Journey of Beta blockers
From hypertension to heart failure
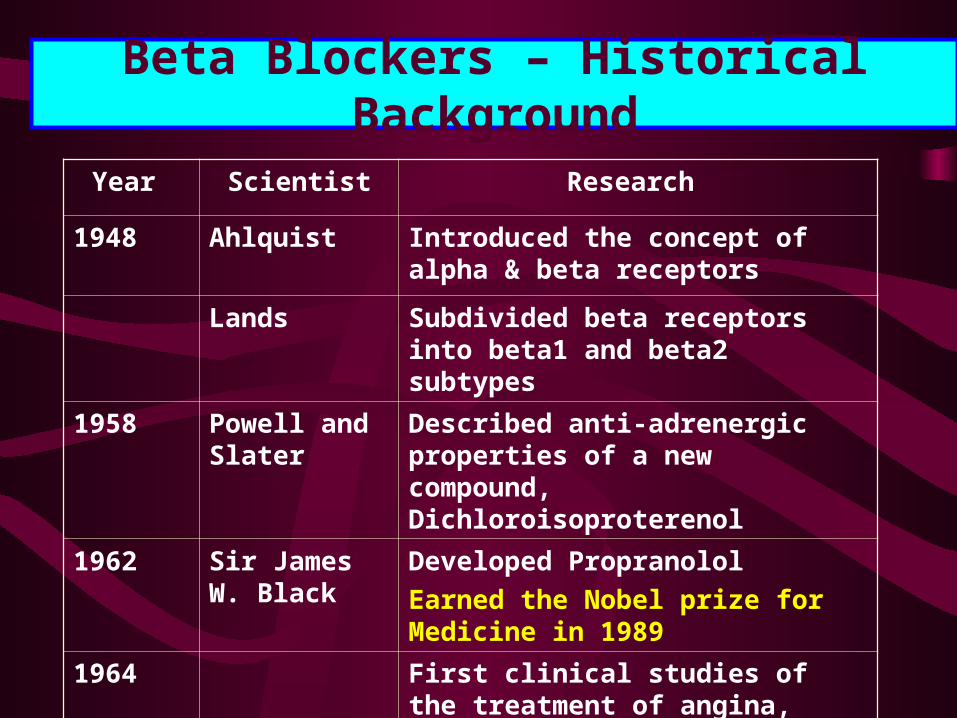
Beta Blockers – Historical Background
Year Scientist Research
1948 Ahlquist Introduced the concept of alpha & beta receptors
Lands Subdivided beta receptors into beta1 and beta2 subtypes
1958 Powell and Slater
Described anti-adrenergic properties of a new compound, Dichloroisoproterenol
1962 Sir James W. Black
Developed Propranolol
Earned the Nobel prize for Medicine in 1989
1964 First clinical studies of the treatment of angina, arterial rhythm and hypertension disorders

Beta Blockers – Historical Background
• Remarks by the Nobel Committee in 1988 about the research of Sir James W. Black “the greatest breakthrough when it comes to pharmaceuticals against heart illness since the discovery of digitalis 200 years ago”.
Radford et.al. NEJM, 1998, Vol. 339:551-553

Beta Blockers
Drugs
Nonselective beta1 & beta2 adrenergic antagonists
Propranolol
Sotalol
Selective beta1 adrenergic antagonists
Atenolol
Bisoprolol
Celoprolol
Nebivolol
Metoprolol
Alpha1 & beta1 adrenergic antagonists
Carvediol
Labetolol

Beta Blockers
Lipid solubility
Peripheral vasodilation
Average daily dosage
Propranolol High 40-80 mg
Sotalol Low 160-320 mg
Atenolol Low 25-100 mg
Bisoprolol Moderate 2.5-10 mg
Celoprolol Moderate + 200-600 mg
Nebivolol Moderate + 2.5-5 mg
Metoprolol High 50-100 mg
Carvediol Moderate + 3.125-50 mg
Labetolol Low + 200-800 mg

Beta blockers
Indications
• Hypertension
• Angina pectoris
• Post-myocardial infarction
• Tachyarrhythmias
• Congestive heart failure

Beta blockers in hypertension
• Atenolol has been most extensively studied in patients with essential hypertension
• Reductions in blood pressure in patients with mild to severe hypertension have been associated with reduced mortality from both stroke and myocardial ischaemia.
Sethi KK et al, Cardiology Today, 2002
Recommended as first line treatment in Hypertension by
•European Society of Hypertension Guidelines
•British Hypertensive Society Guidelines

Beta-blockers in Hypertension
• Established long term mortality and morbidity benefits
• Beta blockers significantly reduce:
Sudden cardiac death
Overall coronary events
Incidence of stroke

Beta Blockers The Cornerstone Of IHD Therapy
• Beta blockade is a standard therapy for effort angina, mixed effort and rest angina and unstable angina.
• Beta blockers decrease mortality in acute MI and in post MI period.
• Beta blockers retain their position among basic therapies of numerous other conditions including hypertension, arrhythmia and cardiomyopathy.
Opie.L.H., Drugs for Heart, 2001
Beta Blockers In acute coronary syndromes
• A summary analysis of randomized trials with threatened or evolving MI showed lower rates of progression to MI with beta-blocker treatment.
www.acc.org/clinical/practice_advisory/ pdfs/COMMITBetaBlockerFACTSheet.pdf
Beta blockers in post MI
• In post MI patients, beta blockers limit infarct size, reduce angina episodes, reinfarction, suppress tachyarrhythmias and sudden cardiac death and improve survival
Roy CP et al, Cardiology Today, 2002
•Life saving potentials of the drugs in IHD are:
-blockers : 33%
Statins : 30%
Aspirin : 23%
Cardiac Drug Therapy, M. Gabriel Khan, Saunder; 1999
Beta blockers in MI
• Reduce mortality during both acute and long-term management of myocardial infarction.
Howard et al., American Family Physician, 2000
• Benefit occurred regardless of the patient's age or sex, infarct location and initial heart rate, or the presence or absence of ventricular arrhythmias.
Lamb RK et al, Eur Heart J. 1988 Jan;9(1):32-6
• Studies indicate that the most marked reduction in mortality (25 percent) occurs in the first two days after infarction.
Yusuf S. et al., JAMA. 1988 Oct 14;260(14):2088-93
Beta blockers in MI
As per ACC/AHA guidelines:
- Recommends beta blocker therapy early during an ongoing MI
- Treatment is recommended in all patients so long as contraindications does not exist, irrespective of whether the patient receives concomitant thrombolytic therapy or primary angioplasty
http://circ.ahajournals.org/cgi/reprint/100/9/1016.pdf

“Beta blockers continue to surprise us”
Cruikshank, Eur. Heart J., 2000

Use of beta-blockers in hypertensive diabetic
CLINICAL EVIDENCE

UKPDSTHE UK PROSPECTIVE DIABETES STUDY
LANDMARK STUDY• Multi-center randomized controlled trial of
different therapies of type II diabetes
• Clinical centers: 23• Type II diabetic patients: 5102• Person years follow up: 53000

UKPDSBLOOD PRESSURE CONTROL STUDY
To determine whether
• Tight blood pressure control policy can reduce the morbidity and mortality in type II diabetes patients
• ACE inhibitor(Captopril) or beta blocker (Atenolol) is advantageous in reducing the risk of development of clinical complications.

ukpds
Blood Pressure : ACE inhibitor vs Beta blockerBlood Pressure : ACE inhibitor vs Beta blocker
60
80
100
140
160
180
0 2 4 6 8
mm
Hg
Years from randomisation
cohort, median values
Less tight control ACE inhibitor Beta blocker
ukpds
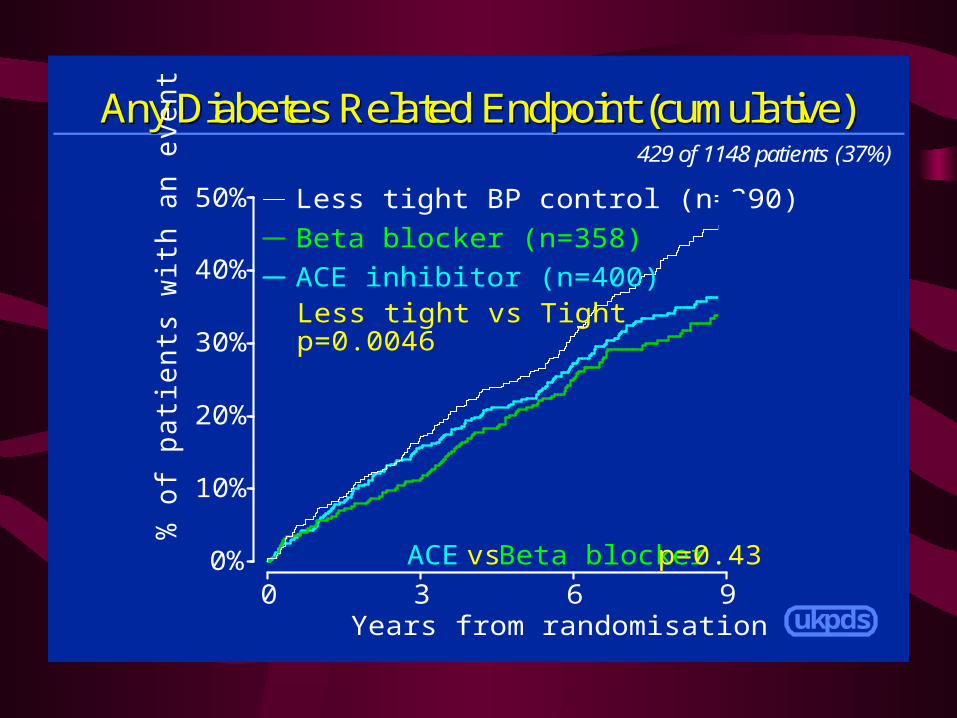
Any Diabetes Related Endpoint (cumulative)Any Diabetes Related Endpoint (cumulative)429 of 1148 patients (37%)
0%
10%
20%
30%
40%
50%
0 3 6 9
% o
f patie
nts
with
an e
vent
Years from randomisation
ACE inhibitor (n=400)
Beta blocker (n=358)
Less tight BP control (n=390)
ACE vs Beta blocker p=0.43
Less tight vs Tightp=0.0046

ukpds
Diabetes Related Deaths (cumulative)Diabetes Related Deaths (cumulative)144 of 1148 patients (13%)
0%
5%
10%
15%
20%
0 3 6 9
% o
f patie
nts
with
an e
vent
Years from randomisation
ACE inhibitor (n=400)
Beta blocker (n=358)
Less tight BP control (n=390)
ACE vs Beta blocker p=0.28
Less tight vs Tightp=0.019

ukpds
Microvascular Endpoints (cumulative)Microvascular Endpoints (cumulative)renal failure or death, vitreous haemorrhage or photocoagulation
122 of 1148 patients (11%)
0%
5%
10%
15%
20%
0 3 6 9
% o
f patie
nts
with
an e
vent
Years from randomisation
ACE inhibitor
Beta blocker
Less tight BP control
ACE vs Beta blocker p=0.30
Less tight vs Tightp=0.0092
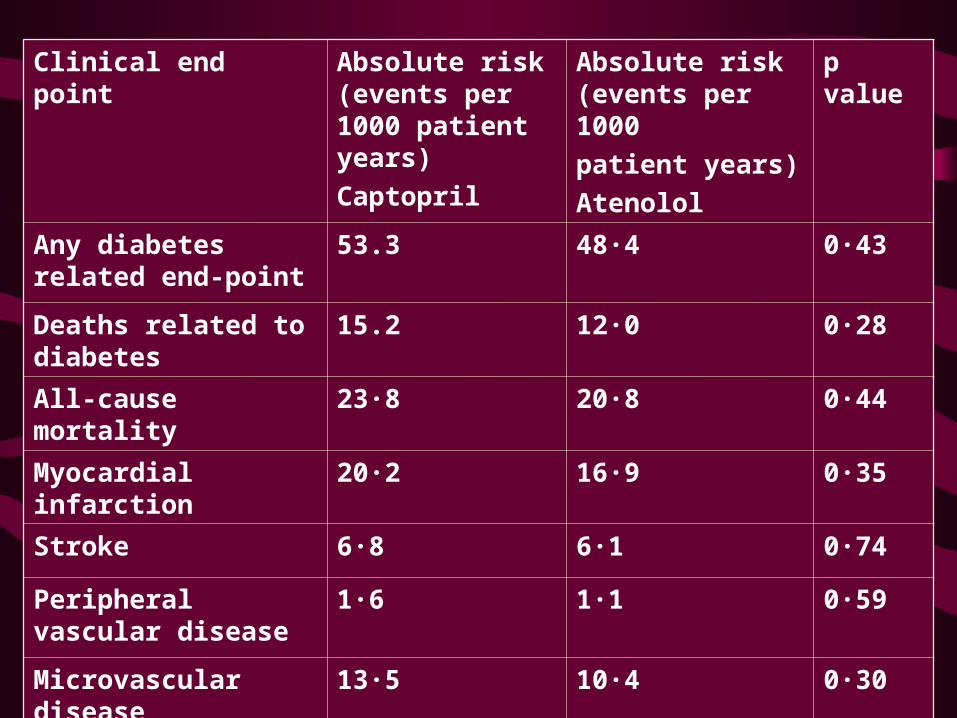
Clinical end point Absolute risk (events per 1000 patient years)
Captopril
Absolute risk (events per 1000
patient years)
Atenolol
p value
Any diabetes related end-point
53.3 48·4 0·43
Deaths related to diabetes
15.2 12·0 0·28
All-cause mortality 23·8 20·8 0·44
Myocardial infarction 20·2 16·9 0·35
Stroke 6·8 6·1 0·74
Peripheral vascular disease
1·6 1·1 0·59
Microvascular disease
13·5 10·4 0·30

UKPDSBLOOD PRESSURE CONTROL STUDY
Conclusion
ACE inhibitors and beta blockers were equally effective in lowering mean blood pressure in hypertensive patients with type II diabetes and in reducing the risk of
– any diabetes related endpoints– diabetes related deaths – microvascular end-points
Use of beta-blockers in heart failure

Use of beta-blockers in heart failure
A Bayesian Meta-Analysis
• 22 trials
• 10 135 patients
James M. Brophy et al, Ann Intern Med. 2001;134:550-560.

Study Year Drug Duration NYHA class
Anderson et al 1985 Metoprolol 19 II–IV
Engelmeier et al. 1985 Metoprolol 12 II–IV
Pollock et al. 1990 Bucindolol 3 II–IV
Woodley et al. 1991 Bucindolol 3 II–III
Paolisso et al. 1992 Metoprolol 3 I–IV
Waagstein et al. 1993 Metoprolol 18 II–III
Wisenbaugh et al. 1993 Nebivelol 3 II–IV

Study Year Drug Duration NYHA class
Fisher et al 1994 Metoprolol 6 II–IV
Bristow et al. 1994 Bucindolol 3 I–IV
CIBIS-I 1994 Bucindolol 23 III–IV
Eichhorn et al. 1994 Metoprolol 3 II–III
Metra et al. 1994 Carvediol 3 II–III
Olsen et al. 1995 Carvediol 4 II–IV
Krum et al. 1995 Carvediol 4 II–IV

Study Year Drug Duration NYHA class
Bristow et al 1996 Carvediol 6 II–IV
Packer et al. 1996 Carvediol 6 II–IV
Colucci et al. 1996 Carvediol 15 II–III
Cohn et al. 1997 Carvediol 8 II–IV
Aust/Nz 1997 Carvediol 19 II–III
CIBIS-II 1999 Bisoprolol 15 III–IV
MERIT-HF 1999 Metoprolol 12 II–IV
RESOLVED 2000 Metoprolol 6 II–IV

Significantly less no. of deaths
Placebo Beta-blocker therapy
Deaths 624/ 4862 444 /5273
% of deaths 12 8
4 lives saved per 100 patients
James M. Brophy et al, Ann Intern Med. 2001;134:550-560.
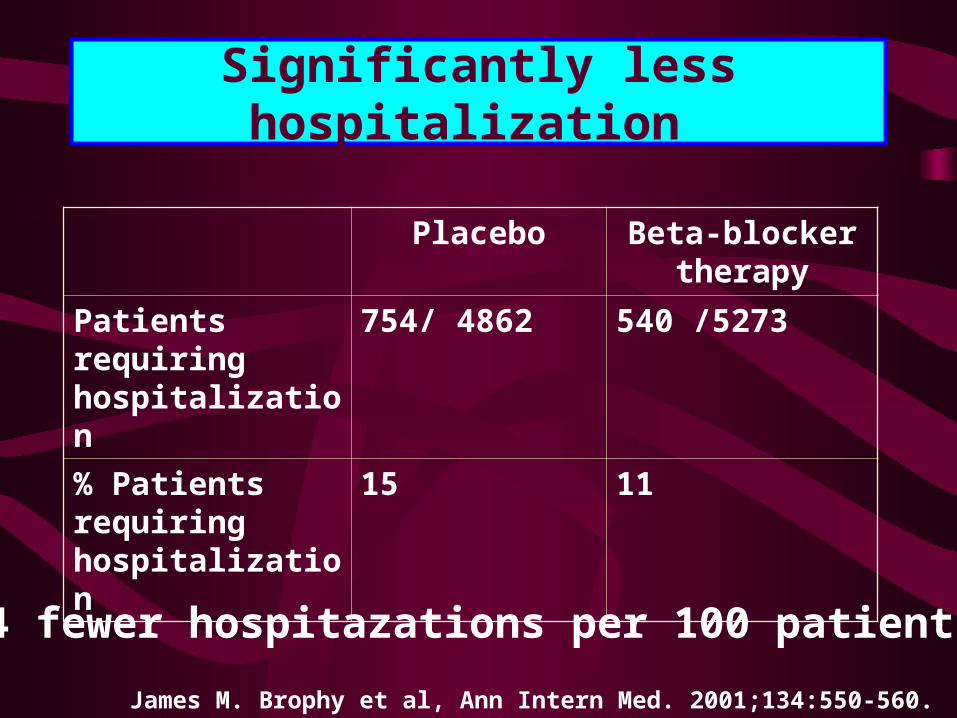
Significantly less hospitalization
Placebo Beta-blocker therapy
Patients requiring hospitalization
754/ 4862 540 /5273
% Patients requiring hospitalization
15 11
4 fewer hospitazations per 100 patients
James M. Brophy et al, Ann Intern Med. 2001;134:550-560.
• Beta-Blocker therapy is associated with clinically meaningful reductions in mortality and morbidity in patients with stable congestive heart failure and should be routinely offered to all patients similar to those included in trials.
The probability that beta-blocker therapy reduced total mortality and hospitalizations for congestive heart failure was almost 100%.
James M. Brophy et al, Ann Intern Med. 2001;134:550-560.
Tolerability of Beta Blockers
• In a meta-analysis of 90 comparative studies of angina, beta blockers were found to be associated with a lower incidence of adverse effects than calcium antagonists.
(Heidenreich et al, JAMA. 1999 May 26;281(20):1927-36.
1-selective blockers such as atenolol appear to be better tolerated than nonselective agents
(Dahlof et al, Circulation, 1991)
Tolerability of Beta Blockers
1-selective blockers are generally equivalent to the ACE inhibitors and calcium antagonists in terms of impact on quality of life.
(Landray MJ et al, J Clin Pharm Ther. 2002 Aug;27(4):233-42. Review)
In patients with reactive airway disease
Meta-analysis of 19 clinical studies•Cardioselective beta-blockers do not produce clinically significant adverse respiratory effects in patients with mild to moderate reactive airway disease. The results were similar for patients with concomitant chronic airways obstruction. •Given their demonstrated benefit in such conditions as heart failure, cardiac arrhythmias, and hypertension, cardioselective beta-blockers should not be withheld from patients with mild to moderate reactive airway disease.
Salpeter SR et al, Ann Intern Med. 2002 Nov 5;137(9):715-25

METOPROLOL
AT A GLANCE

METOPROLOL
• Metoprolol, a relatively selective beta1-blocker, is devoid of intrinsic sympathomimetic activity and possesses weak membrane stabilising activity.
Prakash A et al, Drugs. 2000 Sep;60(3):647-78

METOPROLOL
• Well established in cardiovascular medicine
• Particularly useful in the management of hypertension and ischaemic heart disease.
Plosker GL et al, Drugs. 1992 Mar;43(3):382-414
METOPROLOL
In hypertension, post-myocardial infarction and idiopathic dilated cardiomyopathy
• Beneficial effects on morbidity and mortality, or closely-related end-points.
• Improves quality of life
Peters DH SR et al, Pharmacoeconomics. 1994 Oct;6(4):370-400
METOPROLOL
Controlled release metoprolol • Release the drug at a relatively constant
rate over a 24-hour period• Producing sustained and consistent
metoprolol plasma concentrations and beta 1-blockade while retaining the convenience of once daily administration.
Plosker GL et al, Drugs. 1992 Mar;43(3):382-414
METOPROLOL
Controlled release metoprolol • Similar or lesser degree of adverse effects
related to the central nervous system compared with atenolol or long acting propranolol.
• Less pronounced beta 2-mediated bronchoconstrictor effects than atenolol in asthmatics, and less general fatigue and leg fatigue in healthy subjects.
• These results are presumably due to the beta 1-selectivity of metoprolol in addition to the the avoidance of high peak plasma concentrations.
Plosker GL et al, Drugs. 1992 Mar;43(3):382-414

METOPROLOLIN HEART FAILURE
• Trials in mild to moderate (NYHA functional class II to III) chronic heart failure
MERIT-HF • Metoprolol CR/XL Randomised Intervention
Trial in Congestive Heart Failure trial
RESOLVD • Randomized Evaluation of Strategies for Left
Ventricular Dysfunction pilot study.
Prakash A et al, Drugs. 2000 Sep;60(3):647-78

METOPROLOLIN HEART FAILURE
MERIT-HF
• Treatment with metoprolol CR/XL was initiated at a low dosage of 12.5 to 25 mg once daily and gradually increased at 2-weekly intervals until the target dosage (200 mg once daily) or maximal tolerated dosage had been attained in patients receiving standard therapy for heart failure.
Prakash A et al, Drugs. 2000 Sep;60(3):647-78
METOPROLOLIN HEART FAILURE
MERIT-HF • At 12 months, metoprolol CR/XL was
associated with a 34% reduction in relative risk of all-cause mortality in patients with chronic heart failure due to ischaemic or dilated cardiomyopathy in the MERIT-HF trial.
• The incidence of sudden death and death due to progressive heart failure were both significantly decreased with metoprolol CR/XL.
Prakash A et al, Drugs. 2000 Sep;60(3):647-78

METOPROLOLIN HEART FAILURE
MERIT-HF • The drug is well tolerated when treatment is
initiated in low dosages and gradually increased at intervals of 1 to 2 weeks.
• Conclusions of the study was Metoprolol CR/XL effectively decreases mortality and improves clinical status in patients with stable mild to moderate (NYHA functional class II or III) chronic heart failure due to left ventricular systolic dysfunction, and the drug is effective in patients with ischaemic or dilated cardiomyopathy.
Prakash A et al, Drugs. 2000 Sep;60(3):647-78

THANK YOU







