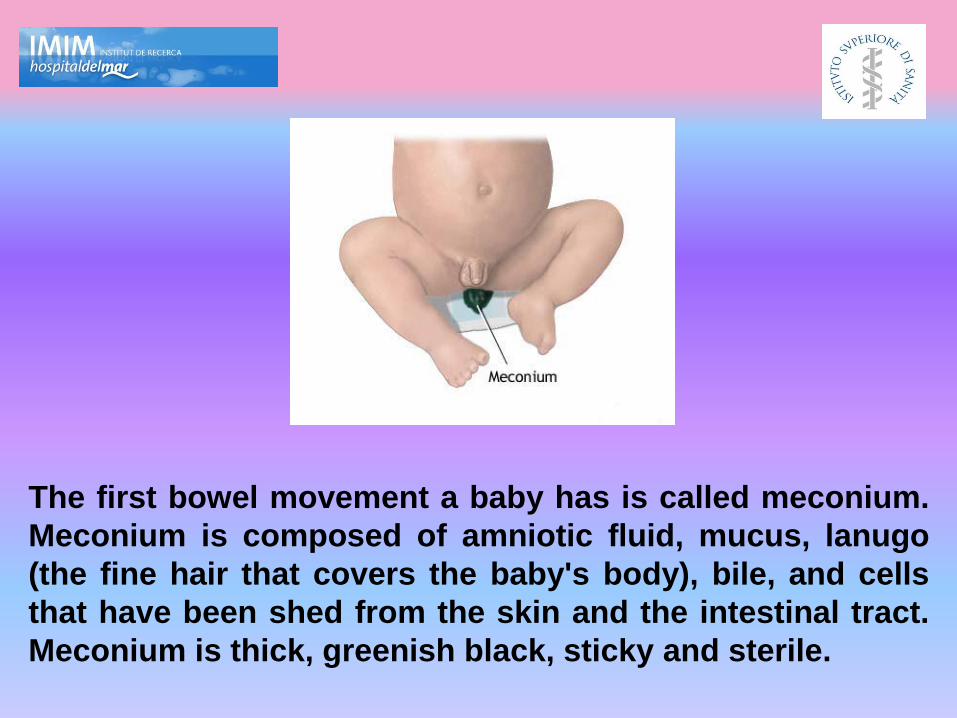
The first bowel movement a baby has is called meconium.
Meconium is composed of amniotic fluid, mucus, lanugo
(the fine hair that covers the baby's body), bile, and cells
that have been shed from the skin and the intestinal tract.
Meconium is thick, greenish black, sticky and sterile.

“The Meconium Project”: An Italian-Spanish
Joint Study to Assess Exposure to Illicit Drugs
During Pregnancy and Birth Outcomes in a
mediterranean city (2004-2008)
Istituto Superiore di Sanità, Roma, Italy
IMIM- Hospital del Mar, Barcelona, Spain
We found in 1209 meconium samples of mother-infant dyads attending the
Hospital during 2002-2004 a prevalence of prenatal exposure to 2.6%
Cocaine, 4.7% heroin and 5.3% cannabis and….
45% daily maternal ethanol measured by FAEEs in
meconium

Chan et al., JPET 2004
Fatty acid ethyl esters (FAEEs) in meconium
Positive cut-off:
7 FAEEs> 2 nmol/g meconium

Are there EtG + EtS in meconium?
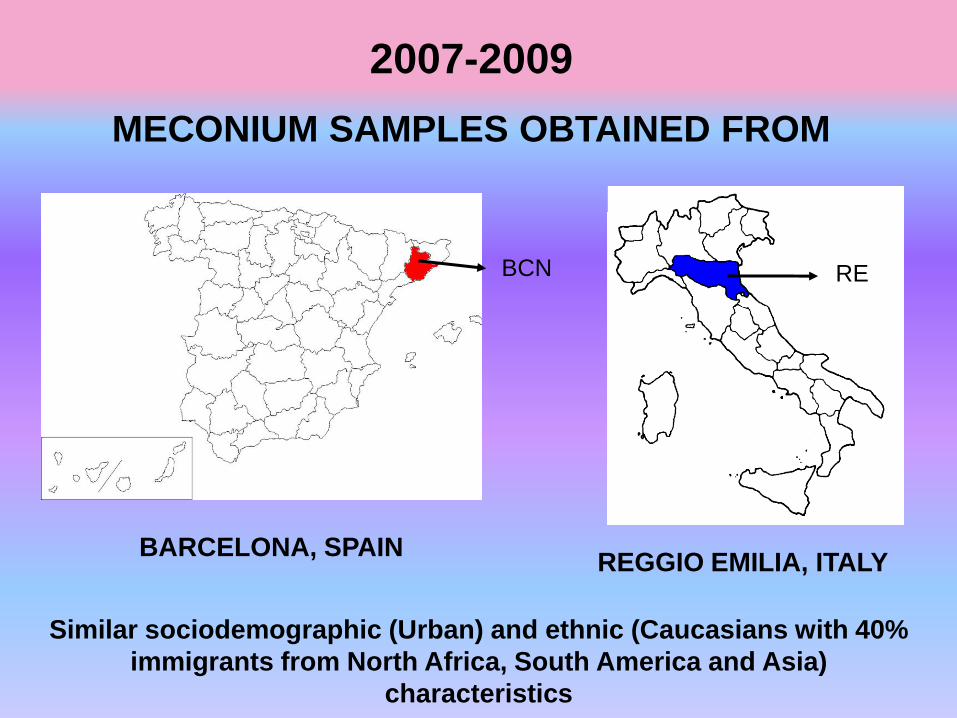
2007-2009
MECONIUM SAMPLES OBTAINED FROM
Similar sociodemographic (Urban) and ethnic (Caucasians with 40%
immigrants from North Africa, South America and Asia)
characteristics
BARCELONA, SPAIN
BCN
REGGIO EMILIA, ITALY
RE
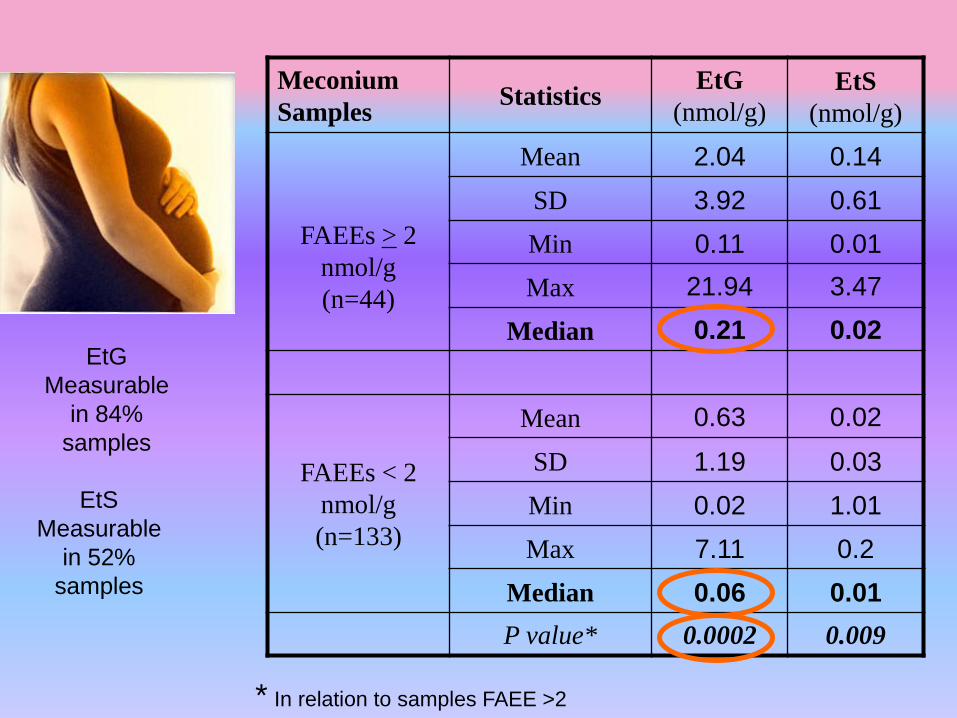
Meconium
Samples Statistics
EtG
(nmol/g) EtS
(nmol/g)
FAEEs > 2
nmol/g
(n=44)
Mean 2.04 0.14
SD 3.92 0.61
Min 0.11 0.01
Max 21.94 3.47
Median 0.21 0.02
FAEEs < 2
nmol/g
(n=133)
Mean 0.63 0.02
SD 1.19 0.03
Min 0.02 1.01
Max 7.11 0.2
Median 0.06 0.01
P value* 0.0002 0.009
* In relation to samples FAEE >2
EtS
Measurable
in 52%
samples
EtG
Measurable
in 84%
samples
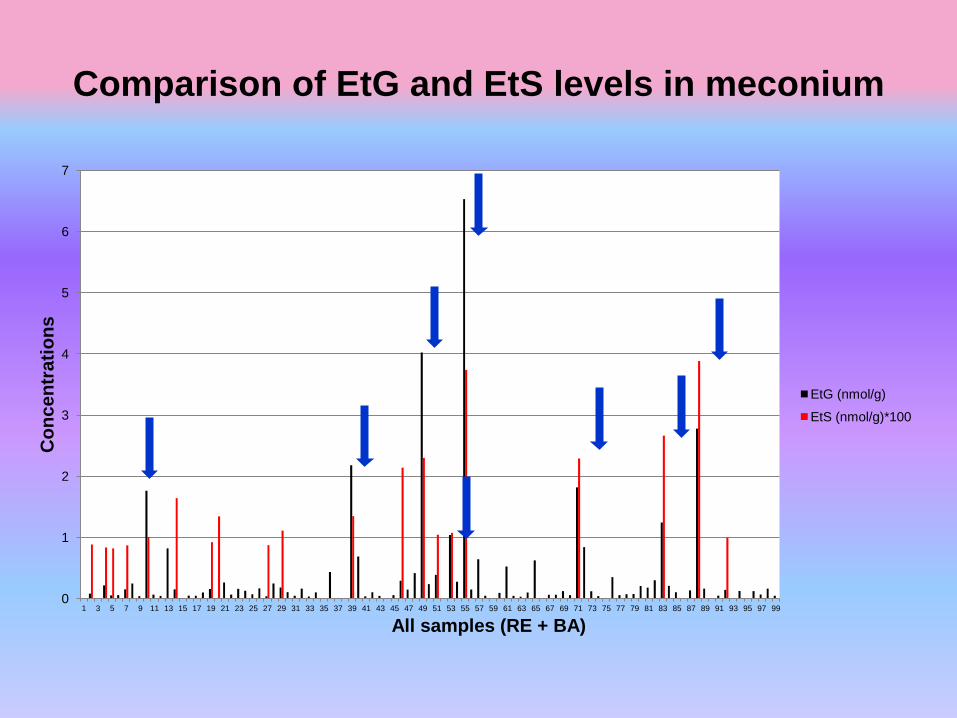
Comparison of EtG and EtS levels in meconium
0
1
2
3
4
5
6
7
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75 77 79 81 83 85 87 89 91 93 95 97 99
Co
nc
en
tra
tio
ns
All samples (RE + BA)
EtG (nmol/g)
EtS (nmol/g)*100
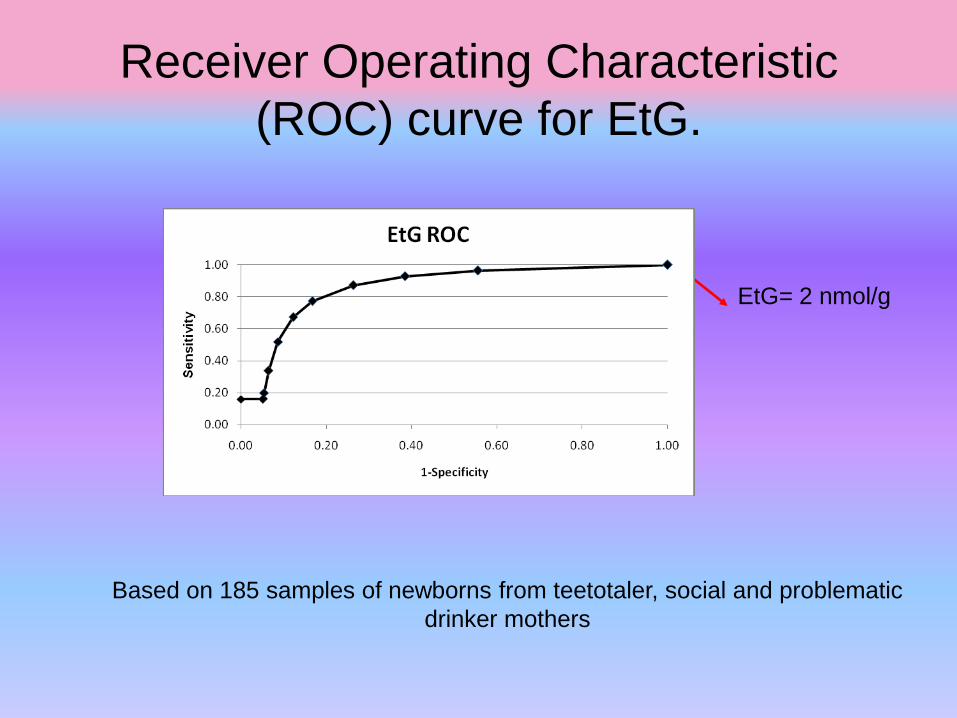
Receiver Operating Characteristic
(ROC) curve for EtG.
EtG= 2 nmol/g
Based on 185 samples of newborns from teetotaler, social and problematic
drinker mothers

ITALIAN MULTICENTRE STUDY
2010
Meconium samples of newborns of
Neonatology Units from:
Reggio Emilia- 160
Roma- 51
Napoli- 61
San Daniele del Friuli- 50
Crotone- 96
Firenze- 99
Verona- 90
All the neonates born in the Unit in a
certain period of time (e.g.1 month)
excluding the ones with severe
pathologies (e.g. prematures, N=8)
requesting intensive care
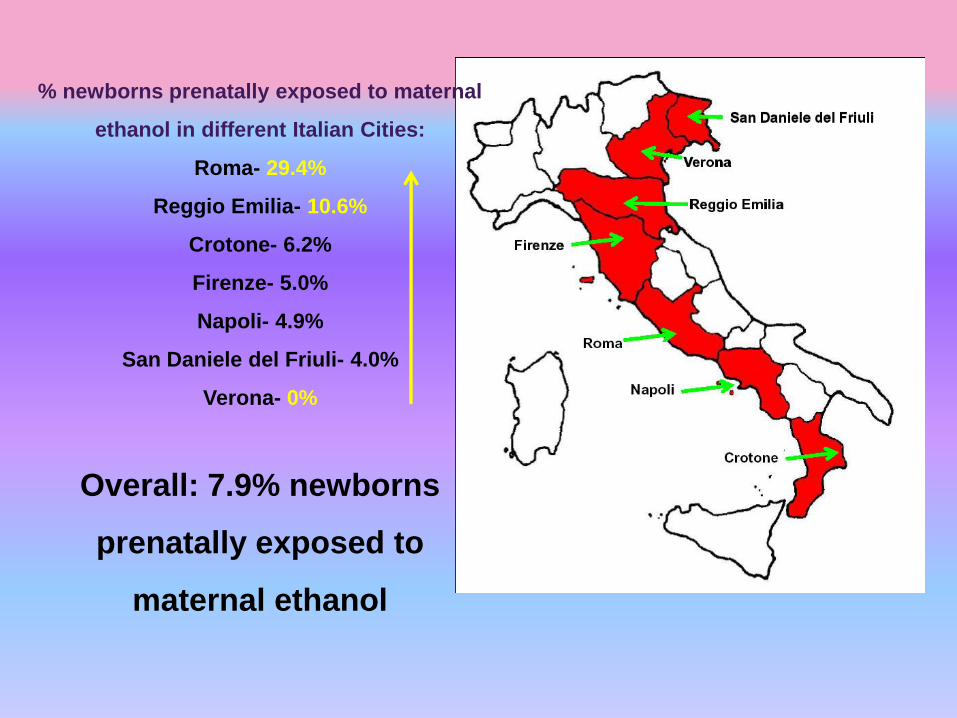
% newborns prenatally exposed to maternal
ethanol in different Italian Cities:
Roma- 29.4%
Reggio Emilia- 10.6%
Crotone- 6.2%
Firenze- 5.0%
Napoli- 4.9%
San Daniele del Friuli- 4.0%
Verona- 0%
Overall: 7.9% newborns
prenatally exposed to
maternal ethanol
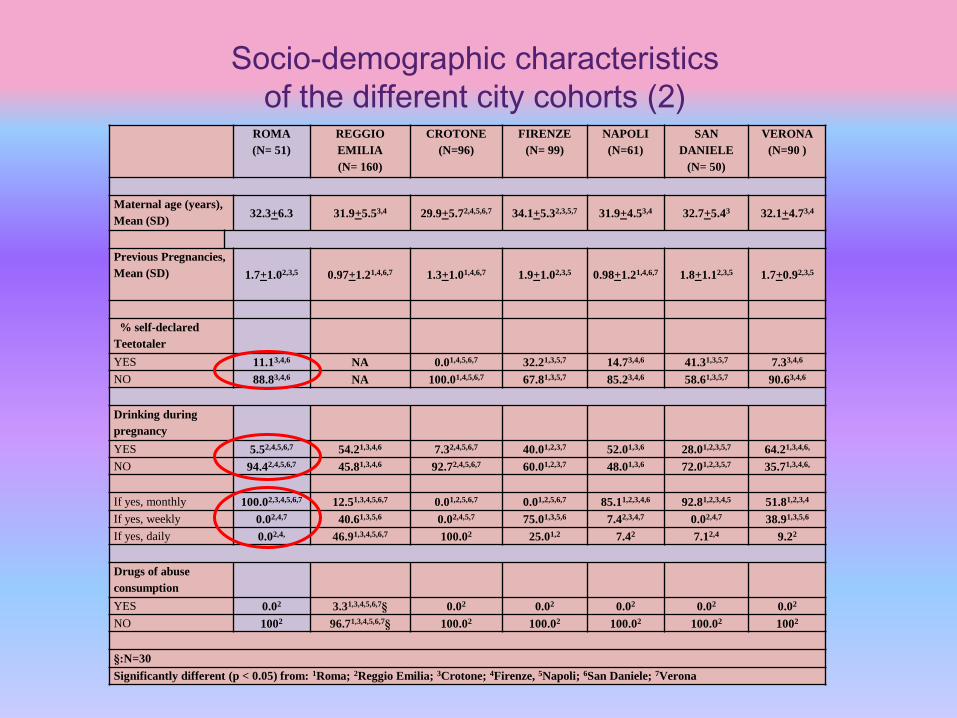
Socio-demographic characteristics
of the different city cohorts (2) ROMA
(N= 51)
REGGIO
EMILIA
(N= 160)
CROTONE
(N=96)
FIRENZE
(N= 99)
NAPOLI
(N=61)
SAN
DANIELE
(N= 50)
VERONA
(N=90 )
Maternal age (years),
Mean (SD) 32.3+6.3 31.9+5.53,4 29.9+5.72,4,5,6,7 34.1+5.32,3,5,7 31.9+4.53,4 32.7+5.43 32.1+4.73,4
Previous Pregnancies,
Mean (SD) 1.7+1.02,3,5 0.97+1.21,4,6,7 1.3+1.01,4,6,7 1.9+1.02,3,5 0.98+1.21,4,6,7 1.8+1.12,3,5 1.7+0.92,3,5
% self-declared
Teetotaler
YES 11.13,4,6 NA 0.01,4,5,6,7 32.21,3,5,7 14.73,4,6 41.31,3,5,7 7.33,4,6
NO 88.83,4,6 NA 100.01,4,5,6,7 67.81,3,5,7 85.23,4,6 58.61,3,5,7 90.63,4,6
Drinking during
pregnancy
YES 5.52,4,5,6,7 54.21,3,4,6 7.32,4,5,6,7 40.01,2,3,7 52.01,3,6 28.01,2,3,5,7 64.21,3,4,6,
NO 94.42,4,5,6,7 45.81,3,4,6 92.72,4,5,6,7 60.01,2,3,7 48.01,3,6 72.01,2,3,5,7 35.71,3,4,6,
If yes, monthly 100.02,3,4,5,6,7 12.51,3,4,5,6,7 0.01,2,5,6,7 0.01,2,5,6,7 85.11,2,3,4,6 92.81,2,3,4,5 51.81,2,3,4
If yes, weekly 0.02,4,7 40.61,3,5,6 0.02,4,5,7 75.01,3,5,6 7.42,3,4,7 0.02,4,7 38.91,3,5,6
If yes, daily 0.02,4, 46.91,3,4,5,6,7 100.02 25.01,2 7.42 7.12,4 9.22
Drugs of abuse
consumption
YES 0.02 3.31,3,4,5,6,7§ 0.02 0.02 0.02 0.02 0.02
NO 1002 96.71,3,4,5,6,7§ 100.02 100.02 100.02 100.02 1002
§:N=30
Significantly different (p < 0.05) from: 1Roma; 2Reggio Emilia; 3Crotone; 4Firenze, 5Napoli; 6San Daniele; 7Verona

Neurodevelopmental characteristics of
newborns exposed to maternal alcohol as
proved by meconium screening: preliminary
data
G. Coriale, L. Tarani, S. Pichini, R. Pacifici, D.
Fiorentino, M. Fiore, F. Di Lauro, R. Marchitelli,
G. Parlapiano, B. Scalese, M. Ceccanti
(See in the Poster Section)
n=8 children (mean age 16 months; s.d. 2.3) positive for FAEEs and EtG in
meconium and n=8 children (mean age 17 months; s.d. 1.4) negative for the
biomarkers in meconium were enrolled in the study.
Physical growth and dysmorphological data collected by pediatrician,
Cognitive motor development and the adaptive abilities assessed using the
Griffiths Mental Development Scales (GMDS ) and Vineland Adaptive
Behaviour Scale (VABS).

46.348.6
32.8
36.3 36.3
42.4
37.9
44.4
52.5
39.3
0
10
20
30
40
50
60
P erso nal S. H earing and
Speech S.
E- H C o -
o rdinat io n S.
P erfo rmance
S.
Lo co mo to r S.
Fig.1 The developmental profiles of the positive and negative meconium sample
on GMDS
Positive Meconium
Negative Meconium
Performance
(Means)
47.9
60.4
49.3
62.855.1
65.0
54.3
68.4
0
10
20
30
40
50
60
70
Comunication
Scale
Daily Living
Scale
Socialization
Scale
Motor Skills
Scale
Figure 2 The developmental profiles of the positive and negative meconium
sample on VABS
Positive Meconium
Negative Meconium
Performance
(Means)
Results
30,0
69,5
50,8 43,5
50,9
60,9 71,6
52,5 51,3 52,5
0
10
20
30
40
50
60
70
80 Positive Meconium
Negative Meconium
Fig.1 The developmental profiles of the positiveand negative meconium sample on GMDS
(Percentile)
* *
*significant comparison ( p < 0.05) 30.0
69.5
50.8 43.5
50.9
60.9 71.6
52.5 51.3 52.5
0
10
20
30
40
50
60
70
80 Positive Meconium
Negative Meconium
Fig.1 The developmental profiles of the positiveand negative meconium sample on GMDS
(Percentile)
* *
*significant comparison ( p < 0.05)
Fig.1 The developmental profiles of the positiveand negative meconium sample on GMDS
(Percentile)
* *
*significant comparison ( p < 0.05)
54,3 55,2 49,9 47,9
68,4 65,0 62,7 60,4
0 10 20 30 40 50 60 70 80 Positive Meconium
Negative Meconium
Figure 2 The developmental profiles of the positive and negative meconium sample
on VABS (raw scores )
* *significant comparison ( p < 0.05)
*
54.3 55.2 49.9 47.9
68.4 65.0 62.7 60.4
0 10 20 30 40 50 60 70 80 Positive Meconium
Negative Meconium
Figure 2 The developmental profiles of the positive and negative meconium sample
on VABS (raw scores )
* *significant comparison ( p < 0.05)
*
Suggested strategy to detect drinking during pregnancy:
Questionnaire and EtG in urine at first antenatal visit; if positive- EtG in hair;
if positive brief intervention or detoxification centre.
If suspicion, EtG in urine at each visit, standard biomarkers
Suggested strategy to detect fetal exposure to maternal
drinking :
EtG in meconium for all newborns; for newborns from risky environments; for
newborns of mothers suspected of drinking during pregnancy

A survey of Italian high school students
regarding awareness of Fetal Alcohol
Syndrome and Fetal Alcohol Spectrum
Disorders
Paolo Berretta1, Roberta Dal Rin Della Mora2, Valeria
Traverso2, Giacomo Toth1, Simona Pichini1, Roberta
Pacifici1, Adele Minutillo1 1 Drug Abuse and Doping Unit, Department of Therapeutic
Research and Medicines Evaluation Istituto Superiore di
Sanità, Roma, Italy 2 IRCCS Istituto Giannina Gaslini

0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20% V
alle
d'A
osta
Pie
monte
Lom
bard
ia
Lig
uria
Tre
ntino A
lto A
dig
e
Veneto
Friuli
Venezia
Giu
lia
Em
ilia R
om
agna
Toscana
Um
bria
Marc
he
Lazio
Abru
zzo
Molis
e
Cam
pania
Basili
cata
Puglia
Cala
bria
Sard
egna
Sic
ilia
0.5%
5.5%
12.0%
2.4% 1.3%
9.9%
3.4%
5.5% 6.1%
2.4%
2.1%
5.0% 5.1%
0.5%
8.7%
2.7%
10.0%
6.3%
2.9%
7.5%
% responding schools in different regions %
Regions

-10%
0%
10%
20%
30%
40%
50%
60%
70%
High school Technical school Vocational school
48.7%
30.5%
20.8%
47.1%
33.5%
19.3%
Distribution by type of schools
public school
private school
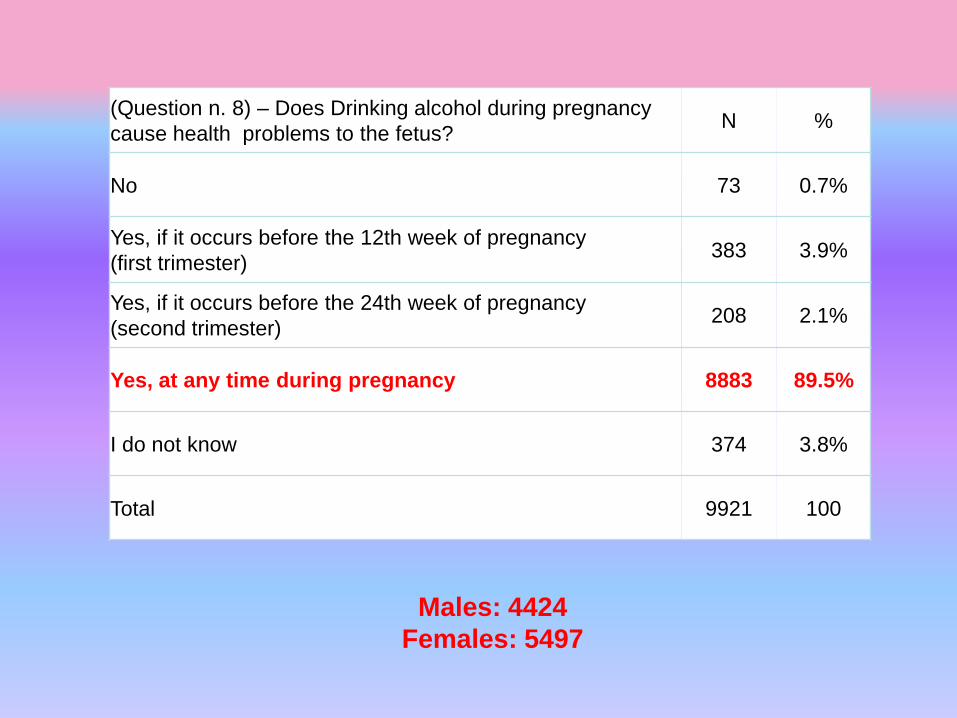
(Question n. 8) – Does Drinking alcohol during pregnancy
cause health problems to the fetus? N %
No 73 0.7%
Yes, if it occurs before the 12th week of pregnancy
(first trimester) 383 3.9%
Yes, if it occurs before the 24th week of pregnancy
(second trimester) 208 2.1%
Yes, at any time during pregnancy 8883 89.5%
I do not know 374 3.8%
Total 9921 100
Males: 4424
Females: 5497
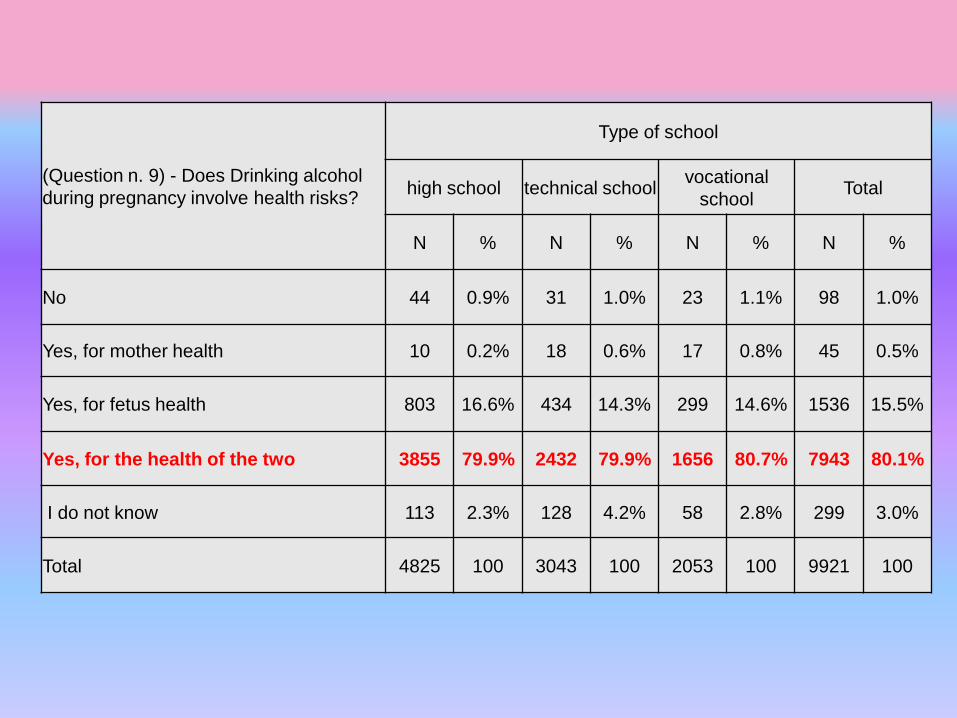
(Question n. 9) - Does Drinking alcohol
during pregnancy involve health risks?
Type of school
high school technical school vocational
school Total
N % N % N % N %
No 44 0.9% 31 1.0% 23 1.1% 98 1.0%
Yes, for mother health 10 0.2% 18 0.6% 17 0.8% 45 0.5%
Yes, for fetus health 803 16.6% 434 14.3% 299 14.6% 1536 15.5%
Yes, for the health of the two 3855 79.9% 2432 79.9% 1656 80.7% 7943 80.1%
I do not know 113 2.3% 128 4.2% 58 2.8% 299 3.0%
Total 4825 100 3043 100 2053 100 9921 100
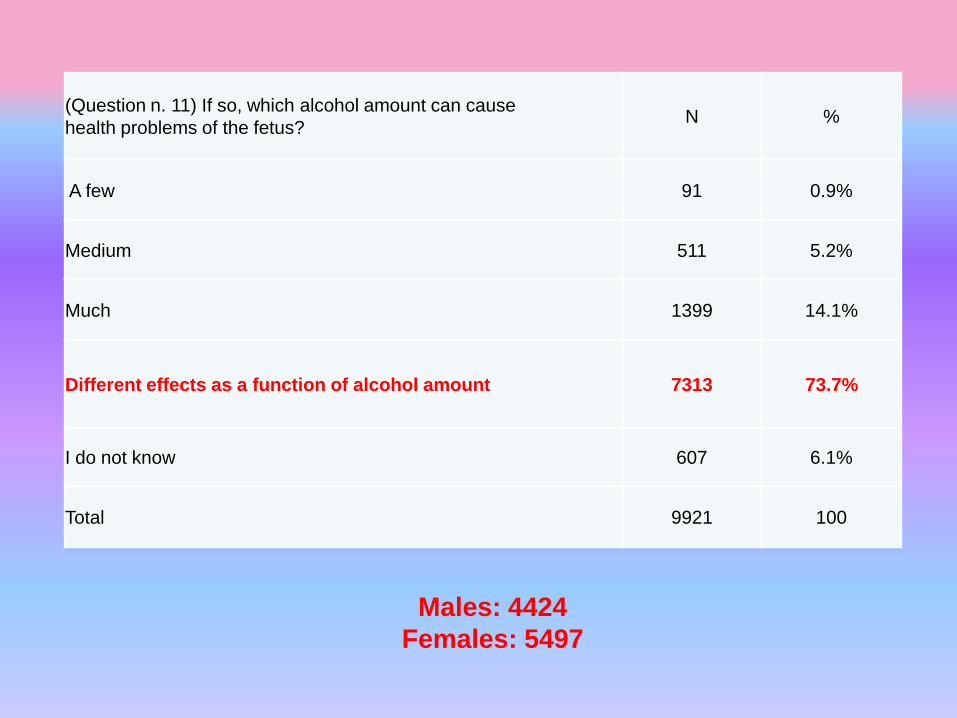
(Question n. 11) If so, which alcohol amount can cause
health problems of the fetus? N %
A few 91 0.9%
Medium 511 5.2%
Much 1399 14.1%
Different effects as a function of alcohol amount 7313 73.7%
I do not know 607 6.1%
Total 9921 100
Males: 4424
Females: 5497
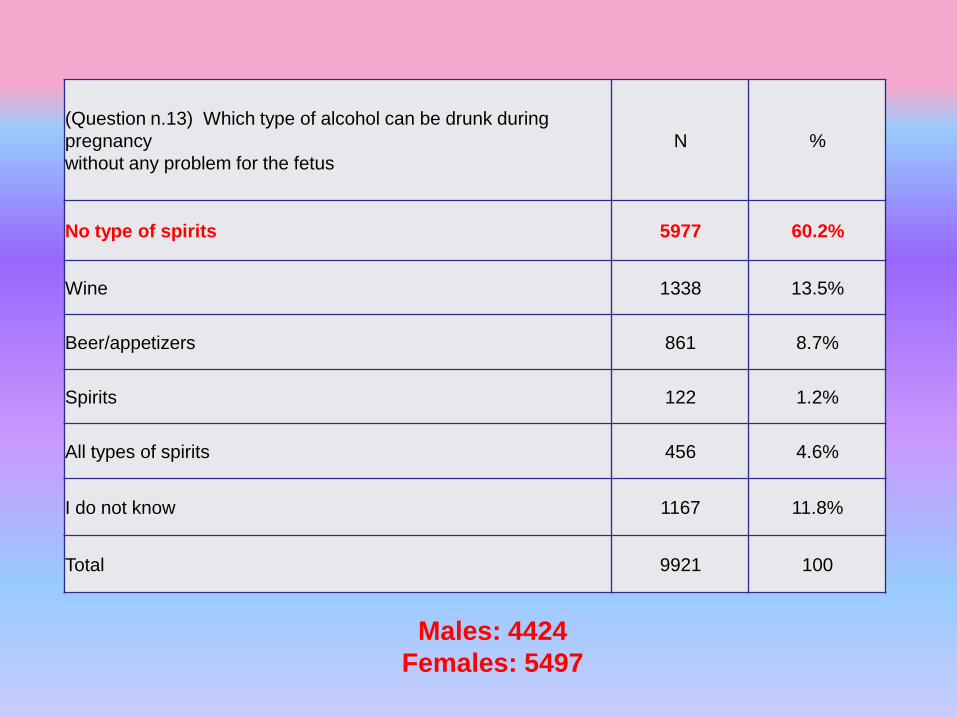
(Question n.13) Which type of alcohol can be drunk during
pregnancy
without any problem for the fetus
N %
No type of spirits 5977 60.2%
Wine 1338 13.5%
Beer/appetizers 861 8.7%
Spirits 122 1.2%
All types of spirits 456 4.6%
I do not know 1167 11.8%
Total 9921 100
Males: 4424
Females: 5497
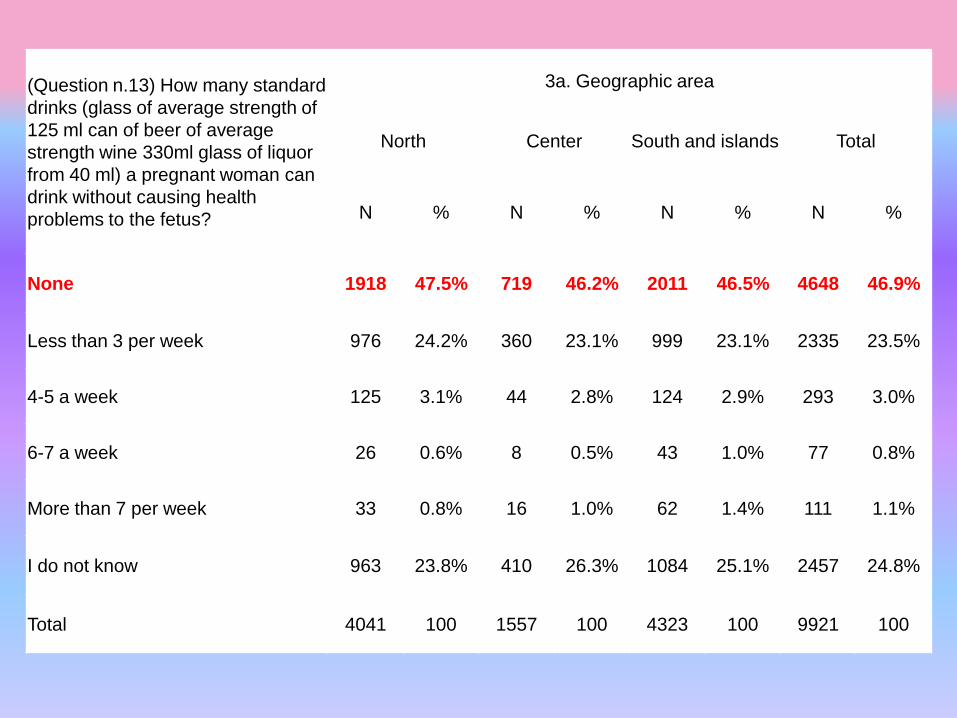
(Question n.13) How many standard
drinks (glass of average strength of
125 ml can of beer of average
strength wine 330ml glass of liquor
from 40 ml) a pregnant woman can
drink without causing health
problems to the fetus?
3a. Geographic area
North Center South and islands Total
N % N % N % N %
None 1918 47.5% 719 46.2% 2011 46.5% 4648 46.9%
Less than 3 per week 976 24.2% 360 23.1% 999 23.1% 2335 23.5%
4-5 a week 125 3.1% 44 2.8% 124 2.9% 293 3.0%
6-7 a week 26 0.6% 8 0.5% 43 1.0% 77 0.8%
More than 7 per week 33 0.8% 16 1.0% 62 1.4% 111 1.1%
I do not know 963 23.8% 410 26.3% 1084 25.1% 2457 24.8%
Total 4041 100 1557 100 4323 100 9921 100


Conclusion
The accurate assessment of fetal exposure to
ethanol through the objective measurement of
biomarkers could provide the basis for
appropriate treatment and follow-up of exposed
newborns.
We are trying to develop an immunoassay
for EtG in meconium, based on the same
principle of that measuring EtG in adult
urine and blood.
This is a simple, low-cost, easy-to-perform
assay (results available in less than an hour)
which can be routinely applied in neonatology
wards for an early diagnosis of prenatal
exposure to ethanol
This last is of outmost importance in order to
establish an early intervention, preferably
before the development of secondary
disabilities.
Thanks







