
1
A Treatment Based Perspective
Pathophysiology of Type 2 Diabetes
2
Learning Objectives
• Review the pathophysiology of Type 2 Diabetes
Mellitus
• Compare the risks and benefits of oral
hypoglycemic agents in the management of Type
2 Diabetes Mellitus
• Discuss future potential new classes or oral
hypoglycemic agents
3
Adapted from Del Prato S et al. Int J Clin Pract. 2005;59:1345–1355. Permission requested.
Published Conceptual Approach
Earlier and More Aggressive Intervention May Improve Patients’ Chances of Reaching Goal
7
8
6
9
10
A1C,
%
Mean A1C
of patients
Duration of Diabetes
OAD
monotherapy
Diet and
exercise
OAD
combination
OAD
up-titration
OAD +
multiple daily insulin
injections
OAD +
basal insulin
Diagnosis of Diabetes 2010-11 Simplified Screening and Detection
• A1C 6.5% (NGSP, DCCT* standard) – non-fasting test
– Fasting glucose 126 mg/dl (8 hour fast)
– 2 hour glucose 200 mg/dl during OGTT (WHO 75
g test)
• If symptoms of hyperglycemia = random glucose 200 mg/dl
PRE-DIABETES (IFG or IGT)
2-h PG > 200 2-h PG 140 – 199 (IGT)
2-h PG < 140
FPG > 126
FPG > 100 – 125 (IFG)
FPG < 100
DIABETES
NORMAL
A1c > 6.5% A1c 5.7 – 6.4%
A1c < 5.7%
American Diabetes Association. Diabetes Care 34 (Suppl 1), 2011
Glucose Control and Treatment - 2011
• Increasing number of treatments available
– 12 distinct classes of medication, unique
mechanisms
– Majority introduced since 1995
• Increasing numbers of diabetes patients
– Represents 10-20% of unique clinic visits
• Multidrug therapy generally required to achieve
targets
– More than 90% of individuals after 10 years
Supports the application of standardized guidelines
for treatment
ADA/EASD – AACE – Others
The Pathophysiology of Type 2 Diabetes
Relative insulin
deficiency
Insulin
resistance
Hyperglycemia
T2 diabetes and pre-diabetes
Adapted from Kendall DM, et al. Am J Med. 2009;122(6 Suppl):S37-50.
Relative insulin
deficiency
Insulin
resistance

2
The Pathophysiology of Type 2 Diabetes
Impaired
incretin effect
Relative insulin
deficiency
Insulin
resistance
Hyperglycemia
T2 diabetes and pre-diabetes
Adapted from Kendall DM, et al. Am J Med. 2009;122(6 Suppl):S37-50.
Incretins
• Gut hormones secreted from intestinal cells in
response to nutrient stimulus which have
favorable effects on glucose metabolism
• Major incretins in humans1,2:
– Glucagon-like peptide-1 (GLP-1)
– Glucose-dependent insulinotropic polypeptide
(GIP)
• Oral glucose elicits greater insulin response
than IV glucose (i.e. the “incretin effect”)
1Drucker DJ. Diabetes Educator. 2006;32(Suppl 2):65S-71S. 2Vilsbøll T, Holst JJ. Diabetologia. 2004;47:357-366.
Time, min
IR In
su
lin
, m
U/L
nm
ol/L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
180 60 120 0
The Incretin Effect
Control Subjects
(n=8)
Type 2 Diabetics
(n=14)
Time, min
IR In
su
lin
, m
U/L
nm
ol / L
0.6
0.5
0.4
0.3
0.2
0.1
0
80
60
40
20
0
180 60 120 0
Oral glucose load Intravenous (IV) glucose infusion
Incretin
Effect
The incretin effect
is diminished
in type 2 diabetes.
Adapted from Nauck M et al. Diabetologia. 1986;29:46–52. Copyright © 1986 Springer-Verlag.
Permission pending.
10
GLP-1 Modes of Action in Humans
GLP-1 is secreted
from the L-cells
in the intestine
This in turn…
• Stimulates glucose-dependent
insulin secretion • Suppresses glucagon secretion
• Slows gastric emptying
Long term effects demonstrated in animals…
• Increases -cell mass and
maintains -cell efficiency
• Improves insulin sensitivity
• Reduces food intake
Upon ingestion of food…
Drucker DJ. Curr Pharm Des 2001; 7:1399-1412
Drucker DJ. Mol Endocrinol 2003; 17:161-171
Mean (SE); *P < 0.05 GLP-1 = glucagon-like peptide-
1
Glucose-dependent Effects of GLP-1
Glucose (mg/dL) Insulin (pmol/L) Glucagon (pmol/L)
Type 2 Diabetes (n =
10)
Placeb
o GLP-1
270
180
90
0 -30 0 60 120 180 240
300
200
100
0 -30 0 60 120 180 240
20
10
0 -30 0 60 120 180 240
Time (min) Time (min) Time (min)
*
*
*
*
* * *
* * * *
* * *
*
* *
* *
Adapted from Nauck MA, et al. Diabetologia. 1993;36:741–744.
12
Glucoregulatory Role of Key Incretin Hormones
GLP-1
Inhibits gastric emptying1,2
Reduces food intake and
body weight2
Inhibits glucagon secretion from
alpha cells in a glucose-dependent
manner1
Stimulates insulin response from
beta cells in a glucose-dependent
manner1
Is released from L cells in ileum and
colon1,2
GIP
Has no significant effects on satiety
or body weight2
Does not affect gastric emptying2
Stimulates insulin response from
beta cells in a glucose-dependent
manner1
Is released from K cells in
duodenum1,2
GLP-1=glucagon-like peptide-1; GIP=glucose-dependent insulinotropic peptide.
1. Meier JJ et al. Best Pract Res Clin Endocrinol Metab. 2004;18:587–606.
2. Drucker DJ. Diabetes Care. 2003;26:2929–2940.

3
13
Intestinal
GLP-1
Release
GLP-1
Inactive
(~80% of pool)
GLP-1
Active
DPP-4
t1/2 = 1 to 2 min
Intestinal
GIP
Release
DPP-4i
DPP-4 Degrades GLP-1
Meal
Drucker DJ. Diabetes Care. 2003;26:2929–2940.
DPP-4= dipeptidyl dipeptidase-4; GLP-1=glucagon-like peptide-1;
GIP=glucose insulinotropic peptide
DPP- 4 Inhibition and Plasma Levels of GLP-1
• DPP- 4 inhibition:
– Prevents the degradation of active GLP-1 levels
– Does not stimulate GLP-1 secretion
– Does not prevent the kidney from rapidly clearing
GLP-11-3
– Decreases secretion of GLP-1, likely via negative
feedback inhibition of the L cell3,4
• Sitagliptin, saxogliptin DPP-4 inhibitors approved
in U.S.5
1. Drucker DJ. Diabetes Care. 2007;30:1335-1343;
2. Herman GA, et al. J Clin Endocrinol Metab.2006; 91:4612-4619;
3. DPP-4: http://www.glucagon.com/dpp4.html. Updated June 9, 2008. Accessed June 25, 2008 4. Deacon DF, et al. J Endocrinology. 2002;172:355-362
Glu
co
se
(mg
/dL
)
bo
dy
weig
ht
Diabetes
diagnosis
50
100
150
200
250
300
350
Fasting glucose
Adapted from Kendall DM, et al. Am J Med. 2009;122(6 Suppl):S37-50.
Years
Rela
tive a
mo
un
t
-10 -5 0 5 10 15 20 25 30
Insulin resistance
Insulin level
Onset
High risk for diabetes
0
50
100
150
200
250
-15
Natural History of Type 2 Diabetes What Role Can Incretin-Based Therapy Play?
Post-meal glucose
Body weight
ADA/EASD Consensus Algorithm for the Initiation and Adjustment of Therapy
Diabetes Care 2009; 32:193–203
a - Sulfonylureas other than glybenclamide (glyburide) or chlorpropamide.
A1C 6.5 – 7.5%**
Monotherapy
MET +
GLP-1 or DPP4 1
TZD 2
Glinide or SU 5
TZD + GLP-1 or DPP4 1
MET + Colesevelam
AGI 3
2 - 3 Mos.***
2 - 3 Mos.***
2 - 3 Mos.***
Dual Therapy
MET +
GLP-1 or DPP4 1
+
TZD 2
Glinide or SU 4,7
A1C > 9.0%
No Symptoms
Drug Naive Under Treatment
INSULIN
± Other
Agent(s) 6
Symptoms
INSULIN
± Other
Agent(s) 6
INSULIN
± Other
Agent(s) 6
Triple Therapy
AACE/ACE Algorithm for Glycemic
Control Committee
Cochairpersons:
Helena W. Rodbard, MD, FACP, MACE
Paul S. Jellinger, MD, MACE
Zachary T. Bloomgarden, MD, FACE
Jaime A. Davidson, MD, FACP, MACE
Daniel Einhorn, MD, FACP, FACE
Alan J. Garber, MD, PhD, FACE
James R. Gavin III, MD, PhD
George Grunberger, MD, FACP, FACE
Yehuda Handelsman, MD, FACP, FACE
Edward S. Horton, MD, FACE
Harold Lebovitz, MD, FACE
Philip Levy, MD, MACE
Etie S. Moghissi, MD, FACP, FACE
Stanley S. Schwartz, MD, FACE
* May not be appropriate for all patients
** For patients with diabetes and A1C < 6.5%,
pharmacologic Rx may be considered
*** If A1C goal not achieved safely
† Preferred initial agent
1 DPP4 if PPG and FPG or GLP-1 if PPG
2 TZD if metabolic syndrome and/or
nonalcoholic fatty liver disease (NAFLD)
3 AGI if PPG
4 Glinide if PPG or SU if FPG
5 Low-dose secretagogue recommended
6 a) Discontinue insulin secretagogue
with multidose insulin
b) Can use pramlintide with prandial insulin
7 Decrease secretagogue by 50% when added
to GLP-1 or DPP-4
8 If A1C < 8.5%, combination Rx with agents
that cause hypoglycemia should be used with caution
9 If A1C > 8.5%, in patients on Dual Therapy,
insulin should be considered
MET +
GLP-1
or DPP4 1 ± SU 7
TZD 2
GLP-1
or DPP4 1 ± TZD 2
A1C 7.6 – 9.0%
Dual Therapy 8
2 - 3 Mos.***
2 - 3 Mos.***
Triple Therapy 9
INSULIN
± Other
Agent(s) 6
MET +
GLP-1 or DPP4 1
or TZD 2
SU or Glinide 4,5
MET +
GLP-1
or DPP4 1 + TZD 2
GLP-1
or DPP4 1 + SU 7
TZD 2
MET † DPP4 1 GLP-1 TZD 2 AGI 3
Available at www.aace.com/pub
© AACE December 2009 Update. May not be reproduced in any form without express written permission from
AACE
What Makes Treatment Algorithms Successful?
• Evidence based (not solely on acquisition cost)
– Pathophysiologic basis for treatment
– Clinical evidence for treatment choice
• Customized, team-centered approach
– Clinicians – Educator – Pharmacist – Other health
professional
– Training support on use is essential
– Individualized to community, clinical setting
• Established treatment targets and timelines
– Updated on a regular basis
Hirsch IB. Diab Res Clin Pract 2002;58:27-36
Choi SH. Clinical Endocrinol 2008;69:549-555
Sperl-Hillen J. Diabetes 2003 (abstract)

4
Patient age
Disease duration
Comorbidities
Hypoglycemia risk
8.0% 7.0%
Behavioral – social - economic
Higher motivation, knowledge Greater self-care capacity, insight, support
Less motivated, non-adherent, Limited self-care capacity, insight support
Established Complications
None Early Micro Advanced Micro CV
Adapted from Ismael-Beigi F. Ann Intern Med. 2011;154(8):554-9.
6.0%
Individualizing Glycemic Targets in Diabetes
20
Therapeutic Options for Type 2 Diabetes Mellitus
Glucose Lowering Therapy: Diabetes Care 2011 and Beyond
1982-5 1995 2001 1922 1950’s 1996 2003
Sulfonylurea
Human insulin
Lispro
Glinides - AGI
Glargine
Animal insulin
Glitazones
Aspart
2005
Exenatide
Pramlintide
Detemir
Metformin
2007 2009 2011
HYPOGLYCEMIC THERAPY TISSUE EFFECT MULTIPLE TISSUES
Exubera
Sitagliptin
Saxagliptin
Cholesevelam
Liraglutide
Bromocriptine
Linagliptin
22
Major Targets of Oral Drug Classes
DPP-4=dipeptidyl peptidase-4; TZD=thiazolidinediones.
1. DeFronzo RA. Ann Intern Med. 1999;131:281–303.
2. Buse JB et al. In: Williams Textbook of Endocrinology. 2003:1427–1483.
Pancreatic
Islet Cells
↓Glucose level
Muscle and Fat
Liver
Sulfonylureas
Meglitinides
Biguanides
TZDs TZDs
Biguanides
alpha-Glucosidase inhibitors
Gut
DPP-4 inhibitors
DPP-4 inhibitors
24
Insulin Secretagogues Sulfonylureas, Repaglinide, and Nateglinide
Riddle MC. Am Fam Physician. 1999;60:2613-2620; Wolffenbuttel et al. Drugs. 1995;50:263-288;
Horton ES et al. Diabetes Care. 2000;23:1660-1665; Hanefeld M et al. Diabetes Care. 2000;23:202-207;
Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: ADA; 1998
Mechanism of action Increase basal and/or postprandial insulin secretion
Efficacy depends upon Functioning -cells
Power Sulfonylureas, repaglinide: decrease A1C 1%–2%
Nateglinide: decreases A1C 0.5%– 1%
Dosing Sulfonylureas: Qd or BID
Repaglinide, nateglinide: TID or QID with meals
Side effects Weight gain, allergy (rare)
Main risk Hypoglycemia
25
Biguanides Metformin
Riddle MC. Am Fam Physician. 1999;60:2613-2620;
Cusi K et al. Diabetes Rev. 1998;6:89-131
Primary mechanism Decreases hepatic glucose of action production
Efficacy depends upon Presence of insulin
Power Decreases A1C 1%–2%
Dosing 2 or 3 times daily (metformin) 1 or 2 times daily (metformin XR)
Side effects Diarrhea, nausea
Main risk Lactic acidosis, need to
monitor Scr

5
All Cause Mortality (%) at 10 years
• Diet + Metformin 14.6%
• Diet + Sulf/Insulin 20%
• Diet alone 21.7%
– RRR 32.7% with metformin + diet vs. diet alone
– ARR 7.1%
– NNT 14
27
α-Glucosidase Inhibitors Acarbose and Miglitol
Mechanism of action Delay carbohydrate absorption
Efficacy depends upon Postprandial hyperglycemia
Power Decrease A1C 0.5%–1%
Dosing 3 times daily
Side effects Flatulence
Main risk Liver enzyme elevation (rare)
Riddle MC. Am Fam Physician. 1999;60:2613-2620;
Lebovitz HE. Endocrinol Metab Clin North Am. 1997;26:539-551
28
Glitazones (TZDs) Pioglitazone and Rosiglitazone
Mechanism of action Enhance tissue response to insulin
Efficacy depends upon Presence of insulin and resistance to its action
Power Decrease A1C 0.9%–1.6%
Dosing Once daily
Side effects Edema, weight gain, anemia
Main risk Congestive heart failure
Riddle MC. Am Fam Physician. 1999;60:2613-2620; Zinman B. Diabetes Obesity
Metab. 2001;3(suppl 1):S34-S43; Actos (pioglitazone hydrochloride) package insert;
Avandia (rosiglitazone maleate) package insert
TZD’s and Fractures ADA Annual Meeting 6/25/2010
• A retrospective analysis conducted by the Scottish Diabetes Research Network of more than 90% of all patients with diabetes in Scotland. About 144,000 patients met the study criteria, taking at least 1 oral antidiabetic agent but not insulin, during the 2000 to 2008 study period.
• Thiazolidinediones also elevate the risk of hip fracture in women by 1.9 times (P<0.001) and in men by 2.23 times ( P=0.016) for a combined hazard ratio of 1.98 (P<0.0001).
– “We calculate that up to 17% of all hip fractures in the diabetic population can be attributed to TZDs.”
DPP-4 Inhibitors
Advantages
• No hypoglycemia
• Weight neutral
• Rapid onset of action
• Able to use in renal
dysfunction
• Few side effects
• No drug interactions
• May preserve cells
Disadvantages
• New medications
• No long-term
studies
• Weight neutral
• Only physiologic
incretin levels
• ? waning efficacy
32
Mean
Ch
an
ge i
n A
1C
, %
c
aCompared with placebo. bLeast squares mean (LSM) adjusted for prior antihyperglycemic therapy status and baseline value. cDifference
from placebo. dCombined number of patients on sitagliptin or placebo. eP<0.001 overall and for treatment-by-subgroup interactions.
CI, confidence interval.
1. Raz I et al. Diabetologia. 2006;49:2564–2571.
2. Aschner P et al. Diabetes Care. 2006;29:2632–2637.
Mean baseline A1C: 8.0%
P < 0.001a
–0.6b
–1.0
–0.8
–0.6
–0.4
–0.2
0.0
–0.8b
Placebo-Adjusted Results
24-week monotherapy study2
(95% CI: –1.0, –0.6)
18-week monotherapy study1
(95% CI: –0.8, –0.4)
n=193
n=229
Inclusion criteria A1C: 7%–10%
Overall <8 ≥8–<9 ≥9 Baseline A1C, %
–1.4
–0.6 –0.7
–1.8
–1.6
–1.4
–1.2
–1.0
–0.8
–0.6
–0.4
–0.2
0.0
n=411d
n=239d
n=119d
Mean
Ch
an
ge i
n A
1C
, %
Prespecified pooled analysis at 18 weekse
–0.7
n=769d
Sitagliptin Monotherapy Studies: A1C Reductions
Study 021 and 023

6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
8.0 7.7 7.9 8.0 7.9 7.8
Adjusted Mean Change from Baseline in HbA1c
at Week 12: Low-Dose Cohort
Ad
jus
ted
me
an
ch
an
ge
in
Hb
A1
c (
%)
*
* P<0.007
*
* *
*
Saxagliptin
Placebo 2.5 mg 5 mg 10 mg 20 mg 40 mg
(n=67) (n=55) (n=47) (n=63) (n=54) (n=52)
Dose
Rosenstock, J. et al., Diabetes Obes Metab 2008;10:376-386.
Colesevelam
• Indicated as an adjunct to diet and exercise to
improve glycemic control in adults with type 2
diabetes mellitus
• Not for treatment of type 1 DM or DKA
• Mechanism of action uncertain
• Contraindications:
– History of bowel obstruction
– Serum triglycerides >500 mg/dL
– History of hypertriglyceridemia-induced
pancreatitis
Colesevelam: Efficacy
• Not studied as monotherapy or in combination
with incretins
• Not extensively studied in combination w/ TZDs
• Clinical trials with pre-existing diabetes therapy
– A1c reductions of 0.5-0.8% as add-on to
metformin, sulfonylurea, or insulin therapy
– Significant LDL-C reductions of 12.3-16.1% vs.
placebo
Bays HE, et al. Arch Intern Med. In press. Fonseca VA, et al. Diabetes Care. 2008; 31: 1479-1484.
Goldberg RB, et al. Arch Intern Med. 2008; 168: 1531-1540.
38 Colesevelam HCl Improves Glycemic Control and Reduces LDL Cholesterol in Patients With Inadequately
Controlled Type 2 Diabetes on Sulfonylurea-Based Therapy
• Significantly reduced A1C and LDL cholesterol in
patients with type 2 diabetes when added to a
sulfonylurea based therapy.
• Colesevelam therapy was safe and well tolerated in
this study.
• No patient reported a severe episode of
hypoglycemia, and none discontinued due to
hypoglycemia.
• Colesevelam did not result in weight gain.
Fonseca VA et al. Diabetes Care 31:1479-1484, 2008
39
Efficacy of Oral Antihyperglycemics Declines With Time
• A1C rises at ~0.2% to 0.3% yearly on stable
therapy
• This rate is the same as for diet alone,
sulfonylureas, and metformin
• -Cell function declines at the same rate with all
these treatments
• Combination treatments are routinely needed
UKPDS Group. Diabetes. 1995;44:1249-1258; Turner RC et al. JAMA. 1999;281:2005-2012
40
Secondary Failure of Monotherapy Overweight Patients in the UKPDS
Turner RC et al. UKPDS 49. JAMA. 1999;281:2005-2012
Percent with A1C <7% on monotherapy
Diet 23 12 11
Sulfonylureas 45 28 21
Metformin 44 34 13
3 years 6 years 9 years

7
41
Cumulative incidence of monotherapy failure (FPG> 180 mg/dL)
Kahn. SE, et al. N Engl J Med 2006;355:2427-43
42
Estimated Improvements in Glycemic Control
DeFronzo, et al. N Engl J Med 1995;333:541-549; Horton, et al. Diabetes Care. 1998;21:1462-1469; Coniff, et al.
Diabetes Care.
1995;18:817-824; Moses, et al. Diabetes Care 1999;22:119-124; Schneider, et al. Diabetes 1999; 48 (Suppl 1): A106;
Egan, et al. Diabetes 1999; 48 (Suppl 1):A117. Fonseca, et al. Diabetes 1999:48 (Suppl 1):A100.
Regimen HbA1c FBG
Sulfonylurea + metformin ~1.7% ~65 mg/dL
Sulfonylurea + troglitazone ~0.9-1.8% ~50-60 mg/dL
Sulfonylurea + pioglitazone ~1.2% ~50 mg/dL
Sulfonylurea + acarbose ~1.3% ~40 mg/dL
Repaglinide + metformin ~1.4% ~40 mg/dL
Pioglitazone + metformin ~0.7% ~40 mg/dL
Rosiglitazone + metformin ~0.8% ~50 mg/dL
Insulin + oral agents Open to Target Open to Target
COMBINATION THERAPY
43
Initial Combination Therapy With Sitagliptin Plus Metformin Study: A1C Results From Patients not
on Antihyperglycemic Therapy at Study Entry
LS
M C
ha
ng
e
Fro
m B
as
elin
e,
%
Study 036
–1.1
n=88
–1.1
n=90
–1.2
n=87
–1.6
n=100
–1.9
n=86
–2.0
–1.8
–1.6
–1.4
–1.2
–1.0
–0.8
–0.6
–0.4
–0.2
0
–0.2
n=83
Sitagliptin 50 mg + metformin 1,000 mg bid
Metformin 1,000 mg bid
Sitagliptin 50 mg + metformin 500 mg bid
Metformin 500 mg bid Sitagliptin 100 mg qd Placebo
LSM=least squares mean change.
Data available on request from Merck & Co., Inc.
44
Initial Combination Therapy With Sitagliptin Plus Metformin Study: Change in
Body Weight and Incidence of Hypoglycemia
Placebo
Sita
100
MF
500
bid
MF
1,000
bid
Sita
50 +
MF 500
bid
Sita
50 +
MF 1,000
bid
Hypoglycemia
n/N (%)
1/176
(0.6)
1/179
(0.6)
1/182
(0.5)
2/182
(1.1)
2/190
(1.1)
4/182
(2.2)
LSM Change
From Baseline, kg
–2
–1
0
1
167 184 178 175 179 175
Rates of Hypoglycemia in
Combination With Sitagliptin
Sitagliptin 50 mg + metformin 1,000 mg bid Metformin 1,000 mg bid Sitagliptin 100 mg qd
Sitagliptin 50 mg + metformin 500 mg bid Metformin 500 mg bid Placebo
Sita=sitagliptin; MF=metformin.
Goldstein B et al. Diabetes Care. 2007;30:1979–1987.
Glycemic Targets
Self-Management • Refer for diabetes education
• SMBG, food & activity
Nutrition and Activity • Refer for Medical Nutrition Therapy
• May lower A1C 1-2 %
SMBG pre-meal 70-120 mg/dL, post-meal <160
mg/dL
A1C < 7%
Emotional Health • Psychosocial support / motivation
• Assess for anxiety and/or depression
Advance/initiate drug treatment if not at target
METFORMIN If not tolerated or if contraindicated select initial
therapy from TWO DRUG THERAPY below
At Presentation
A1C 7-8.9%
FPG 150-200 mg/dL
RPG 200-300 mg/dL
Titrate to clinically effective dose Advance if not at target in 3 months
TWO DRUG THERAPY
Incretin Defect Insulin Deficiency Insulin Resistance
A1C 9-11%
FPG 201-300 mg/dL
RPG 301-350 mg/dL
Treatment of Type 2 Diabetes: Glycemic Control
© Copyright International Diabetes Center (IDC) 2009. From
www.internationaldiabetescenter.com
Add Sulfonylurea Glimepiride or Glipizide XL
Rapid glucose lowering
Long history of use
Lowest cost
Risk of hypoglycemia, weight gain
Add DPP-4 Inhibitor Sitagliptin – Saxagliptin
Linagliption
Well tolerated, simple oral
dosing
No hypoglycemia
Higher cost
Weight neutral
Add GLP -1 Agonist Exenatide - Liraglutide
Weight loss, no hypoglycemia
Injectable (pen)
Higher cost
GI side effects - nausea
Add PPAR Agonist Pioglitazone
Targets insulin resistance, CV risk
Improves lipids (HDL, TG)
Higher cost
Edema, weight gain, bone effects Advance if not at target in 3 months Titrate to clinically effective dose
THREE DRUG THERAPY
Add Background Insulin* or TZD, SU Add Background Insulin
or
TZD, DPP-4, GLP-1
Background & Mealtime (main meal) + Oral Agent(s)* Premixed Insulin + Sensitizer(s)*
MULTI-DOSE INSULIN THERAPY
* Limited published data for use of
insulin plus either DPP-4 inhibitor or
GLP-1 agonist
Add Background Insulin
or
SU, DPP-4, GLP-1 A1C >11%
FPG >300 mg/dL
RPG >350 mg/dL
Start
Background or
Premix Insulin +
Metformin
Background & Mealtime (all meals) + Sensitizer(s)*
Glu
co
se
(mg
/dL
)
bo
dy
weig
ht
Diabetes
diagnosis
50
100
150
200
250
300
350
Fasting glucose
Adapted from Kendall DM, et al. Am J Med. 2009;122(6 Suppl):S37-50.
Years
Rela
tive a
mo
un
t
-10 -5 0 5 10 15 20 25 30
Insulin resistance
Insulin level
Onset
High risk for diabetes
0
50
100
150
200
250
-15
Post-meal glucose
Body weight
Weight loss
& Activity Insulin
Incretin therapy
Secretagogue
Metformin
TZD
8
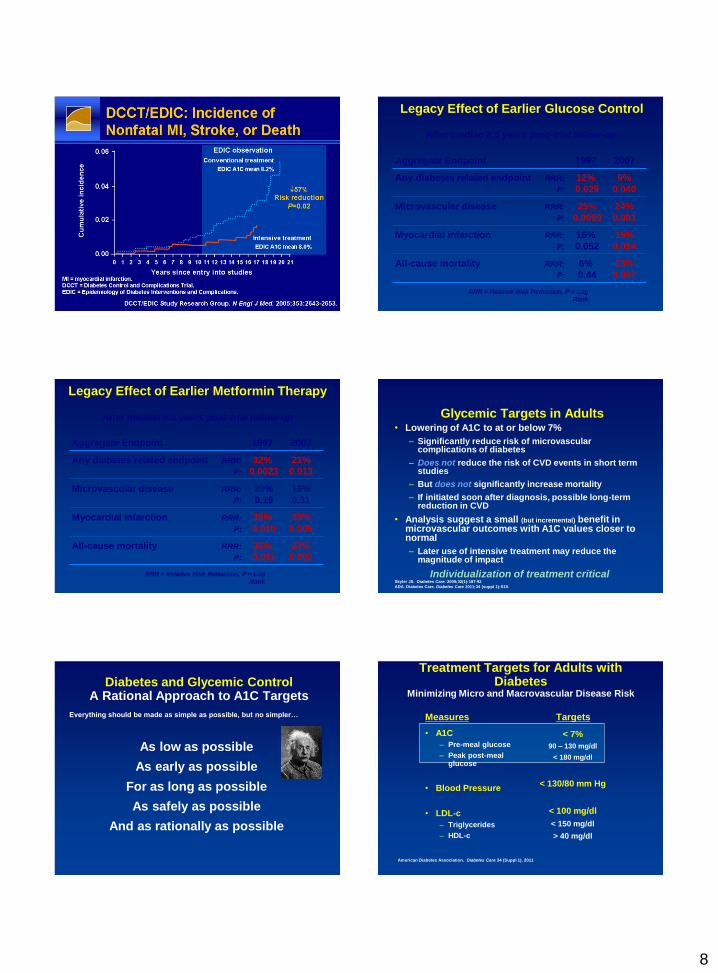
DCCT/EDIC: Incidence of Nonfatal MI, Stroke, or Death After median 8.5 years post-trial follow-up
Aggregate Endpoint 1997 2007
Any diabetes related endpoint RRR: 12% 9%
P: 0.029 0.040
Microvascular disease RRR: 25% 24%
P: 0.0099 0.001
Myocardial infarction RRR: 16% 15%
P: 0.052 0.014
All-cause mortality RRR: 6% 13%
P: 0.44 0.007
RRR = Relative Risk Reduction, P = Log
Rank
Legacy Effect of Earlier Glucose Control
After median 8.8 years post-trial follow-up
Aggregate Endpoint 1997 2007
Any diabetes related endpoint RRR: 32% 21%
P: 0.0023 0.013
Microvascular disease RRR: 29% 16%
P: 0.19 0.31
Myocardial infarction RRR: 39% 33%
P: 0.010 0.005
All-cause mortality RRR: 36% 27%
P: 0.011 0.002
RRR = Relative Risk Reduction, P = Log
Rank
Legacy Effect of Earlier Metformin Therapy
Glycemic Targets in Adults • Lowering of A1C to at or below 7%
– Significantly reduce risk of microvascular complications of diabetes
– Does not reduce the risk of CVD events in short term studies
– But does not significantly increase mortality
– If initiated soon after diagnosis, possible long-term reduction in CVD
• Analysis suggest a small (but incremental) benefit in microvascular outcomes with A1C values closer to normal
– Later use of intensive treatment may reduce the magnitude of impact
Individualization of treatment critical
Skyler JS. Diabetes Care. 2009;32(1):187-92
ADA. Diabetes Care. Diabetes Care 2011;34 (suppl 1):S19.
Diabetes and Glycemic Control A Rational Approach to A1C Targets
As low as possible
As early as possible
For as long as possible
As safely as possible
And as rationally as possible
Everything should be made as simple as possible, but no simpler…
Treatment Targets for Adults with Diabetes
Minimizing Micro and Macrovascular Disease Risk
Measures
• A1C
– Pre-meal glucose
– Peak post-meal glucose
• Blood Pressure
• LDL-c
– Triglycerides
– HDL-c
Targets
< 7%
90 – 130 mg/dl
< 180 mg/dl
< 130/80 mm Hg
< 100 mg/dl
< 150 mg/dl
> 40 mg/dl
American Diabetes Association. Diabetes Care 34 (Suppl 1), 2011

9







