Download - Management of Alcoholism 2010

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 1/14
Alcohol and Alcoholism
Fran M. Gengo Pharm.D FCPOffice
Dent Neurologic Institute3980 Sheridan Drive
( Time and Temperature Building)250-2007
Hours by appointment
Alcohol and Alcoholism
• Objectives: After learning this material you should be able to : – Differentiate Alcoholism from Alcohol Dependence – Explain the mechanism of ethanol’s acute and chronic effects in the
brain – Know the chronic effects of ethanol in major organ systems
– Know the basic pharmacokinetic characteristics of ethanol – Be able to calculate a Blood Alcohol Concentration when give patient
physical characteristics, dose of ethanol, and time of consumption
– Be able to recognize the signs and symptoms of ethanol withdrawal – Be able to recommend patient specific treatments for ethanol withdrawal
– Know the role of pharmacologic therapy in maintenance of abstinence
Alcohol and Alcoholism
• Definitions
• Alcohol as a Drug ( see notes from PHC 533)
• Management of Alcohol Withdrawal• Pharmacologic Management of Alcohol
Dependence

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 2/14
• Alcoholism – A disease resulting in
compulsive, out of control use of alcoholwith negative consequences
• Alcohol Dependence (DSM 4)
– Alcohol abuse: A destructive pattern ofalcohol use, leading to significant social,occupational, or medical impairment.
Definitions
Definitions
• Alcoholism
– Type I alcoholism develops gradually overthe lifespan.
• It is equally prevalent in men and women.
• It is generally less severe in its healthconsequences.
– Type II alcoholism has an early onset.• It is much more prevalent in men and more severe.
Alcohol DependenceDSM 4 criteria
• Must have three (or more) of the following, occurring when thealcohol use was at its worst:Alcohol withdrawal symptoms: Either (a) or (b).
– (a) Two (or more) of the following, developing within severalhours to a few days of reduction in heavy or prolonged alcohol
use: – sweating or rapid pulse – increased hand tremor
– insomnia – nausea or vomiting
– physical agitation – anxiety
– transient visual, tactile, or auditory hallucinations or illusions
– grand mal seizures

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 3/14
Alcohol Dependence• Must have three (or more) of the following, occurring when the alcohol use
was at its worst:Alcohol withdrawal symptoms: Either (a) or (b).
– (b) Alcohol is taken to relieve or avoid withdrawal symptoms. – Alcohol was often taken in larger amounts or over a longer period than
was intended – Persistent desire or unsuccessful efforts to cut down or control alcohol
use – Great deal of time spent in using alcohol, or recovering from hangovers – Important social, occupational, or recreational activities given up or
reduced because of alcohol use. – Continued alcohol use is continued despite knowledge of having a
persistent or recurrent physical or psychological problem that is likely tohave been worsened by alcohol (e.g., continued drinking despiteknowing that an ulcer was made worse by drinking alcohol)
Twelve-month prevalence and populationestimates of DSM-IV alcohol dependence
0.060.240.060.130.110.3965+
0.151.890.171.150.252.6745–64
0.233.770.262.610.344.9830–
44
0.419.240.405.520.6813.018–
29
0.143.810.132.320.215.42Total
Total
S.E.%S.E.%S.E.%
TotalFemaleMale
Michigan Alcohol Screening TestMAST
• A 22 item questionnaire to identify those at
risk for Alcohol Dependence
• http://counsellingresource.com/quizzes/alc
ohol-mast/index.html
• You should all take this test annually
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 4/14
Alcohol and Alcoholism
• Definitions
• Alcohol as a Drug• Management of Alcohol Withdrawal
• Pharmacologic Management of AlcoholDependence
Pharmacodynamics: CNSEffects
• Alcohol is a CNS depressant
• Apparent stimulatory effects result fromdepression of inhibitory control
mechanisms in the brain
• Characteristic response: euphoria,impaired thought processes, decreasedmechanical efficiency
Neuropharmacology of Ethanol
• Effects on GABA system – Interaction with GABA-A receptor and facilitation of GABA transmission
• Sedative and anxiolytic effects
• Withdrawal
• Effects on Dopamine system
– Increase dopamine in mesocorticolimbic system• Reinforcing, rewarding effects
• Effects on Opioid peptide system – Activation of opioid peptide system
• Reinforcing and rewarding effects (Mu)• Craving
• Effects on NMDA Glutamate system – Blockage of NMDA receptor (allosteric effect)
• Neuroadaptation• Withdrawal
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 5/14
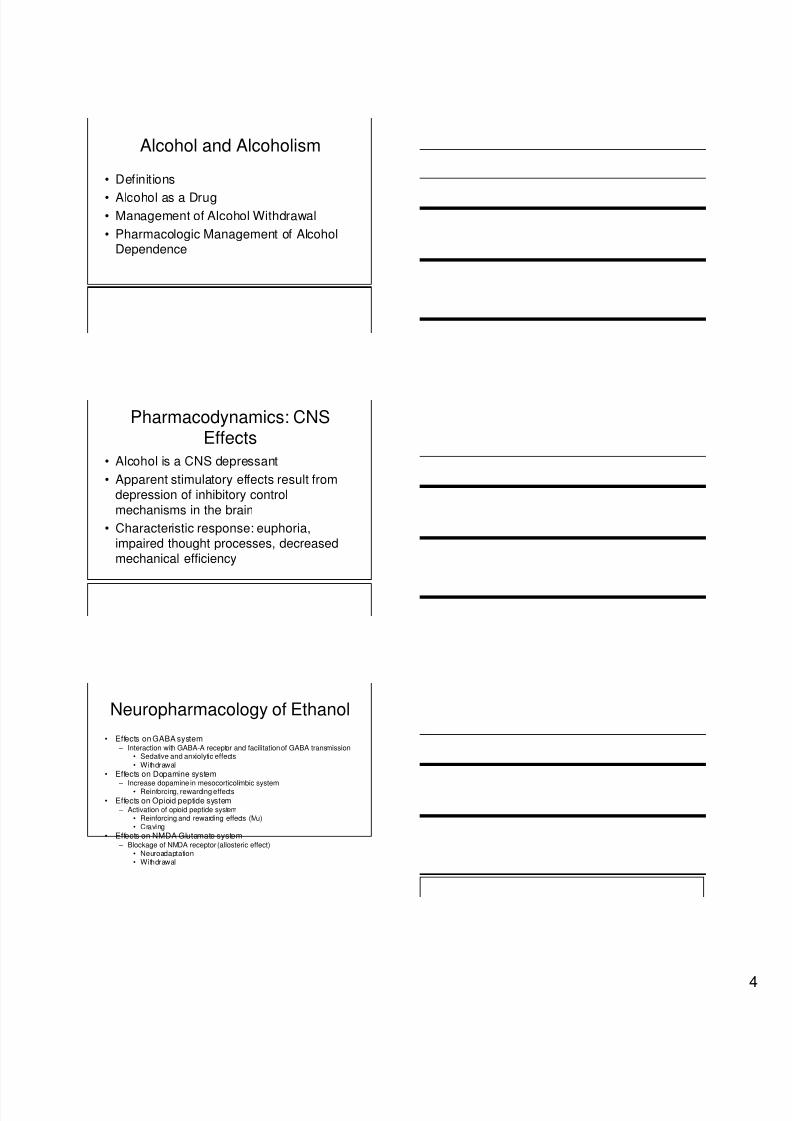
Ethanol Mechanism of ActionEthanol facilitates GABAnergic transmission, GABA is an inhibitory neurotransmitter.Ethanol blocks glutamate transmission, Glutamate is an excitatory neurotransmitter
Ethanol results in the release of Dopamine in the nucleus accumbens
Ethanol Mechanism of Action
Ethanol facilitates GABAnergic transmission, GABA is an inhibitory neurotransmitter.
Ethanol blocks glutamate transmission, Glutamate is an excitatory neurotransmitterEthanol results in the release of Dopamine in the nucleus accumbens
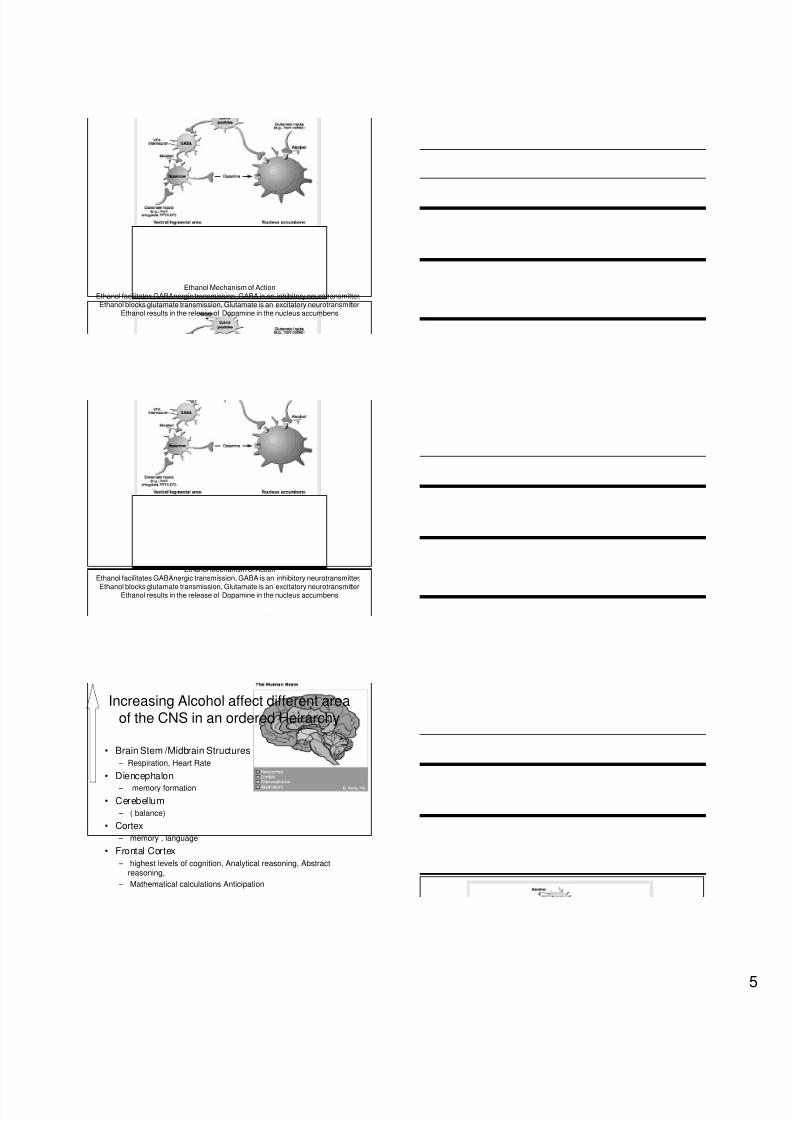
• Brain Stem /Midbrain Structures
– Respiration, Heart Rate
• Diencephalon
– memory formation
• Cerebellum
– ( balance)
• Cortex
– memory , language
• Frontal Cortex
– highest levels of cognition, Analytical reasoning, Abstractreasoning,
– Mathematical calculations Anticipation
Increasing Alcohol affect different areaof the CNS in an ordered Heirarchy
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 6/14
Chronic Effects of Ethanol
• Digestive
• CNS
• Cardiac
• Immunologic
• Hormonal
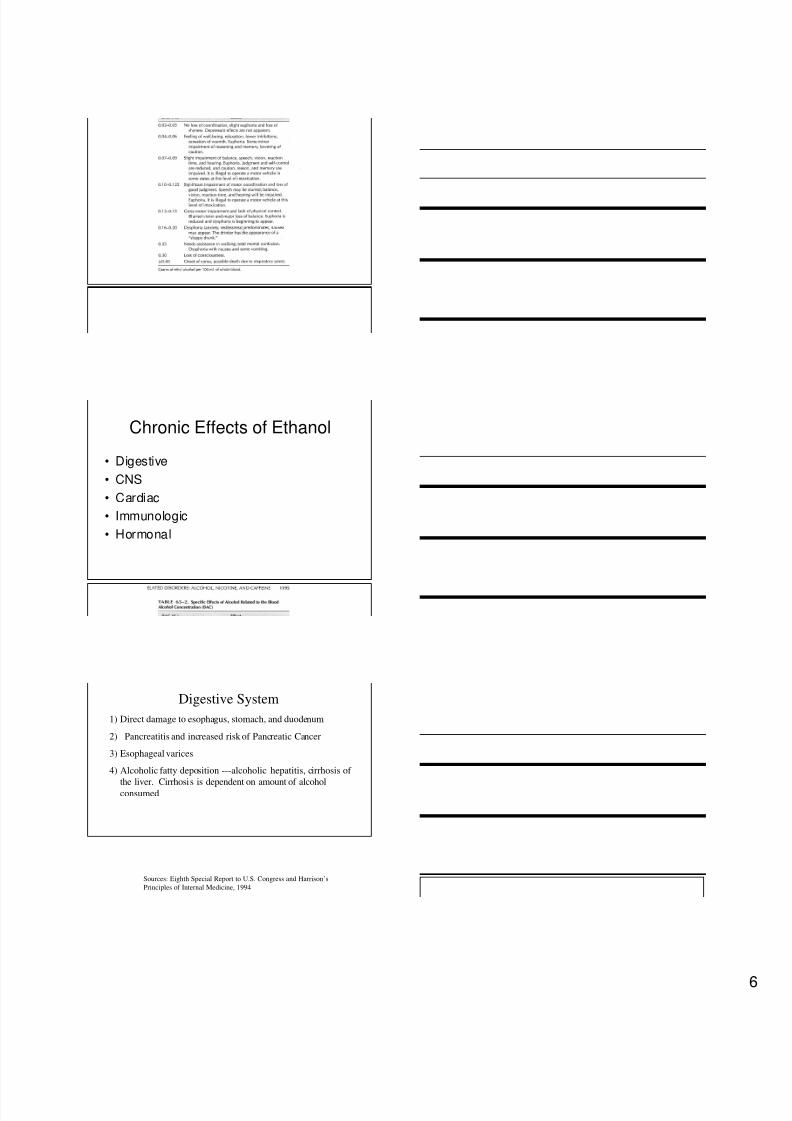
Digestive System
1) Direct damage to esophagus, stomach, and duodenum
2) Pancreatitis and increased risk of Pancreatic Cancer
3) Esophageal varices
4) Alcoholic fatty deposition ---alcoholic hepatitis, cirrhosis of
the liver. Cirrhosis is dependent on amount of alcoholconsumed
Sources: Eighth Special Report to U.S. Congress and Harrison’s
Principles of Internal Medicine, 1994
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 7/14
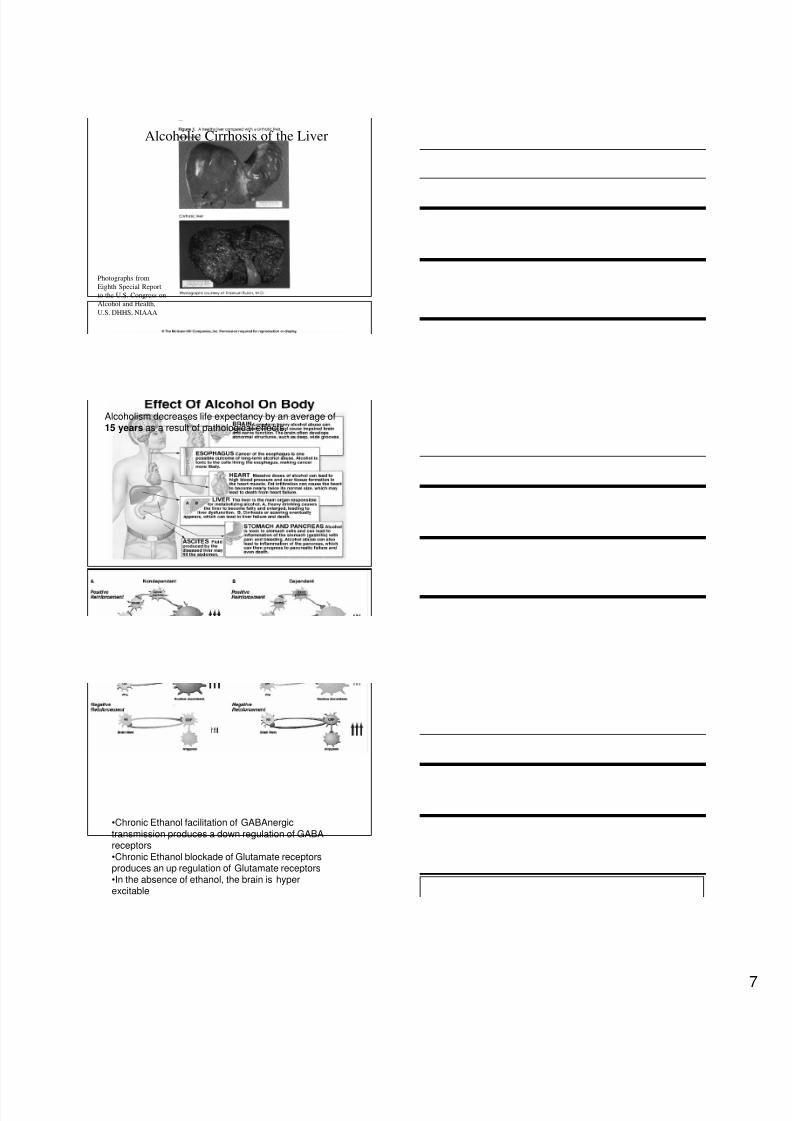
Alcoholic Cirrhosis of the Liver
Photographs from
Eighth Special Report
to the U.S. Congress on
Alcohol and Health,
U.S. DHHS, NIAAA
Alcoholism decreases life expectancy by an average of15 years as a result of pathological effects.
•Chronic Ethanol facilitation of GABAnergictransmission produces a down regulation of GABAreceptors•Chronic Ethanol blockade of Glutamate receptorsproduces an up regulation of Glutamate receptors•In the absence of ethanol, the brain is hyperexcitable
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 8/14
Non Alcoholics drink to feel goodAlcoholics drink to keep from feeling bad
Chronic Effects of Ethanol
• Digestive
• CNS
• Cardiac
• Immunologic
• Hormonal
Various Presentations of AcuteETOH Withdrawal
Minor Withdrawal Symptoms:
-occur w/i 6 hours of cessation
-insomnia, tremulousness, mild anxiety, GIupset, diaphoresis, HA, palpitations, and
anorexia.
-usually resolve w/i 24-48 hrs.
-vary from episode to episode

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 9/14
Various Presentations of AcuteETOH Withdrawal
Withdrawal Seizures:
-w/i 48 hours of last drink-generalized tonic-clonic
-3% of chronic alcoholics develop this
-3% of those who seize develop StatusEpilepticus
Various Presentations of AcuteETOH Withdrawal
Alcoholic Hallucinosis:
- 12- 24 hr. onset after last drink
- usually visual
- Resolve w/i 24-48 hr.
- NOT synonymous with DT’s
*other signs may or may not be present
* time course is different
* not usually associated with clouding of the sensorium
Delirium Tremens:
- 5% of patients who withdraw
- typically begin b/w 48 and 96 hours- typically last 1-5 days
- longer periods requiring massive doses ofmedications have been described (Wolf et.
Al 1993)
Various Presentation of AcuteETOH Withdrawal
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 10/14
Delirium Tremens
- Early figures of associated mortality were
as high as 37%- Now mortality is felt to be 5%. This is likely
due to earlier diagnosis, improvedpharmacological, and non-pharmocologicmanagement, and improved treatment ofco-morbid conditions.
Hallmarks of Delirium Tremens
• Hallucinations
• Disorientation
• Tachycardia
• Hypertension
• Low Grade Fever
• Agitation
• Diaphoresis
Hallmarks of Delirium Tremens
• Elevated cardiac indices, oxygen delivery
and oxygen consumption
• Hyperventilation and Respiratory alkalosis
which result in reduced cerebral blood flow
• Sensorium Clouding

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 11/14
Delirium Tremens
-Mortality risk is greater:
1. Elderly2. Concomitant COPD
3. Core body temp >104
4. Co-existing liver Dx.
- Death is usually due to arrhythmia orsecondary complications. (pneumonia,liver
failure)
Management of Alcohol Withdrawal
• Thiamine 50 – 100 mg daily
• D 5 and 0. 45 Normal Saline
• Clonidine 0.3 mg
• Multi Vitamin
• .
Wernicke-Korsakoff syndrome
• From severe acute deficiency of thiamine
• glucose metabolism will exacerbate anexisting clinical or sub-clinical thiamine
deficiency.• Korsakoff's psychosis is a chronic
neurologic sequela after Wernicke'sencephalopathy..
7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 12/14
•NAUSEA AND VOMITING 0 -7
•TACTILE DISTURBANCES 0-7•TREMOR 0 -7•AUDITORY DISTURBANCES 0 -7•PAROXYSMAL SWEATS. 0 -7•VISUAL DISTURBANCES 0 -7•ANXIETY 0 -7• HEADACHE, FULLNESS IN HEAD 0 -7• AGITATION 0 -7•ORIENTATION AND CLOUDING OF SENSORIUM 0 -4
•Maximum Possible Score 67
Clinical Institute Withdrawal Assessment of Alcohol Scale,(CIWA-Ar)
Management of Alcohol Withdrawal
• Monitoring:
• -Monitor patient every 4-8 hours by means of CIWA-Aruntil score has been < 8-10 for 24 hours; use additionalassessments as needed.
• -For patients with CIWA-Ar <8-10, supportive non-pharmacologic monitoring is acceptable.
• -Patients with CIWA-Ar scores 8-15 benefit frommedication thus reducing risk of complications.
• -CIWA-Ar scores ≥ 15 have a significant risk of majorcomplications if left untreated.
• .
• Symptom Triggered Regimens:
• Administer one of the following every hour
when the CIWA-Ar ≥ 8-10:
• Librium 50-100 mg
• Diazepam 10-20 mg
• Lorazepam 2-4 mg
• Repeat CIWA-Ar 1 hour after every dose
to assess need for further medication
Management of Alcohol Withdrawal

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 13/14
• Fixed Schedule Regimens:
• If necessary to give medication on a fixed schedule thenadminister one of the following:
• Librium 50 mg every 6 hours for 4 doses then 25 mgevery 6 hours for 8 doses
• Diazepam 10 mg every 6 hours for 4 doses then 5 mgevery 6 ours four 8 doses
• Lorazepam 2 mg every 6 hours for 4 doses then 1 mgevery 6 hours for 8 doses
• Provide additional medication as needed CIWA-Ar ≥ 8-10 with above.
• Other benzodiazepines may be used at equivalent doses
Management of Alcohol Withdrawal
Use of anticonvulsants as adjuncttherapy for alcohol withdrawal
• Valproic Acid
• Leveteracetam
• Gabapentin
Management of Alcoholism
• Group Support ( Friends of Bill)
• Naltrexone
• Acamprosate

7/31/2019 Management of Alcoholism 2010
http://slidepdf.com/reader/full/management-of-alcoholism-2010 14/14
• Natrexone
– Dose• Oral: 25 mg; if no withdrawal signs within 1 hour give another 25
mg; maintenance regimen is flexible, variable and individualized (50mg/day to 100-150 mg 3 times/week for 12 weeks); up to 800mg/day has been tolerated in a small number of healthy adultswithout an adverse effect.
• I.M.: 380 mg once every 4 weeks• Mechanism of Action
– Naltrexone acts as a competitive antagonist at opioid receptor sites,showing the highest affinity for mu receptors.
• Pharmacokinetics – Half-life elimination: Oral: 4 hours; 6-beta-naltrexol: 13 hours; I.M.:
naltrexone and 6-beta-naltrexol: 5-10 days – Time to peak, serum: Oral: ~60 minutes; I.M.: Biphasic: 2 hours (first
peak), 2-3 days (second peak)
– Excretion: Primarily urine (as metabolites and unchanged drug)
Management of Alcoholism
AcamprosateDosing: ( Patient must be Abstinent)
• Adult Oral: 666 mg 3 times/day (a lower dose may be effective insome patients).
• Adjustment in patients with low body weight (unlabeled): A lowerdose (4 tablets/day) may be considered in patients with low bodyweight (eg, <60 kg).
• Note: Treatment should be initiated as soon as possible followingthe period of alcohol withdrawal, when the patient has achievedabstinence
• Mechanism of Action – Structurally similar to gamma-amino butyric acid (GABA), acamprosate
appears to increase the activity of the GABA-ergic system, anddecreases activity of glutamate within the CNS, including a decrease inactivity at N-methyl D-aspartate (NMDA) receptors; may also affect CNScalcium channels.
– Pharmacokinetics• Metabolism: Not metabolized
• Bioavailability: 11%• Half-life elimination: 20-33 hours
• Excretion: Urine (as unchanged drug)• Clcr 30-50 mL/minute: Initial dose should be reduced to 333 mg 3times/day.
• Clcr <30 mL/minute: Contraindicated in severe renal impairment.
Management of Alcoholism







