Malnutrition:
Where are we headed?
Kris M. Mogensen, MS, RD-AP, LDN, CNSC
Team Leader Dietitian
Brigham and Women’s Hospital
Instructor
Boston University College of Health and Rehabilitation Sciences:
Sargent College

Disclosures
• I have no disclosures related to this
topic

• It helps to look back before we look
forward, so:
– Review prior malnutrition efforts
– What’s happening with Academy-
ASPEN characteristics
– Where are we headed?
Objectives

Kickin’ it Old School
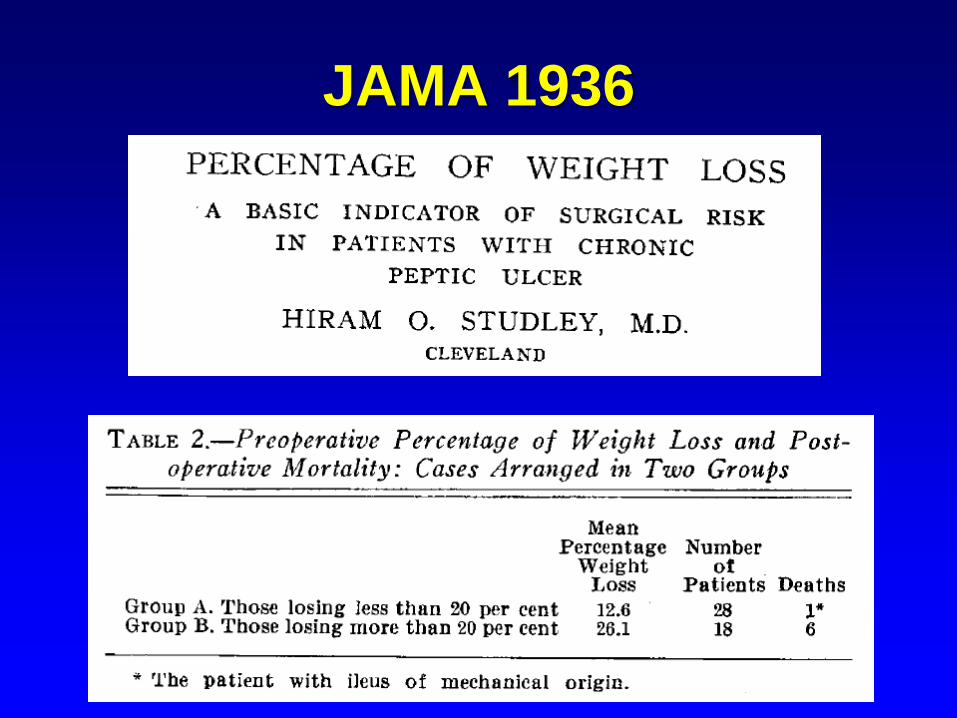
JAMA 1936
Nutrition Today
1974

JPEN
1977 – Issue 1!!

SGA!

“Old” Evaluation Parameters
• % IBW
• % UBW
• Presence of fat/muscle wasting
• Presence of edema
• Adequacy of intake
• Circulating proteins
• Anergy
• Other direct anthropometric measurements

Old Malnutrition Diagnoses
• Kwashiorkor
• Marasmus
• Mild, moderate, severe protein-calorie
malnutrition
• Protein-calorie malnutrition, NOS
Old Malnutrition Diagnoses

Blast from the Past!
From ~ 1992!
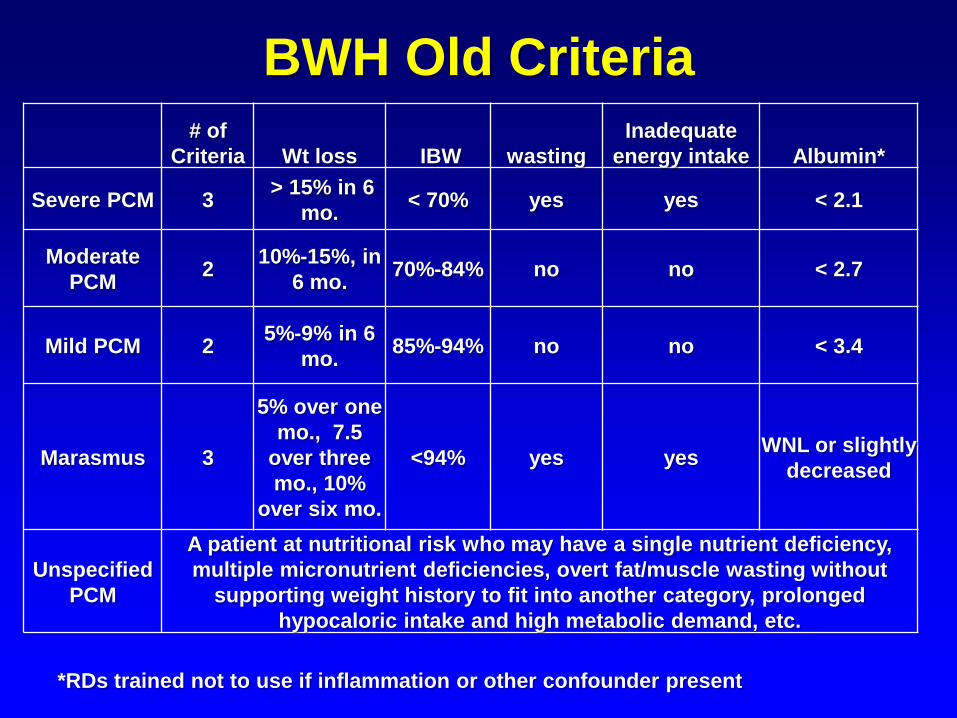
# of
Criteria Wt loss IBW wasting
Inadequate
energy intake Albumin*
Severe PCM 3 > 15% in 6
mo. < 70% yes yes < 2.1
Moderate
PCM 2
10%-15%, in
6 mo. 70%-84% no no < 2.7
Mild PCM 2 5%-9% in 6
mo. 85%-94% no no < 3.4
Marasmus 3
5% over one
mo., 7.5
over three
mo., 10%
over six mo.
<94% yes yes WNL or slightly
decreased
Unspecified
PCM
A patient at nutritional risk who may have a single nutrient deficiency,
multiple micronutrient deficiencies, overt fat/muscle wasting without
supporting weight history to fit into another category, prolonged
hypocaloric intake and high metabolic demand, etc.
BWH Old Criteria
*RDs trained not to use if inflammation or other confounder present

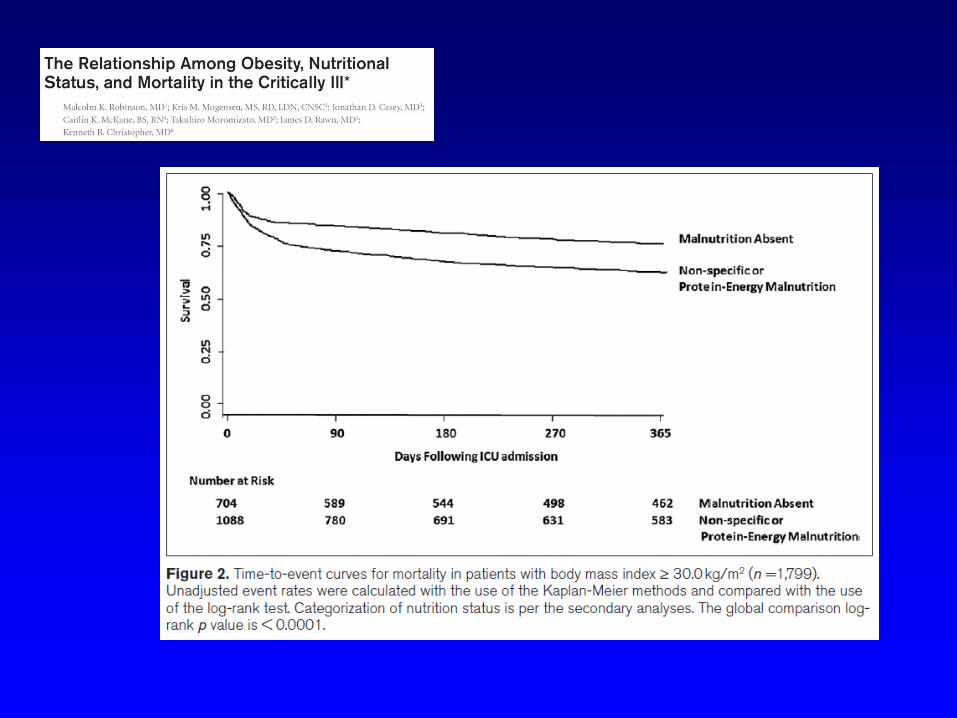
Malnutrition Outcomes:
Old Characteristics
CCM 2015
CCM 2015
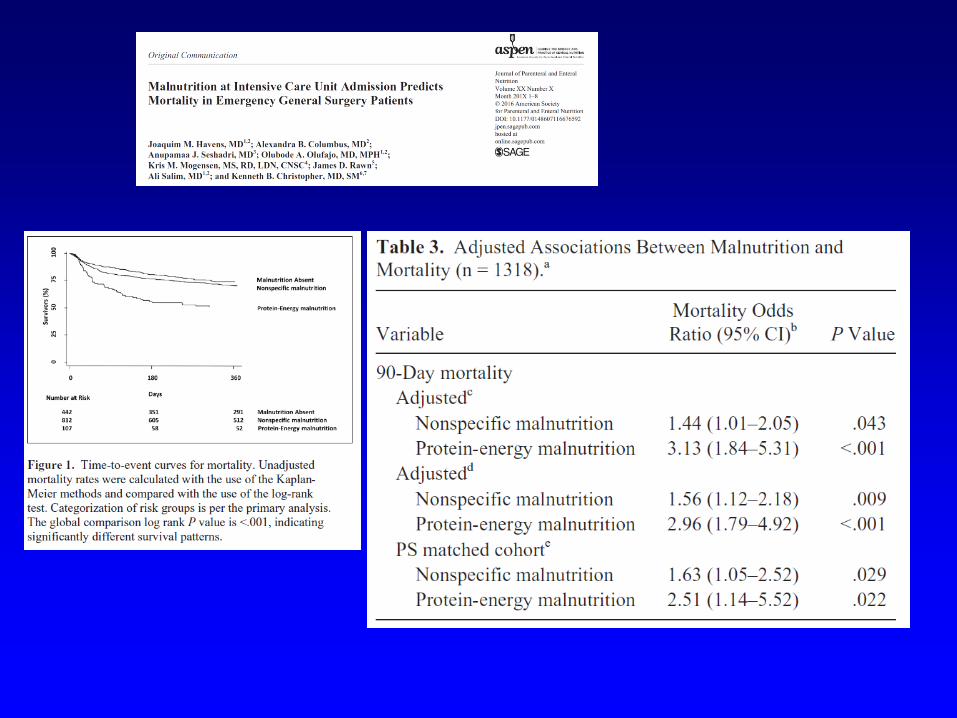
JPEN epub 2016; print Feb 2017
JPEN epub 2016



Moving into modern times…
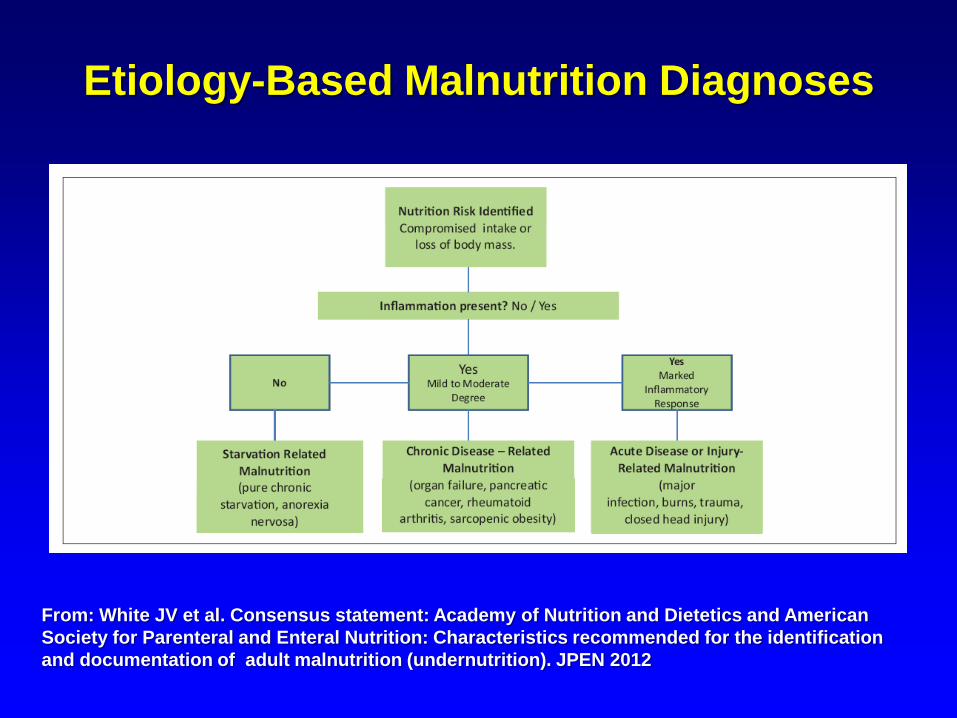
Etiology-Based Malnutrition Diagnoses
From: White JV et al. Consensus statement: Academy of Nutrition and Dietetics and American
Society for Parenteral and Enteral Nutrition: Characteristics recommended for the identification
and documentation of adult malnutrition (undernutrition). JPEN 2012

2012 Malnutrition Clinical
Characteristics Parameters
• Insufficient energy intake
• Weight loss
• Loss of muscle mass
• Loss of subcutaneous fat
• Localized or generalized fluid
accumulation that may sometimes mask
weight loss
• Diminished functional status as measured
by hand grip strength From: White JV et al. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and
Enteral Nutrition: Characteristics recommended for the identification and documentation of adult malnutrition
(undernutrition). JPEN 2012
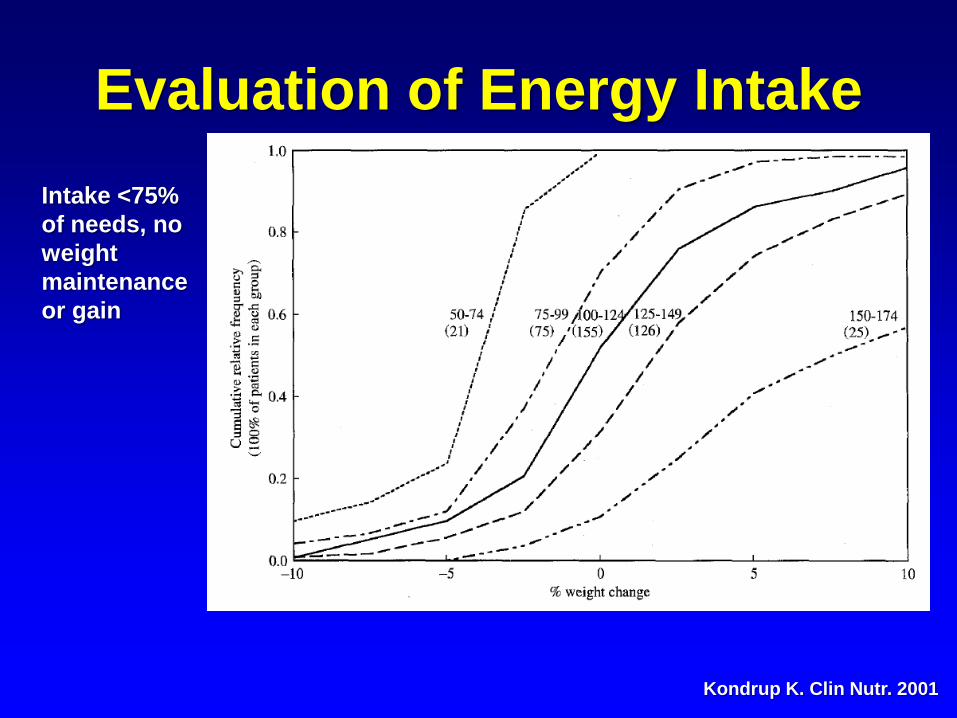
Evaluation of Energy Intake
Kondrup K. Clin Nutr. 2001
Intake <75%
of needs, no
weight
maintenance
or gain
Weight Loss Evaluation
Physical Examination

Hand Grip Strength

Where are we headed?
First stop: Validation!

Validation of the Academy/ASPEN Malnutrition Clinical
Characteristics. Hand RK et al. JAND 2016

Current research with 2012 Adult
Malnutrition Clinical Characteristics
• Nicolo M et al. Feasibility of accessing data in hospitalized patients to
support diagnosis of malnutrition by the Academy- A.S.P.E.N.
malnutrition consensus recommended clinical characteristics. JPEN
2014;38:954-959
• Hand RK et al. Validation of the Academy/ASPEN Malnutrition Clinical
Characteristics. J Acad Nutr Diet. 2016
• Hiller LD et al. Difference in composite end point of readmission and
death between malnourished and nonmalnourished veterans assessed
using Academy of Nutrition and Dietetics/American Society for
Parenteral and Enteral Nutrition Clinical Characteristics. JPEN epub Sept
2016
• Mulasi U et al. Malnutrition identified by the Academy of Nutrition and
Dietetics and American Society for Parenteral and Enteral Nutrition
consensus criteria and other bedside tools is highly prevalent in a
sample of individuals undergoing treatment for head and neck cancer.
JPEN epub Oct 2016

Feasibility of accessing data in hospitalized patients to
support diagnosis of malnutrition by the Academy-
A.S.P.E.N. malnutrition consensus recommended clinical
characteristics. Nicolo M et al. JPEN 2014

Validation of the Academy/ASPEN
Malnutrition Clinical Characteristics. Hand RK et al. JAND 2016
Clinical Characteristic Evaluated?
Intake 96%
Wgt loss 92%
Muscle 98%
Fat 100%
Edema 98%
Hand grip 64%
28 patients enrolled in the study

Validation of the Academy/ASPEN Malnutrition
Clinical Characteristics. Hand RK et al. JAND 2016
• Was there agreement between RDs?
– 24 of 28 had evaluation done by 2 RDs
• Context: agreed ~ 88% of the time
• Diagnosis: agreed for ~ 67% of pts

Validation of the Academy/ASPEN
Malnutrition Clinical Characteristics. Hand RK et al. JAND 2016
• Full outcome data for 11 pts
– Malnourished pts had
• longer LOS
• higher charges
• more frequent ED visits
• More frequent readmissions

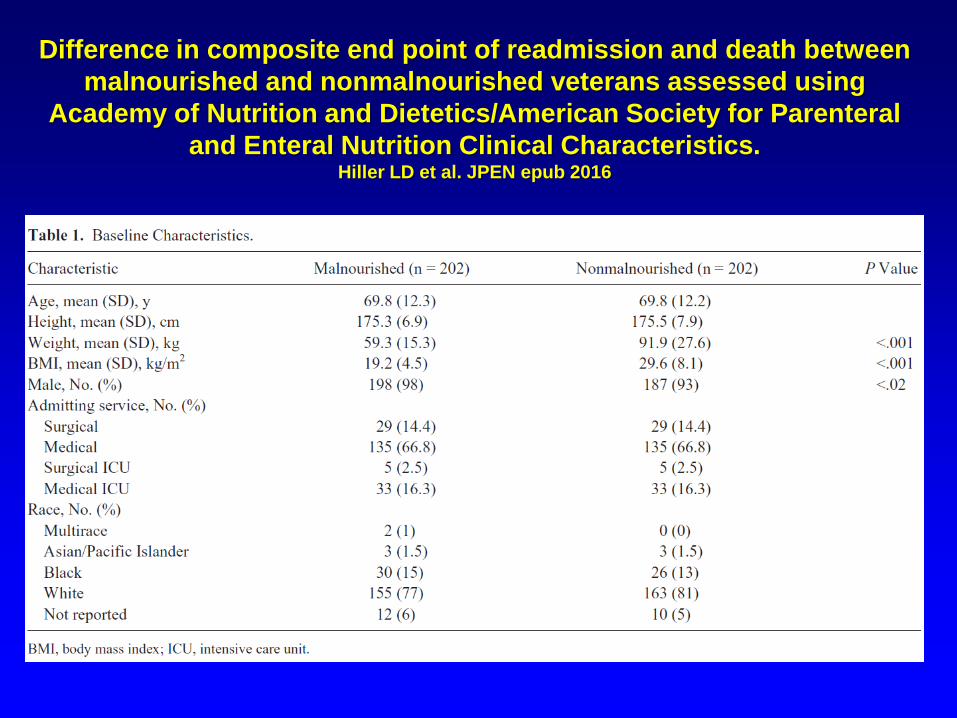
Difference in composite end point of readmission and death between
malnourished and nonmalnourished veterans assessed using
Academy of Nutrition and Dietetics/American Society for Parenteral
and Enteral Nutrition Clinical Characteristics. Hiller LD et al. JPEN epub 2016
• Retrospective medical record review
• Used all characteristics except hand grip
strength
• Matched malnourished vs nonmalnourished:
202 in each group
• Composite end point: 30 day readmission
rate and 90 day mortality rate
Difference in composite end point of readmission and death between
malnourished and nonmalnourished veterans assessed using
Academy of Nutrition and Dietetics/American Society for Parenteral
and Enteral Nutrition Clinical Characteristics. Hiller LD et al. JPEN epub 2016

Difference in composite end point of readmission and death between
malnourished and nonmalnourished veterans assessed using
Academy of Nutrition and Dietetics/American Society for Parenteral
and Enteral Nutrition Clinical Characteristics. Hiller LD et al. JPEN epub 2016

Comparisons to other
markers…

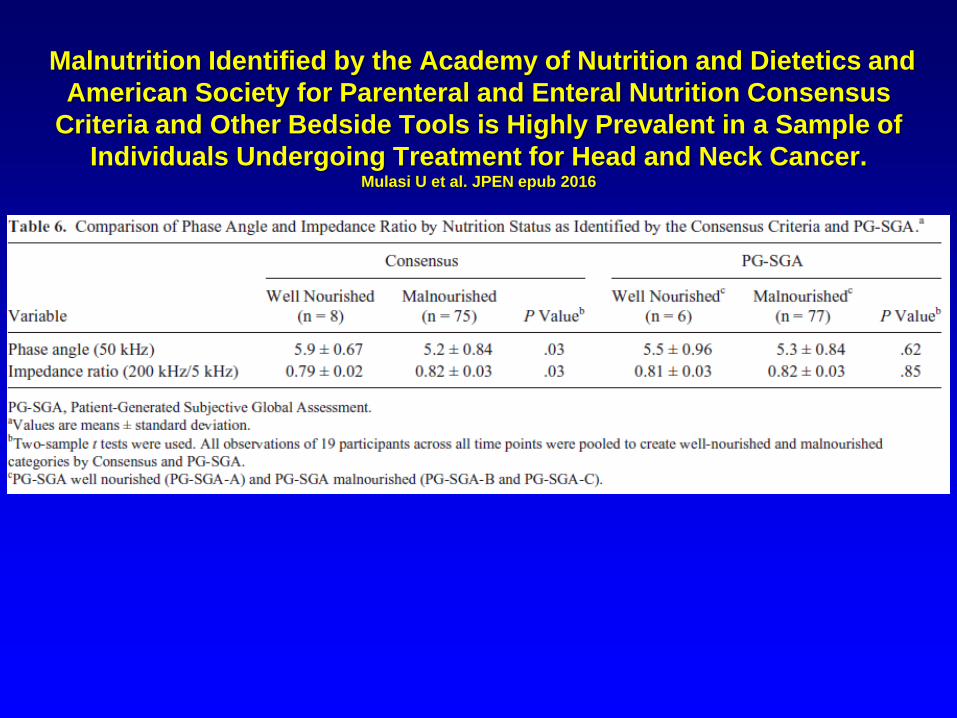
Malnutrition Identified by the Academy of Nutrition and Dietetics and
American Society for Parenteral and Enteral Nutrition Consensus
Criteria and Other Bedside Tools is Highly Prevalent in a Sample of
Individuals Undergoing Treatment for Head and Neck Cancer. Mulasi U et al. JPEN epub 2016
Malnutrition Identified by the Academy of Nutrition and Dietetics and
American Society for Parenteral and Enteral Nutrition Consensus
Criteria and Other Bedside Tools is Highly Prevalent in a Sample of
Individuals Undergoing Treatment for Head and Neck Cancer. Mulasi U et al. JPEN epub 2016

Validation, refining the
characteristics, and
more…where do we go from
here?

Functional Status and
Outcomes
CCM 2016
Surgery 2016
Functional Status and
Outcomes • Formal PT assessment using the
Functional Independence Measure
– Independent, low, intermediate, high, and very
high risk
• High & very high risk
– Increased odds of 90-day post-discharge
mortality in ICU and trauma patients
– Higher prevalence of malnutrition in these
groups


Crit Care
Med. 2016

Functional Status and
Outcomes
• Can we collaborate with other
colleagues evaluating patients? – Could the PT scoring system be part of our
malnutrition characteristics in adults?
– Are our OT colleagues measuring hand grip
strength?

Measures of Muscle Mass
• What are the roles of
– BIA
– CT
– Ultrasound
• Will these move into prime time?

Role of Metabolomics?
Mogensen et al. JPEN
2017

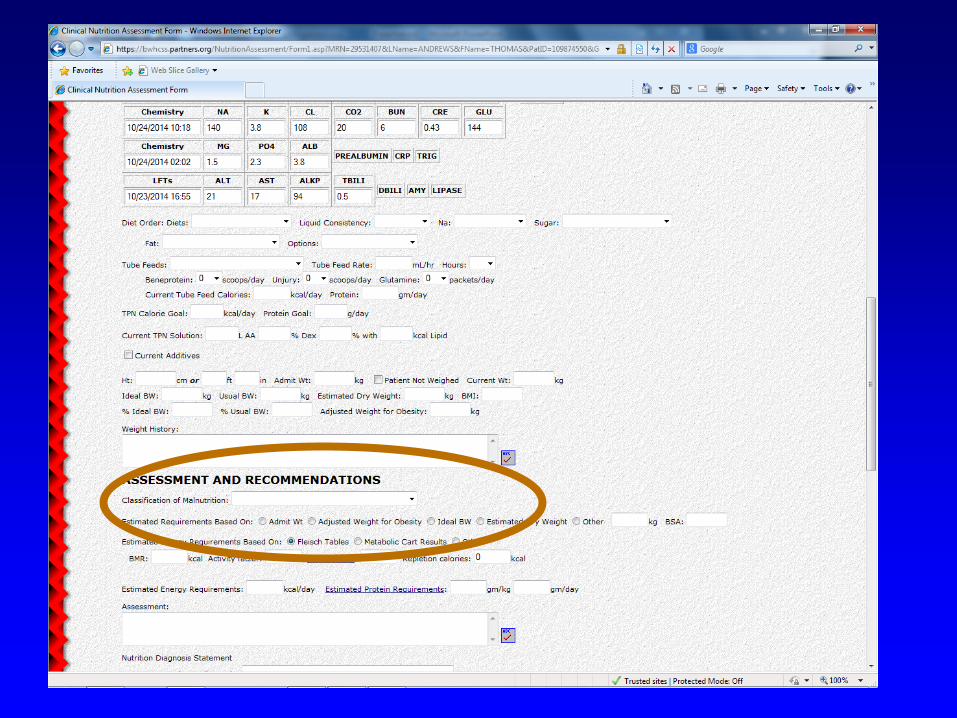
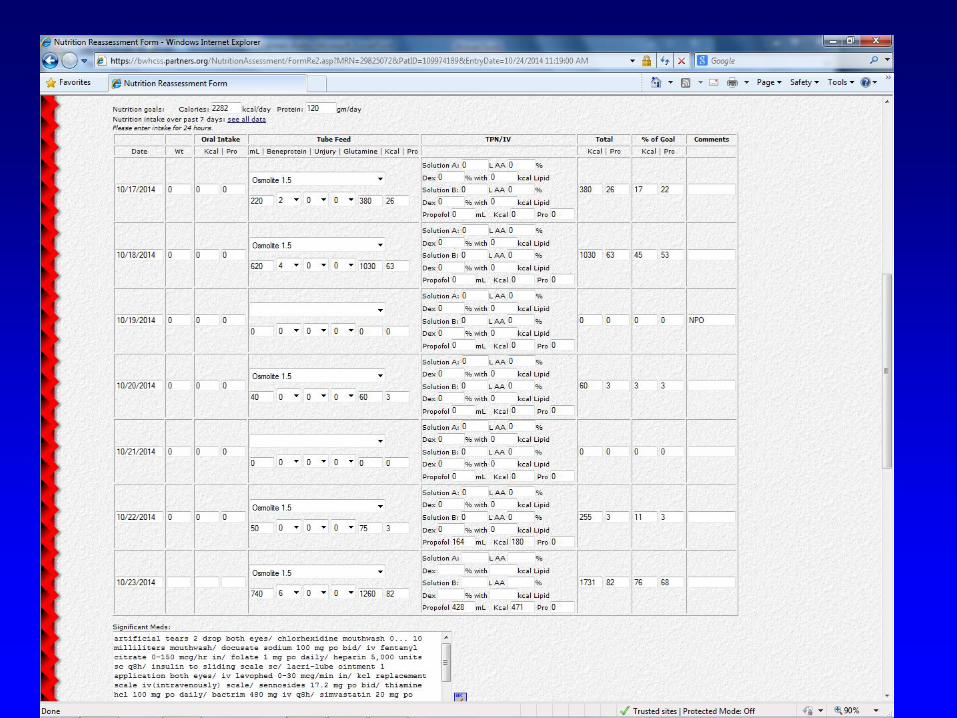
Coding and Data Collection
• We need to continue to work on
getting malnutrition coded
appropriately
• Not just a $$$ issue, but allows for
ongoing research for prevalence and
outcomes
Data Collection and Storage
• If you are still in your building phase
of your EHR or you actually have
programmers who want to work with
you…
– Document data in a structured format
– Limit free text for data

Treatment of Malnourished
Patients
• Is there a difference in clinical
response in malnourished vs. well
nourished patients?
• How do we study this?

Conclusions
• Validation studies of current malnutrition
characteristics are in progress
• Will there be refinement of these characteristics
in the future?
• Keep collecting data and outcomes! Push for
appropriate coding!
• I hope that future research includes other
evaluation tools to expand the characteristics
• Finally, my hope is that future research evaluates
impact of nutrition interventions for malnourished
patients

Thank you!







